
Finding Stability—A Case Report on the Benefits of Adapted Kata Training for Children with Autism Spectrum Disorder

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participant
- Official ASD diagnosis;
- Does not exhibit behavioral problems (The information that the participant did not have any behavioral problems was obtained as a result of the participant’s health report and the information of his family.);
- No health problems;
- Not disturbed by social interactions (touching);
- Had not previously been enrolled in any physical activity programs or classes to enhance his balance skills for any objective.
2.2. Measurement Tools
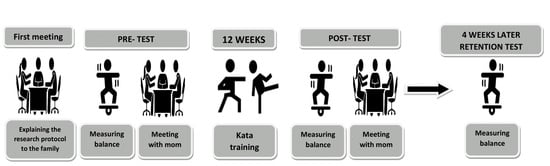
2.3. Procedure
2.4. Data Analysis
2.5. Validity and Reliability
2.6. AKTP
Kata
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Cook, J.L.; Blakemore, S.J.; Press, C. Atypical basic movement kinematics in autism spectrum conditions. Brain 2013, 136, 2816–2824. [Google Scholar] [CrossRef] [PubMed]
- Schurink, J.; Hartman, E.; Scherder, E.J.A.; Houwen, S.; Visscher, C. Relationship between motor and executive functioning in school-age children with pervasive developmental disorder not otherwise specified. Res. Autism Spectr. Disord. 2012, 6, 726–732. [Google Scholar] [CrossRef]
- Whyatt, C.P.; Craig, C.M. Motor skills in children aged 7–10 years, diagnosed with autism spectrum disorder. J. Autism Dev. Disord. 2012, 42, 1799–1809. [Google Scholar] [CrossRef] [PubMed]
- Libertus, K.; Sheperd, K.A.; Ross, S.W.; Landa, R.J. Limited fine motor and grasping skills in 6-month-old infants at high risk for autism. Child Dev. 2014, 85, 2218–2231. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Miller, V.S.; Cauller, L.; Kendall, R.; Mehta, J.; Dodd, M. Effectiveness of N, N-dimethylglycine in autism and pervasive developmental disorder. J. Child Neurol. 2001, 16, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Vernazza-Martin, S.; Martin, N.; Vernazza, A.; Lepellec-Muller, A.; Rufo, M.; Massion, J.; Assaiante, C. Goal directed locomotion and balance control in autistic children. J. Autism Dev. Disord. 2005, 35, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Memari, A.H.; Ghanouni, P.; Gharibzadeh, S.; Eghlidi, J.; Ziaee, V.; Moshayedi, P. Postural sway patterns in children with autism spectrum disorder compared with typically developing children. Res. Autism Spectr. Disord. 2013, 7, 325–332. [Google Scholar] [CrossRef]
- Travers, B.G.; Powell, P.S.; Klinger, L.G.; Klinger, M.R. Motor difficulties in autism spectrum disorder: Linking symptom severity and postural stability. J. Autism Dev. Disord. 2013, 43, 1568–1583. [Google Scholar] [CrossRef] [PubMed]
- Stins, J.F.; Emck, C.; de Vries, E.M.; Doop, S.; Beek, P.J. Attentional and sensory contributions to postural sway in children with autism spectrum disorder. Gait Posture 2015, 42, 199–203. [Google Scholar] [CrossRef]
- Sam, K.L.; Smith, A.W.; Kai, L.S. Visual Cognition and Dynamic Balance in Persons with Autism Spectrum Disorder. Int. J. Soc. Sci. Humanit. 2017, 7, 274–277. [Google Scholar] [CrossRef]
- Jasmin, E.; Couture, M.; McKinley, P.; Reid, G.; Fombonne, E.; Gisel, E. Sensori-motor and daily living skills of preschool children with autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 231–241. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Theory and practical applications. In Motor Control; Williams & Wilkins: Baltimore, MD, USA, 1995. [Google Scholar]
- Cignetti, F.; Caudron, S.; Vaugoyeau, M.; Assaiante, C. Body schema disturbance in adolescence: From proprioceptive integration to the perception of human movement. J. Mot. Learn. Dev. 2013, 1, 49–58. [Google Scholar] [CrossRef][Green Version]
- Assaiante, C.; Barlaam, F.; Cignetti, F.; Vaugoyeau, M. Body schema building during childhood and adolescence: A neurosensory approach. Neurophysiologie Clin. Clin. Neurophysiol. 2014, 44, 3–12. [Google Scholar] [CrossRef]
- Glazebrook, C.M.; Elliott, D.; Lyons, J. A kinematic analysis of how young adults with and without autism plan and control goal-directed movements. Mot. Control 2006, 10, 244–264. [Google Scholar] [CrossRef]
- Graham, S.A.; Abbott, A.E.; Nair, A.; Lincoln, A.J.; Müller, R.A.; Goble, D.J. The influence of task difficulty and participant age on balance control in ASD. J. Autism Dev. Disord. 2015, 45, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Oster, L.M.; Zhou, G. Balance and Vestibular Deficits in Pediatric Patients with Autism Spectrum Disorder: An Underappreciated Clinical Aspect. Autism Res. Treat. 2022, 2022, 7568572. [Google Scholar] [CrossRef]
- Mulligan, S. Validity of the postrotary nystagmus test for measuring vestibular function. OTJR Occup. Particip. Health 2011, 31, 97–104. [Google Scholar] [CrossRef]
- Zanelli, G.; Cappa, P.; Petrarca, M.; Berthoz, A. Vestibular and proprioceptive estimation of imposed rotation and spatial updating in standing subjects. Gait Posture 2011, 33, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Clyse, S.J.; Short, M.A. The Relationship between Dynamic Balance and Postrotary Nystagmus in Learning Disabled Children. Phys. Occup. Ther. Pediatr. 1983, 3, 25–32. [Google Scholar] [CrossRef]
- Blanche, E.I.; Botticelli, T.M.; Hallway, M.K. Combining Neuro-Developmental Treatment and Sensory Integration Principles: An Approach to Pediatric Therapy; Therapy Skill Builders: Canning Vale, WA, Australia, 1995. [Google Scholar]
- Stins, J.F.; Emck, C. Balance Performance in Autism: A Brief Overview. Front. Psychol. 2018, 9, 901. [Google Scholar] [CrossRef]
- Roșca, A.M.; Rusu, L.; Marin, M.I.; Ene Voiculescu, V.; Ene Voiculescu, C. Physical Activity Design for Balance Rehabilitation in Children with Autism Spectrum Disorder. Children 2022, 9, 1152. [Google Scholar] [CrossRef]
- Hariri, R.; Nakhostin-Ansari, A.; Mohammadi, F.; Memari, A.H.; Oskouie, I.M.; Haghparast, A. An Overview of the Available Intervention Strategies for Postural Balance Control in Individuals with Autism Spectrum Disorder. Autism Res. Treat. 2022, 2022, 3639352. [Google Scholar] [CrossRef]
- Djordjević, M.; Memisevic, H.; Potic, S.; Djuric, U. Exercise-Based Interventions Aimed at Improving Balance in Children with Autism Spectrum Disorder: A Meta-Analysis. Percept. Mot. Ski. 2022, 129, 90–119. [Google Scholar] [CrossRef]
- Ji, Y.Q.; Tian, H.; Zheng, Z.Y.; Ye, Z.Y.; Ye, Q. Effectiveness of exercise intervention on improving fundamental motor skills in children with autism spectrum disorder: A systematic review and meta-analysis. Front. Psychiatry 2023, 14, 1132074. [Google Scholar] [CrossRef]
- Crane, L.; Goddard, L.; Pring, L. Sensory processing in adults with autism spectrum disorders. Autism 2009, 13, 215–228. [Google Scholar] [CrossRef]
- Cordo, P.J.; Nashner, L.M. Properties of postural adjustments associated with rapid arm movements. J. Neurophysiol. 1982, 47, 287–302. [Google Scholar] [CrossRef]
- Orhan, B.E. Otizm Spektrum Bozukluğunda Problem Davranışlar ve Uyarlanmış Fiziksel Aktivite Etkinlikleri; Lap Lambert: Beau Bassin, Mauritius, 2021. [Google Scholar]
- Orhan, B.E. Uyarlanmış Fiziksel Aktivitelere Katılan Otizm Spektrum Bozukluğu Olan bir Bireyin Davranış Problemlerindeki Değişimlerin Incelenmesi. Yayınlanmamış Doktora Tezi, Gazi Üniversitesi, Ankara, Turkey, 2020. [Google Scholar]
- Orhan, B.E. Otizm Spektrum Bozukluğu ve Fiziksel Aktivite İlişkisi. In Psiko-Sosyalden Antrenmana Spor Bilimlerinde Güncel Çalışmalar; LAM LAMBERT Academic Publishing: Chisinau, Moldova, 2021; pp. 143–156. [Google Scholar]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Creswell, J.W.; Clark, V.L.P. Designing and Conducting Mixed Methods Research; Sage: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Emerson, R.W. Convenience sampling revisited: Embracing its limitations through thoughtful study design. J. Vis. Impair. Blind. 2021, 115, 76–77. [Google Scholar] [CrossRef]
- Liviu, M.; Ilie, M.; Fernando, G. Determination of balance parameters as physical training factors in Athletics. J. Phys. Educ. Sport 2018, 18, 2054. [Google Scholar] [CrossRef]
- Klostermann, A. Test-Retest Reliability of The Interactive Training Software Neuromuscular Control Tests Using The Sensbalance MiniBoard in Healthy Young Adults. Doctoral Dissertation, FOAF, Rotterdam, The Netherlands, 2015. [Google Scholar]
- Porciuncula, F.; Wasserman, P.; Marder, K.S.; Rao, A.K. Quantifying postural control in premanifest and manifest huntington disease using wearable sensors. Neurorehabilit. Neural Repair. 2020, 34, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Vila-Chã, C.; Riis, S.; Lund, D.; Møller, A.; Farina, D.; Falla, D. effect of unaccustomed eccentric exercise on proprioception of the knee in weight and non-weight bearing tasks. J. Electromyogr. Kinesiol. 2011, 21, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Waddington, G.S.; Adams, R.D. The effect of a 5-week wobble-board exercise intervention on ability to discriminate different degrees of ankle inversion, barefoot and wearing shoes: A study in healthy elderly. J. Am. Geriatr. Soc. 2004, 52, 573–576. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.B.; Huberman, A.M. Qualitative Data Analysis: An Expanded Sourcebook; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Yıldırım, A.; Şimşek, H. Sosyal Bilimlerde Nitel Araştırma Yöntemleri, 10th ed.; Seçkin Yayıncılık: Ankara, Turkey, 2016. [Google Scholar]
- Nakayama, M. Best Karate: Heian, Tekki, 5th ed.; Kodansha USA Incorporated: New York, NY, USA, 1979. [Google Scholar]
- Bahrami, F.; Movahedi, A.; Marandi, S.M.; Abedi, A. Kata techniques training consistently decreases stereotypy in children with autism spectrum disorder. Res. Dev. Disabil. 2012, 33, 1183–1193. [Google Scholar] [CrossRef]
- Ansari, S.; Hosseinkhanzadeh, A.A.; AdibSaber, F.; Shojaei, M.; Daneshfar, A. The effects of aquatic versus kata techniques training on static and dynamic balance in children with autism spectrum disorder. J. Autism Dev. Disord. 2021, 51, 3180–3186. [Google Scholar] [CrossRef]
- Filingeri, D.; Bianco, A.; Zangla, D.; Paoli, A.; Palma, A. Is karate effective in improving postural control? Arch. BUDO 2012, 8, 191–194. [Google Scholar] [CrossRef]
- Vando, S.; Filingeri, D.; Maurino, L.; Chaabène, H.; Bianco, A.; Salernitano, G.; Padulo, J. Postural adaptations in preadolescent karate athletes due to a one week karate training camp. J. Hum. Kinet. 2013, 38, 45. [Google Scholar] [CrossRef]
- Cheldavi, H.; Shakerian, S.; Boshehri, S.N.S.; Zarghami, M. The effects of balance training intervention on postural control of children with autism spectrum disorder: Role of sensory information. Res. Autism Spectr. Disord. 2014, 8, 8–14. [Google Scholar] [CrossRef]
- Cesari, P.; Bertucco, M. Coupling between punch efficacy and body stability for elite karate. J. Sci. Med. Sport 2008, 11, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Fong, S.M. Effect of Taekwondo Training on Sensori-Motor Performance and Postural Control in Children with and without Developmental Coordination Disorder. Ph.D. Thesis, Hong Kong Polytechnic University, Hong Kong, China, 2012. [Google Scholar]
- Henderson, S.E.; Sugden, D.; Barnett, A.L. Movement Assessment Battery for Children-2; Research in Developmental Disabilities; Pearson: London, UK, 1992. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Sanford, C.B. Test of Gross Motor Development, 2nd ed.; Proed: Austin, TX, USA, 2000. [Google Scholar]
- Emck, C.; Bosscher, R.J.; Van Wieringen, P.C.; Doreleijers, T.; Beek, P.J. Gross motor performance and physical fitness in children with psychiatric disorders. Dev. Med. Child Neurol. 2011, 53, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Berkeley, S.L.; Zittel, L.L.; Pitney, L.V.; Nichols, S.E. Locomotor and object control skills of children diagnosed with autism. Adapt. Phys. Act. Q. 2001, 18, 405–416. [Google Scholar] [CrossRef]
- Yilmaz, I.; Yanardağ, M.; Birkan, B.; Bumin, G. Effects of swimming training on physical fitness and water orientation in autism. Pediatr. Int. 2004, 46, 624–626. [Google Scholar] [CrossRef]
- Baccouch, R.; Rebai, H.; Sahli, S. Kung-fu versus swimming training and the effects on balance abilities in young adolescents. Phys. Ther. Sport 2015, 16, 349–354. [Google Scholar] [CrossRef]
- Kim, Y.; Todd, T.; Fujii, T.; Lim, J.C.; Vrongistinos, K.; Jung, T. Effects of Taekwondo intervention on balance in children with autism spectrum disorder. J. Exerc. Rehabil. 2016, 12, 314. [Google Scholar] [CrossRef]
- Battaglia, G.; Agrò, G.; Cataldo, P.; Palma, A.; Alesi, M. Influence of a specific aquatic program on social and gross motor skills in adolescents with autism spectrum disorders: Three case reports. J. Funct. Morphol. Kinesiol. 2019, 4, 27. [Google Scholar] [CrossRef]
- Sarabzadeh, M.; Azari, B.B.; Helalizadeh, M. The effect of six weeks of Tai Chi Chuan training on the motor skills of children with Autism Spectrum Disorder. J. Bodyw. Mov. Ther. 2019, 23, 284–290. [Google Scholar] [CrossRef]
- Salar, S.; Daneshmandi, H.; Karimizadeh Ardakani, M.; Nazari Sharif, H. The relationship of core strength with static and dynamic balance in children with autism. Ann. Appl. Sport Sci. 2014, 2, 33–42. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, M.; Park, C.; You, J.H. Effects of Integrative Autism Therapy on Multiple Physical, Sensory, Cognitive, and Social Integration Domains in Children and Adolescents with Autism Spectrum Disorder: A 4-Week Follow-Up Study. Children 2022, 9, 1971. [Google Scholar] [CrossRef]
- Movahedi, A.; Bahrami, F.; Marandi, S.M.; Abedi, A. Improvement in social dysfunction of children with autism spectrum disorder following long term Kata techniques training. Res. Autism Spectr. Disord. 2013, 7, 1054–1061. [Google Scholar] [CrossRef]
- Bahrami, F.; Movahedi, A.; Marandi, S.M.; Sorensen, C. The effect of karate techniques training on communication deficit of children with autism spectrum disorders. J. Autism Dev. Disord. 2016, 46, 978–986. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Balance Performance | 1. Measurement (%) | 2. Measurement (%) | 3. Measurement (%) |
|---|---|---|---|
| Static | 75 | 81 | 86 |
| Proprioceptive | 73 | 77 | 81 |
| Left–Right Horizontal | 72 | 77 | 84 |
| Front–Back Vertical | 81 | 84 | 95 |
| Average Deviation | Static Balance | Proprioceptive Balance | Left–Right Horizontal Dynamic Balance | Forward–Backwards Dynamic Balance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Measurements | Measurements | Measurements | Measurements | |||||||||
| 1. | 2. | 3. | 1. | 2. | 3. | 1. | 2. | 3. | 1. | 2. | 3. | |
| Front Avg. Dev. | 0.85 | 1.69 | 1.01 | 0.37 | 0.40 | 0.39 | 1.91 | 1.20 | 1.02 | 2.37 | 2.42 | 2.46 |
| Back Avg. Dev. | −1.74 | −1.44 | −0.79 | −2.13 | −1.66 | −0.81 | −1.29 | −1.01 | −0.90 | −1.16 | −1.20 | −1.21 |
| Left Avg. Dev. | −1.90 | −0.86 | −0.82 | −1.78 | −0.85 | −0.65 | −2.76 | −2.82 | −2.90 | −1.75 | −1.60 | −1.50 |
| Right Avg. Dev. | 1.53 | 0.80 | 0.99 | 1.33 | 1.42 | 1.10 | 2.19 | 2.30 | 2.46 | 1.27 | 1.10 | 1.10 |
| Categories | Question | Quotations |
|---|---|---|
| Socialization | Did he have friends or spend time with other children regularly? What prevented him from socializing or hindered his socializing? | “He did not have many friends at school that he had communicated with before, and the situation made my son very sad; he did not want to talk too much and closed himself in communication. However, as the course went on, he spent more time with other kids, and as he got involved in the games and became successful, he became more confident and happier.” “We used to have many problems with walking and running; for these reasons, he was worried and closed himself off in social situations.” |
| Physical changes | Have you observed any change in his physical condition? What would you consider the most significant physical benefits for your son after following the programme? | “We noticed the change a lot; for example, before the AKTP, he could not climb the stairs without holding on and without support, but now he can go up and down the stairs independently.” “Before AKTP, they had much stumbling and falling almost every time he ran, and much swaying was in place. After AKTP, he occasionally falls like every normal kid, but it is almost non-existent, and his swaying has disappeared. Apart from the disappearance of the swaying, his body shape has started to improve. The doctor who followed my son noticed these developments and told us we should stop.” |
| Psychological changes | What was his typical reaction when going outside to play? How would you describe his confidence level before and after the program? | “When we went to the playground before AKTP, he quickly got bored and wanted to leave. I could see his fear and anxiety when on the playground. However, he has enjoyed the park very much and can play independently in the park.” “Previously, he was very reluctant to do something. I spent a long time convincing my son to do something. Usually, he was saying’’ I do not know that; I cannot do this. Later, he realized what he could and could do with the training, and now his motivation has increased in many places, including at school.” “Nowadays, he is expressing himself more with the self-confidence of acting completely independently.” |
| Emotional changes | What was a typical emotional response to difficulties or challenges? Was he able to build emotional connections with his peers? | “Before AKTP, my son had behaviours such as shouting, crying, throwing himself on the ground and hitting the person in front of him, albeit a little. However, he calmed down after the training, and his communication and attention span with us and his surroundings increased.” “While playing with his friends, he preferred to play for a short time and then get away from them, and he only spent time with children younger than him because he did not need to say much. However, after AKTP, he spoke a lot more. He started to trust himself, and even his eye contact improved; he seemed happier.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orhan, B.E.; Uzunçayır, D.; Canlı, U.; Karaçam, A.; Özdemir, A.S.; Popa, C.; Iconomescu, T.-M.; Talaghir, L.-G. Finding Stability—A Case Report on the Benefits of Adapted Kata Training for Children with Autism Spectrum Disorder. Children 2024, 11, 523. https://doi.org/10.3390/children11050523
Orhan BE, Uzunçayır D, Canlı U, Karaçam A, Özdemir AS, Popa C, Iconomescu T-M, Talaghir L-G. Finding Stability—A Case Report on the Benefits of Adapted Kata Training for Children with Autism Spectrum Disorder. Children. 2024; 11(5):523. https://doi.org/10.3390/children11050523
Chicago/Turabian StyleOrhan, Bekir Erhan, Dilek Uzunçayır, Umut Canlı, Aydın Karaçam, Ali Selman Özdemir, Cristian Popa, Teodora-Mihaela Iconomescu, and Laurențiu-Gabriel Talaghir. 2024. "Finding Stability—A Case Report on the Benefits of Adapted Kata Training for Children with Autism Spectrum Disorder" Children 11, no. 5: 523. https://doi.org/10.3390/children11050523
APA StyleOrhan, B. E., Uzunçayır, D., Canlı, U., Karaçam, A., Özdemir, A. S., Popa, C., Iconomescu, T.-M., & Talaghir, L.-G. (2024). Finding Stability—A Case Report on the Benefits of Adapted Kata Training for Children with Autism Spectrum Disorder. Children, 11(5), 523. https://doi.org/10.3390/children11050523