
Testicular Vascularization after Pediatric Inguinal Hernia Repair: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Article Selection
2.4. Data Extraction and Statistical Analysis
2.5. Risk of Bias Assessment
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Methodological Quality
3.4. Primary Outcome
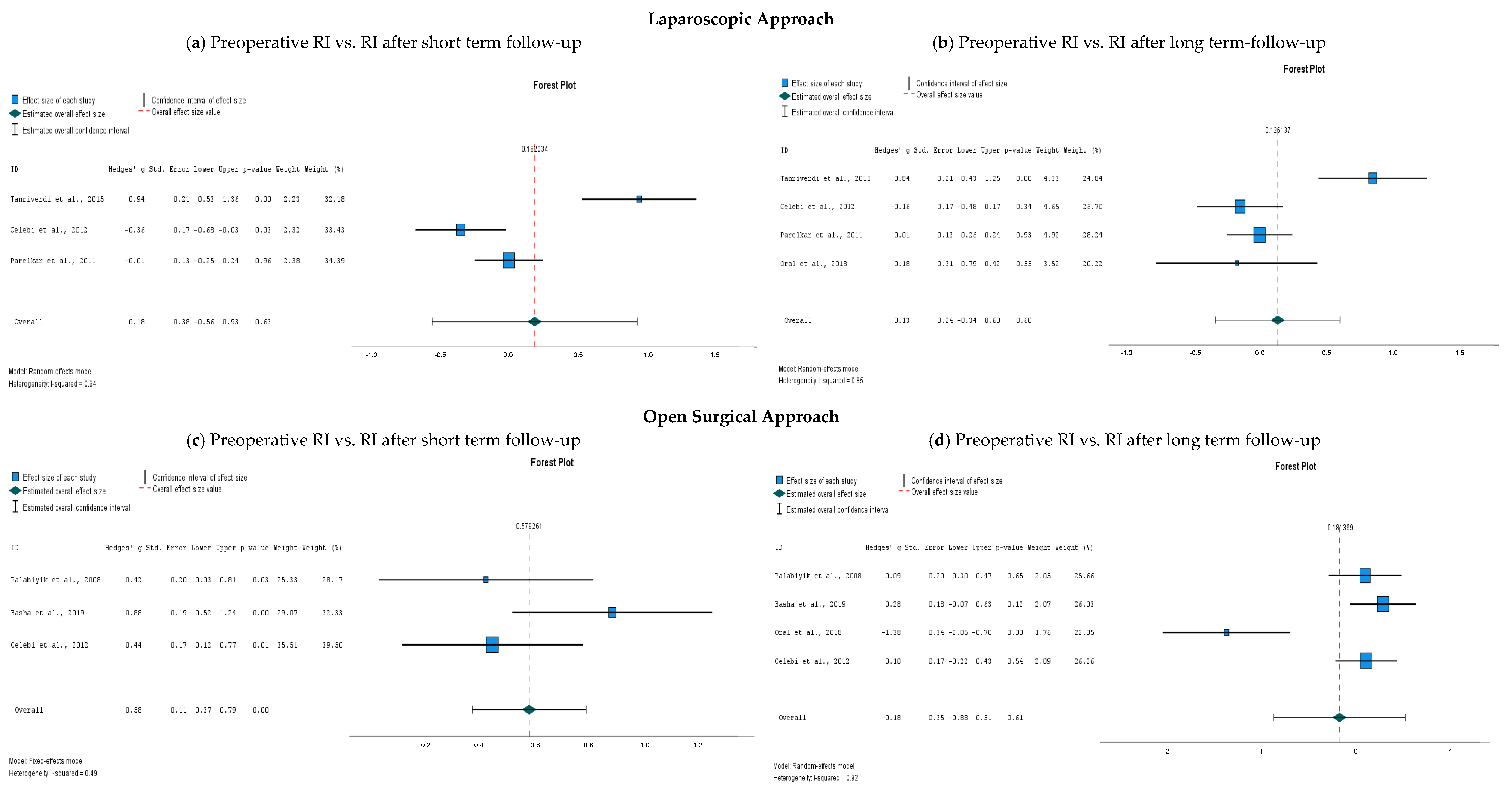
3.4.1. Preoperative Resistive Index Compared to Postoperative Resistive Index
3.4.2. Resistive Index Values after Laparoscopy Compared to Open Surgery
3.5. Secondary Outcomes
3.5.1. Testicular Volume
3.5.2. Other Clinical Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yeap, E.; Pacilli, M.; Nataraja, R.M. Inguinal hernias in children. Aust. J. Gen. Pract. 2020, 49, 38–43. [Google Scholar] [CrossRef]
- Esposito, C.; Escolino, M.; Turrà, F.; Roberti, A.; Cerulo, M.; Farina, A.; Caiazzo, S.; Cortese, G.; Servillo, G.; Settimi, A. Current concepts in the management of inguinal hernia and hydrocele in pediatric patients in laparoscopic era. Semin. Pediatr. Surg. 2016, 25, 232–240. [Google Scholar] [CrossRef]
- Feng, S.; Zhao, L.; Liao, Z.; Chen, X. Open Versus Laparoscopic Inguinal Herniotomy in Children: A Systematic Review and Meta-Analysis Focusing on Postoperative Complications. Surg. Laparosc. Endosc. Percutan. Tech. 2015, 25, 275. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; St Peter, S.D.; Escolino, M.; Juang, D.; Settimi, A.; Holcomb, G.W. Laparoscopic Versus Open Inguinal Hernia Repair in Pediatric Patients: A Systematic Review. J. Laparoendosc. Adv. Surg. Tech. 2014, 24, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Shun, A.; Puri, P. Inguinal hernia in the newborn A 15-year review. Pediatr. Surg. Int. 1988, 3, 156–157. [Google Scholar] [CrossRef]
- McGregor, D.B.; Halverson, K.; McVay, C.B. The unilateral pediatric inguinal hernia: Should the contralateral side by explored? J. Pediatr. Surg. 1980, 15, 313–317. [Google Scholar] [CrossRef]
- Puri, P.; Guiney, E.J.; O’Donnell, B. Inguinal hernia in infants: The fate of the testis following incarceration. J. Pediatr. Surg. 1984, 19, 44–46. [Google Scholar] [CrossRef] [PubMed]
- Janik, J.S.; Shandling, B. The vulnerability of the vas deferens (II): The case against routine bilateral inguinal exploration. J. Pediatr. Surg. 1982, 17, 585–588. [Google Scholar] [CrossRef]
- Potts, W.J.; Riker, W.L.; Lewis, J.E. The treatment of inguinal hernia in infants and children. Ann. Surg. 1950, 132, 566–576. [Google Scholar] [CrossRef]
- Le Coultre, C.; Cuendet, A.; Richon, J. Frequency of testicular atrophy following incarcerated hernia. Z. Kinderchir. Organ. Dtsch. Schweiz. Osterreichischen Ges. Kinderchir. Surg. Infancy Child. 1983, 38, 39–41. [Google Scholar] [CrossRef]
- Walc, L.; Bass, J.; Rubin, S.; Walton, M. Testicular fate after incarcerated hernia repair and/or orchiopexy performed in patients under 6 months of age. J. Pediatr. Surg. 1995, 30, 1195–1197. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.; Schwartzbard, A.; Velcek, F.T.; Klotz, D.H.; Kottmeier, P.K. The government and the inguinal hernia. J. Pediatr. Surg. 1979, 14, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Sonderman, K.A.; Wolf, L.L.; Armstrong, L.B.; Taylor, K.; Jiang, W.; Weil, B.R.; Koehlmoos, T.P.; Ricca, R.L.; Weldon, C.B.; Haider, A.H.; et al. Testicular atrophy following inguinal hernia repair in children. Pediatr. Surg. Int. 2018, 34, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Ein, S.H.; Njere, I.; Ein, A. Six thousand three hundred sixty-one pediatric inguinal hernias: A 35-year review. J. Pediatr. Surg. 2006, 41, 980–986. [Google Scholar] [CrossRef]
- Miyake, H.; Fukumoto, K.; Yamoto, M.; Nouso, H.; Kaneshiro, M.; Nakajima, H.; Koyama, M.; Urushihara, N. Comparison of percutaneous extraperitoneal closure (LPEC) and open repair for pediatric inguinal hernia: Experience of a single institution with over 1000 cases. Surg. Endosc. 2016, 30, 1466–1472. [Google Scholar] [CrossRef]
- Niedzielski, J.; Kr, L.R.; Gawłowska, A. Could incarceration of inguinal hernia in children be prevented? Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2003, 9, CR16–CR18. [Google Scholar]
- Orth, R.C.; Towbin, A.J. Acute testicular ischemia caused by incarcerated inguinal hernia. Pediatr. Radiol. 2012, 42, 196–200. [Google Scholar] [CrossRef]
- Grosfeld, J.L. Current concepts in inguinal hernia in infants and children. World J. Surg. 1989, 13, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P.T. Chapter 25: Assessing risk of bias in a non-randomized study. In Cochrane Handbook for Systematic Reviews of Interventions; 6.3. Cochrane; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley: Hoboken, NJ, USA, 2022; Available online: https://training.cochrane.org/handbook (accessed on 18 July 2023).
- Palabiyik, F.B.; Cimilli, T.; Kayhan, A.; Toksoy, N. Do the manipulations in pediatric inguinal hernia operations affect the vascularization of testes? J. Pediatr. Surg. 2009, 44, 788–790. [Google Scholar] [CrossRef] [PubMed]
- Parelkar, S.V.; Oak, S.; Bachani, M.K.; Sanghvi, B.; Prakash, A.; Patil, R.; Sahoo, S.; Patel, J. Laparoscopic repair of pediatric inguinal hernia—Is vascularity of the testis at risk? A study of 125 testes. J. Pediatr. Surg. 2011, 46, 1813–1816. [Google Scholar] [CrossRef] [PubMed]
- Basha, M.A.A.; Saber, S.; El-Hamid, M.; Abdalla, A.A.; Aly, S.A.; GObran, T.; Waly, A.; Arafa, A.S. Assessment of the testicular vascularity after inguinal herniotomy in children: A prospective color Doppler study. Acta Radiol. 2020, 61, 128–135. [Google Scholar] [CrossRef]
- Çelebi, S.; Yıldız, A.; Üçgül, A.; Karadağ, Ç.A.; Sever, N.; Akın, M.; Dokucu, A.İ. Do open repair and different laparoscopic techniques in pediatric inguinal hernia repairs affect the vascularization of testes? J. Pediatr. Surg. 2012, 47, 1706–1710. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, H.I.; Senel, U.; Ozmen, Z.; Aktaş, F. Does the Percutaneous Internal Ring Suturing Technique Impair Testicular Vascularization in Children Undergoing Inguinal Hernia Repair? J. Laparoendosc. Adv. Surg. Tech. A 2015, 25, 951–953. [Google Scholar] [CrossRef]
- Oral, A.; Karaca, L.; Ahiskalioglu, A.; Yildiz, A.; Yigiter, M.; Celikkaya, M.E.; Chyndolotov, T.; Salman, A.B. Effects of Laparoscopic Hernia Repair by PIRS (Percutan Internal Ring Suturing) Technique on Testicular Artery Blood Supply. J. Investig. Surg. Off. J. Acad. Surg. Res. 2019, 32, 343–347. [Google Scholar] [CrossRef]
- Tuncer, A.A.; Peker, T.; Acar, M.B.; Embleton, D.B.; Cetinkursun, S. A comparison of preoperative and postoperative testicular volume and blood flow in patients with inguinal hernia, hydrocele, and cord cyst: A prospective cohort study. Pak. J. Med. Sci. 2017, 33, 363–368. [Google Scholar] [CrossRef]
- Seher, N.; Nayman, A.; Koplay, M.; Çiftci, İ. Comparison of Preoperative and Postoperative Testicular Elasticity and Vascularity in Pediatric Patients with Inguinal Hernia. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2022, 41, 71–78. [Google Scholar] [CrossRef]
- Schier, F.; Turial, S.; Hückstädt, T.; Klein, K.U.; Wannik, T. Laparoscopic inguinal hernia repair does not impair testicular perfusion. J. Pediatr. Surg. 2008, 43, 131–135, discussion 135. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.Y.M.; Poon, M.; Fan, T.W.; Siu, K.W.; Chung, K.W.; Kwok, W.K.; Kwok, C.H. Testicular volume of boys after inguinal herniotomy: Combined clinical and radiological follow-up. Pediatr. Surg. Int. 1999, 15, 40–41. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Pavlica, P.; Barozzi, L. Imaging of the acute scrotum. Eur. Radiol. 2001, 11, 220–228. [Google Scholar] [CrossRef]
- Wantz, G.E. Testicular atrophy as a sequela of inguinal hernioplasty. Int. Surg. 1986, 71, 159–163. [Google Scholar] [PubMed]
- Turgut, A.T.; Ölçücüoğlu, E.; Turan, C.; Kiliçoğlu, B.; Koşar, P.; Geyik, P.Ö.; Koşar, U.; Dogra, V. Preoperative ultrasonographic evaluation of testicular volume and blood flow in patients with inguinal hernias. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2007, 26, 1657–1666, quiz 1667–1669. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Saito, M.; Kinoshita, Y.; Shomori, K.; Satoh, I.; Satoh, K. Ischemic preconditioning and post-conditioning to decrease testicular torsion-detorsion injury. J. Urol. 2009, 182, 1637–1643. [Google Scholar] [CrossRef]
- Li, J.; Yan, Z.; Wang, Q.; Wei, S.; Liu, Q.; Liu, T.; Hu, Z. Pretreatment with remote ischemic conditioning attenuates testicular damage after testicular ischemia and reperfusion injury in rats. PLoS ONE 2023, 18, e0287987. [Google Scholar] [CrossRef]
- Zhang, X.; Lv, F.; Tang, J. Protection from ischemia by preconditioning, postconditioning, and combined treatment in rabbit testicular ischemia reperfusion injury. Arch. Biochem. Biophys. 2016, 608, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sahinkanat, T.; Ozkan, K.U.; Tolun, F.I.; Ciralik, H.; Imrek, S.S. The protective effect of ischemic preconditioning on rat testis. Reprod. Biol. Endocrinol. RBE 2007, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Mansour, M.; Degheili, J.; Khalifeh, I.; Tamim, H.; Jaafar, R.F.; El-Hout, Y. Remote ischemic conditioning in a rat model of testicular torsion: Does it offer testicular protection? J. Pediatr. Urol. 2019, 15, 43.e1–43.e7. [Google Scholar] [CrossRef] [PubMed]
- Duru, F.I.O.; Olabiyi, O.; Noronha, C.C.; Akinwande, A.I.; Okanlawon, A.O. Brief ischaemia reduces testicular lipid peroxidation following subsequent ischaemia: An evidence for ischaemic preconditioning. Niger. Q. J. Hosp. Med. 2008, 18, 149–152. [Google Scholar]
- Pinggera, G.; Mitterberger, M.; Bartsch, G.; Strasser, H.; Gradl, J.; Aigner, F.; Pallwein, L.; Frauscher, F. Assessment of the intratesticular resistive index by colour Doppler ultrasonography measurements as a predictor of spermatogenesis. BJU Int. 2008, 101, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Kay, G.W.; Grobbelaar, J.A.; Hattingh, J. Effect of surgical restriction of growth of the testicular artery on testis size and histology in bulls. J. Reprod. Fertil. 1992, 96, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Yavetz, H.; Harash, B.; Yogev, L.; Homonnai, Z.T.; Paz, G. Fertility of men following inguinal hernia repair. Andrologia 1991, 23, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Silber, S.; Becker, V.M.; Seufert, R.; Muensterer, O.J. Fertility in males after childhood, adolescent, and adult inguinal operations. J. Pediatr. Surg. 2019, 54, 177–183. [Google Scholar] [CrossRef]
- Zendejas, B.; Zarroug, A.E.; Erben, Y.M.; Holley, C.T.; Farley, D.R. Impact of childhood inguinal hernia repair in adulthood: 50 years of follow-up. J. Am. Coll. Surg. 2010, 211, 762–768. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Author and Publication Year | Country | Study Design | Level of Evidence | Indication | Operation Technique | Intervention Comparison | No. of Participants | No. of IH | Mean Age (Range) | Duration of FU in Months | Outcome Measurement | Reported Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tanriverdi et al., 2015 [29] | Turkey | Prospective study | VI | Unilateral IH | Laparoscopic repair (PIRS) | Preoperative measures | 49 | 49 | 5.27 y (1 y–14 y) | 1 | DUS | PSV, EDV, RI |
| Palabiyik et al., 2009 [25] | Turkey | Prospective study | VI | Unilateral IH | Open approach (High ligation) | Preoperative measures | 51 | 51 | 6.33 y (2 y–14 y) | 1 | power DUS | PSV, EDV, RI |
| Çelebi et al., 2012 [28] | Turkey | Prospective study | VI | Unilateral IH | Laparoscopic repair (N-suture and Purse string) | Open approach Contralateral side Preoperative measures | 72 | 72 | 5.65 y | 1 | DUS | PSV, RI |
| Basha et al., 2020 [27] | Egypt | Prospective study | VI | Unilateral and Bilateral IH | Open approach (High ligation) | Preoperative measures | 60 | 63 | 9.46 m ± 14.46 m (2 m–6 y) | 6 | color DUS | PSV, EDV, RI Testicular volume |
| Parelkar et al., 2011 [26] | India | Prospective study | VI | Unilateral and Bilateral IH | Laparoscopic repair (Purse string) | Contralateral side Preoperative measures | 100 | 125 | 4.45 y (1.5 m–12 y) | 6 | color DUS | PSV, EDV, RI Testicular volume |
| Oral et al., 2019 [30] | Turkey | Prospective study | VI | Unilateral IH | Laparoscopic repair (PIRS) | Open approach Contralateral side Preoperative measures | 40 | 40 | 6.80 y ± 3.5 y | 1 | SMI (color DUS) | RI |
| Tuncer et al., 2017 [31] | Turkey | Prospective study | VI | Inguinal hernia Hydrocele Cord cyst | Open approach (High ligation) | Preoperative measures | 23 | 11 | 3.59 y ± 2.67 y (20 d–12 y) | 1 | color DUS | PSV Testicular volume |
| Leung et al., 1999 [34] | Hong Kong | Prospective study | VI | Unilateral IH | Open approach (High ligation) | Preoperative measures | 173 | 173 | (10 m–179 m) | 123 | US | Testicular volume |
| Seher et al., 2022 [32] | Turkey | Prospective study | VI | Unilateral IH | Open approach (High ligation) | Contralateral side Preoperative measures | 44 | 44 | 3.8 y (0 y–10 y) | 6 | SMI (color DUS) + SWE | Testicular volume VI Tissue elasticity/stiffness |
| Schier et al., 2008 [33] | Germany | Prospective study | VI | Unilateral and Bilateral IH | Laparoscopic repair (No technique reported) | Matched controls Preoperative measures | 65 | 78 | (6 w–11 y) | 1.5 | O2C | O2 Saturation at venous end of capillaries Hb in micro vessels Flow, Velocity |
| Study | Technique | Preop RI (Mean ± SD) | Early Postop FU RI (Mean ± SD) | Late Postop FU RI (Mean ± SD) | Preop vs. Early FU (p-Value) | Preop vs. Late FU (p-Value) | Early vs. Late FU (p-Value) |
|---|---|---|---|---|---|---|---|
| Tanriverdi et al., 2015 [29] | Laparoscopic repair (PIRS) | 0.59 ± 0.04 | 0.62 ± 0.02 | 0.62 ± 0.03 | 0.21 | 0.28 | 0.856 |
| Parelkar et al., 2011 [26] | Laparoscopic repair (Purse string) | 0.499 ± 0.36 | 0.497 ± 0.35 | 0.495 ± 0.33 | 0.296 | 0.122 | 0.684 |
| Çelebi et al., 2012 [28] | Laparoscopic repair (N-suture) | 0.66 ± 0.18 | 0.68 ± 0.13 | 0.64 ± 0.10 | 0.309 | NR | 0.692 |
| Laparoscopic repair (Purse string) | 0.66 ± 0.13 | 0.62 ± 0.09 | 0.64 ± 0.12 | 0.452 | NR | 0.673 | |
| Open approach (High ligation) | 0.59 ± 0.13 | 0.64 ± 0.09 | 0.60 ± 0.05 | 0.69 | NR | 0.337 | |
| Oral et al., 2019 [30] | Laparoscopic repair (PIRS) | 0.66 ± 0.45 | NR | 0.60 ± 0.04 | NR | 0.175 | NR |
| Open approach (High ligation) | 0.66 ± 0.07 | NR | 0.58 ± 0.04 | NR | 0.447 | NR | |
| Palabiyik et al., 2009 [25] | Open approach (High ligation) | 0.56 ± 0.09 | 0.61 ± 0.14 | 0.57 ± 0.13 | 0.008 * | 0.764 | 0.036 * |
| Basha et al., 2020 [27] | Open approach (High ligation) | 0.67 ± 0.10 | 0.76 ± 0.10 | 0.68 ± 0.11 | <0.0001 * | 0.181 | NR |
| Preoperative RI (p-Value) | Early Follow-Up RI (p-Value) | Late Follow-Up RI (p-Value) | |
|---|---|---|---|
| N-suture vs. open | 0.125 | 0.231 | 0.099 |
| Purse string vs. open | 0.063 | 0.436 | 0.140 |
| Study | Technique | Preop TV (Mean + SD) | Early Postop FU TV (Mean + SD) | Late Postop FU TV (Mean + SD) | Preop vs. Early FU (p-Value) | Preop vs. Late FU (p-Value) | Ratio TV Preop | Ratio TV Postop | Preop vs. Postop (p-Value) |
|---|---|---|---|---|---|---|---|---|---|
| Basha et al., 2020 [27] | Open approach (high ligation) | 0.779 ± 0.395 | 0.741 ± 0.226 | 0.780 ± 0.310 | 0.25 | 0.98 | NR | NR | NR |
| Parelkar et al., 2011 [26] | Laparoscopic repair (Purse string) | 1.22 ± 0.52 | NR | 1.23 ± 0.54 | NR | 0.291 | 1.029 ± 0.103 | 1.022 ± 0.092 | 0.161 |
| Leung et al., 1999 [34] | Open approach (high ligation) | NR | NR | NR | NR | NR | NR | 1.023 95% CI [0.988–1.058] | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eurlings, R.; Killaars, R.E.M.; Visschers, R.G.J.; van Gemert, W.G. Testicular Vascularization after Pediatric Inguinal Hernia Repair: A Systematic Review and Meta-Analysis. Children 2024, 11, 409. https://doi.org/10.3390/children11040409
Eurlings R, Killaars REM, Visschers RGJ, van Gemert WG. Testicular Vascularization after Pediatric Inguinal Hernia Repair: A Systematic Review and Meta-Analysis. Children. 2024; 11(4):409. https://doi.org/10.3390/children11040409
Chicago/Turabian StyleEurlings, Roxanne, Rianne E. M. Killaars, Ruben G. J. Visschers, and Wim G. van Gemert. 2024. "Testicular Vascularization after Pediatric Inguinal Hernia Repair: A Systematic Review and Meta-Analysis" Children 11, no. 4: 409. https://doi.org/10.3390/children11040409
APA StyleEurlings, R., Killaars, R. E. M., Visschers, R. G. J., & van Gemert, W. G. (2024). Testicular Vascularization after Pediatric Inguinal Hernia Repair: A Systematic Review and Meta-Analysis. Children, 11(4), 409. https://doi.org/10.3390/children11040409