
Use of Validated Questionnaires to Predict Cosmetic Outcomes of Hypospadias Repair

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
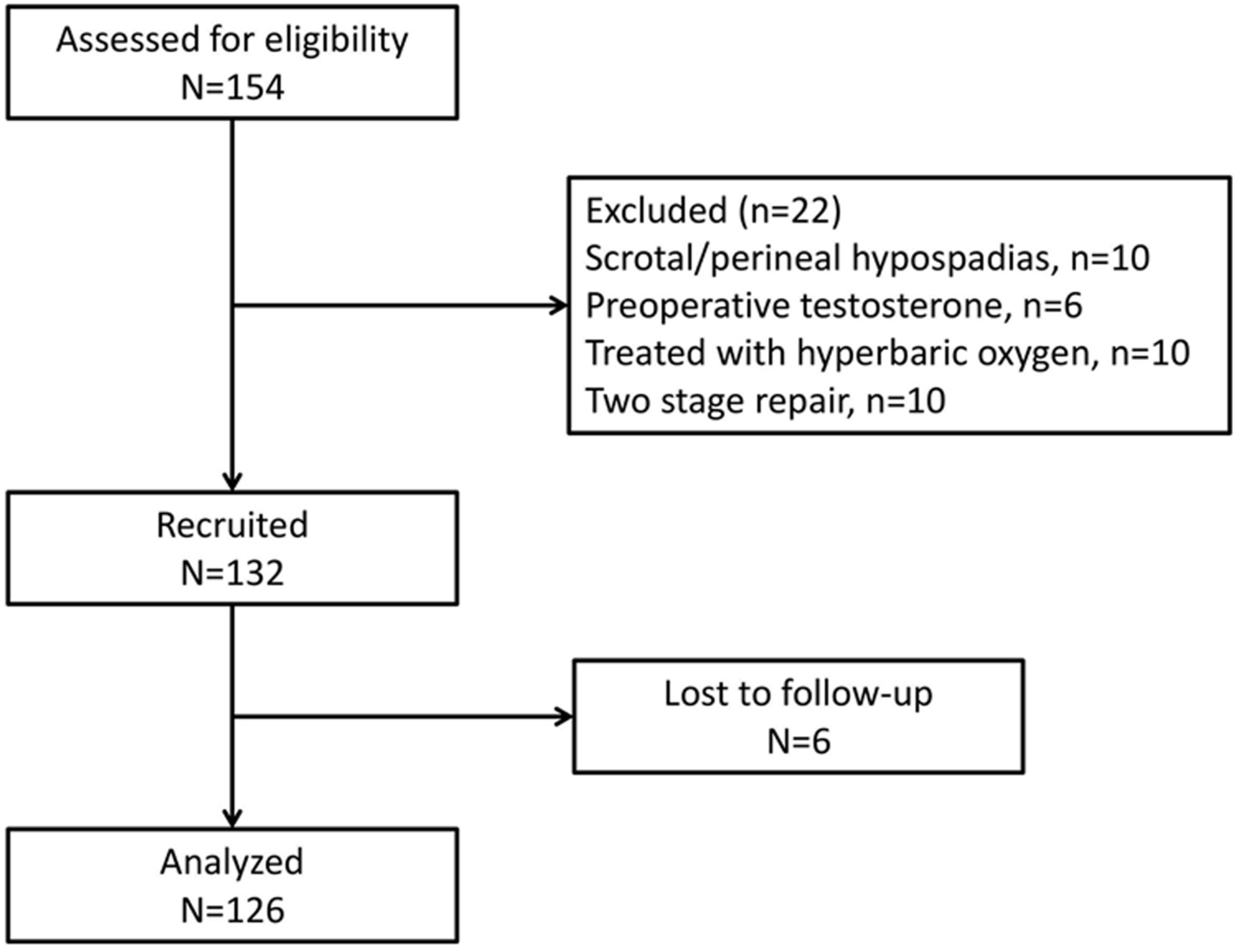
2.1. Study Population
2.2. Study Tools
2.3. Pre-Urethroplasty Information
2.4. Surgical Technique
2.5. Study Outcome Measures
2.6. Statistics
Sample Size Calculation
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | Area under curve |
| CI | Confidence interval |
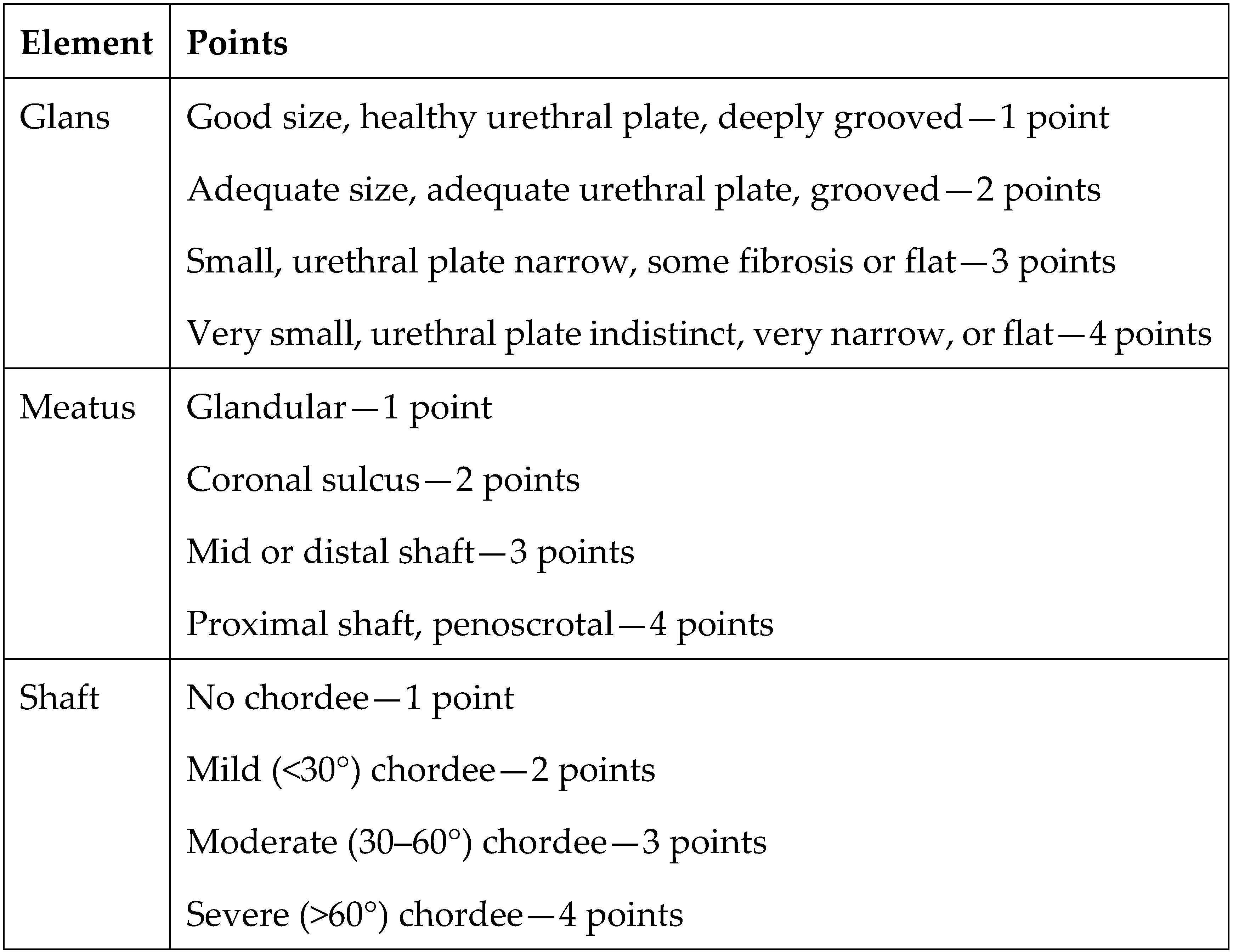
| GMS | Glans–Urethral Meatus–Shaft |
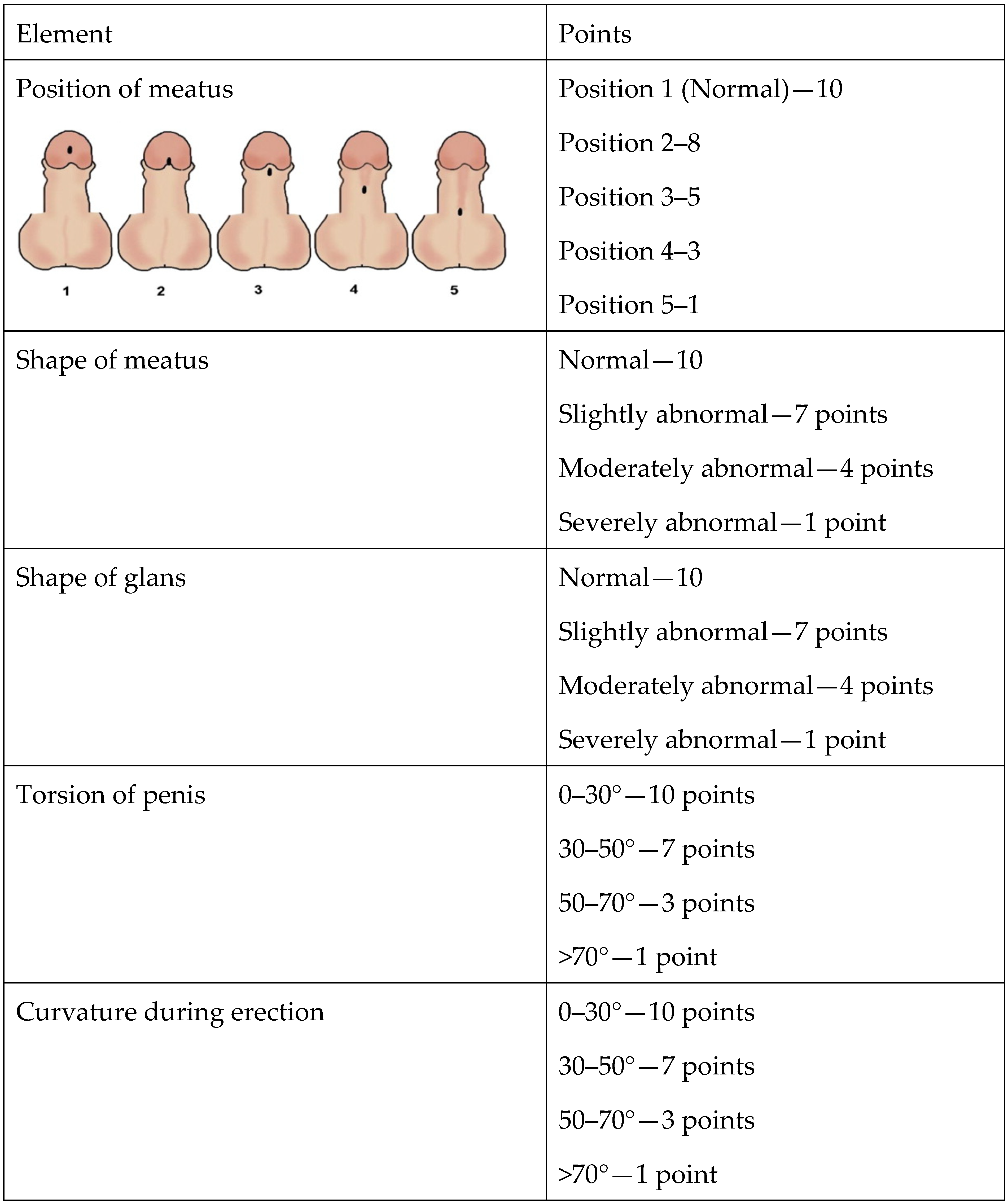
| HOPE | Hypospadias Objective Penile Evaluation |
| PDS | Polydioxanone suture |
| ROC | Receiver Operating Characteristic |
| OR | Odds ratio |
| UC | Urethroplasty complications |
References
- Elliott, C.S.; Halpern, M.S.; Paik, J.; Maldonado, Y.; Shortliffe, L.D. Epidemiologic trends in penile anomalies and hypospadias in the state of California, 1985–2006. J. Pediatr. Urol. 2011, 7, 294–298. [Google Scholar] [CrossRef]
- Springer, A.; van den Heijkant, M.; Baumann, S. Worldwide prevalence of hypospadias. J. Pediatr. Urol. 2016, 12, 152.e1–152.e7. [Google Scholar] [CrossRef]
- Pfistermuller, K.L.M.; McArdle, A.J.; Cuckow, P.M. Meta-analysis of complication rates of the tubularized incised plate (TIP) repair. J. Pediatr. Urol. 2015, 11, 54–59. [Google Scholar] [CrossRef]
- Snodgrass, W.; Cost, N.; Nakonezny, P.A.; Bush, N. Analysis of risk factors for glans dehiscence after tubularized incised plate hypospadias repair. J. Urol. 2011, 185, 1845–1849. [Google Scholar] [CrossRef] [PubMed]
- Leunbach, T.L.; O’Toole, S.; Springer, A.; Williamson, P.R.; Ahmed, S.F. A Systematic Review of Core Outcomes for Hypospadias Surgery. Sex. Dev. 2019, 13, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Spinoit, A.-F.; Poelaert, F.; Van Praet, C.; Groen, L.-A.; Van Laecke, E.; Hoebeke, P. Grade of hypospadias is the only factor predicting for re-intervention after primary hypospadias repair: A multivariate analysis from a cohort of 474 patients. J. Pediatr. Urol. 2015, 11, 70.e1–70.e6. [Google Scholar] [CrossRef] [PubMed]
- Van der Toorn, F.; de Jong, T.P.V.M.; de Gier, R.P.E.; Callewaert, P.R.H.; van der Horst, E.H.J.R.; Steffens, M.G.; Hoebeke, P.; Nijman, R.J.M.; Bush, N.C.; Wolffenbuttel, K.P.; et al. Introducing the HOPE (Hypospadias Objective Penile Evaluation)-score: A validation study of an objective scoring system for evaluating cosmetic appearance in hypospadias patients. J. Pediatr. Urol. 2013, 9, 1006–1016. [Google Scholar] [CrossRef]
- Arlen, A.M.; Kirsch, A.J.; Leong, T.; Broecker, B.H.; Smith, E.A.; Elmore, J.M. Further analysis of the Glans-Urethral Meatus-Shaft (GMS) hypospadias score: Correlation with postoperative complications. J. Pediatr. Urol. 2015, 11, 71.e1–71.e5. [Google Scholar] [CrossRef] [PubMed]
- Merriman, L.S.; Arlen, A.M.; Broecker, B.H.; Smith, E.A.; Kirsch, A.J.; Elmore, J.M. The GMS hypospadias score: Assessment of inter-observer reliability and correlation with post-operative complications. J. Pediatr. Urol. 2013, 9, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, M.; Chaudhary, G.; Rastogi, A.; Kansal, S.; Kumar, D.; Chaudhary, H. Correlation of gms scoring system of hypospadias with post-operative complications correlation of glans-urethral meatus-shaft scoring system of hypospadias with post-operative complications. J. Surg. Sci. 2021, 8, 117–121. [Google Scholar]
- Babu, R.; Chandrasekharam, V.V.S. A meta-analysis comparing dorsal plication and ventral lengthening for chordee correction during primary proximal hypospadias repair. Pediatr. Surg. Int. 2022, 38, 389–398. [Google Scholar] [CrossRef]
- Moscardi, P.R.M.; Gosalbez, R.; Castellan, M.A. Management of High-Grade Penile Curvature Associated with Hypospadias in Children. Front. Pediatr. 2017, 5, 189. [Google Scholar] [CrossRef]
- Keays, M.A.; Dave, S. Current hypospadias management: Diagnosis, surgical management, and long-term patient-centred outcomes. CUAJ 2017, 11, 48. [Google Scholar] [CrossRef]
- Snodgrass, W. Tubularized, incised plate urethroplasty for distal hypospadias. J. Urol. 1994, 151, 464–465. [Google Scholar] [CrossRef]
- Rowe, C.K.; Jamdee, T.; Foster, C.; Burke, K.A. Do the materials matter? A review of the literature and analysis of the materials properties of urethral stents for hypospadias repair. J. Pediatr. Urol. 2022, 18, 160–167. [Google Scholar] [CrossRef]
- Gong, E.M.; Cheng, E.Y. Current challenges with proximal hypospadias: We have a long way to go. J. Pediatr. Urol. 2017, 13, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Castagnetti, M.; Scarpa, M.-G.; Musi, L.; Rigamonti, W. Evaluation of cosmetic results in uncomplicated distal hypospadias repairs. J. Androlog. Sci. 2009, 16, 121–124. [Google Scholar]
- Baskin, L. Hypospadias: A critical analysis of cosmetic outcomes using photography. BJU Int. 2001, 87, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.J.; Smith, G.H.; Ross, F.I.; Cass, D.T. HOSE: An objective scoring system for evaluating the results of hypospadias surgery. BJU Int. 2001, 88, 255–258. [Google Scholar] [CrossRef]
- Weber, D.M.; Landolt, M.A.; Gobet, R.; Kalisch, M.; Greeff, N.K. The Penile Perception Score: An instrument enabling evaluation by surgeons and patient self-assessment after hypospadias repair. J. Urol. 2013, 189, 189–193. [Google Scholar] [CrossRef]
- Patil, J.D.; Mohamed, Y.M.; Farhan, A.; Corbally, M. Outcomes Assessment of Hypospadias Repair. Cureus 2023, 15, e48808. [Google Scholar] [CrossRef] [PubMed]
- Haid, B.; Becker, T.; Koen, M.; Berger, C.; Strasser, C.; Roesch, J.; Zniva, C.; Oswald, J. Penile Appearance After Hypospadias Correction from a Parent’s Point of View: Comparison of the Hypospadias Objective Penile Evaluation Score and Parents Penile Perception Score. J. Pediatr. Urol. 2016, 12, 33.e1–33.e7. [Google Scholar] [CrossRef] [PubMed]
- Duckett, J.W. Hypospadias. Pediatr Rev 1989, 11, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Springer, A. Assessment of outcome in hypospadias surgery—A review. Front. Pediatr. 2014, 2, 2. [Google Scholar] [CrossRef] [PubMed]
- Naumeri, F.; Munir, M.A.; Ahmad, H.M.; Sharif, M.; Awan, N.U.; Butt, G. Comparison of Urethrocutaneous Fistula Rate After Single Dartos and Double Dartos Tubularized Incised Plate Urethroplasty in Pediatric Hypospadias. Cureus 2021, 13, e13378. [Google Scholar] [CrossRef] [PubMed]
- Yiğiter, M.; Yildiz, A.; Oral, A.; Salman, A.B. A comparative study to evaluate the effect of double dartos flaps in primary hypospadias repair: No fistula anymore. Int. Urol. Nephrol. 2010, 42, 985–990. [Google Scholar] [CrossRef] [PubMed]
- van der Horst, H.J.R.; de Wall, L.L. Hypospadias, all there is to know. Eur. J. Pediatr. 2017, 176, 435–441. [Google Scholar] [CrossRef]
- Rynja, S.P.; de Jong, T.P.V.M.; Bosch, J.L.H.R.; de Kort, L.M.O. Functional, cosmetic and psychosexual results in adult men who underwent hypospadias correction in childhood. J. Pediatr. Urol. 2011, 7, 504–515. [Google Scholar] [CrossRef]
- Wirmer, J.; Fawzy, M.; Sennert, M.; Hadidi, A.T. Should we correct hypospadias during childhood? Decision Regret And QUality of Life Assessment (DRAQULA) study. J. Pediatr. Urol. 2023, in press. [Google Scholar] [CrossRef]
- Spinoit, A.-F.; Poelaert, F.; Groen, L.-A.; Van Laecke, E.; Hoebeke, P. Hypospadias repair at a tertiary care center: Long-term followup is mandatory to determine the real complication rate. J. Urol. 2013, 189, 2276–2281. [Google Scholar] [CrossRef]
- Luchtenberg, M.L.; Maeckelberghe, E.L.M.; Locock, L.; Verhagen, A.A.E. Understanding the child-doctor relationship in research participation: A qualitative study. BMC Pediatr. 2020, 20, 353. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, U.; Nilakantan, A.; Bajpai, R.; Addya, K. Comprehensive assessment in cosmetic rhinoplasty: The use of the Derriford Appearance Scale for evaluation of patients. Med. J. Armed Forces India 2019, 75, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Rosa, F.; Lohuis, P.J.F.M.; Almeida, J.; Santos, M.; Oliveira, J.; Sousa, C.A.E.; Ferreira, M. The Portuguese version of “The Utrecht questionnaire for outcome assessment in aesthetic rhinoplasty”: Validation and clinical application. Braz. J. Otorhinolaryngol. 2019, 85, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Ghilli, M.; Mariniello, M.D.; Ferrè, F.; Morganti, R.; Perre, E.; Novaro, R.; Colizzi, L.; Camilleri, V.; Baldetti, G.; Rossetti, E.; et al. Quality of life and satisfaction of patients after oncoplastic or traditional breast-conserving surgery using the BREAST-Q (BCT module): A prospective study. Breast Cancer 2023, 30, 802–809. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | HOPE ≥ 57 | HOPE < 57 | p-Value |
|---|---|---|---|
| n = 102 (81%) | n = 24 (19%) | ||
| Birth weight (g) | 3125 ± 613 | 3125 ± 716 | 0.99 |
| Week of birth | 38 ± 2.2 | 38 ± 1.8 | 0.63 |
| Circumcised (%) | 38 (37) | 10 (40) | 0.94 |
| Meatal location (%) | 0.013 | ||
| Subcoronal | 74 (73) | 13 (54) | |
| Shaft | 26 (25) | 6 (25) | |
| Proximal | 2 (2) | 5 (21) | |
| Chordee (%) | <0.001 | ||
| Mild | 68 (67) | 5 (20) | |
| Moderate | 28 (27) | 14(60) | |
| Severe | 6 (6) | 5 (20) | |
| Degree of Chordee (°) | 10 (0–30) | 40 (30–50) | <0.001 |
| Glans width (mm) | 13.8 ± 1.5 | 12.7 ± 1.1 | 0.003 |
| Preoperative HOPE score | 47 ± 4.8 | 41 ± 5 | <0.001 |
| GMS score | 6 ± 1.8 | 8 ± 2.1 | <0.001 |
| GMS score severity, n (%) | <0.001 | ||
| 1 | 66 (65) | 5 (21) | |
| 2 | 32 (31) | 13 (54) | |
| 3 | 4 (4) | 6 (25) | |
| Penile straightening procedure, n (%) | 50 (51) | 17 (71) | <0.001 |
| Boys requiring ancillary procedure secondary to UC, n (%) | 10 (10) | 11 (46) | <0.001 |
| Overall number of operations | 1 (1–2) | 2 (1–3) | <0.001 |
| Days with stent | 7.3 ± 2.1 | 7.6 ± 2.3 | 0.52 |
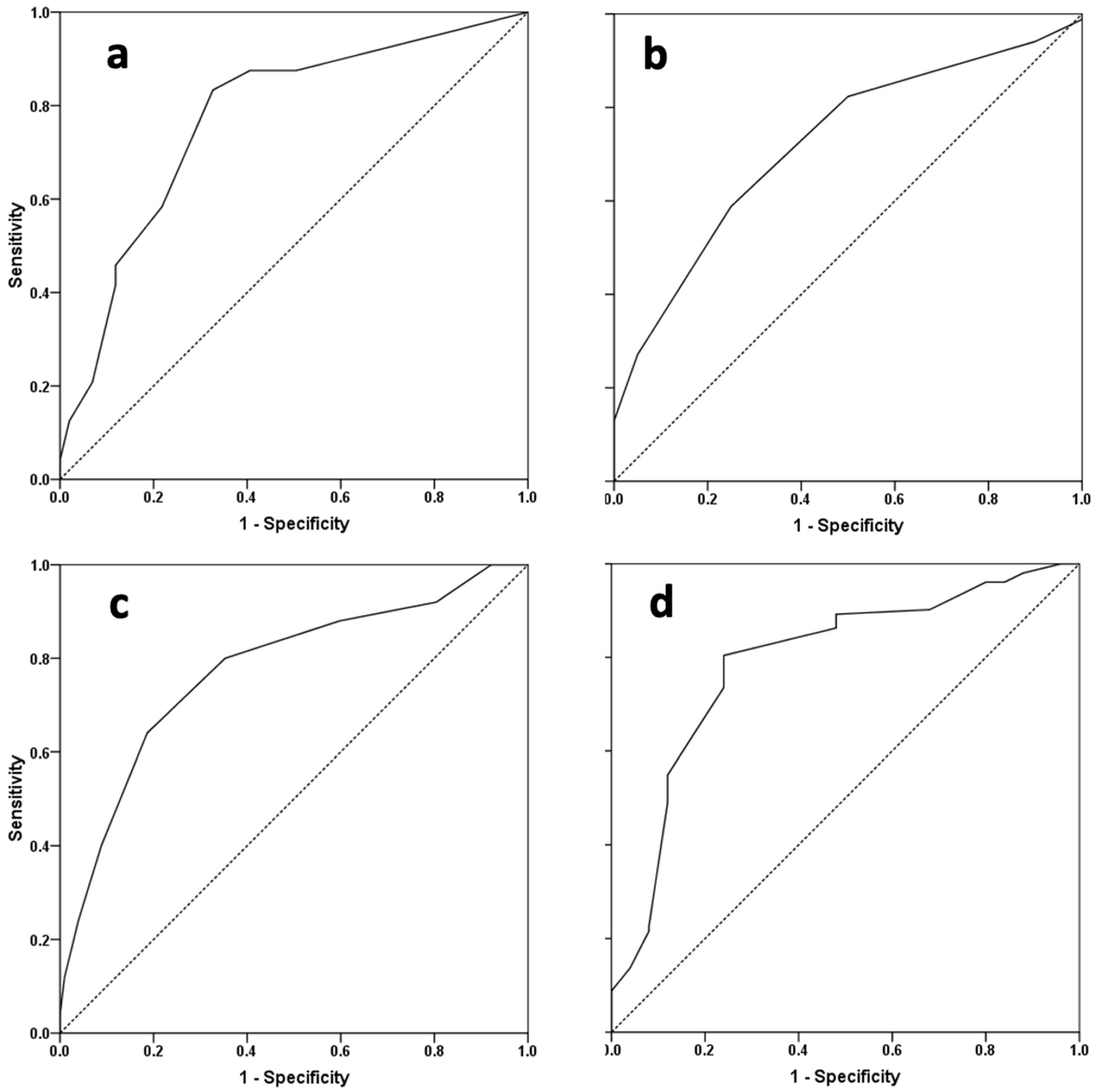
| Variable | AUC | OR (95% CI) | p-Value | Cutoff | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|
| Chordee degree | 0.77 | 0.67–0.87 | <0.001 | 25° | 83 | 67 |
| Glans width | 0.72 | 0.60–0.84 | 0.002 | 12.5 mm | 82 | 50 |
| GMS score | 0.78 | 0.67–0.88 | <0.001 | 7 | 80 | 65 |
| Preoperative HOPE score | 0.79 | 0.69–0.89 | <0.001 | 45 | 76 | 76 |
| Variable | Univariate | Multivariate * | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Chordee degree | 1.05 (1.02–1.07) | <0.001 | 1.04 (1.01–1.07) | 0.013 |
| Chordee degree ≥ 25° | 10.3 (3.26–32.6) | <0.001 | 7.30 (1.74–30.56) | 0.007 |
| Glans width | 0.55 (0.37–0.83) | 0.005 | 0.52 (0.34–0.80) | 0.003 |
| Glans width ≥ 12.5 mm | 0.21 (0.08–0.61) | 0.005 | 0.20 (0.07–0.63) | 0.005 |
| Meatal location | ||||
| Subcoronal | Ref. | - | Ref. | - |
| Shaft | 1.53 (0.55–4.26) | 0.4 | 1.18 (0.38–3.63) | 0.77 |
| Proximal | 14.2 (2.5–81.2) | 0.005 | 7.54 (0.43–130.86) | 0.17 |
| GMS score | 1.75 (1.24–2.29) | <0.001 | 1.66 (1.15–2.38) | 0.007 |
| GMS score ≥ 7 | 7.3 (2.53–21.1) | <0.001 | 4.31 (1.31–14.23) | 0.017 |
| Preoperative HOPE score | 0.80 (0.73–0.89) | <0.001 | 0.82 (0.73–0.93) | 0.002 |
| Preoperative HOPE score ≥ 45 | 0.1 (0.04–0.28) | <0.001 | 0.15 (0.05–0.49) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neheman, A.; Schwarztuch Gildor, O.; Shumaker, A.; Beberashvili, I.; Bar-Yosef, Y.; Arnon, S.; Zisman, A.; Stav, K. Use of Validated Questionnaires to Predict Cosmetic Outcomes of Hypospadias Repair. Children 2024, 11, 189. https://doi.org/10.3390/children11020189
Neheman A, Schwarztuch Gildor O, Shumaker A, Beberashvili I, Bar-Yosef Y, Arnon S, Zisman A, Stav K. Use of Validated Questionnaires to Predict Cosmetic Outcomes of Hypospadias Repair. Children. 2024; 11(2):189. https://doi.org/10.3390/children11020189
Chicago/Turabian StyleNeheman, Amos, Omri Schwarztuch Gildor, Andrew Shumaker, Ilia Beberashvili, Yuval Bar-Yosef, Shmuel Arnon, Amnon Zisman, and Kobi Stav. 2024. "Use of Validated Questionnaires to Predict Cosmetic Outcomes of Hypospadias Repair" Children 11, no. 2: 189. https://doi.org/10.3390/children11020189
APA StyleNeheman, A., Schwarztuch Gildor, O., Shumaker, A., Beberashvili, I., Bar-Yosef, Y., Arnon, S., Zisman, A., & Stav, K. (2024). Use of Validated Questionnaires to Predict Cosmetic Outcomes of Hypospadias Repair. Children, 11(2), 189. https://doi.org/10.3390/children11020189