
Use of Suctioning during Newborn Resuscitation and Its Effects on Heart Rate in a Low-Resource Setting, Tanzania

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
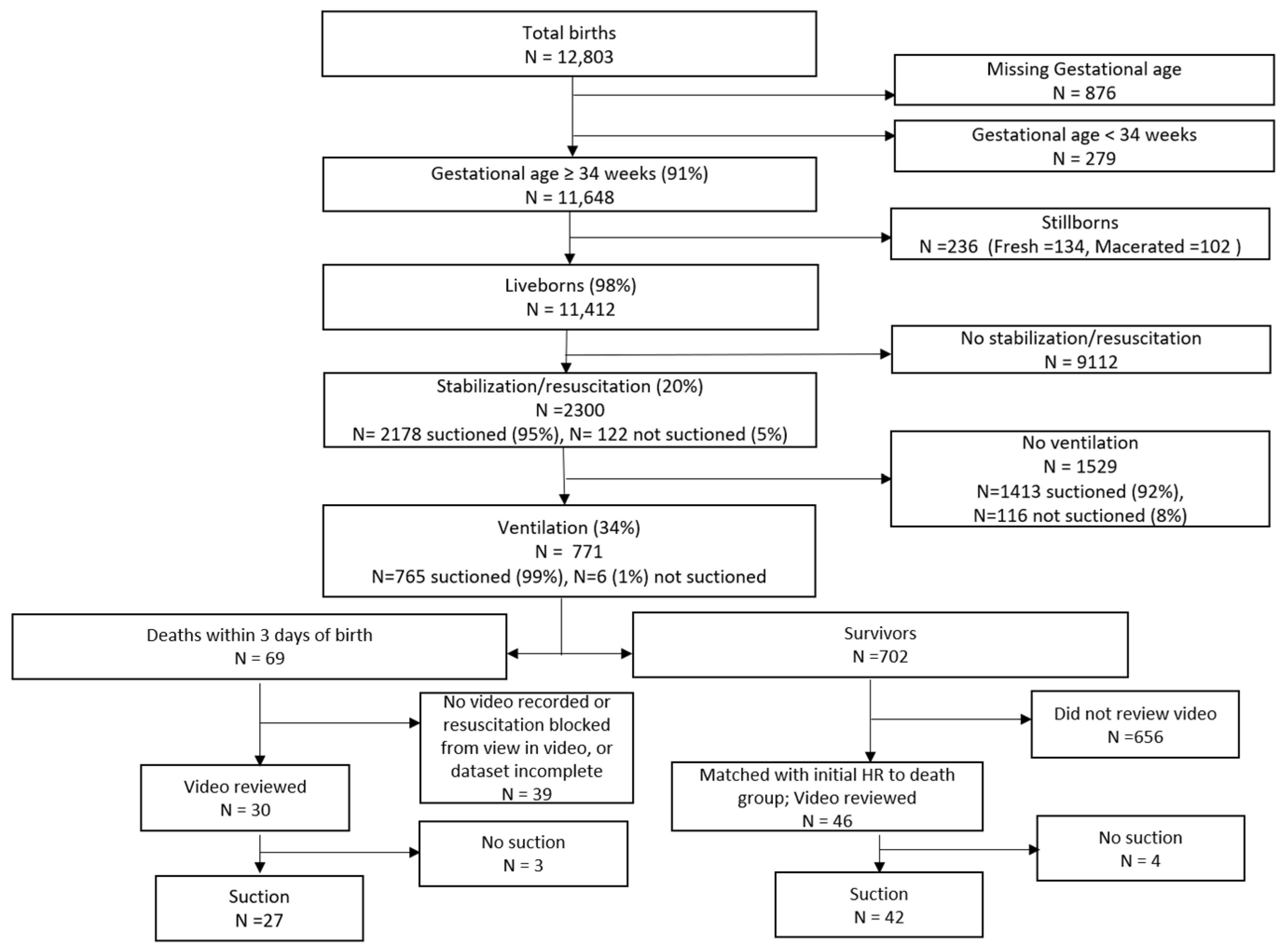
2.2. Subjects
2.3. Development of the Annotation Protocol
2.4. Video Annotations
2.5. Suction Annotations
2.6. Heart Rate and Ventilation Extraction
2.7. Statistical Analyses
3. Results
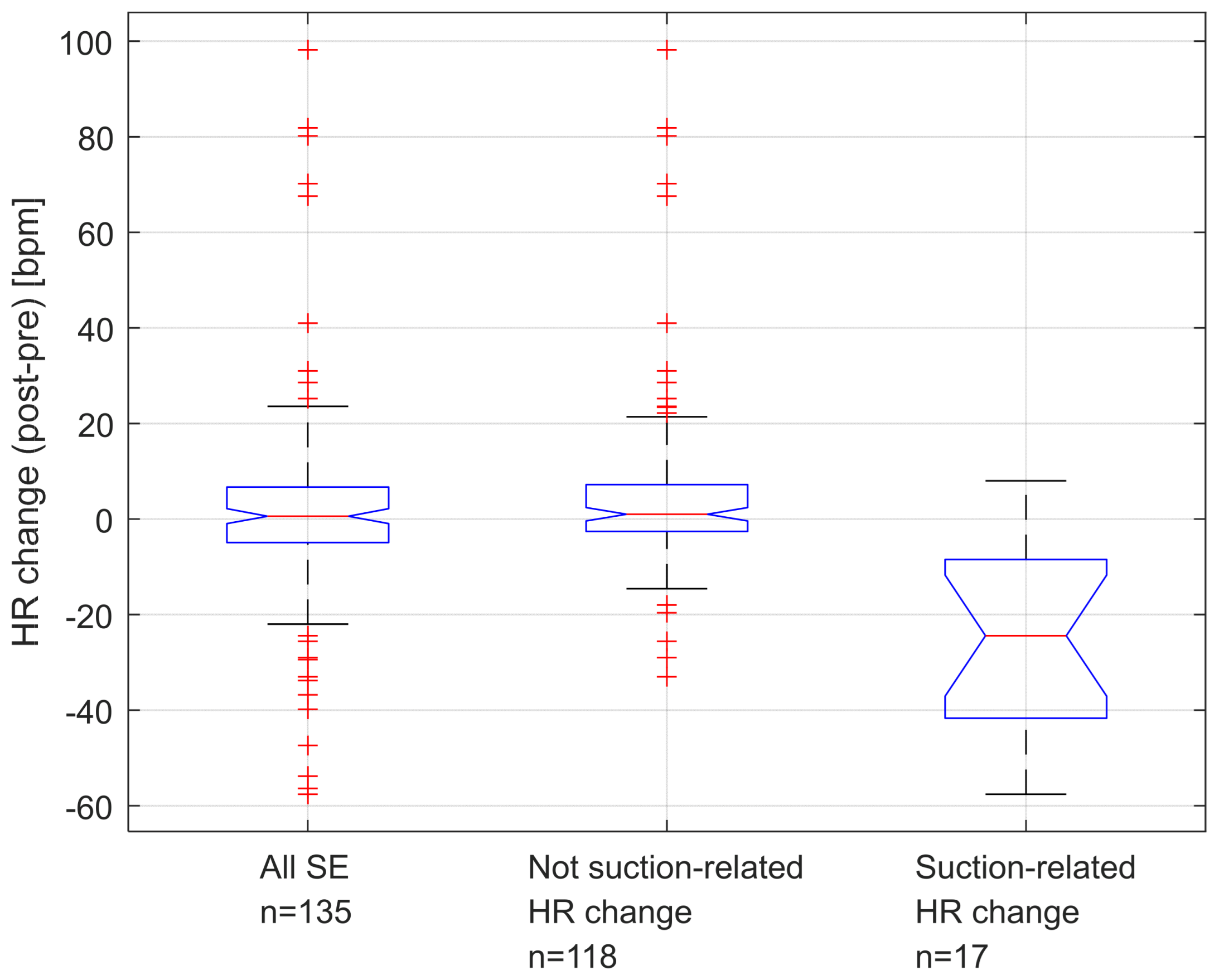
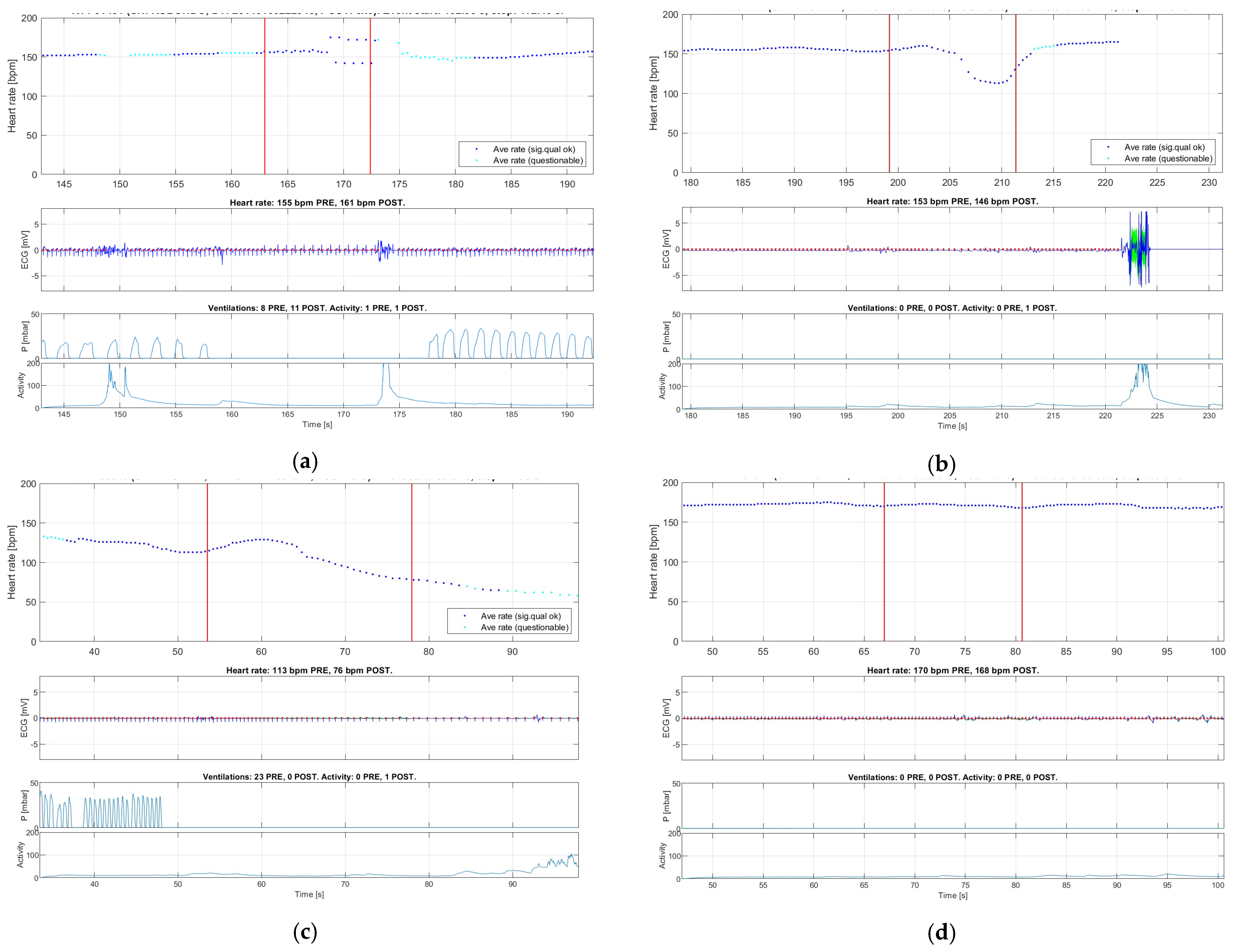
3.1. Suction Events and Heart Rate Changes
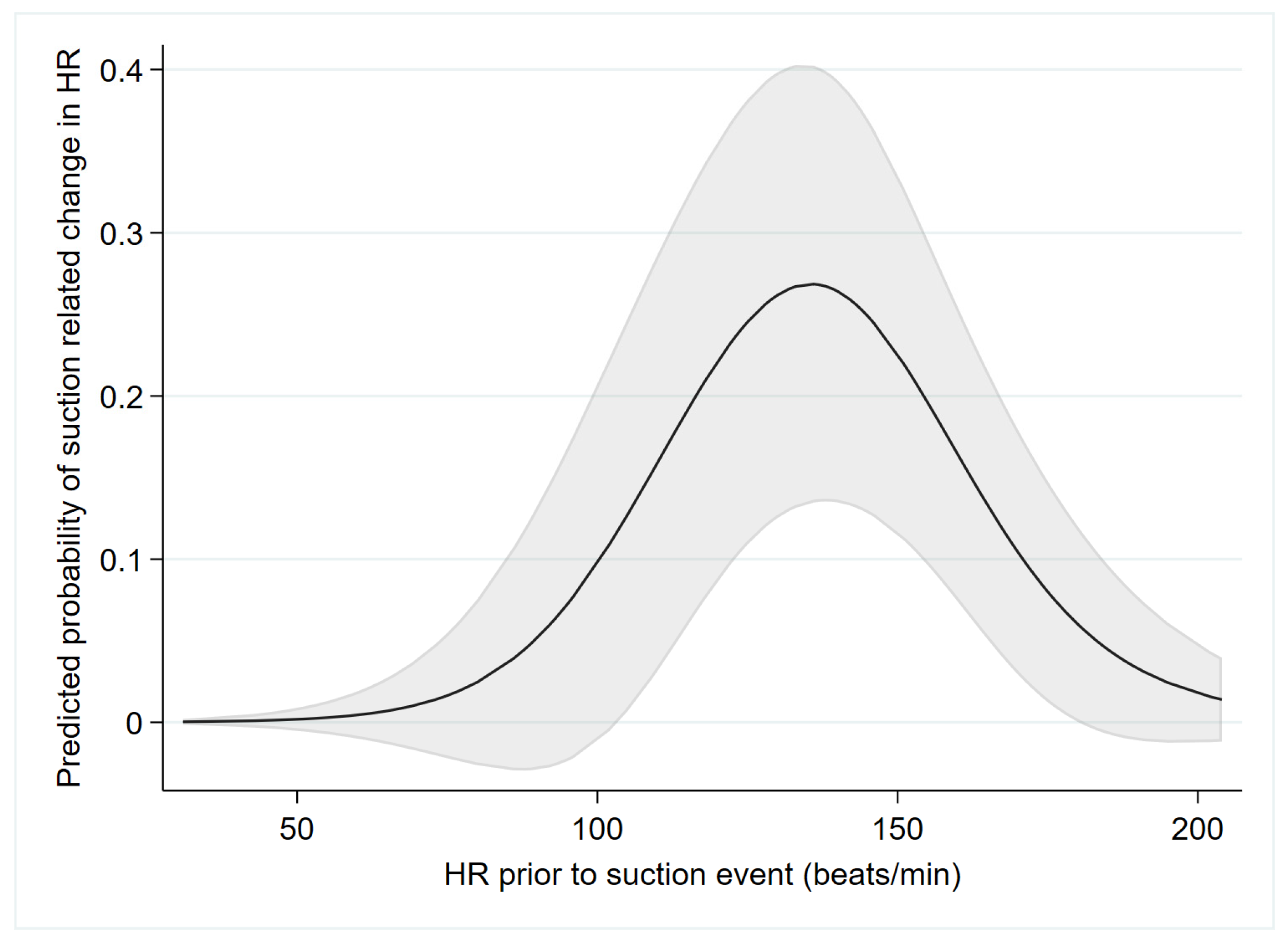
3.2. Probability of Suction-Related HR Changes in Relation to Newborn Characteristics and Other Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skåre, C.; Kramer-Johansen, J.; Steen, T.; Ødegaard, S.; Niles, D.E.; Nakstad, B.; Solevåg, A.L.; Nadkarni, V.M.; Olasveengen, T.M. Incidence of Newborn Stabilization and Resuscitation Measures and Guideline Compliance during the First Minutes of Life in Norway. Neonatology 2015, 108, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Ersdal, H.L.; Mduma, E.; Svensen, E.; Perlman, J.M. Early initiation of basic resuscitation interventions including face mask ventilation may reduce birth asphyxia related mortality in low-income countries. Resuscitation 2012, 83, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Modarresnejad, V. Oronasopharyngeal Suction Versus No Suction in Normal and Term Infants Delivered Vaginally in Afzalipoor Hospital, 2008: A Prospective Randomized Controlled Trial. Pediatr. Res. 2011, 70, 106. [Google Scholar]
- McCartney, P.R. Bulb syringes in newborn care. MCN Am. J. Matern./Child Nurs. 2000, 25, 217. [Google Scholar] [CrossRef]
- Gungor, S.; Kurt, E.; Teksoz, E.; Goktolga, U.; Ceyhan, T.; Baser, I. Oronasopharyngeal Suction versus No Suction in Normal and Term Infants Delivered by Elective Cesarean Section: A Prospective Randomized Controlled Trial. Gynecol. Obstet. Investig. 2006, 61, 9–14. [Google Scholar] [CrossRef]
- Gungor, S.; Teksoz, E.; Ceyhan, T.; Kurt, E.; Goktolga, U.; Baser, I. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: A prospective randomized controlled trial. Aust. N. Z. J. Obstet. Gynaecol. 2005, 45, 453–456. [Google Scholar]
- Carrasco, M.; Martell, M.; Estol, P.C. Oronasopharyngeal suction at birth: Effects on arterial oxygen saturation. J. Pediatr. 1997, 130, 832–834. [Google Scholar] [CrossRef]
- Linde, J.; Schulz, J.; Perlman, J.; Øymar, K.; Blacy, L.; Kidanto, H.; Ersdal, H. The relation between given volume and heart rate during newborn resuscitation. Resuscitation 2017, 117, 80–86. [Google Scholar] [CrossRef]
- Patterson, J.K.; Ishoso, D.; Eilevstjønn, J.; Bauserman, M.; Haug, I.; Iyer, P.; Kamath-Rayne, B.D.; Lokangaka, A.; Lowman, C.; Mafuta, E.; et al. Delayed and Interrupted Ventilation with Excess Suctioning after Helping Babies Breathe with Congolese Birth Attendants. Children 2023, 10, 652. [Google Scholar] [CrossRef]
- Linde, J.; Perlman, J.; Øymar, K.; Schulz, J.; Eilevstjønn, J.; Thallinger, M.; Kusulla, S.; Kidanto, H.; Ersdal, H. Predictors of 24-h outcome in newborns in need of positive pressure ventilation at birth. Resuscitation 2018, 129, 1–5. [Google Scholar] [CrossRef]
- Kattwinkel, J. (Ed.) Lesson 2. In Textbook of Neonatal Resuscitation, 6th ed.; American Academy of Pediatrics and American Heart Association: Elk Grove Village, IL, USA, 2011; pp. 37–69. [Google Scholar]
- Guidelines on Basic Newborn Resuscitation. World Health Organization. 2012. Available online: https://apps.who.int/iris/handle/10665/75157/ (accessed on 1 May 2023).
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; De Almeida, M.F.; Fabres, J.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020, 142, S185–S221. [Google Scholar] [CrossRef]
- Fawke, J.; Wyllie, J.; Udaeta, E.; Rüdiger, M.; Ersdal, H.; Wright, M.-D.; Wyckoff, M.H.; Liley, H.G.; Rabi, Y.; Weiner, G.M.; et al. Suctioning of clear amniotic fluid at birth: A systematic review. Resusc. Plus 2022, 12, 100298. [Google Scholar] [CrossRef]
- Msemo, G.; Massawe, A.; Mmbando, D.; Rusibamayila, N.; Manji, K.; Kidanto, H.L.; Mwizamuholya, D.; Ringia, P.; Ersdal, H.L.; Perlman, J. Newborn Mortality and Fresh Stillbirth Rates in Tanzania After Helping Babies Breathe Training. Pediatrics 2013, 131, e353–e360. [Google Scholar] [CrossRef]
- Helping Babies Breathe [Internet]. American Academy of Pediatrics. Available online: https://www.aap.org/en/aap-global/helping-babies-survive/our-programs/helping-babies-breathe/helping-babies-breathe-2nd-edition/ (accessed on 1 May 2023).
- Lindbäck, C.; Kc, A.; Wrammert, J.; Vitrakoti, R.; Ewald, U.; Målqvist, M. Poor adherence to neonatal resuscitation guidelines exposed; an observational study using camera surveillance at a tertiary hospital in Nepal. BMC Pediatr. 2014, 14, 233. [Google Scholar] [CrossRef]
- Sobel, H.L.; Silvestre, M.A.A.; Iii, J.B.V.M.; Oliveros, Y.E.; Nyunt-U, S. Immediate newborn care practices delay thermoregulation and breastfeeding initiation. Acta Paediatr. 2011, 100, 1127–1133. [Google Scholar] [CrossRef]
- Skåre, C.; Boldingh, A.-M.; Nakstad, B.; Calisch, T.E.; Niles, D.E.; Nadkarni, V.M.; Kramer-Johansen, J.; Olasveengen, T.M. Ventilation fraction during the first 30 s of neonatal resuscitation. Resuscitation 2016, 107, 25–30. [Google Scholar] [CrossRef]
- Research and Development to Save Newborn Lives [Internet]. Safer Births. Available online: http://www.saferbirths.com/ (accessed on 1 May 2023).
- Boo, N.; Suhaida, A.; Rohana, J. Frequent nasopharyngeal suctioning as a risk factor associated with neonatal coagulase-negative staphylococcal colonisation and sepsis. Singap. Med. J. 2015, 56, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Volpe, J.J. Suctioning in the Preterm Infant: Effects on Cerebral Blood Flow Velocity, Intracranial Pressure, and Arterial Blood Pressure. Pediatrics 1983, 72, 329–334. [Google Scholar] [CrossRef]
- Foster, J.P.; Dawson, J.A.; Davis, P.G.; Dahlen, H.G. Routine oro/nasopharyngeal suction versus no suction at birth. Cochrane Database Syst. Rev. 2017, 2017, CD010332. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, J.; Bhat, R.; Salas, A.A.; Addis, D.; Mills, E.C.; Mallick, H.; Tripathi, A.; Pruitt, E.P.; Roane, C.; McNair, T.; et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: A randomised equivalency trial. Lancet 2013, 382, 326–330. [Google Scholar] [CrossRef]
- Bancalari, A.; Díaz, V.; Araneda, H. Effects of pharyngeal suction on the arterial oxygen saturation and heart rate in healthy newborns delivered by elective cesarean section. J. Neonatal-Perinatal Med. 2019, 12, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Cordero, L.; Hon, E.H. Neonatal bradycardia following nasopharyngeal stimulation. J. Pediatr. 1971, 78, 441–447. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total n = 76 | Deaths n = 30 | Survivors n = 46 | p 1 | p 2 |
|---|---|---|---|---|---|
| Birth weight (grams) | 3060 ± 560 | 2841 ± 491 | 3203 ± 561 | 0.004 | 0.009 |
| Gestational age (weeks) | 38.1 ± 1.6 n = 72 | 37.9 ± 1.4 n = 27 | 38.2 ± 1.6 n = 45 | 0.35 | 0.47 |
| Female | 26 (34%) | 13 (43%) | 13 (28%) | 0.18 | 0.26 |
| Abnormal FHR on admission | 2 (3%) n = 66 | 1 (4%) n = 24 | 1 (2%) n = 42 | 0.69 | 0.56 |
| Cervical dilatation on admission (cm) | 6.3 ± 2.4 n = 64 | 6.2 ± 2.6 n = 22 | 6.4 ± 2.3 n = 42 | 0.84 | 0.96 |
| Fetal presentation | 0.60 | 0.49 | |||
| Cephalic | 67 (88%) | 26 (87%) | 41 (89%) | ||
| Breech | 6 (8%) | 2 (7%) | 4 (9%) | ||
| Others (transverse, prolapse) | 3 (4%) | 2 (7%) | 1 (2%) | ||
| Abnormal FHR during labor | 9 (15%) n = 62 | 7 (30%) n = 23 | 2 (5%) n = 39 | 0.007 | 0.010 |
| Amniotic fluid 5 | (n = 75) | (n = 45) | 0.22 | 0.37 | |
| Clear | 39 (52%) | 12 (40%) | 27 (60%) | ||
| Slight meconium | 11 (15%) | 6 (20%) | 5 (11%) | ||
| Thick meconium | 24 (32%) | 12 (40%) | 12 (27%) | ||
| Blood stained | 1 (1%) | 0 (0%) | 1 (2%) | ||
| Abnormal final FHR before delivery | 9 (14%) n = 64 | 7 (29%) n = 24 | 2 (5%) n = 40 | 0.008 | 0.010 |
| Multiples (twins) | 3 (4%) | 1 (3%) | 2 (4%) | 0.82 | 0.60 |
| Labor complications 6 | 6 (8%) | 2 (7%) | 4 (9%) | 0.75 | 0.93 |
| Mode of delivery | 0.53 | 0.85 | |||
| Spontaneous vaginal delivery | 41 (54%) | 14 (47%) | 27 (59%) | ||
| Cesarean section | 32 (42%) | 15 (50%) | 17 (37%) | ||
| Assisted breech delivery | 3 (4%) | 1 (3%) | 2 (4%) | ||
| Apgar score assigned by attending midwife | |||||
| 1 min | 7 (4, 7) | 4 (3, 5) | 7 (7, 8) | <0.001 3 | <0.001 3 |
| 5 min | 10 (8, 10) | 9 (6, 10) | 10 (10, 10) | <0.001 3 | <0.001 3 |
| First newborn HR (bpm) | 77 (55, 139) | 66 (52, 94) | 94 (59, 154) | 0.098 4 |
| Characteristics | Total n = 76 | Deaths n = 30 | Survivors n = 46 | p 1 | p 2 |
|---|---|---|---|---|---|
| General | |||||
| Duration of resuscitation | 388 (223, 602) | 609 (336, 1218) | 288 (182, 438) | 0.003 3 | 0.013 3 |
| Time from birth to cord clamping (sec) | 33 (15, 57) n = 74 | 19 (14, 50) n = 29 | 35 (12, 58) n = 45 | 0.10 3 | 0.69 3 |
| Time from birth to placement of ECG sensor (sec) | 107 (71, 142) n = 72 | 115 (71, 131) n = 28 | 103 (71, 166) n = 44 | 0.50 3 | 0.42 3 |
| Time from birth to start ventilation (sec) | 108 (76, 158) n = 74 | 125 (81, 146) n = 29 | 104 (73, 176) n = 45 | 0.32 3 | 0.63 3 |
| Duration from first to final ventilation (sec) | 174 (104, 344) n = 72 | 557 (208, 700) n = 28 | 122 (77, 192) n = 44 | <0.001 3 | <0.001 3 |
| HR at start of first ventilation (bpm) | 82 (61, 133) n = 58 | 61 (54, 79) n = 22 | 121 (69, 160) n = 36 | 0.002 3 | 0.81 3 |
| HR at cessation of ventilation (bpm) | 150 (129, 167) n = 70 | 142 (123, 155) n = 25 | 156 (140, 171) n = 45 | 0.096 3 | 0.31 3 |
| HR increase from first to final ventilation (bpm) | 27 (2, 82) n = 52 | 63 (9, 92) n = 17 | 25 (1, 74) n = 35 | 0.085 3 | 0.40 3 |
| Ventilation Parameters | |||||
| Inflated volume (ml) 4 | 39 (25, 49) | 36 (25, 46) | 41 (25, 51) | 0.48 3 | 0.47 3 |
| Mask leakage (%) 4 | 50 ± 21 | 47 ± 22 | 52 ± 20 | 0.39 | 0.50 |
| Expired volume (ml) 4 | 14 (8, 25) | 16 (7, 25) | 13 (8, 26) | 0.35 3 | 0.37 3 |
| Expired volume (ml/kg) 4 | 6.2 (3.7, 10.1) | 9.7 (3.8, 11.9) | 4.8 (3.3, 8.2) | 0.001 3 | 0.001 3 |
| Ventilation frequency (per minute) 4 | 52 (41, 68) | 51 (41, 67) | 54 (40, 68) | 0.64 3 | 0.84 3 |
| Peak inflation pressure (mBar) 4 | 34 ± 8 | 33 ± 7 | 34 ± 8 | 0.43 | 0.56 |
| Expired CO2 (%) 4 | 3.2 (1.8, 4.2) | 3.1 (1.3, 3.8) | 3.5 (2.1, 4.4) | 0.57 3 | 0.57 3 |
| Suctioning during Resuscitation | |||||
| Resuscitation period analyzed for suctioning (sec) | 391 (245, 420) | 420 (360, 471) | 312 (213, 416) | ||
| Babies with at least one SE | 69 (91%) | 27 (90%) | 42 (91%) | 0.85 | 0.86 |
| Number of SEs per baby | 2 (1, 4) | 2 (1, 4) | 2 (1, 4) | ||
| Total duration of suctioning (sec) | 32 (15, 64) | 32 (18, 67) | 32 (13, 61) | ||
| Proportion of time spent suctioning (%) | 10 (5, 19) | 10 (4, 17) | 11 (6, 20) | ||
| Infants receiving at least one catheter suction (vs. only bulb suction or no suction) | 17 (22%) | 8 (27%) | 9 (20%) | 0.47 | 0.67 |
| Number of suction insertions per baby | 9 (5, 16) | 9 (6, 15) | 11 (5, 18) | ||
| Number of mouth suction insertions | 6 (3, 9) | 5 (3, 8) | 6 (3, 11) | ||
| Number of nose suction insertions | 4 (2, 7) | 4 (2, 7) | 4 (2, 7) | ||
| Number of suction insertions/SE 5 | 3.6 (3.0, 5.4) n = 68 | 3.4 (2.4, 6.0) n = 26 | 3.9 (3.0, 5.1) n = 42 | ||
| Number of mouth suction/SE | 2.0 (1.5, 3.0) | 1.8 (1.3, 3.1) | 1.3 (1.0, 2.0) | ||
| Number of nose suctions/SE | 1.5 (0.8, 2.1) | 1.6 (0.6, 2.6) | 1.3 (1.0, 2.0) |
| Predictors | Suction-Related Change in HR (n = 17) | No Suction-Related Change in HR (n = 118) | OR 1 (95% CI) | p 2 | pNL 4 |
|---|---|---|---|---|---|
| Categorical | |||||
| Female | 6 (35%) | 26 (22%) | 1.93 (0.51–7.33) | 0.33 | |
| Amniotic fluid | (n = 115) | 0.10 | |||
| Clear | 6 (35%) | 61 (53%) | 1 (ref) | ||
| Slight | 2 (12%) | 14 (12%) | 1.45 (0.26–8.15) | 0.67 | |
| Thick/Blood | 9 (53%) | 40 (35%) | 2.29 (0.69–7.53) | 0.17 | |
| Catheter (vs. bulb) | 3 (18%) | 32 (27%) | 0.58 (0.16–2.02) | 0.39 | |
| Ventilation prior to SE | 8 (47%) | 60 (51%) | 0.86 (0.28–2.66) | 0.79 | |
| Stimulation prior to SE | 13 (76%) | 75 (64%) | 1.86 (0.56–6.16) | 0.31 | |
| Continuous | |||||
| Gestational Age (weeks) | 39 (38, 39) n = 15 | 38 (36, 39) n = 114 | 1.37 (0.98–1.93) | 0.066 | 0.095 |
| Birthweight (g) | 2780 (2530, 3320) | 3100 (2730, 3350) | 0.080 3 | 0.043 | |
| First observed HR (bpm) | 74 (58, 123) | 72 (52, 131) | 0.96 (0.85–1.07) | 0.45 | 0.089 |
| Time post delivery to initiation of SE (sec) | 113 (64, 160) | 103 (54, 183) | 0.12 3 | 0.047 | |
| HR prior to SE (bpm) | 144 (129, 155) | 137 (89, 170) | 0.003 3 | 0.001 | |
| Duration of SE (sec) | 18 (10, 23) | 14 (7, 23) | 1.02 (0.99–1.04) | 0.14 | 0.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Purington, C.; Eilevstjønn, J.; Dalen, I.; Yeconia, A.; Blacy, L.; Mduma, E.; Haug, I.; Holte, K.; Chang, C.; Perlman, J.; et al. Use of Suctioning during Newborn Resuscitation and Its Effects on Heart Rate in a Low-Resource Setting, Tanzania. Children 2023, 10, 1540. https://doi.org/10.3390/children10091540
Purington C, Eilevstjønn J, Dalen I, Yeconia A, Blacy L, Mduma E, Haug I, Holte K, Chang C, Perlman J, et al. Use of Suctioning during Newborn Resuscitation and Its Effects on Heart Rate in a Low-Resource Setting, Tanzania. Children. 2023; 10(9):1540. https://doi.org/10.3390/children10091540
Chicago/Turabian StylePurington, Carolyn, Joar Eilevstjønn, Ingvild Dalen, Anita Yeconia, Ladislaus Blacy, Estomih Mduma, Ingunn Haug, Kari Holte, Catherine Chang, Jeffrey Perlman, and et al. 2023. "Use of Suctioning during Newborn Resuscitation and Its Effects on Heart Rate in a Low-Resource Setting, Tanzania" Children 10, no. 9: 1540. https://doi.org/10.3390/children10091540
APA StylePurington, C., Eilevstjønn, J., Dalen, I., Yeconia, A., Blacy, L., Mduma, E., Haug, I., Holte, K., Chang, C., Perlman, J., & Ersdal, H. (2023). Use of Suctioning during Newborn Resuscitation and Its Effects on Heart Rate in a Low-Resource Setting, Tanzania. Children, 10(9), 1540. https://doi.org/10.3390/children10091540