
Reliability of Agreement between Insulin, Clonidine, and Glucagon Stimulation Tests for the Diagnosis of Growth Hormone Deficiency in Children: A Retrospective Cohort Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
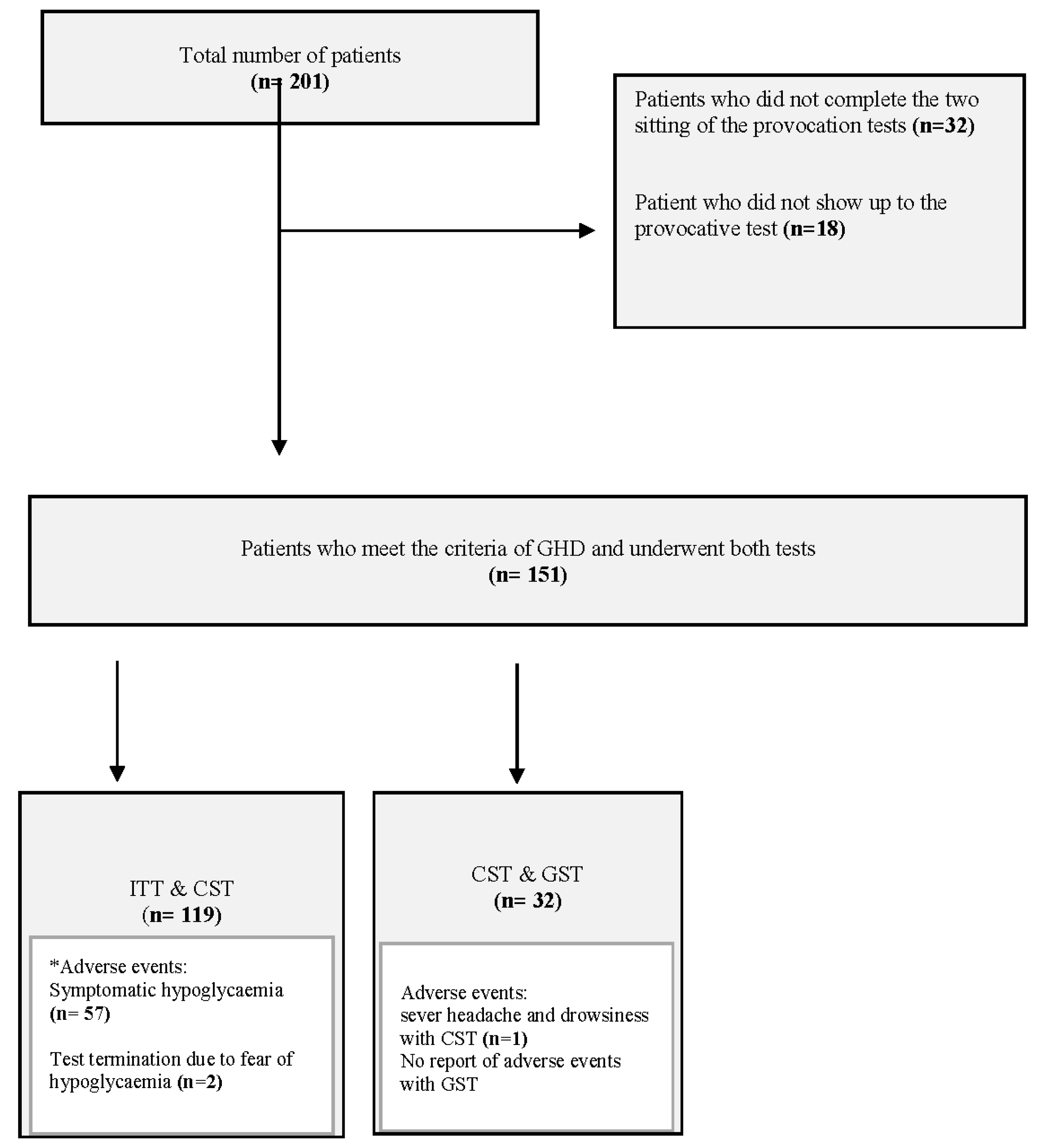
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Inter-Rater Reliability
3.2. Correlation Coefficient
4. Discussion
Strength and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jorge, A.A.L.; Grimberg, A.; Dattani, M.T.; Baro, J. Disorders of childhood growth. In Sperling Pediatric Endocrinology, 5th ed.; Sperling, M., Ed.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 336–337. [Google Scholar]
- Rosenfeld, R.G.; Albertsson-Wikland, K.; Cassorla, F.; Frasier, S.D.; Hasegawa, Y.; Hintz, R.L.; Lafranchi, S.; Lippe, B.; Loriaux, L.; Melmed, S. Diagnostic controversy: The diagnosis of childhood growth hormone deficiency revisited. J. Clin. Endocrinol. Metab. 1995, 80, 1532–1540. [Google Scholar] [CrossRef]
- Wagner, I.V.; Paetzold, C.; Gausche, R.; Vogel, M.; Koerner, A.; Thiery, J.; Arsene, C.G.; Henrion, A.; Guettler, B.; Keller, E.; et al. Clinical evidence-based cutoff limits for GH stimulation tests in children with a backup of results with reference to mass spectrometry. Eur. J. Endocrinol. 2014, 171, 389–397. [Google Scholar] [CrossRef]
- Stanley, T.L.; Levitsky, L.L.; Grinspoon, S.K.; Misra, M. Effect of Body Mass Index on Peak Growth Hormone Response to Provocative Testing in Children with Short Stature. J. Clin. Endocrinol. Metab. 2009, 94, 4875–4881. [Google Scholar] [CrossRef] [PubMed]
- Adan, L.; Souberbielle, J.C.; Brauner, R. Diagnostic markers of permanent idiopathic growth hormone deficiency. J. Clin. Endocrinol. Metab. 1994, 78, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.; Rosenfeld, R.G. Clinical utility of insulin-like growth factor assays. Pediatrician 1987, 14, 154–161. [Google Scholar]
- Audí, L.; Granada, M.L.; Carrascosa, A. Growth hormone secretion assessment in the diagnosis of short stature. J. Pediatr. Endocrinol. Metab. 1996, 9 (Suppl. S3), 313–324. [Google Scholar]
- Rosenfeld, R.G. Is Growth Hormone Deficiency a Viable Diagnosis? J. Clin. Endocrinol. Metab. 1997, 82, 349–351. [Google Scholar] [CrossRef]
- Saggese, G.; Cesaretti, G. Criteria for Recognition of the Growth-Inefficient Child Who May Respond to Treatment with Growth Hormone. Arch. Pediatr. Adolesc. Med. 1989, 143, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Zadik, Z.; Chalew, S.A.; Gilula, Z.; Kowarski, A.A. Reproducibility of Growth Hormone Testing Procedures: A Comparison between 24-hour Integrated Concentration and Pharmacological Stimulation. J. Clin. Endocrinol. Metab. 1990, 71, 1127–1130. [Google Scholar] [CrossRef]
- Ranke, M.B.; Haber, P. Growth hormone stimulation tests. In Functional Endocrinologic Diagnostics in Children and Adolescents; Mannheim, J., Verlag, J., Ranke, M.B., Eds.; Huthig Fachverlage Vertrieb: Mainz, Germany, 1992; pp. 61–75. [Google Scholar]
- Yuen, K.C.J.; Johannsson, G.; Ho, K.K.Y.; Miller, B.S.; Bergada, I.; Rogol, A.D. Diagnosis and testing for growth hormone deficiency across the ages: A global view of the accuracy, caveats, and cut-offs for diagnosis. Endocr. Connect. 2023, 12, e220504. [Google Scholar] [CrossRef]
- Yackobovitch-Gavan, M.; Lazar, L.; Diamant, R.; Phillip, M.; Oron, T. Diagnosis of Growth Hormone Deficiency in Children: The Efficacy of Glucagon versus Clonidine Stimulation Test. Horm. Res. Paediatr. 2020, 93, 470–476. [Google Scholar] [CrossRef]
- Lone, S.W.; Khan, Y.N.; Qamar, F.; Atta, I.; Ibrahim, M.N.; Raza, J. Safety of insulin tolerance test for the assessment of growth hormone deficiency in children. J. Pak. Med. Assoc. 2011, 61, 153. [Google Scholar]
- Ibrahim, M.N.; Noor, N.; Nisa, M.; Leghari, T.M.; Khan, Y.N.; Raza, J. Peak Growth Hormone Level Variability during Insulin Tolerance Test in Children with Short Stature. J. Coll. Physicians Surg. Pak. 2021, 31, 1081–1084. [Google Scholar] [CrossRef] [PubMed]
- Research Society Consensus Guidelines for the Diagnosis and Treatment of Growth Hormone (GH) Deficiency in Childhood and Adolescence: Summary Statement of the GH Research Society. J. Clin. Endocrinol. Metab. 2000, 85, 3990–3993. [CrossRef]
- Collett-Solberg, P.F.; Ambler, G.; Backeljauw, P.F.; Bidlingmaier, M.; Biller, B.M.; Boguszewski, M.C.; Cheung, P.T.; Choong, C.S.Y.; Cohen, L.E.; Cohen, P.; et al. Diagnosis, Genetics, and Therapy of Short Stature in Children: A Growth Hormone Research Society International Perspective. Horm. Res. Paediatr. 2019, 92, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Light, R.J. Measures of response agreement for qualitative data: Some generalizations and alternatives. Psychol. Bull. 1971, 76, 365–377. [Google Scholar] [CrossRef]
- Hallgren, K.A. Computing Inter-Rater Reliability for Observational Data: An Overview and Tutorial. Tutorials Quant. Methods Psychol. 2012, 8, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Myburgh, H.C.; Jose, S.; Swanepoel, D.W.; Laurent, C. Towards low cost automated smartphone- and cloud-based otitis media diagnosis. Biomed. Signal Process. Control. 2018, 39, 34–52. [Google Scholar] [CrossRef]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology; Pearson Education: London, UK, 2007. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Molitch, M.E.; Clemmons, D.R.; Malozowski, S.; Merriam, G.R.; Vance, M.L. Evaluation and Treatment of Adult Growth Hormone Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1587–1609. [Google Scholar] [CrossRef]
- Hoffman, D.; O’Sullivan, A.; Ho, K.; Baxter, R. Diagnosis of growth-hormone deficiency in adults. Lancet 1994, 343, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Weintrob, N.; Sprecher, E.; Josefsberg, Z.; Weininger, C.; Aurbach-Klipper, Y.; Lazard, D.; Karp, M.; Pertzelan, A. Standard and Low-Dose Short Adrenocorticotropin Test Compared with Insulin-Induced Hypoglycemia for Assessment of the Hypothalamic-Pituitary-Adrenal Axis in Children with Idiopathic Multiple Pituitary Hormone Deficiencies. J. Clin. Endocrinol. Metab. 1998, 83, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Hanukoglu, A.; Weisglass, R. Is the fear from insulin tolerance test in the evaluation of short stature justified? Eur. J. Pediatr. 2022, 181, 2867–2871. [Google Scholar] [CrossRef]
- Kaplan, S.L.; Abrams, C.A.L.; Bell, J.J.; Conte, F.A.; Grumbach, M.M. Growth and Growth Hormone: I. changes in Serum Level of Growth Hormone Following Hypoglycemia in 134 children with Growth Rctardation. Pediatr. Res. 1968, 2, 43–63. [Google Scholar] [CrossRef]
- Galloway, P.J.; McNeill, E.; Paterson, W.F.; Donaldson, M.D.C. Safety of the insulin tolerance test. Arch. Dis. Child. 2002, 87, 354–356. [Google Scholar] [CrossRef] [PubMed]
- Gil-Ad, I.; Topper, E.; Laron, Z. Oral Clonidine as a Growth Hormone Stimulation Test. Lancet 1979, 314, 278–280. [Google Scholar] [CrossRef]
- Borges, M.d.F.; Teixeira, F.C.C.; Feltrin, A.K.; Ribeiro, K.A.; Nascentes, G.A.N.; Resende, E.A.M.R.; Ferreira, B.P.; Silva, A.P.; Palhares, H.M.C. Clonidine-stimulated growth hormone concentrations (cut-off values) measured by immunochemiluminescent assay (ICMA) in children and adolescents with short stature. Clinics 2016, 71, 226–231. [Google Scholar] [CrossRef]
- Marui, S.; Oliveira, C.H.M.C.; Souza, S.C.A.L.; Berger, K.; Khawali, C.; Hauache, O.M.; Maciel, R.M.B.; Vieira, J.M.B. Tolerance of oral clonidine test in 180 patients: Efficacy of saline resuscitation in controlling arterial hypotension. Arq. Bras. Endocrinol. Metab. 2015, 49, 510–515. [Google Scholar] [CrossRef]
- May, M.; Rose, S.R. Oral Hydration During Growth Hormone Stimulation with Clonidine. J. Pediatr. Nurs. 2007, 22, 383–387. [Google Scholar] [CrossRef]
- Thakur, D.S.; Bhagwat, N.M.; Bhide, M.M.; Yerawar, C.G.; Ghanekar, G.A.; Sonawane, A.B.; Chadha, M.D.; Varthakavi, P.K. Clonidine Stimulation Test: Is Single Best Time Point, Convenient Yet Efficacious? Indian J. Endocrinol. Metab. 2018, 22, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Gillis, D.; Gillis, D.; Magiel, E.; Terespolsky, N.; Naugolny, L.; Strich, D. Clonidine stimulation test for GH deficiency: A new look at sample timing. Endocr. Pract. 2016, 22, 338–342. [Google Scholar] [CrossRef]
- Lim, S.H.; Vasanwala, R.; Lek, N.; Yap, F. Quantifying the risk of hypoglycaemia in children undergoing the glucagon stimulation test. Clin. Endocrinol. 2011, 75, 489–494. [Google Scholar] [CrossRef]
- Böttner, A.; Kratzsch, J.; Liebermann, S.; Keller, A.; Pfäffle, R.; Kiess, W.; Keller, E. Comparison of Adrenal Function Tests in Children—The Glucagon Stimulation Test Allows the Simultaneous Assessment of Adrenal Function and Growth Hormone Response in Children. J. Pediatr. Endocrinol. Metab. 2005, 18, 433–442. [Google Scholar] [CrossRef]
- Hindmarsh, P.C.; Swift, P.G. An assessment of growth hormone provocation tests. Arch. Dis. Child. 1995, 72, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Tenenbaum, A.; Phillip, M.; de Vries, L. The Intramuscular Glucagon Stimulation Test Does Not Provide Good Discrimination between Normal and Inadequate ACTH Reserve When Used in the Investigation of Short Healthy Children. Horm. Res. Paediatr. 2014, 82, 194–200. [Google Scholar] [CrossRef]
- Conceição, F.L.; Silva, A.d.C.e.; Costa, A.J.L.; Vaisman, M. Glucagon stimulation test for the diagnosis of GH deficiency in adults. J. Endocrinol. Investig. 2003, 26, 1065–1070. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | Mean ± SD |
|---|---|
| Age (years) | 10.03 ± 2.88 |
| Height (below the age and sex standard means) | −2.3 ± 1.2 |
| BMI (kg/m2) | 15.95 ± 4.053 |
| Tanner stage of puberty | 2 ± 1.2 |
| Growth velocity (cm/12 months) | 3.074 ± 2.093 |
| Bone age (years) | 8.34 ± 4.51 |
| Peak GH (ng/mL) | |
| With insulin | 5.79 ± 3.01 |
| With clonidine | 5.85 ± 2.94 |
| With glucagon | 7.64 ± 4.51 |
| Diagnosis | Number of cases |
| Isolated GHD | 137 (68%) |
| Hypopituitarism | 18 (9%) |
| Brain tumor | 40 (20%) |
| Syndromes with growth failure | 6 (3%) |
| 3 M syndrome | 3 |
| Wiedemann–Steiner syndrome | 1 |
| Bartter syndrome | 2 |
| Patients underwent the ITT and CST (n = 119) and were diagnosed with GHD | 54 (45.3%) |
| Patients underwent the GST and CST (n = 32) and were diagnosed with GHD | 18 (56.2%) |
| * Total number | 201 |
| Value | Asymptotic Standard Error a | Approximate T b | Approximate Significance | ||
|---|---|---|---|---|---|
| Measure of Agreement | Kappa | 0.258 | 0.091 | 2.816 | 0.005 |
| N of Valid Cases | 119 | ||||
| Value | Asymptotic Standard Error a | Approximate T b | Approximate Significance | ||
|---|---|---|---|---|---|
| Measure of Agreement | Kappa | 0.178 | 0.183 | 1.007 | 0.314 |
| N of Valid Cases | 32 | ||||
| A: Spearman’s Rank Correlation Coefficient (ITT and CST) | ||||
| ITT | CST | |||
| Spearman’s rho | ITT | Correlation Coefficient | 1.000 | 0.710 |
| Significance (2-tailed) | <0.001 | |||
| N | 119 | 119 | ||
| CST | Correlation Coefficient | 0.710 | 1.000 | |
| Significance (2-tailed) | <0.001 | |||
| N | 119 | 119 | ||
| B: Spearman’s Rank Correlation Coefficient (GST and CST) | ||||
| GST | CST | |||
| Spearman’s rho | GST | Correlation Coefficient | 1.000 | 0.702 |
| Significance (2-tailed) | <0.001 | |||
| N | 32 | 32 | ||
| CST | Correlation Coefficient | 0.702 | 1.000 | |
| Significance (2-tailed) | <0.001 | |||
| N | 32 | 32 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Balwi, R.; Al-Qahtani, M.; Alrowished, A.K.; Shash, H.A.; Alatrash, R.; Alhareth, A.; Aldossary, R.; Alahmari, M.; Hejazi, Y.; Alammari, A.; et al. Reliability of Agreement between Insulin, Clonidine, and Glucagon Stimulation Tests for the Diagnosis of Growth Hormone Deficiency in Children: A Retrospective Cohort Study. Children 2023, 10, 1381. https://doi.org/10.3390/children10081381
Al Balwi R, Al-Qahtani M, Alrowished AK, Shash HA, Alatrash R, Alhareth A, Aldossary R, Alahmari M, Hejazi Y, Alammari A, et al. Reliability of Agreement between Insulin, Clonidine, and Glucagon Stimulation Tests for the Diagnosis of Growth Hormone Deficiency in Children: A Retrospective Cohort Study. Children. 2023; 10(8):1381. https://doi.org/10.3390/children10081381
Chicago/Turabian StyleAl Balwi, Rana, Mohammad Al-Qahtani, Amani K. Alrowished, Hwazen A. Shash, Reem Alatrash, Alanoud Alhareth, Roba Aldossary, Maha Alahmari, Yara Hejazi, Alia Alammari, and et al. 2023. "Reliability of Agreement between Insulin, Clonidine, and Glucagon Stimulation Tests for the Diagnosis of Growth Hormone Deficiency in Children: A Retrospective Cohort Study" Children 10, no. 8: 1381. https://doi.org/10.3390/children10081381
APA StyleAl Balwi, R., Al-Qahtani, M., Alrowished, A. K., Shash, H. A., Alatrash, R., Alhareth, A., Aldossary, R., Alahmari, M., Hejazi, Y., Alammari, A., AlShawaf, S., Al Balwi, R., & AlKhater, S. (2023). Reliability of Agreement between Insulin, Clonidine, and Glucagon Stimulation Tests for the Diagnosis of Growth Hormone Deficiency in Children: A Retrospective Cohort Study. Children, 10(8), 1381. https://doi.org/10.3390/children10081381