


Magnetic Compression Anastomosis–Past Experience and Current Proposals for Further Development in Pediatric Minimally Invasive Surgery
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
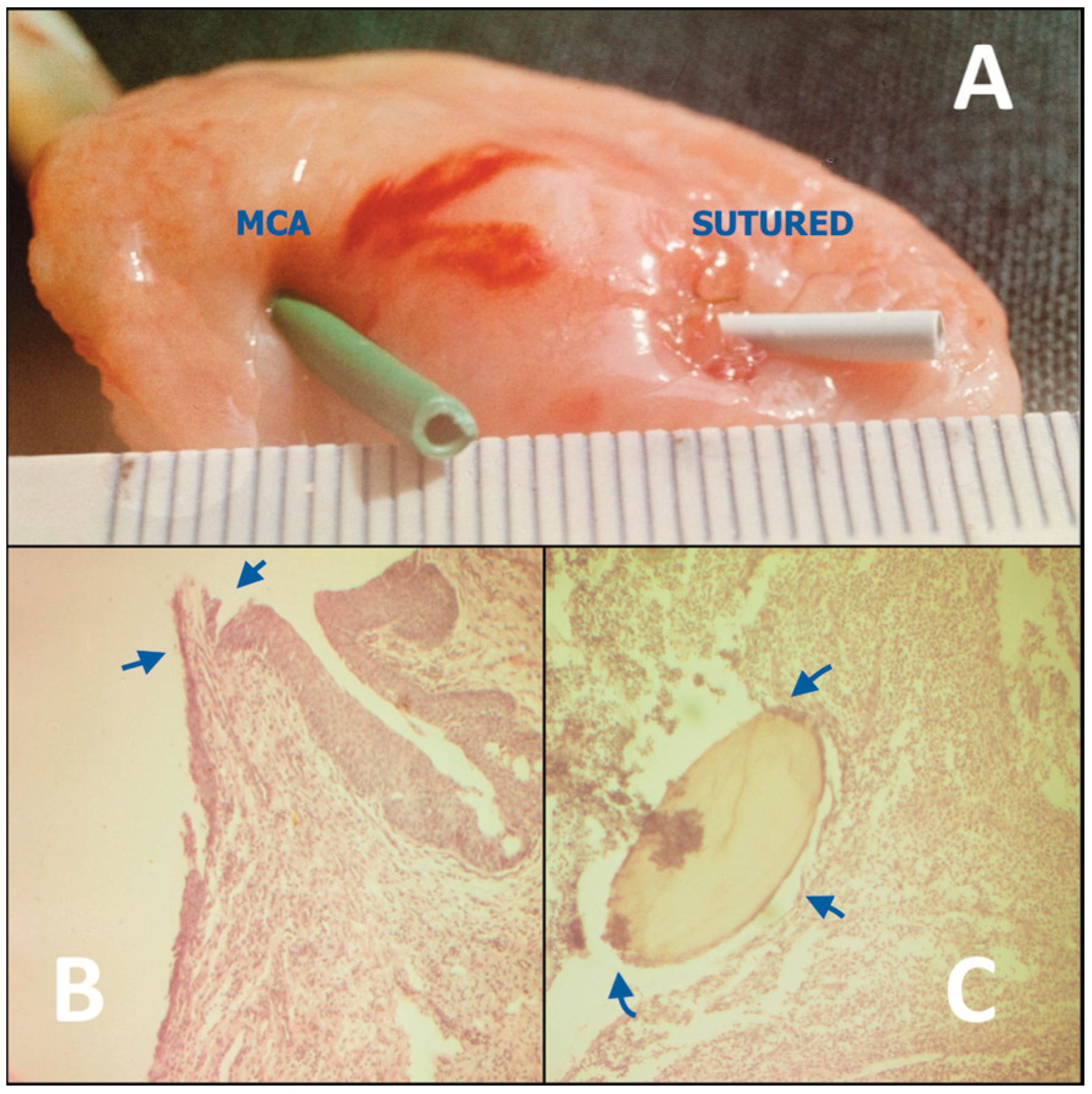
3.1. General Aspects and Preclinical Experiments
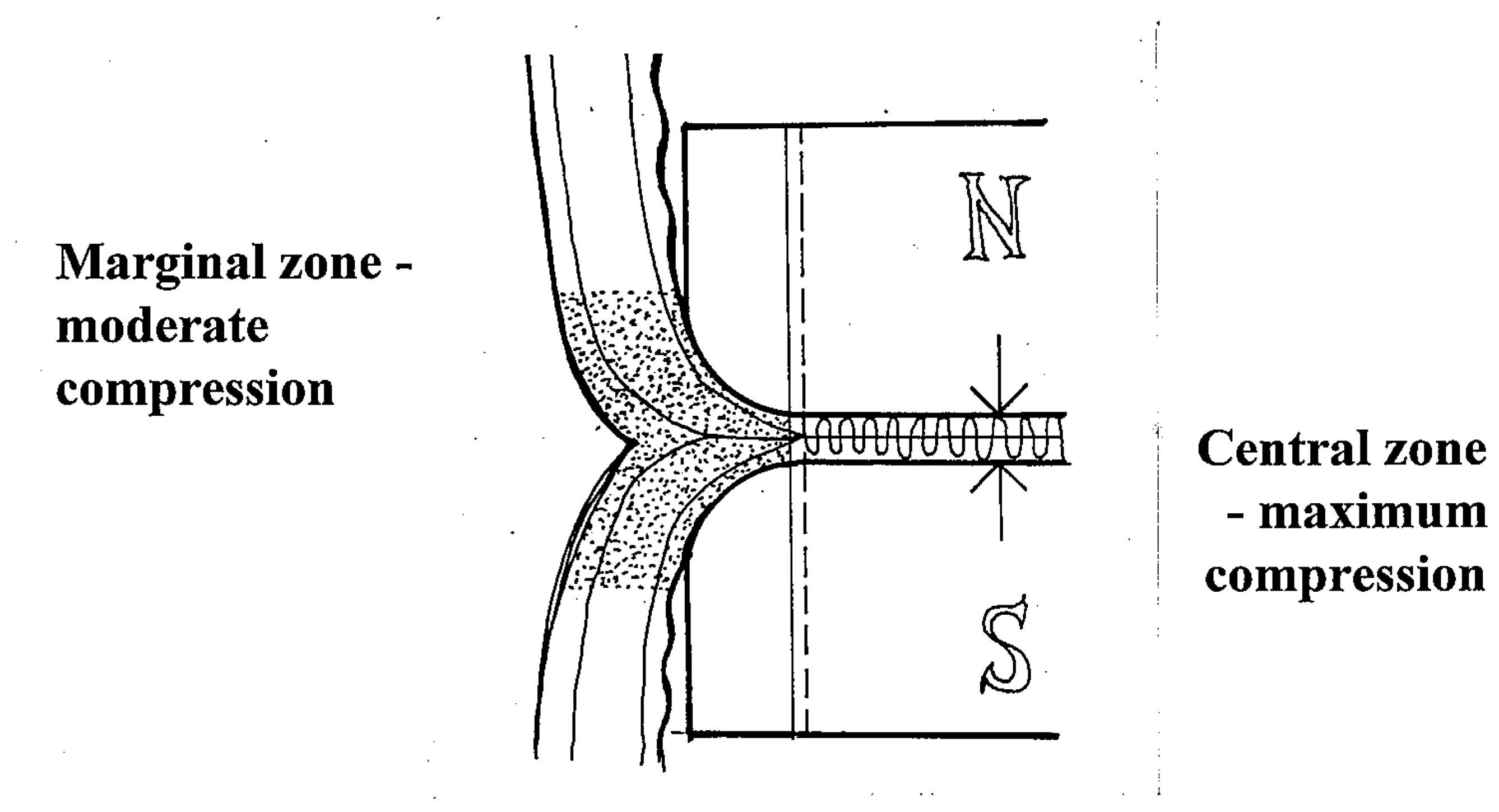
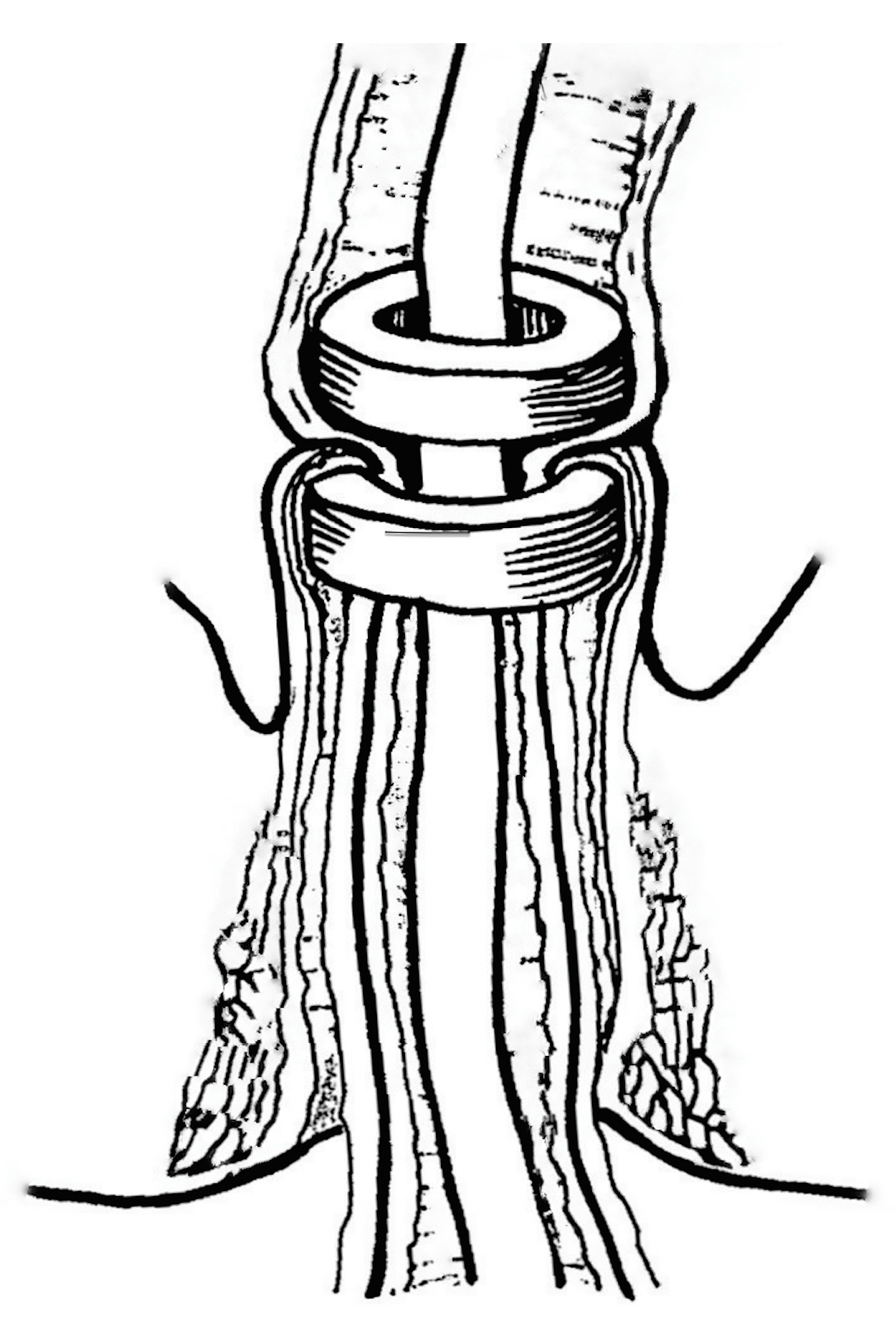
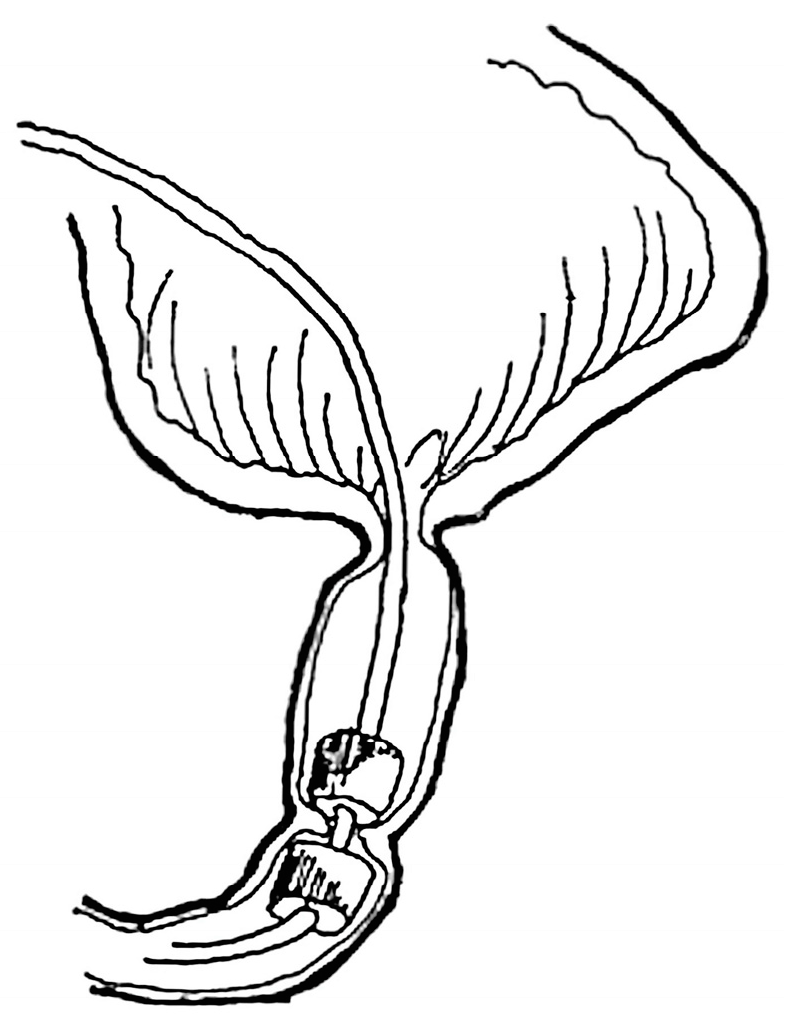
- At the anastomotic line, epithelization and connective tissue matrix proliferation dynamically develop at the so called “zone of moderate compression”, where the compression forces decrease gradually towards the periphery. This is effectively modulated by the rounded edges of magnetic compression surfaces. Flat magnets should not be used for MCA because they are associated with a higher degree of scarring and, thus, stricture formation.
- In the demarcated central zone, maximal compression is required to ensure reliable anastomotic coaptation, and to exponentially compress the subjected tissue to the point of desiccation and necrosis, preventing suppurative necrosis with inflammation within the anastomosis itself, which may lead to inadequate anastomosis formation and increased proliferation of granulation tissue.
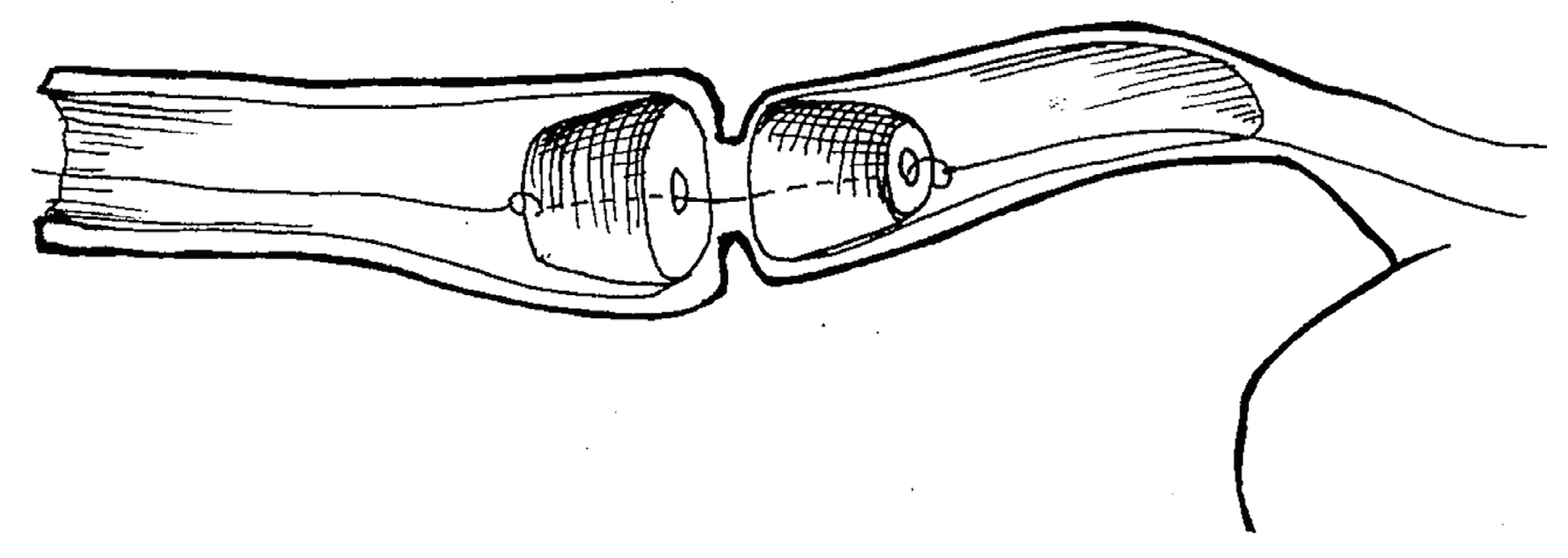
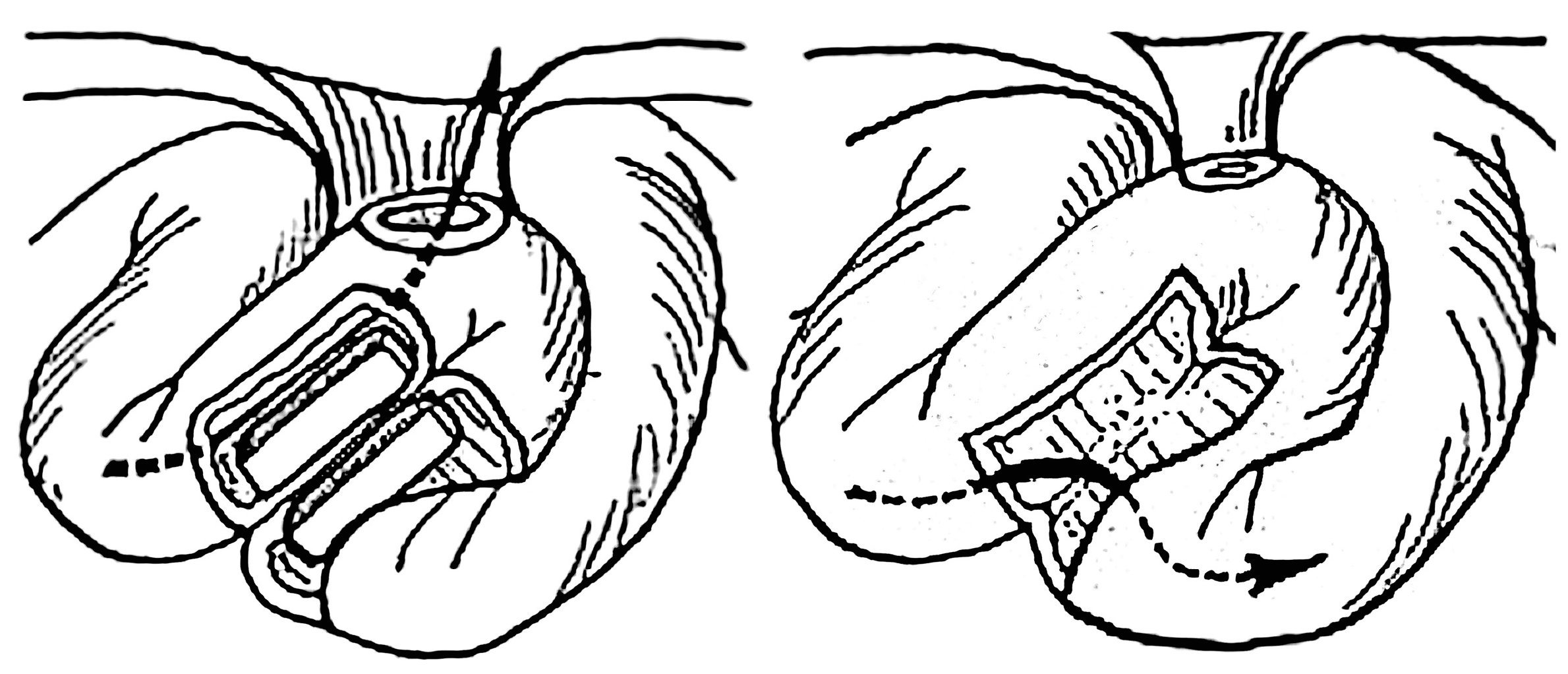
- At the demarcation zone that constitutes the inner anastomotic line, epithelization steadily progresses and bridges the rim of the thinned desiccated central tissue. The magnet thereby gradually becomes detached and passes distally within 7 to 10 days; thus, the anastomotic healing by primary intention is completed (Figure 2) [15,17,18,20].
3.2. Review of Clinical Trials
3.2.1. Non-Operative MCA Esophageal Recanalization
3.2.2. Non-Operative MCA Ileostomy Undiversion
3.2.3. Swenson Type MCA-Based Pull-through for Hirschsprung Disease
3.2.4. Non-Operative Urethral Recanalization
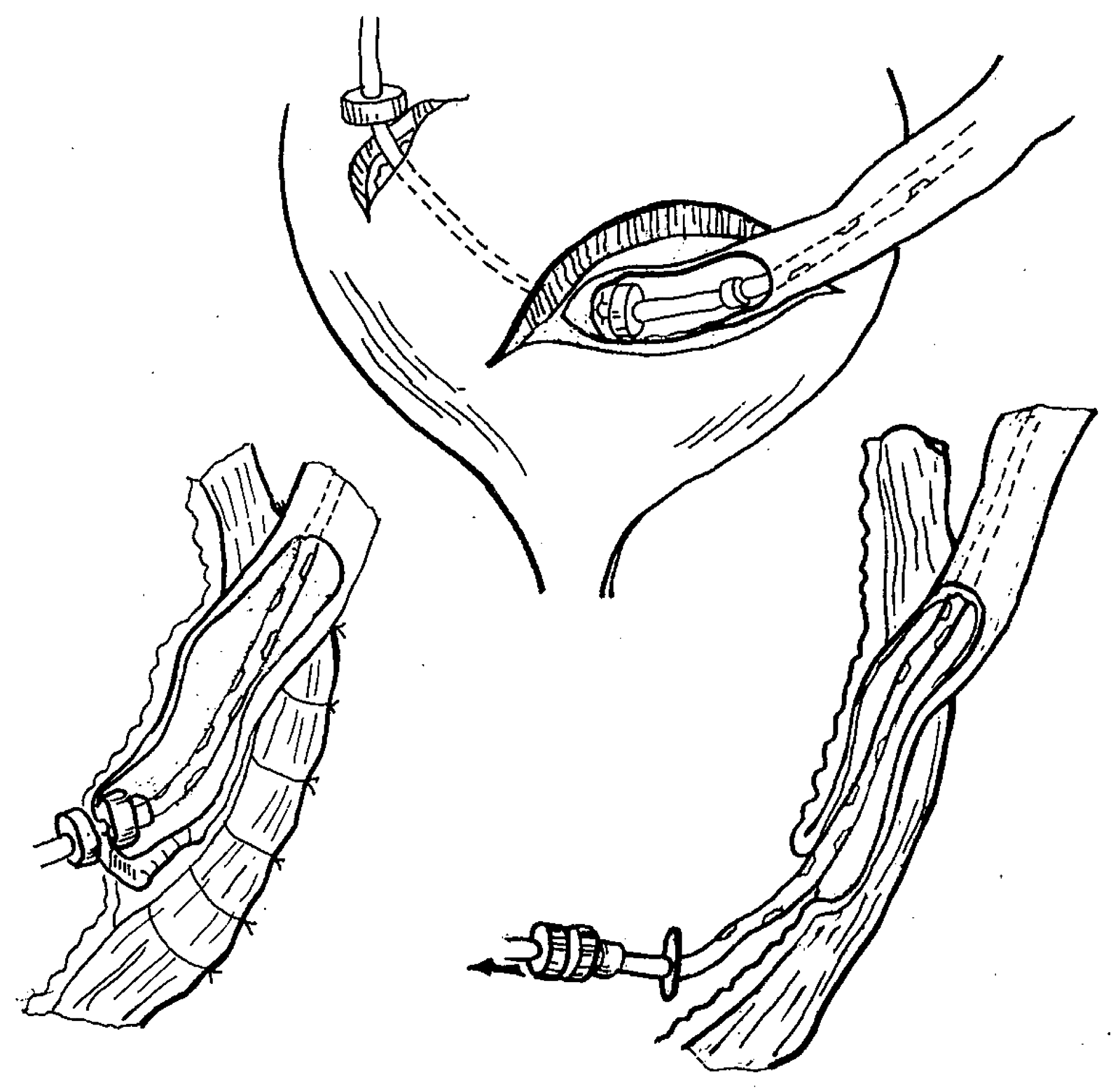
3.2.5. Extravesical Ureterocystoneostomy
3.3. Clinical Success for MCA
3.4. Recognized Adverse Effects Associated with MCA
- Inability to safely perform ileostomy undiversion in two patients due to interposing of excessively thick tissue, so that the procedure was aborted due to safety concerns [24];
4. Discussion
- Designing and industrially manufacturing biocompatible and safe rare earth magnetic devices for specific anastomotic indications with optimal parameters of compression, size, and specific geometrical shape for creating MCA in pediatric gastrointestinal and urinary structures.
- Designing and industrially manufacturing an auxiliary magnetic driving device with computerized technology that would facilitate intraluminal magnet positioning and coaptation, ensuring efficient MCA creation while electronically monitoring and securing optimal tissue compression. This should be facilitated by measuring the distance and the resulting effective magnetic coercivity force, thereby detecting possible undue anastomotic tissue tension and/or bulky tissue interposition between magnets in real-time.
- Push for further research into the development and standardization of MCA in conjuncture with pediatric MIS with a focus on the following procedures:
- ▪
- Endoluminal recanalization in short-length obstructive lesions with a various pathogenesis and localization;
- ▪
- Non-operative undiversion of intestinal stomas;
- ▪
- Laparoscopic pull-through;
- ▪
- Laparoscopic extravesical ureteric reimplantation;
- ▪
- Laparoscopic biliary-digestive reconstruction;
- ▪
- Laparoscopic duodenal atresia repair;
- ▪
- Laparoscopic-assisted repair of certain anorectal malformations;
- ▪
- Thoracoscopic esophageal atresia repair with and without a fistula.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jansen, A.; Keeman, J.N.; Davies, G.A.; Klopper, P.J. Early experiences with magnetic rings in resection of the distal colon. Neth. J. Surg. 1980, 32, 20–27. Available online: https://pubmed.ncbi.nlm.nih.gov/7366876/ (accessed on 28 July 2023).
- Jamshidi, R.; Stephenson, J.T.; Clay, J.G.; Pichakron, K.O.; Harrison, M.R. Magnamosis: Magnetic compression anastomosis with comparison to suture and staple techniques. J. Pediatr. Surg. 2009, 44, 222–228. [Google Scholar] [CrossRef]
- Gonzales, K.D.; Douglas, G.; Pichakron, K.O.; Kwiat, D.A.; Gallardo, S.G.; Encinas, J.L.; Hirose, S.; Harrison, M.R. Magnamosis III: Delivery of a magnetic compression anastomosis device using minimally invasive endoscopic techniques. J. Pediatr. Surg. 2012, 47, 1291–1295. [Google Scholar] [CrossRef] [PubMed]
- Wall, J.; Diana, M.; Leroy, J.; DeRuijter, V.; Gonzales, K.D.; Lindner, V.; Harrison, M.; Marescaux, J. Magnamosis IV: Magnetic compression anastomosis for minimally invasive colorectal surgery. Endoscopy 2013, 45, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Dorman, R.M.; Vali, K.; Harmon, C.M.; Zaritzky, M.; Bass, K.D. Repair of esophageal atresia with proximal fistula using endoscopic magnetic compression anastomosis (Magnamosis) after staged lengthening. Pediatr. Surg. Int. 2016, 32, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Toselli, L.; Martinez-Ferro, M.; Cervio, G.; Kwiat, D.; Imamura-Ching, J.; Graves, C.E.; Gaston, B.; Harrison, M. Magnetic Compression Anastomosis (Magnamosis) for Functional Undiversion of Ileostomy in Pediatric Patients. J. Laparoendosc. Adv. Surg. Technol. 2017, 27, 1314–1317. [Google Scholar] [CrossRef] [PubMed]
- Woo, R.; Wong, C.M.; Trimble, Z.; Puapong, D.; Koehler, S.; Miller, S.; Johnson, S. Magnetic compression stricturoplasty for treatment of refractory esophageal strictures in children: Technique and lessons learned. Surg. Innov. 2017, 24, 432–439. [Google Scholar] [CrossRef]
- Liu, S.Q.; Lv, Y.; Fang, Y.; Luo, R.X.; Zhao, J.R.; Luo, R.G.; Li, Y.M.; Zhang, J.; Zhang, P.F.; Guo, J.Z.; et al. Magnetic compression for anastomosis in treating an infant born with long-gap oesophageal atresia: A case report. Medicine 2020, 99, e22472. [Google Scholar] [CrossRef]
- Liu, S.Q.; Li, Q.F.; Lv, Y.; Zhao, J.R.; Luo, R.X.; Zhang, P.F.; Guo, J.Z.; Zhang, A.P.; Li, Q.H. Magnetic compression anastomosis for rectal atresia following necrotizing enterocolitis: A case report. Medicine 2020, 99, e23613. [Google Scholar] [CrossRef]
- Liu, S.; Fang, Y.; Lv, Y.; Zhao, J.; Luo, R.; Luo, R.; Cheng, J.; Yang, H.; Zhang, A.; Shen, Y.; et al. Magnetic compression stricturoplasty in patients with severe stricture after simultaneous esophageal atresia and duodenal obstruction repair: A case report. Exp. Ther. Med. 2022, 23, 93. [Google Scholar] [CrossRef]
- Muensterer, O.J.; Evans, L.L.; Sterlin, A.; Sahlabadi, M.; Aribindi, V.; Lindner, A.; König, T.; Harrison, M.R. Novel device for endoluminal esophageal atresia repair: First-in-human experience. Pediatrics 2021, 148, e2020049627. [Google Scholar] [CrossRef]
- Holler, A.-S.; König, T.T.; Chen, C.; Harrison, M.R.; Muensterer, O.J. Esophageal magnetic compression anastomosis in esophageal atresia repair: A PRISMA-compliant systematic review and comparison with a novel approach. Children 2022, 9, 1113. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.G.; Evans, L.L.; Johnson, S.M.; Woo, R.K. The evolving use of magnets in surgery: Biomedical considerations and a review of their current applications. Bioengineering 2023, 10, 442. [Google Scholar] [CrossRef] [PubMed]
- Isakov, Y.F.; Geras’kin, V.I.; Vasil’ev, G.S.; Sharipov, N.A. Using permanent magnets in pediatric surgery. Klin. Khir. 1981, 6, 36–39. Available online: https://pubmed.ncbi.nlm.nih.gov/7024620/ (accessed on 28 July 2023).
- Sharipov, N.A. Colorectal Resections with the Use of Permanent Magnets in Children. Ph.D. Thesis, N.I. Pirogov National Medical University, Moscow, Russia, 1982. [Google Scholar]
- Stepanov, E.A.; Vasil’Ev, G.S.; Sharipov, N.A.; Rudakov, S.S.; Romakhin, I.A. Use of permanent magnets in digestive tract surgery in children. Vestn. Akad. Med. Nauk SSSR 1984, 9, 6–11. Available online: https://pubmed.ncbi.nlm.nih.gov/6388182/ (accessed on 28 July 2023).
- Nikolaev, V.V. Treatment of Urethral Strictures with the Use of Permanent Magnets in Children. Ph.D. Thesis, N.I. Pirogov National Medical University, Moscow, Russia, 1987. [Google Scholar]
- Kotlovsky, A.M. Ureteric Reimplantation with the Use of Permanent Magnets in Children. Ph.D. Thesis, N.I. Pirogov National Medical University, Moscow, Russia, 1987. [Google Scholar]
- Isakov, I.F.; Stepanov, E.A.; Erokhin, A.P.; Nikolaev, V.V.; Vasi’Lev, G.S. Surgical treatment of urethral strictures in children. Vestn. Khir. Im. I I Grek. 1989, 142, 61–66. Available online: https://pubmed.ncbi.nlm.nih.gov/2800174/ (accessed on 28 July 2023).
- Lubashevskiĭ, V.T.; Shabanov, A.M.; Vasil’ev, G.S. The inflammatory-reparative processes in the implantation of the ureter into the bladder by using the mechanical forces of permanent magnets. Bull. Exp. Biol. Med. 1993, 116, 550–552. Available online: https://pubmed.ncbi.nlm.nih.gov/8312560/ (accessed on 28 July 2023). [CrossRef]
- Nikolaev, V.V. Technical principles of urethral compression anastomoses. Bull. Exp. Biol. Med. 1998, 126, 855–858. [Google Scholar] [CrossRef]
- Stepanov, E.A.; Vasilév, G.S.; Nikolaev, V.V.; Guz, V.I.; Sharipov, N.A.; Romanov, A.V.; Goritskaia, T.A.; Vasilév, K.G. Treatment of short esophageal stricture in children. Vestn. Ross. Akad. Med. Nauk. 1994, 3, 15–19. Available online: https://pubmed.ncbi.nlm.nih.gov/7516212/ (accessed on 28 July 2023).
- Sharipov, N.A. Treatment of Esophageal Strictures. Ph.D. Thesis, N.I. Pirogov National Medical University, Moscow, Russia, 1996. [Google Scholar]
- Stepanov, E.A.; Vasil’ev, G.S.; Nikolaev, V.V. The treatment of intestinal fistulas in children by applying a by-pass anastomosis using magnetic devices. Khirurgiia (Mosk) 1992, 11, 93–95. Available online: https://pubmed.ncbi.nlm.nih.gov/1294807/ (accessed on 28 July 2023).
- Stepanov, E.A.; Nikolaev, V.V.; Kotlovsky, A.M.; Vasilév, G.S. Method of Correction of Urethral Strictures; Patent for Invention—Authors’ copyright No. 1361753; Bulletin Inventions and Discoveries, 49; USSR: Moscow, Russia, 1987. [Google Scholar]
- Isakov, Y.F.; Stepanov, E.A.; Kotlovsky, A.M.; Vasilév, G.S. Method of Ureterocystoneostomy; Patent for Invention—Authors’ copyright No. 1277452; Bulletin Inventions and Discoveries, 46; USSR: Moscow, Russia, 1986. [Google Scholar]
- Evans, L.L.; Chen, C.S.; Muensterer, O.J.; Sahlabadi, M.; Lovvorn, H.N.; Novotny, N.M.; Upperman, J.S.; Martinez, J.A.; Bruzoni, M.; Dunn, J.C.; et al. The novel application of an emerging device for salvage of primary repair in high-risk complex esophageal atresia. J. Pediatr. Surg. 2022, 57, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Liu, S.; Lei, P.; Lv, Y.; Wu, R.; Ma, F.; Wang, H.; Luo, R. Fast and Effective Nonsuture Anastomosis of Magnetic Artificial Blood Vessel Transplantation for Caval Reconstruction in Canines. Ann. Vasc. Surg. 2020, 68, 487–496. [Google Scholar] [CrossRef]
- Mascagni, P.; Tringali, A.; Boškoski, I.; Bove, V.; Schepis, T.; Perri, V.; Costamagna, G. Magnetic kissing for the endoscopic treatment of a complete iatrogenic stenosis of the hypopharynx. Endoscopy 2023, 55, E499–E500. [Google Scholar] [CrossRef]
- Sterlin, A.; Evans, L.; Mahler, S.; Lindner, A.; Dickmann, J.; Heimann, A.; Sahlabadi, M.; Aribindi, V.; Harrison, M.R.; Muensterer, O.J. An experimental study on long term outcomes after magnetic esophageal compression anastomosis in piglets. J. Pediatr. Surg. 2022, 57, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Hornok, Z.; Kubiak, R.; Csukas, D.; Ferencz, A.; Cserni, T. Esophageal Magnetic Anastomosis Device (EMAD) to simplify and improve outcome of thoracoscopic repair for esophageal atresia with tracheoesophageal fistula: A proof of concept study. J. Pediatr. Surg. 2023, 58, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.-H.; Lv, Y.; Liu, S.-Q.; Cui, X.-H.; Suo, R.-Y. Esophageal magnetic compression anastomosis in dogs. World J. Gastroenterol. 2022, 28, 5313–5323. [Google Scholar] [CrossRef]
- Gagner, M.; Krinke, T.; Lapointe-Gagner, M.; Buchwald, J.N. Side-to-side duodeno-ileal magnetic compression anastomosis: Design and feasibility of a novel device in a porcine model. Surg. Endosc. 2023, 37, 6197–6207. [Google Scholar] [CrossRef]
- Gagner, M.; Abuladze, D.; Koiava, L.; Buchwald, J.N.; Van Sante, N.; Krinke, T. First-in-Human Side-to-Side Magnetic Compression Duodeno-ileostomy with the Magnet Anastomosis System. Obes. Surg. 2023, 33, 2282–2292. [Google Scholar] [CrossRef]
- Zhang, J.; Xue, W.; Tian, P.; Yan, H.; Zheng, J.; Li, X.; Wang, Y.; Ding, X.; Lyu, Y. Clinical effect of magnetic compression anastomosis on ureterostenosis after kidney transplantation. Chin. Med. J. 2023, 136, 1006–1008. [Google Scholar] [CrossRef]
- Gökçe, D.T.; Ödemiş, B.; Erdoğan, Ç. Magnetic compression anastomosis using a double-balloon enteroscope for complete obstruction of Roux-en-Y hepaticojejunostomy anastomosis. Endoscopy 2022, 54, E945–E947. [Google Scholar] [CrossRef]
- Suyama, K.; Takamori, H.; Yamanouchi, E.; Tanaka, H.; Sakamoto, Y.; Ikuta, Y.; Maki, Y.; Sakurai, K.; Hirota, M.; Baba, H.; et al. Recanalization of Obstructed Choledochojejunostomy Using the Magnet Compression Anastomosis Technique. Am. J. Gastroenterol. 2010, 105, 230–231. [Google Scholar] [CrossRef] [PubMed]
- Ödemiş, B.; Başpınar, B.; Tola, M.; Torun, S. Magnetic Compression Anastomosis Is a Good Treatment Option for Patients with Completely Obstructed Benign Biliary Strictures: A Case Series Study. Dig. Dis. Sci. 2022, 67, 4906–4918. [Google Scholar] [CrossRef] [PubMed]
- Akita, H.; Hikita, H.; Yamanouchi, E.; Marubashi, S.; Nagano, H.; Umeshita, K.; Dono, K.; Tsutsui, S.; Hayashi, N.; Monden, M. Use of a metallic-wall stent in the magnet compression anastomosis technique for bile duct obstruction after liver transplantation. Liver Transplant. 2007, 14, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Scientific Committee of the Third International Conference of Magnetic Surgery; Zhang, N.; Lv, Y. Expert consensus on magnetic recanalization technique for biliary anastomotic strictures after liver transplantation. HepatoBiliary Surg. Nutr. 2021, 10, 401–404. [Google Scholar] [CrossRef]
- Isozaki, T.; Murakami, K.; Yamanouchi, E.; Uesato, M.; Toyozumi, T.; Koide, Y.; Tsukamoto, S.; Sakata, H.; Hayano, K.; Kano, M.; et al. Magnetic compression anastomosis is effective in treating stenosis after esophageal cancer surgery: A case report. Surg. Case Rep. 2020, 6, 213. [Google Scholar] [CrossRef]
- Liu, K.; Lu, Q.; Huang, G.-B.; Zhou, J.-W.; Wang, X.-Y.; Chang, P.-K.; Zhang, W.; Yu, J.-W.; Lyu, Y.; Wang, S.-P. Use of the magnetic compression technique in sleeve gastrectomy. Chin. Med. J. 2020, 133, 2768–2770. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MCA Locations and Types | Animal Model | n |
|---|---|---|
| Small intestine (end-to-end and side-to-side) | rabbit | 96 (42 and 54) |
| Colorectal end-to-end | canine | 47 |
| Ureterovesical side-to-side with Lich-Gregoir tunnelling | canine | 55 |
| Urethral end-to-end | canine | 52 |
| Indications for MCA | Successful Outcomes | Adverse Outcomes |
|---|---|---|
| Esophageal recanalization (n = 15) | Esophageal patency restored (n = 9) | Perforation (n = 1) Restenosis (n = 5) |
| Ileostomy undiversion (n = 46) | Intestinal passage restored (n = 44) | Technical failure (n = 2) |
| Swenson pull-through (n = 10) | Colorectal junction patent (n = 6) | Postop stenosis (n = 2) |
| Urethral recanalization (n = 5) | Urethral patency restored (n = 4) | Partial restenosis (n = 1) |
| Extravesical ureterocystostomy (n = 11) | Neo-orifice functional (n = 11) | none |
| Total (n = 87) | n = 76, overall success rate 87.3% | n = 11, adverse outcomes in 12.6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotlovsky, A.M.; Muensterer, O.J.; Nikolaev, V.V.; Razumovskiy, A.Y. Magnetic Compression Anastomosis–Past Experience and Current Proposals for Further Development in Pediatric Minimally Invasive Surgery. Children 2023, 10, 1328. https://doi.org/10.3390/children10081328
Kotlovsky AM, Muensterer OJ, Nikolaev VV, Razumovskiy AY. Magnetic Compression Anastomosis–Past Experience and Current Proposals for Further Development in Pediatric Minimally Invasive Surgery. Children. 2023; 10(8):1328. https://doi.org/10.3390/children10081328
Chicago/Turabian StyleKotlovsky, Anatole M., Oliver J. Muensterer, Vasily V. Nikolaev, and Alexander Y. Razumovskiy. 2023. "Magnetic Compression Anastomosis–Past Experience and Current Proposals for Further Development in Pediatric Minimally Invasive Surgery" Children 10, no. 8: 1328. https://doi.org/10.3390/children10081328
APA StyleKotlovsky, A. M., Muensterer, O. J., Nikolaev, V. V., & Razumovskiy, A. Y. (2023). Magnetic Compression Anastomosis–Past Experience and Current Proposals for Further Development in Pediatric Minimally Invasive Surgery. Children, 10(8), 1328. https://doi.org/10.3390/children10081328