
Bacterial Pathogens and Antimicrobial Susceptibility Patterns of Urinary Tract Infections in Children during COVID-19 2019–2020: A Large Tertiary Care Center in Saudi Arabia

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Patients and Bacterial Isolates
2.3. Microbiological Culturing of Urine Samples: Stringent Selection and Methodological Approaches
2.4. Utilization of the BD Phoenix System for Identification of Bacterial Isolates
2.5. Antimicrobial Susceptibility Testing of Escherichia coli Strains using the Kirby Bauer Method
2.6. Application of the Double-Disc Synergy Test (DDST) for the Detection of Extended-Spectrum Beta-Lactamase (ESBL) Activity
2.7. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics
3.2. Antimicrobial Susceptibility Patterns
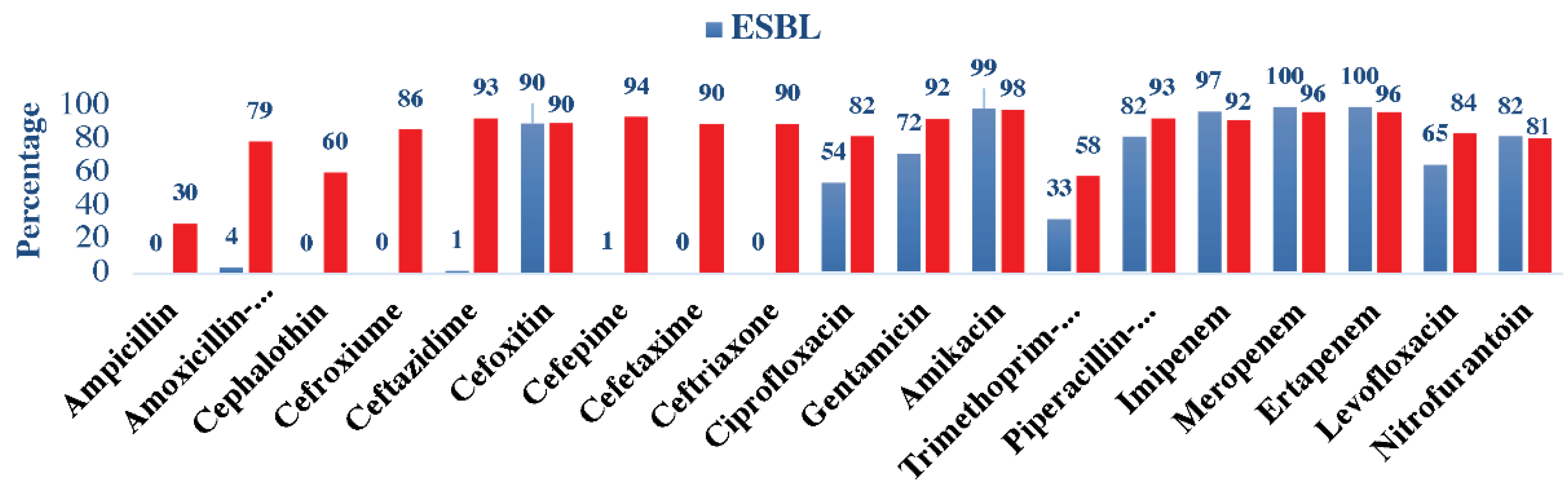
3.3. Susceptibility Patterns among ESBL and Non-ESBL Uropathogens
4. Discussion
4.1. Antimicrobial Susceptibility Patterns in COVID-19 Era
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Wing, H.L.; Yip, H.W.; Au-Yeung, A.W.S.; Chan, J.C.S. Imaging in pediatric urinary tract infection: A 9-year local experience. Am. J. Roentgenol. 2009, 192, 1253–1260. [Google Scholar]
- Quan, J.; Dai, H.; Liao, W.; Zhao, D.; Shi, Q.; Zhang, L.; Shi, K.; Akova, M.; Yu, Y. Etiology and prevalence of ESBLs in adult community-onset urinary tract infections in East China: A prospective multicenter study. J. Infect. 2021, 83, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Dai, B.; Liu, Y.; Jia, J.; Mei, C. Long-term antibiotics for the prevention of recurrent urinary tract infection in children: A systematic review and meta-analysis. Arch. Dis. Child. 2010, 95, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, L.E. Catheter associated urinary tract infections. Antimicrob. Resist. Infect. Control 2014, 3, 23. [Google Scholar] [CrossRef]
- Renda, R. Diagnosis and Antibiotic Resistance Distribution in Children with Urinary Tract Infection: A Single Center Experience. Int. J. Pediatr. 2018, 6, 6815–6822. [Google Scholar] [CrossRef]
- Kang, C.I.; Kim, J.; Park, D.W.; Kim, B.N.; Ha, U.S.; Lee, S.J.; Wie, S.H. Clinical practice guidelines for the antibiotic treatment of community-acquired urinary tract infections. Infect. Chemother. 2018, 50, 67–100. [Google Scholar] [CrossRef]
- Mamishi, S.; Shalchi, Z.; Mahmoudi, S.; Sadeghi, R.H.; Ashtiani, M.T.H.; Pourakbari, B. Antimicrobial Resistance and Genotyping of Bacteria Isolated from Urinary Tract Infection in Children in an Iranian Referral Hospital. Infect. Drug Resist. 2020, 13, 3317–3323. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E. Resistance Trends and Epidemiology of Citrobacter-Enterobacter-Serratia in Urinary Tract Infections of Inpatients and Outpatients (RECESUTI): A 10-Year Survey. Medicina 2019, 55, 285. [Google Scholar] [CrossRef]
- Goyal, D.; Dean, N.; Neill, S.; Jones, P.; Dascomb, K. Risk Factors for Community-Acquired Extended-Spectrum Beta-Lactamase–Producing Enterobacteriaceae Infections—A Retrospective Study of Symptomatic Urinary Tract Infections. Open Forum Infect. Dis. 2019, 6, ofy357. [Google Scholar] [CrossRef]
- Gunduz, S.; Altun, H.U. Antibiotic resistance patterns of urinary tract pathogens in Turkish children. Glob. Health Res. Policy 2018, 3, 10. [Google Scholar] [CrossRef]
- Balkhi, B.; Mansy, W.; Alghadeer, S.; Alnuaim, A.; AlShehri, A.; Somily, A. Antimicrobial susceptibility of microorganisms causing Urinary Tract Infections in Saudi Arabia. J. Infect. Dev. Ctries 2018, 12, 220–227. [Google Scholar] [CrossRef]
- Ironmonger, D.; Edeghere, O.; Gossain, S.; Hawkey, P.M. Use of antimicrobial resistance information and prescribing guidance for management of urinary tract infections: Survey of general practitioners in the West Midlands. BMC Infect. Dis. 2016, 16, 226. [Google Scholar] [CrossRef]
- Bono, M.J.; Leslie, S.W.; Reygaert, W.C. Urinary Tract Infection. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2023. [Google Scholar]
- Cornaglia, G.; Courcol, R.; Herrmann, J.L.; Kahlmeter, G.; Peigue-Lafeuille, H.; Jordi, V. (Eds.) European Manual of Clinical Microbiology; European Society for Clinical Microbiology and Infectious Diseases: Basel, Switzerland, 2012. [Google Scholar]
- Abalkhail, A.; AlYami, A.S.; Alrashedi, S.F.; Almushayqih, K.M.; Alslamah, T.; Alsalamah, Y.A.; Elbehiry, A. The Prevalence of Multidrug-Resistant Escherichia coli Producing ESBL among Male and Female Patients with Urinary Tract Infections in Riyadh Region, Saudi Arabia. Healthcare 2022, 10, 1778. [Google Scholar] [CrossRef]
- Vandepitte, J.; Verhaegen, J.; Engbaek, K.; Piot, P.; Heuck, C.C.; Rohner, P.; Heuck, C.C. Basic Laboratory Procedures in Clinical Bacteriology; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Carroll, K.C.; Glanz, B.D.; Borek, A.P.; Burger, C.; Bhally, H.S.; Henciak, S.; Flayhart, D. Evaluation of the BD Phoenix automated microbiology system for identification and antimicrobial susceptibility testing of Enterobacteriaceae. J. Clin. Microbiol. 2006, 44, 3506–3509. [Google Scholar] [CrossRef]
- Kosikowska, U.; Andrzejczuk, S.; Grywalska, E.; Chwiejczak, E.; Winiarczyk, S.; Pietras-Ożga, D.; Stępień-Pyśniak, D. Prevalence of susceptibility patterns of opportunistic bacteria in line with CLSI or EUCAST among Haemophilus parainfluenzae isolated from respiratory microbiota. Sci. Rep. 2020, 10, 11512. [Google Scholar] [CrossRef]
- Duttaroy, B.; Mehta, S. Extended spectrum b lactamases (ESBL) in clinical isolates of Klebsiella pneumoniae and Escherichia coli. Indian J. Pathol. Microbiol. 2005, 48, 45–48. [Google Scholar]
- Odoki, M.; Aliero, A.A.; Tibyangye, J.; Maniga, J.N.; Wampande, E.; Kato, C.D.; Agwu, E.; Bazira, J. Prevalence of Bacterial Urinary Tract Infections and Associated Factors among Patients Attending Hospitals in Bushenyi District, Uganda. Int. J. Microbiol. 2019, 2019, 4246780. [Google Scholar] [CrossRef]
- Al Nafeesah, A.; Al Fakeeh, K.; Chishti, S.; Hameed, T. E. coli versus Non-E. coli Urinary Tract Infections in Children: A Study from a Large Tertiary Care Center in Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2022, 9, 46–48. [Google Scholar] [CrossRef]
- Hameed, T.; Al Nafeesah, A.; Chishti, S.; Al Shaalan, M.; Al Fakeeh, K. Community-acquired urinary tract infections in children: Resistance patterns of uropathogens in a tertiary care center in Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2019, 6, 51–54. [Google Scholar] [CrossRef]
- Afsharpaiman, S.; Bairaghdar, F.; Torkaman, M.; Kavehmanesh, Z.; Amirsalari, S.; Moradi, M.; Safavimirmahalleh, J. Bacterial pathogens and re-sistance patterns in children with community-acquired urinary tract infection: A cross sectional study. J. Compr. Ped. 2012, 3, 16–20. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, J.; de Malet, A.; Cano, M.E.; de la Rubia, L.; Wallmann, R.; Martínez-Martínez, L.; Calvo, J. Antimicrobial susceptibility of microorganisms that cause urinary tract infections in pediatric patients. Enferm. Infecc. Microbiol. Clin. 2018, 36, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Shakibaie, M.R.; Adeli, S.; Salehi, M.H. Antimicrobial Susceptibility Pattern and ESBL Production among Uropathogenic Escherichia coli Isolated from UTI Children in Pediatric Unit of a Hospital in Kerman, Iran. Br. Microbiol. Res. J. 2014, 4, 262–271. [Google Scholar] [CrossRef]
- Sharifian, M.; Karimi, A.; Tabatabaei, S.R.; Anvaripour, N. Microbial sensitivity pattern in urinary tract infections in children: A single center experience of 1,177 urine cultures. Jpn. J. Infect. Dis. 2006, 59, 380–382. [Google Scholar] [PubMed]
- El-Gamasy, M.A.; Amin, E.K.; Zaid, A.M.A.; Kotb, A.E.R.I. Incidence, risk factors and causative bacteria of urinary tract infections and their antimicrobial sensitivity patterns in toddlers and children: A report from two tertiary care hospitals. Saudi J. Kidney Dis. Transplant. 2020, 31, 200–208. [Google Scholar] [CrossRef]
- Vazouras, K.; Velali, K.; Tassiou, I.; Anastasiou-Katsiardani, A.; Athanasopoulou, K.; Barbouni, A.; Jackson, C.; Folgori, L.; Zaoutis, T.; Basmaci, R.; et al. Antibiotic treatment and antimicrobial resistance in children with urinary tract infections. J. Glob. Antimicrob. Resist. 2020, 20, 4–10. [Google Scholar] [CrossRef]
- Edlin, R.S.; Shapiro, D.J.; Hersh, A.L.; Copp, H.L. Antibiotic Resistance Patterns of Outpatient Pediatric Urinary Tract Infections. J. Urol. 2013, 190, 222–227. [Google Scholar] [CrossRef]
- Alavudeen, S.S.; Asiri, A.A.; Fageeh, S.A.; Aljarie, A.A.; Iqbal, M.J.; Khan, N.A.; Tabassum, F.; Rahamathulla, M.; Hani, U.; Akhtar, S. Evaluation of Antibiotic Prescribing Practices and Antimicrobial Sensitivity Patterns in Urinary Tract Related Infectious Diseases in Pediatric Patients. Front. Pediatr. 2021, 9, 740106. [Google Scholar] [CrossRef]
- Ali, E.; Osman, A. Acute Urinary Tract Infections in Children in Khartoum State: Pathogens, Antimicrobial Susceptibility and Associated Risk Factors. Arab. J. Nephrol. Transplant. 2010, 2, 11–15. [Google Scholar] [CrossRef][Green Version]
- Al-Balas, M.; Al-Balas, H.I.; Jaber, H.M.; Obeidat, K.; Al-Balas, H.; Aborajooh, E.A.; Al-Taher, R.; Al-Balas, B. Distance learning in clinical medical education amid COVID-19 pandemic in Jordan: Current situation, challenges, and perspectives. BMC Med. Educ. 2020, 20, 341. [Google Scholar] [CrossRef]
- Tasbakan, M.I.; Pullukcu, H.; Sipahi, O.R.; Yamazhan, T.; Ulusoy, S. Nitrofurantoin in the treatment of extended-spectrum β-lactamase-producing Escherichia coli-related lower urinary tract infection. Int. J. Antimicrob. Agents 2012, 40, 554–556. [Google Scholar] [CrossRef]
- Pinheiro, F.R.; Rozza-de-Menezes, R.E.; Blum, M.C.; Pereira, R.F.A.; Rocha, J.A.; Guedes Pinto, M.C.F.; Penna, B.A.; Riley, L.W.; Aguiar-Alves, F. Evaluation of changes in antimicrobial susceptibility in bacteria infecting children and their mothers in pediatric, neonatal-intensive care unit, and gynecology/obstetrics wards of a quaternary referral hospital during the COVID-19 pandemic. Front. Microbiol. 2023, 14, 1096223. [Google Scholar] [CrossRef]
- Collignon, P.; Beggs, J.J. CON: COVID-19 will NOT result in increased AMR prevalence. JAC Antimicrob. Resist. 2020, 2, dlaa051. [Google Scholar] [CrossRef]


{kind=link}
| AGE | Neonates (3.8%) | Infants (24.8%) | Children (71.4%) | Pearson | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bacteria | Total (N = 39) | Male (n = 22) | Female (n = 17) | Total (N = 253) | Male (n = 155) | Female (n = 98) | Total (N = 730) | Male (n = 206) | Female (n = 524) | Chi-Square | p |
| E. coli | 59.0 | 59.1 | 58.8 | 42.7 | 36.8 | 52.0 | 64.1 | 40.3 | 73.5 | 68.729 | 0.000 |
| Klebsiella sp. | 25.6 | 22.7 | 29.4 | 37.5 | 41.3 | 31.6 | 19.0 | 30.6 | 14.5 | 11.114 | 0.004 |
| Proteus sp. | 0.0 | 0.0 | 0.0 | 3.6 | 3.2 | 4.1 | 5.8 | 8.3 | 4.8 | 1.687 | 0.407 |
| Enterobacter sp. | 2.6 | 4.5 | 0.0 | 3.2 | 1.3 | 6.1 | 3.7 | 7.3 | 2.3 | 3.333 | 0.189 |
| Citrobacter sp. | 2.6 | 4.5 | 0.0 | 1.2 | 1.3 | 1.0 | 1.2 | 2.4 | 0.8 | 3.001 | 0.221 |
| Serratia sp. | 2.6 | 0.0 | 5.9 | 1.6 | 1.9 | 1.0 | 0.1 | 0.0 | 0.2 | 3.000 | 0.223 |
| Pseudomonas sp. | 7.7 | 9.1 | 5.9 | 10.3 | 14.2 | 4.1 | 6.0 | 11.2 | 4.0 | 7.462 | 0.024 |
| Antibiotic | E. coli | Klebsiella | Proteus sp. | Enterobacter sp. | Citrobacter sp. | Serratia | Pseudomonas sp. | Overall Sensitive |
|---|---|---|---|---|---|---|---|---|
| (n = 599) | (n = 244) | (n = 51) | (n = 36) | (n = 13) | (n = 6) | (n = 73) | ||
| Ampicillin | 28.4 | 0 | 33.3 | 0 | 0 | 0 | NT | 19.7 |
| Amoxicillin-Clavulanate | 54.4 | 55.3 | 86.3 | 0 | 53.8 | 0 | NT | 54.0 |
| Cephalothin | 36.7 | 49.6 | 74.5 | 0 | 23.1 | 0 | NT | 40.3 |
| Cefuroxime | 61.6 | 54.1 | 80.4 | 5.6 | 38.5 | 0 | NT | 57.9 |
| Ceftazidime | 65.4 | 59.4 | 94.1 | 63.9 | 92.3 | 50.0 | 86.3 | 67.1 |
| Cefoxitin | 91.7 | 84.4 | 100.0 | 0 | 38.5 | 0 | NT | 85.5 |
| Cefepime | 66.1 | 60.2 | 96.1 | 72.2 | 84.6 | 50.0 | 87.7 | 68.1 |
| Cefotaxime | 64.4 | 56.6 | 80.4 | 47.2 | 76.9 | 16.7 | NT | 62.5 |
| Ceftriaxone | 64.4 | 56.6 | 80.4 | 47.2 | 76.9 | 16.7 | NT | 62.5 |
| Ciprofloxacin | 71.3 | 80.3 | 76.5 | 83.3 | 92.3 | 100.0 | 84.9 | 75.5 |
| Gentamicin | 89.0 | 81.1 | 74.5 | 88.9 | 100.0 | 33.3 | 87.7 | 86.1 |
| Amikacin | 99.0 | 97.1 | 96.1 | 100.0 | 100.0 | 100.0 | 93.2 | 98.0 |
| Trimethoprim-Sulfamethoxazole | 47.6 | 59.4 | 43.1 | 63.9 | 84.6 | 100.0 | NT | 51.8 |
| Piperacillin-Tazobactam | 94.3 | 76.6 | 100.0 | 72.2 | 100.0 | 50.0 | 84.9 | 88.7 |
| Imipenem | 95.2 | 88.9 | 92.2 | 91.7 | 100.0 | 83.3 | 80.8 | 92.4 |
| Meropenem | 99.2 | 92.2 | 100.0 | 94.4 | 100.0 | 83.3 | 83.6 | 96.2 |
| Ertapenem | 99.2 | 92.2 | 100.0 | 94.4 | 100.0 | 83.3 | NT | 97.2 |
| Levofloxacin | 73.8 | 90.2 | 76.5 | 91.7 | 92.3 | 100.0 | 74.0 | 78.9 |
| Nitrofurantoin | 96.8 | 59.4 | 2.0 | 44.4 | 61.5 | NT | NT | 79.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altamimi, I.; Almazyed, A.; Alshammary, S.; Altamimi, A.; Alhumimidi, A.; Alnutaifi, R.; Malhis, M.; Altamimi, A. Bacterial Pathogens and Antimicrobial Susceptibility Patterns of Urinary Tract Infections in Children during COVID-19 2019–2020: A Large Tertiary Care Center in Saudi Arabia. Children 2023, 10, 971. https://doi.org/10.3390/children10060971
Altamimi I, Almazyed A, Alshammary S, Altamimi A, Alhumimidi A, Alnutaifi R, Malhis M, Altamimi A. Bacterial Pathogens and Antimicrobial Susceptibility Patterns of Urinary Tract Infections in Children during COVID-19 2019–2020: A Large Tertiary Care Center in Saudi Arabia. Children. 2023; 10(6):971. https://doi.org/10.3390/children10060971
Chicago/Turabian StyleAltamimi, Ibraheem, Abeer Almazyed, Sami Alshammary, Abdulaziz Altamimi, Abdullah Alhumimidi, Raed Alnutaifi, Mohammed Malhis, and Abdullah Altamimi. 2023. "Bacterial Pathogens and Antimicrobial Susceptibility Patterns of Urinary Tract Infections in Children during COVID-19 2019–2020: A Large Tertiary Care Center in Saudi Arabia" Children 10, no. 6: 971. https://doi.org/10.3390/children10060971
APA StyleAltamimi, I., Almazyed, A., Alshammary, S., Altamimi, A., Alhumimidi, A., Alnutaifi, R., Malhis, M., & Altamimi, A. (2023). Bacterial Pathogens and Antimicrobial Susceptibility Patterns of Urinary Tract Infections in Children during COVID-19 2019–2020: A Large Tertiary Care Center in Saudi Arabia. Children, 10(6), 971. https://doi.org/10.3390/children10060971