

Effectiveness of Psychomotor Therapy among Children with Graphomotor Impairment with and without DCD-Diagnosis

 , , ,
, , ,
Abstract
1. Introduction
1.1. Handwriting Research in Children
1.2. Developmental Coordination Disorder and Handwriting Difficulties
1.3. Developmental Dysgraphia without DCD
1.4. Consequences of Poor Handwriting
1.5. Therapeutic Approaches for Children with DCD
1.6. Therapeutic Approaches for Children with Handwriting Difficulties
2. Materials and Methods
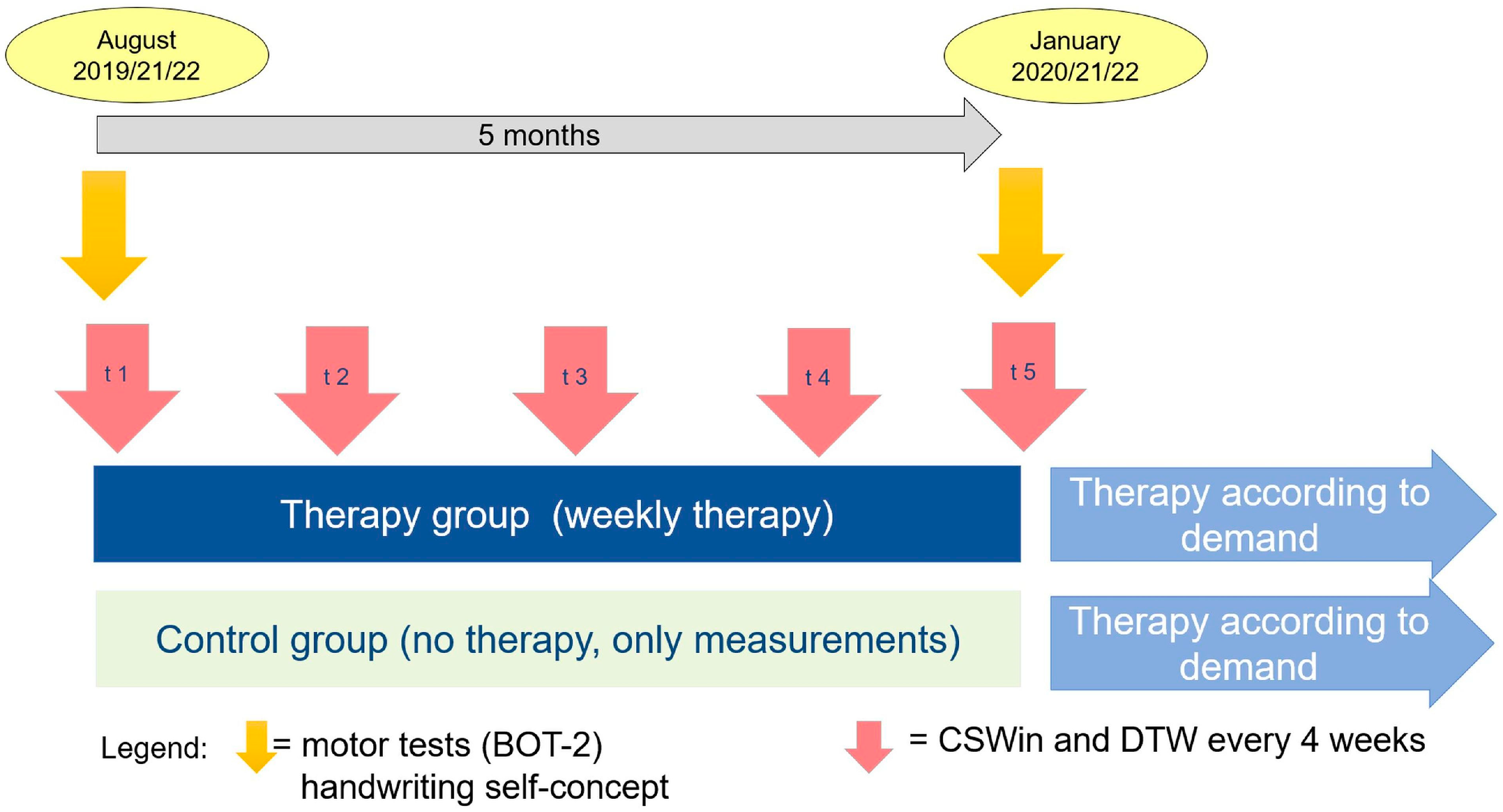
2.1. Design
2.2. Participants
2.3. Material
2.4. Procedure
2.5. Measures
2.5.1. Fine Motor Performance
2.5.2. Process-Based Handwriting Measures
2.5.3. Handwriting Self-Concept
2.5.4. Therapy Aims and Therapy Protocols
2.5.5. Data Analysis
3. Results
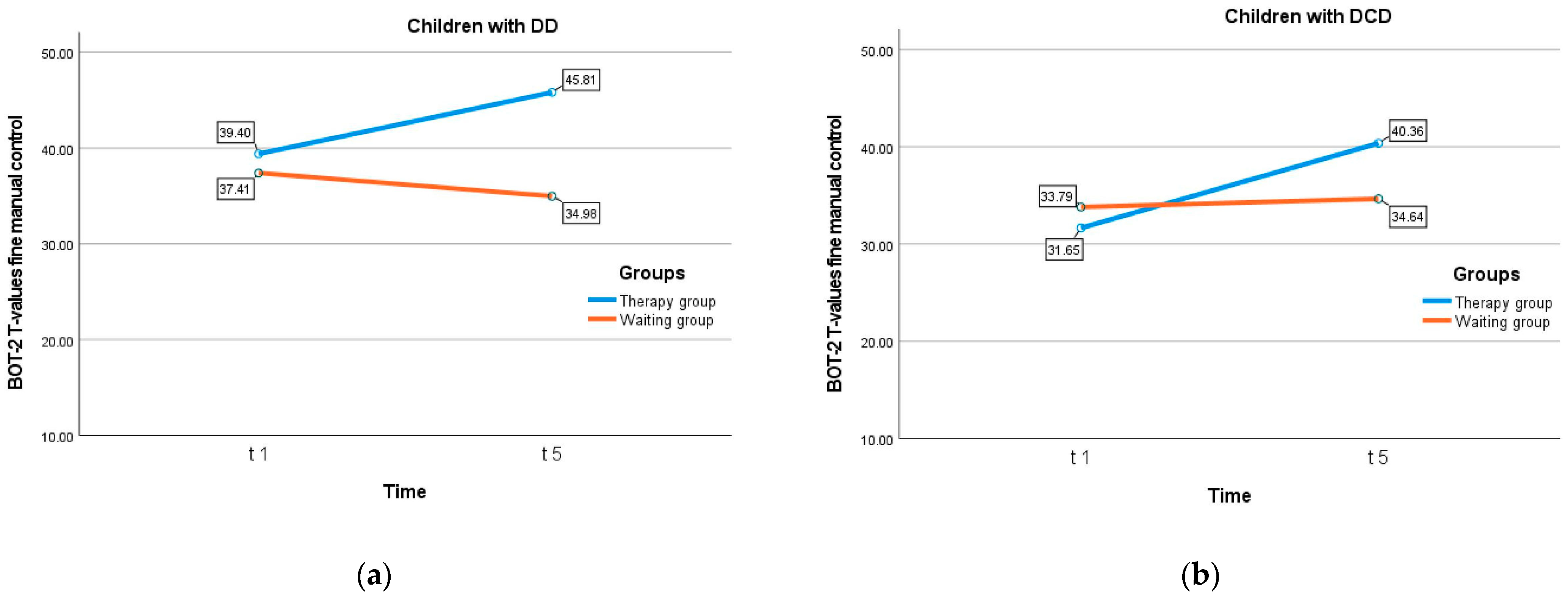
3.1. Fine Motor Skills
3.2. Process-Based Handwriting Results
3.3. Handwriting Self-Concept
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| t1 | t2 | t3 | t4 | t5 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | |
| Measures | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) |
| FREQ 3 | 2.41 (0.99) | 2.29 (0.94) | 2.53 (1.03) | 2.61 (0.96) | 2.72 (0.97) | 2.50 (0.95) | 2.73 (1.06) | 2.78 (1.02) | 2.69 (1.12) | 2.77 (0.97) | 2.80 (0.94) | 2.74 (1.02) | 2.69 (0.83) | 2.76 (0.82) | 2.62 (0.85) |
| NIV 3 | 1.87 (1.05) | 1.90 (0.99) | 1.84 (1.28) | 1.68 (0.94) | 1.52 (0.78) | 1.84 (1.06) | 1.47 (0.77) | 1.43 (0.82) | 1.51 (0.69) | 1.51 (0.94) | 1.38 (0.65) | 1.65 (1.17) | 1.57 (1.52) | 1.43 (0.96) | 1.74 (1.99) |
| FREQ 5 | 3.44 (1.00) | 3.60 (0.98) | 3.26 (1.01) | 3.71 (0.98) | 3.86 (1.00) | 3.55 (0.94) | 3.69 (1.01) | 3.73 (1.04) | 3.65 (0.99) | 3.68 (1.11) | 3.79 (1.11) | 3.58 (1.10) | 3.67 (0.96) | 3.70 (0.87) | 3.64 (1.05) |
| NIV 5 | 1.26 (0.99) | 1.21 (1.09) | 1.31 (0.87) | 1.12 (0.33) | 1.13 (0.31) | 1.11 (0.35) | 1.11 (0.26) | 1.10 (0.19) | 1.12 (0.32) | 1.51 (0.45) | 1.17 (0.55) | 1.13 (0.34) | 1.10 (0.31) | 1.09 (0.37) | 1.11 (0.24) |
| FREQ 7 | 2.62 (0.96) | 2.65 (0.98) | 2.58 (0.95) | 2.75 (0.96) | 2.89 (0.96) | 2.62 (0.95) | 2.84 (0.90) | 2.92 (0.81) | 2.75 (0.98) | 2.83 (0.97) | 2.95 (0.92) | 2.71 (1.01) | 2.80 (0.88) | 2.83 (0.81) | 2.77 (0.94) |
| NIV 7 | 1.86 (1.58) | 1.82 (1.55) | 1.90 (1.63) | 1.75 (1.73) | 1.61 (1.55) | 1.89 (1.89) | 1.47 (0.83) | 1.39 (0.85) | 1.56 (0.81) | 1.70 (1.78) | 1.49 (1.20) | 1.91 (2.20) | 1.47 (0.84) | 1.43 (0.64) | 1.52 (1.02) |
| FREQ 8 | 1.12 (0.38) | 1.20 (0.42) | 1.06 (0.32) | 1.33 (0.49) | 1.32 (0.52) | 1.34 (0.46) | 1.32 (0.44) | 1.24 (0.38) | 1.42 (0.49) | 1.42 (0.54) | 1.35 (0.49) | 1.50 (0.58) | 1.38 (0.51) | 1.27 (0.45) | 1.50 (0.55) |
| NIV 8 | 5.47 (2.37) | 5.06 (2.15) | 5.86 (2.53) | 4.57 (2.76) | 4.85 (1.07) | 4.26 (2.37) | 4.13 (2.10) | 4.41 (1.99) | 3.82 (2.20) | 4.05 (2.64) | 4.38 (2.71) | 3.71 (2.55) | 4.17 (2.54) | 4.50 (2.45) | 3.79 (2.61) |
| FREQ 9 | 1.70 (0.54) | 1.74 (0.55) | 1.66 (0.54) | 2.00 (0.68) | 1.99 (0.71) | 2.01 (0.65) | 0.99 (0.39) | 1.89 (0.74) | 2.07 (0.76) | 2.05 (0.76) | 2.09 (0.77) | 2.01 (0.76) | 2.15 (0.76) | 2.08 (0.69) | 2.22 (0.83) |
| NIV 9 | 3.03 (1.67) | 2.91 (1.54) | 3.15 (1.81) | 2.51 (1.49) | 2.51 (1.48) | 2.51 (1.52) | 2.54 (1.52) | 2.57 (1.30) | 2.50 (1.77) | 2.46 (1.69) | 2.27 (1.23) | 2.65 (2.06) | 2.15 (1.12) | 2.12 (1.06) | 2.19 (1.20) |
| FREQ 10 | 0.89 (0.28) | 0.90 (0.31) | 0.87 (0.24) | 1.09 (0.41) | 1.10 (0.45) | 1.07 (0.38) | 0.99 (0.39) | 0.95 (0.37) | 1.05 (0.42) | 1.07 (0.42) | 0.98 (0.36) | 1.16 (0.45) | 1.10 (0.41) | 1.01 (0.38) | 1.21 (0.43) |
| NIV 10 | 8.03 (3.51) | 8.09 (3.80) | 7.98 (3.23) | 6.22 (3.21) | 6.24 (3.43) | 6.19 (2.99) | 7.11 (3.82) | 7.29 (3.42) | 6.89 (4.28) | 6.53 (4.12) | 7.30 (4.74) | 5.71 (3.17) | 6.22 (3.71) | 6.97 (4.08) | 5.40 (3.07) |
| FREQ 13 | 1.03 (0.45) | 1.08 (0.44) | 0.99 (0.46) | 1.16 (0.56) | 1.21 (0.57) | 1.11 (0.56) | 1.25 (0.56) | 1.23 (0.54) | 1.26 (0.60) | 1.37 (0.63) | 1.39 (0.59) | 1.35 (0.67) | 1.45 (0.63) | 1.46 (0.63) | 1.43 (0.65) |
| NIV 13 | 6.98 (5.99) | 6.49 (6.20) | 7.50 (5.76) | 5.99 (4.98) | 5.60 (4.43) | 6.40 (5.49) | 5.30 (4.03) | 4.99 (3.06) | 5.63 (4.85) | 4.53 (3.68) | 4.11 (2.79) | 4.94 (4.37) | 3.98 (3.44) | 3.74 (2.53) | 4.23 (4.17) |
| FREQ 14 | 1.15 (0.52) | 1.15 (0.48) | 1.14 (0.56) | 1.36 (0.59) | 1.37 (0.58) | 1.34 (0.60) | 1.46 (0.61) | 1.46 (0.57) | 1.45 (0.65) | 1.57 (0.69) | 1.60 (0.65) | 1.56 (0.74) | 1.57 (0.59) | 1.57 (0.49) | 1.57 (0.68) |
| NIV 14 | 5.41 (3.57) | 5.20 (3.60) | 5.64 (3.56) | 4.50 (3.59) | 4.36 (3.17) | 4.64 (3.99) | 3.97 (3.28) | 3.67 (2.23) | 4.27 (4.07) | 3.42 (2.21) | 3.17 (1.82) | 3.68 (2.54) | 3.32 (2.41) | 3.04 (1.86) | 3.61 (2.85) |
| FREQ 15 | 1.63 (0.68) | 1.64 (0.71) | 1.63 (0.65) | 1.78 (0.72) | 1.85 (0.76) | 1.72 (0.68) | 1.90 (0.80) | 1.97 (0.81) | 1.82 (0.78) | 2.00 (0.84) | 2.06 (0.77) | 1.95 (0.90) | 2.07 (0.86) | 2.03 (0.82) | 2.11 (0.90) |
| NIV 15 | 3.42 (2.58) | 3.56 (2.93) | 3.28 (2.18) | 2.91 (2.01) | 2.83 (2.06) | 3.00 (1.96) | 2.78 (2.22) | 2.59 (1.96) | 2.98 (2.46) | 2.50 (1.76) | 2.28 (1.50) | 2.72 (1.97) | 2.37 (1.57) | 2.36 (1.61) | 2.38 (1.55) |
| t1 | t2 | t3 | t4 | t5 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | Total | Therapy Group | Waiting Group | |
| Measures | M | M | M | M | M | M | M | M | M | M | M | M | M | M | M |
| (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | |
| DTW 8 Distance | 0.08 | 0.08 | 0.09 | 0.08 | 0.08 | 0.09 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 | 0.08 |
| (0.04) | (0.03) | (0.04) | (0.33) | (0.03) | (0.04) | (0.03) | (0.03) | (0.03) | (0.08) | (0.02) | (0.04) | (0.07) | (0.3) | (0.03) | |
| DTW 8 Consistency | 35.57 | 37.95 | 33.26 | 29.81 | 31.92 | 27.48 | 29.91 | 32.09 | 27.49 | 30.81 | 32.92 | 28.59 | 31.33 | 34.11 | 28.19 |
| (22.44) | (21.99) | (22.95) | (24.04) | (20.43) | (20.24) | (17.63) | (19.11) | (15.73) | (21.02) | (21.97) | (20.03) | (19.47) | (20.14) | (18.39) | |
| DTW 8 | 20.05 | 20.24 | 19.86 | 23.51 | 22.58 | 24.53 | 22.23 | 22.23 | 22.23 | 21.37 | 19.56 | 23.27 | 21.3 | 19.93 | 22.84 |
| Deviance | (18.05) | (18.42) | (17.94) | (18.79) | (16.92) | (20.86) | (17.62) | (19.40) | (15.67) | (17.36) | (16.29) | (18.42) | (20.27) | (16.99) | (23.52) |
| DTW 9 Distance | 0.10 | 0.09 | 0.10 | 0.09 | 0.09 | 0.09 | 0.10 | 0.10 | 0.10 | 0.10 | 0.09 | 0.10 | 0.10 | 0.09 | 0.10 |
| (0.05) | (0.04) | (0.05) | (0.04) | (0.03) | (0.04) | (0.04) | (0.04) | (0.40) | (0.04) | (0.03) | (0.04) | (0.03) | (0.03) | (0.30) | |
| DTW 9 Consistency | 26.17 | 27.25 | 26.17 | 23.89 | 24.63 | 23.89 | 20.13 | 23.84 | 20.13 | 20.19 | 22.85 | 20.19 | 19.19 | 22.58 | 19.19 |
| (18.21) | (21.5) | (18.21) | (18.24) | (18.7) | (18.24) | (16.01) | (19.00) | (16.01) | (15.83) | (18.14) | (15.83) | (14.67) | (18.42) | (14.67) | |
| DTW 9 | 28.75 | 26.77 | 28.75 | 32.01 | 28.48 | 32.01 | 31.93 | 29.59 | 31.93 | 32.44 | 29.82 | 32.44 | 32.68 | 27.84 | 32.68 |
| Deviance | (21.68) | (22.02) | (21.68) | (26.05) | (21.33) | (26.05) | (22.52) | (24.94) | (22.52) | (22.79) | (21.59) | (22.79) | (20.37) | (21.25) | (20.37) |
| DTW 10 Distance | 0.10 | 0.08 | 0.10 | 0.09 | 0.08 | 0.09 | 0.08 | 0.08 | 0.08 | 0.09 | 0.08 | 0.09 | 0.08 | 0.07 | 0.08 |
| (0.05) | (0.04) | (0.05) | (0.04) | (0.03) | (0.04) | (0.05) | (0.04) | (0.05) | (0.04) | (0.04) | (0.04) | (0.03) | (0.03) | (0.03) | |
| DTW 10 Consistency | 25.76 | 35.25 | 25.76 | 29.16 | 31.54 | 29.16 | 29.61 | 32.66 | 29.61 | 25.96 | 34.9 | 25.96 | 29.13 | 36.53 | 29.13 |
| (19.27) | (24.94) | (19.27) | (17.79) | (23.39) | (17.79) | (19.88) | (21.50) | (19.88) | (16.00) | (22.07) | (16.00) | (17.75) | (20.76) | (17.75) | |
| DTW 10 | 27.46 | 22.47 | 27.46 | 25.71 | 17.72 | 25.71 | 20.08 | 19.89 | 20.08 | 24.23 | 19.06 | 24.23 | 23.79 | 16.32 | 23.79 |
| Deviance | (23.44) | (19.18) | (23.44) | (19.92) | (16.05) | (19.92) | (22.23) | (20.57) | (22.23) | (19.8) | (19.38) | (19.8) | (18.97) | (15.98) | (18.97) |
References
- Kandel, S.; Peereman, R.; Grosjacques, G.; Fayol, M. For a psycholinguistic model of handwriting production: Testing the syllable-bigram controversy. J. Exp. Psychol. Hum. Percept. Perform. 2011, 37, 1310–1322. [Google Scholar] [CrossRef] [PubMed]
- van Galen, G.P. Handwriting: Issues for a psychomotor theory. Hum. Mov. Sci. 1991, 10, 165–191. [Google Scholar] [CrossRef]
- van Galen, G.P.; Meulenbroek, R.G.J.; Hylkema, H. On the simultaneous monitoring of words, letter and strokes in handwriting: Evidence for a mixed linear and parallel model. In Graphonomics: Contemporary Research in Handwriting; Kao, H.S.R., van Galen, G.P., Hoosain, R., Eds.; Elsevier Science Ltd.: Amsterdam, NY, USA, 1986; pp. 5–20. [Google Scholar]
- Delattre, M.; Bonin, P.; Barry, C. Written spelling to dictation: Sound-to-spelling regularity affects both writing latencies and durations. J. Exp. Psychol. Learn. Mem. Cogn. 2006, 32, 1330–1340. [Google Scholar] [CrossRef]
- Fayol, M.; Lété, B. Contributions of online studies to understanding translation from ideas to written text. In Translation of Thought to Written Text While Composing: Advancing Theory, Knowledge, Methods, and Applications; Fayol, M., Alamargot, D., Berninger, V.W., Eds.; Psychology Press: East Sussex, UK, 2012; pp. 289–313. [Google Scholar]
- Kandel, S.; Peereman, R.; Ghimenton, A. Further evidence for the interaction of central and peripheral processes: The impact of double letters in writing English words. Front. Psychol. 2013, 4, 729. [Google Scholar] [CrossRef] [PubMed]
- Olive, T.; Alves, R.A.; Castro, S.L. Cognitive in writing during pause and execution periods. Eur. J. Cogn. Psychol. 2009, 21, 758–785. [Google Scholar] [CrossRef]
- Olive, T.; Kellogg, R.T. Concurrent activation of high- and low-level production processes in written composition. Mem. Cogn. 2002, 30, 594–600. [Google Scholar] [CrossRef]
- Roux, S.; McKeff, T.J.; Grosjacques, G.; Afonso, O.; Kandel, S. The interaction between central and peripheral processes in hand-writing production. Cognition 2013, 127, 235–241. [Google Scholar] [CrossRef]
- Abbott, R.D.; Berninger, V.W.; Fayol, M. Longitudinal relationships of levels of language in writing and between writing and reading in grades 1 to 7. J. Educ. Psychol. 2010, 102, 281–298. [Google Scholar] [CrossRef]
- Bosga-Stork, I.M.; Bosga, J.; Meulenbroek, R.G. Intentional control and biomechanical exploitation in preparatory handwriting. Hum. Mov. Sci. 2011, 30, 687–697. [Google Scholar] [CrossRef]
- Bosga-Stork, I.M.; Bosga, J.; Meulenbroek, R.G. Developing Movement Efficiency between 7 and 9 Years of Age. Mot. Control 2014, 18, 1–17. [Google Scholar] [CrossRef]
- Graham, S.; Berninger, V.; Weintraub, N.; Schafer, W. Development of Handwriting Speed and Legibility in Grades 1–9. J. Educ. Res. 1998, 92, 42–52. [Google Scholar] [CrossRef]
- Meulenbroek, R.G.J.; van Galen, G.P. Foreperiod duration and the analysis of motor stages in a line-drawing task. Acta Psychol. 1988, 69, 19–33. [Google Scholar] [CrossRef]
- Wicki, W.; Hurschler Lichtsteiner, S.; Saxer Geiger, A.; Müller, M. Handwriting fluency in children: Impact and correlates. Swiss J. Psychol. 2014, 73, 87–96. [Google Scholar] [CrossRef]
- Nottbusch, G. Handschriftliche Sprachproduktion. Sprachstrukturelle und Ontogenetische Aspekte; Max Niemeyer: Tübingen, Germany, 2008. [Google Scholar]
- Marquardt, C.; Gentz, W.; Mai, N. Visual control of automated handwriting movements. Exp. Brain Res. 1999, 128, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, P.; Vander Hart, N.; Cortesa, C. The Influence of Instructional Variables and Task Constraints on Handwriting Per-formance. J. Educ. Res. 2013, 106, 216–234. [Google Scholar] [CrossRef]
- Khalid, P.I.; Yunus, J.; Adnan, R. Extraction of dynamic features from hand drawn data for the identification of children with handwriting difficulty. Res. Dev. Disabil. 2010, 31, 256–262. [Google Scholar] [CrossRef]
- Quenzel, I.; Mai, N. Kinematische Analyse von Schreibbewegungen im Erstschreibunterricht. Unterr. Z. Für Lernforschung 2000, 28, 290–303. [Google Scholar]
- Rosenblum, S.; Parush, S.; Weiss, P.L. Computerized Temporal Handwriting Characteristics of Proficient and Non-Proficient Handwriters. Am. J. Occup. Ther. 2003, 57, 129–138. [Google Scholar] [CrossRef]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef]
- WHO. Internationale Klassifikation Psychischer Störungen. ICD-10 Kapitel V (F). Diagnostische Kriterien für Forschung und Praxis; Hogrefe: Bern, Switzerland, 2016. [Google Scholar]
- Visser, L.; Röschinger, J.; Barck, K.; Büttner, G.; Hasselhorn, M. Learning Difficulties in Children with Symptoms of DCD And/or ADHD: Analyses from a Categorical and a Continuous Approach. Int. J. Disabil. Dev. Educ. 2020, 69, 1505–1521. [Google Scholar] [CrossRef]
- Gomez, A.; Piazza, M.; Jobert, A.; Dehaene-Lambertz, G.; Dehaene, S.; Huron, C. Mathematical difficulties in developmental coordination disorder: Symbolic and nonsymbolic number processing. Res. Dev. Disabil. 2015, 43, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Biotteau, M.; Péran, P.; Vayssière, N.; Tallet, J.; Albaret, J.-M.; Chaix, Y. Neural changes associated to procedural learning and automatization process in Developmental Coordination Disorder and/or Developmental Dyslexia. Eur. J. Paediatr. Neurol. 2017, 21, 286–299. [Google Scholar] [CrossRef] [PubMed]
- Visser, J. Developmental coordination disorder: A review of research on subtypes and comorbidities. Hum. Mov. Sci. 2003, 22, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Sugden, D.A. (Ed.) Leeds Consensus Statement: Developmental Coordination Disorder as a Specific Learning Difficulty; DCD-UK/Dyscovery Centre: Leeds, UK, 2006. [Google Scholar]
- Jover, M.; Schmitz, C.; Centelles, L.; Chabrol, B.; Assaiante, C. Anticipatory postural adjustments in a bimanual load-lifting task in children with developmental coordination disorder. Dev. Med. Child Neurol. 2010, 52, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Asonitou, K.; Koutsouki, D.; Kourtessis, T.; Charitou, S. Motor and cognitive performance differences between children with and without developmental coordination disorder (DCD). Res. Dev. Disabil. 2012, 33, 996–1005. [Google Scholar] [CrossRef]
- Vaivre-Douret, L.; Lalanne, C.; Ingster-Moati, I.; Boddaert, N.; Cabrol, D.; Dufier, J.-L.; Golse, B.; Falissard, B. Subtypes of Developmental Coordination Disorder: Research on Their Nature and Etiology. Dev. Neuropsychol. 2011, 36, 614–643. [Google Scholar] [CrossRef]
- Missiuna, C.; Rivard, L.; Pollock, N. They’re Bright but Can’t Write: Developmental Coordination Disorder in school aged children. TEACHING Except. Child. Plus 2004, 1, n1. [Google Scholar]
- Biotteau, M.; Danna, J.; Baudou, E.; Puyjarinet, F.; Velay, J.-L.; Albaret, J.-M.; Chaix, Y. Developmental coordination disorder and dysgraphia: Signs and symptoms, diagnosis, and rehabilitation. Neuropsychiatr. Dis. Treat. 2019, 15, 1873–1885. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.C.M.; van Galen, G.P. Dysgraphia in children: Lasting psychomotor deficiency or transient developmental delay? J. Exp. Child Psychol. 1997, 67, 164–184. [Google Scholar] [CrossRef]
- Rosenblum, S.; Livneh-Zirinski, M. Handwriting process and product characteristics of children diagnosed with developmental coordination disorder. Hum. Mov. Sci. 2008, 27, 200–214. [Google Scholar] [CrossRef]
- Huau, A.; Velay, J.-L.; Jover, M. Graphomotor skills in children with developmental coordination disorder (DCD): Handwriting and learning a new letter. Hum. Mov. Sci. 2015, 42, 318–332. [Google Scholar] [CrossRef]
- Bo, J.; Colbert, A.; Lee, C.-M.; Schaffert, J.; Oswald, K.; Neill, R. Examining the relationship between motor assessments and handwriting consistency in children with and without probable Developmental Coordination Disorder. Res. Dev. Disabil. 2014, 35, 2035–2043. [Google Scholar] [CrossRef] [PubMed]
- Prunty, M.M.; Barnett, A.L.; Wilmut, K.; Plumb, M. Handwriting speed in children with Developmental Coordination Disorder: Are they really slower? Res. Dev. Disabil. 2013, 34, 2927–2936. [Google Scholar] [CrossRef] [PubMed]
- Jolly, C.; Huron, C.; Albaret, J.M.; Gentaz, É. Analyse comparative des tracés de lettres cursives d’une enfant atteinte d’un trouble d’acquisition de la coordination et scolarisée en CP avec ceux d’enfants ordinaires de GSM et de CP. Psychol. Française 2010, 55, 145–170. [Google Scholar] [CrossRef]
- Prunty, M.M.; Barnett, A.L.; Wilmut, K.; Plumb, M.S. An examination of writing pauses in the handwriting of children with Developmental Coordination Disorder. Res. Dev. Disabil. 2014, 35, 2894–2905. [Google Scholar] [CrossRef]
- Hamstra-Bletz, L.; Blöte, A.W. A Longitudinal Study on Dysgraphic Handwriting in Primary School. J. Learn. Disabil. 1993, 26, 689–699. [Google Scholar] [CrossRef]
- Berninger, V.W. Understanding the “Graphia” in Developmental Dysgraphia. In Developmental Motor Disorders: A Neuropsycho-Logical Perspective; Dewey, D., Tupp.er, D.E., Eds.; Guilford press: New York, NY, USA, 2004; pp. 328–350. [Google Scholar]
- McCloskey, M.; Rapp, B. Developmental dysgraphia: An overview and framework for research. Cogn. Neuropsychol. 2017, 34, 65–82. [Google Scholar] [CrossRef] [PubMed]
- Berninger, V.W.; Abbott, R.D.; Abbott, S.P.; Graham, S.; Todd, R. Writing and reading: Connections between language by hand and language by eye. J. Learn. Disabil. 2002, 35, 39–56. [Google Scholar] [CrossRef]
- Prunty, M.M.; Barnett, A.L. Understanding handwriting difficulties: A comparison of children with and without motor impair-ment. Cogn. Neuropsychol. 2017, 34, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Di Brina, C.; Niels, R.; Overvelde, A.; Levi, G.; Hulstijn, W. Dynamic time warping: A new method in the study of poor hand-writing. Hum. Mov. Sci. 2008, 27, 242–255. [Google Scholar] [CrossRef]
- Rosenblum, S.; Weiss, P.L.; Parush, S. Product and Process Evaluation of Handwriting Difficulties. Educ. Psychol. Rev. 2003, 15, 41–81. [Google Scholar] [CrossRef]
- Engel-Yeger, B.; Nagauker-Yanuv, L.; Rosenblum, S. Handwriting Performance, Self-Reports, and Perceived Self-Efficacy Among Children with Dysgraphia. Am. J. Occup. Ther. 2009, 63, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.; Struck, M.; Santoro, J.; Berninger, V.W. Dimensions of Good and Poor Handwriting Legibility in First and Second Graders: Motor Programs, Visual–Spatial Arrangement, and Letter Formation Parameter Setting. Dev. Neuropsychol. 2006, 29, 43–60. [Google Scholar] [CrossRef] [PubMed]
- Kandel, S.; Lassus-Sangosse, D.; Grosjacques, G.; Perret, C. The impact of developmental dyslexia and dysgraphia on movement production during word writing. Cogn. Neuropsychol. 2017, 34, 219–251. [Google Scholar] [CrossRef] [PubMed]
- Wicki, W.; Lichtsteiner, S.H. Improvement of handwriting automaticity among children treated for graphomotor difficulties over a period of six months. J. Occup. Ther. Sch. Early Interv. 2018, 11, 148–160. [Google Scholar] [CrossRef]
- Hurschler Lichtsteiner, S.; Wicki, W. Kinematische Untersuchung der Handschrift mit STREGA CSWin: Ein Verfahren zur Förderplanung und zur Wirksamkeitsforschung. Empir. Sonderpädagogik 2017, 4, 406–425. [Google Scholar]
- Overvelde, A.; Hulstijn, W. Handwriting development in grade 2 and grade 3 primary school children with normal, at risk, or dysgraphic characteristics. Res. Dev. Disabil. 2011, 32, 540–548. [Google Scholar] [CrossRef]
- Graham, S.; Berninger, V.W.; Abbott, R.D.; Abbott, S.P.; Whitaker, D. Role of mechanics in composing of elementary school stu-dents: A new methodological app.roach. J. Educ. Psychol. 1997, 89, 170–182. [Google Scholar] [CrossRef]
- Prunty, M.M.; Barnett, A.L.; Wilmut, K.; Plumb, M.S. The impact of handwriting difficulties on compositional quality in children with developmental coordination disorder. Br. J. Occup. Ther. 2016, 79, 591–597. [Google Scholar] [CrossRef]
- Graham, S.; Harris, K.R.; Hebert, M. It Is More Than Just the Message: Presentation Effects in Scoring Writing. Focus Except. Child. 2011, 44, 1–12. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.C.M.; Blank, R.; van der Kaay, A.-C.; Mosterd-van der Meijs, R.; Vlugt-van der Brand, E.; Polatajko, H.; Wilson, P.H. Efficacy of interventions to improve motor performance in children with developmental coordination disorder: A combined systematic review and meta-analysis. Dev. Med. Child Neurol. 2013, 55, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Niemeijer, A.S. Neuromotor Task Training: Physiotherapy for Children with Developmental Coordination Disorder. Ph.D. Thesis, Rijkuniversiteit Groningen, Groningen, The Netherlands, 2007. [Google Scholar]
- Schoemaker, M.M.; Niemeijer, A.S.; Reynders, K.; Smits-Engelsman, B.C.M. Effectiveness of Neuromotor Task Training for Chil-dren with Developmental Coordination Disorder: A Pilot Study. Neural Plast. 2003, 10, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Polatajko, H.J.; Mandich, A.D. Enabling Occupation in Children. The Cognitive Orientation to Daily Occupational Performance (CO-OP) Approach; CAOT Publications ACE: Ottawa, ON, USA, 2004. [Google Scholar]
- Henderson, S.E.; Sugden, D.A. Ecological Intervention for Children with Movement Difficulties; Pearson: London, UK, 2007. [Google Scholar]
- Adams, I.L.J.; Lust, J.M.; Steenbergen, B. Development of motor imagery ability in children with developmental coordination disorder–A goal-directed pointing task. Br. J. Psychol. 2018, 109, 187–203. [Google Scholar] [CrossRef]
- Rainer, B.; Sabine, V. Deutsch-Österreichisch-Schweizerische (DACH) Versorgungsleitlinie zu Definition, Diagnostik, Behandlung Und Psychosozialen Aspekten Bei Umschriebenen Entwicklungsstörungen Motorischer Funktionen (UEMF), 2020: Kurzfassung. Available online: https://www.awmf.org/uploads/tx_szleitlinien/022-017k_S3_Umschriebene-Entwicklungsstoerungen-motorischer-Funktionen-UEMF_2020-08_01.pdf (accessed on 1 April 2023).
- Graham, S. Want to improve children’s handwriting? Don’t neglect their handwriting. Am. Educ. 2009, 33, 20–40. [Google Scholar]
- Berninger, V.W.; Vaughan, K.B.; Abbott, R.D.; Abbott, S.P.; Rogan, L.W.; Brooks, A.; Reed, E.; Graham, S. Treatment of hand-writing problems in beginning writers: Transfer from handwriting to composition. J. Educ. Psychol. 1997, 89, 652–666. [Google Scholar] [CrossRef]
- Fuchs, M. Grafomotoriktherapie Mit Jüngeren undmit älteren Kindern-Eine Fallstudie. Bachelor’s Thesis, University of Teacher Education in Special Needs, Zürich, Switzerland, 2010. [Google Scholar]
- Jongmans, M.J.; Linthorst-Bakker, E.; Westenberg, Y.; Smits-Engelsman, B.C. Use of a task-oriented self-instruction method to supp.ort children in primary school with poor handwriting quality and speed. Hum. Mov. Sci. 2003, 22, 549–566. [Google Scholar] [CrossRef]
- Vetter, M. Bildungspolitische Entwicklungen in der Schweiz und die Organisation des Angebotes der Psychomotorik in der Stadt Zürich: Ein nachahmenswerter Prozess? Motorik 2016, 39, 19–24. [Google Scholar] [CrossRef]
- Kuhlenkamp, S. Lehrbuch Psychomotorik; Ernst Reinhardt: München, Germany, 2017. [Google Scholar]
- Eggert, D.; Lütje-Klose, B. Theorie und Praxis der psychomotorischen Förderung, 7th ed.; verb. Aufl.; Borgmann: Dortmund, Germany, 2008; ISBN 3861453029. [Google Scholar]
- Zimmer, R. Handbuch Der Psychomotorik. Theorie Und Praxis Der Psychomotorischen Förderung Von Kindern; Herder: Freiburg i.B., Germany, 2010. [Google Scholar]
- Vetter, M.; Sandmeier, A. Psychomotricity: Effects of psychomotor interventions from the perspective of teachers. Eur. Psychomot. J. 2020, 12, 30–42. [Google Scholar]
- Häusler, M. Spielen, zeichnen, schreiben. Grafomotorik-das Schreibenlernen verstehen, Lernschwierigkeiten behandeln. In Psychomotorik-Therapie Und Individuelle Entwicklung; Buchmann, T., Ed.; Schweizerische Zentralstelle für Heilpädagogik (SZH): Luzern, Switzerland, 2007; pp. 21–23. [Google Scholar]
- Hurschler Lichtsteiner, S. Erfahrungen mit der Basisschrift. Eine grosse Erleichterung-und wie weiter? Die Grund. 2013, 265–266, 28–31. [Google Scholar]
- Sturm, A.; Nänny, R.; Wyss, S. Entwicklung hierarchieniedriger Schreibprozesse. In Handbuch Schriftspracherwerb Und Weiterführendes Lesen Und Schreiben; Philipp, M., Ed.; Beltz Juventa: Weinheim, Germany, 2017; pp. 84–104. ISBN 978-3-7799-3130-0. [Google Scholar]
- Jucker, D. Die Professionalisierung Der Psychomotoriktherapie in Der Deutschschweiz. Ph.D. Thesis, Universität Zürich, Zürich, Germany, 2012. [Google Scholar]
- Buchmann, T. Entwicklung des Kindes durch Bewegung fördern. In Psychomotorik-Therapie Und Individuelle Entwicklung; Buchmann, T., Ed.; Schweizerische Zentralstelle für Heilpädagogik (SZH): Luzern, Switzerland, 2007; p. 97. [Google Scholar]
- Kranz, I.; Sammann, K.; Amft, S.; Vetter, M. Effekte einer grafomotorisch ausgerichteten psychomotorischen Intervention bei Kindern im Vorschulalter. Psychol. Erzieh. Unterr. 2011, 58, 139–151. [Google Scholar] [CrossRef]
- Avet L’Oiseau-Tissot, S.; Senn, B.; Balligand Lecompte, K. Evaluation des effets de la thérapie psychomotrice: Résultats de recherche principaux. Rev. Suisse Pédagogie Spécialisée 2011, 2, 48–53. [Google Scholar]
- Hoy, M.M.P.; Egan, M.; Feder, K.P. A Systematic Review of Interventions to Improve Handwriting. Can. J. Occup. Ther. 2011, 78, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Wyss, S.; Hurschler Lichtsteiner, S.; Wicki, W. Wirksamkeit der Psychomotoriktherapie: Sekundäranalyse Therapieziele und Protokolle. Zwischenbericht. Forschungsgrupp.e Sprachen und Schrift. 2022. Available online: https://www.phlu.ch/7050 (accessed on 1 May 2023).
- Petermann, F. Movement Assessment Battery for Children-2 (M-ABC-2; Deutsche Version); Pearson Assessment: Frankfurt/M, Germany, 2009. [Google Scholar]
- Wilson, B.N.; Crawford, S.G.; Green, D.; Roberts, G.; Aylott, A.; Kaplan, B.J. Psychometric Properties of the Revised Developmental Coordination Disorder Questionnaire. Phys. Occup. Ther. Pediatr. 2009, 29, 182–202. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.N.; Rodger, S.; Mickan, S.; Kennedy-Behr, A. Cross-Cultural Adaptation of the Developmental Coordination Disorder Questionnaire 2007 for German-Speaking Countries: DCDQ-G. Neuropediatrics 2013, 44, 245–251. [Google Scholar] [CrossRef]
- Marquardt, C. CSWin DTW. Computerunterstützte Analyse Der Bewegungsabläufe Beim Schreiben. Bedienungshandbuch; Verlag MedCom: München, Germany, 2020. [Google Scholar]
- Marquardt, C.; Di Brina, C.; Hurschler Lichtsteiner, S.; Nideröst, M.; Wicki, W. CSWin DTW Plugin; Pädagogische Hochschule Luzern: Luzern, Switzerland, 2021. [Google Scholar]
- Marquardt, C.; Mai, N. A computational procedure for movement analysis in handwriting. J. Neurosci. Methods 1994, 52, 39–45. [Google Scholar] [CrossRef]
- Lichtsteiner, S.H.; Wicki, W.; Falmann, P. Impact of handwriting training on fluency, spelling and text quality among third graders. Read. Writ. 2018, 31, 1295–1318. [Google Scholar] [CrossRef] [PubMed]
- Blank, R.; Jenetzky, E.; Vinçon, S. Bruininks-Oseretzky Test Der Motorischen Fähigkeiten. 2. Ausgabe. Deutschsprachige Version; Pearson: Frankfurt a.M., Germany, 2014. [Google Scholar]
- Bruininks, R.H.; Bruininks, B.D. Brunininks-Oseretsky Test of Motor Proficiency (BOT-2), 2nd ed.; Pearson Assessment: Minneapolis, MN, USA, 2005. [Google Scholar]
- Mai, N.; Marquardt, C. CSWin-Computergestützte Analyse Der Bewegungsabläufe Beim Schreiben. Bedienungshandbuch; MedCom: München, Germany, 2007. [Google Scholar]
- Freund, H.J.; Büttner, U.; Cohen, B.; Noth, J. Time Control of Hand Movements. Prog. Brain Res. 1986, 64, 287–294. [Google Scholar]
- Niels, R. Allograph Based Writer Identification, Handwriting Analysis and Character Recognition. Ph.D. Thesis, Radboud University Nijmegen, Nijmegen, The Netherlands, 2010. [Google Scholar]
- Vuori, V. Adaptive Methods for Online Recognition of Isolated Handwritten Characters. Ph.D. Thesis, University of Technology Helsinki, Helsinki, Finland, 2002. [Google Scholar]
- Hurschler, S.; Saxer, A.; Wicki, W. Schreibmotorische Leistungen Im Frühen Primarschulalter in Abhängigkeit Vom Unterrichteten Schrifttyp. Forschungsbericht Nr. 18 Der Pädagogischen Hochschule Zentralschweiz, Luzern; PHZ Luzern: Luzern, Switzerland, 2008. [Google Scholar]
- Hubbard, A.E.; Ahern, J.; Fleischer, N.L.; van der Laan, M.; Lippman, S.A.; Jewell, N.; Bruckner, T.; Satariano, W.A. To GEE or not to GEE: Comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology 2010, 21, 467–474. [Google Scholar] [CrossRef]
- Ghisletta, P.; Spini, D. An Introduction to Generalized Estimating Equations and an Application to Assess Selectivity Effects in a Longitudinal Study on Very Old Individuals. J. Educ. Behav. Stat. 2004, 29, 421–437. [Google Scholar] [CrossRef]
- López-Escribano, C.; Martín-Babarro, J.; Pérez-López, R. Promoting Handwriting Fluency for Preschool and Elementary-Age Students: Meta-Analysis and Meta-Synthesis of Research From 2000 to 2020. Front. Psychol. 2022, 13, 841573. [Google Scholar] [CrossRef]
- Tucha, O.; Lange, K.W. The Effect of Conscious Control on Handwriting in Children with Attention Deficit Hyperactivity Disorder. J. Atten. Disord. 2005, 9, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Jenni, O. Die Kindliche Entwicklung Verstehen: Praxiswissen über Phasen und Störungen, 1st ed.; Springer: Berlin/Heidelberg, Germany, 2021; ISBN 9783662624470. [Google Scholar]
- Pellegrini, A.D.; Huberty, P.D.; Jones, I. The Effects of Recess Timing on Children’s Playground and Classroom Behaviors. Am. Educ. Res. J. 1995, 32, 845. [Google Scholar] [CrossRef]
- Hurschler Lichtsteiner, S. Übst du noch oder schreibst du schon? Eine Untersuchung zum Handschrifterwerb in der zweiten Klasse mit Anregungen für den Unterricht. In Schreibunterricht-Schreibdidaktische Perspektiven auf Medien, Flüssigkeit, Impulse, Arrangements und Diagnostik; Kruse, N., Lemke, V., Steinhoff, T., Sturm, A., Eds.; Waxmann: München, Germany, 2023; in press. [Google Scholar]
- McCutchen, D. Knowledge, Processing, and Working Memory: Implications for a Theory of Writing. Educ. Psychol. 2000, 35, 13–23. [Google Scholar] [CrossRef]
- Ruploh, B.; Martzy, F.; Bischoff, A.; Matschulat, N.; Zimmer, R. Veränderungen im Selbstkonzept nach psychomotorischer Förderung: Eine Pilotstudie im Mixed Methods Design. Motorik 2013, 36, 180–189. [Google Scholar] [CrossRef]
- Fischer, K. Einführung in die Psychomotorik: Mit 11 Tabellen, 3rd ed.; überarb. und erw. Aufl.; Reinhardt; UTB: München, Germany; Stuttgart, Germany, 2009; ISBN 9783497019915. [Google Scholar]
- Marsh, H.W. Self-Concept Theory, Measurement and Research into Practice: The Role of Self-Concept in Educational Psychology; British Psychological Society: Leicester, UK, 2006; ISBN 9781854334480. [Google Scholar]



| Therapy Group | Control Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | n | % | n | % | n | % | χ2 | p |
| 121 | 100 | 61 | 50.4 | 60 | 49.6 | |||
| Sex | 0.068 | n.s. | ||||||
| -Female | 31 | 25.6 | 15 | 24.6 | 16 | 26.7 | ||
| -Male | 90 | 74.4 | 46 | 75.4 | 44 | 73.3 | ||
| Handedness | 0.743 | n.s. | ||||||
| -Righthanders | 106 | 87.6 | 55 | 90.2 | 51 | 85 | ||
| -Lefthanders | 15 | 12.4 | 6 | 9.8 | 9 | 15 | ||
| Diagnosis | 0.752 | n.s. | ||||||
| -DCD | 42 | 34.7 | 22 | 36.1 | 20 | 33.3 | ||
| -DD | 79 | 65.3 | 39 | 63.9 | 40 | 66.7 | ||
| Class | 0.089 | n.s. | ||||||
| -First graders | 48 | 39.7 | 25 | 41 | 23 | 38.3 | ||
| -Second graders | 73 | 60.3 | 36 | 59 | 37 | 61.7 | ||
| Item No. | Task | Item No. | Task |
|---|---|---|---|
| 1 | Scribbling (for trying out, not evaluated) | 8 | Repetitive letter sequences (writing at least 8 times the letter “a”, no speed specification) |
| 2 | Finger movements (no speed specification) | 9 | Repetitive letter sequences (writing at least 8 times the letter “a”, as fast as possible) |
| 3 | Finger movements (fast) | 10 | Repetitive letter sequences (writing at least 8 times the letter “a”, as precisely as possible) |
| 4 | Wrist movements (no speed specification) | 11 | Patterns (garlands) |
| 5 | Wrist movements (fast) | 12 | Patterns (double loops) |
| 6 | Combined finger and wrist movements when circling (no speed specification) | 13 | Copying the word “neu” (new) three times |
| 7 | Combined finger and wrist movements when circling (fast) | 14 | Copying a sentence “Die Kinder fliegen nach Amerika” (”The children fly to America”, no speed specification) |
| 15 | Copying a sentence “Die Kinder fliegen nach Amerika” (“The children fly to America”, fast). |
| Therapy Group | Control Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| DD | DCD | DD | DCD | Time | Group | Diagnosis | Time × Group | Time × Diagnosis | |
| Measures | M | M | M | M | F | F | F | F | F |
| (SD) | (SD) | (SD) | (SD) | df | df | df | df | df | |
| Eta2 | Eta2 | Eta2 | Eta2 | Eta2 | |||||
| p | p | p | p | p | |||||
| t1 | 39.4 | 31.65 | 37.41 | 33.79 | 2.699 | 7.19 | 7.563 | 28.74 | 3.082 |
| (1.43) | (1.89) | (1.41) | (1.96) | 1/108 | 1/108 | 1/108 | 1/108 | 1/108 | |
| t5 | 45.81 | 40.38 | 34.98 | 34.64 | 0.024 | 0.062 | 0.065 | 0.21 | 0.028 |
| (1.49) | (1.96) | (1.46) | (2.04) | n.s. | 0.008 | 0.007 | 0 | 0.082 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hurschler Lichtsteiner, S.; Nideröst, M.; Di Brina, C.; Marquardt, C.; Wyss, S.; Buholzer, A.; Wicki, W. Effectiveness of Psychomotor Therapy among Children with Graphomotor Impairment with and without DCD-Diagnosis. Children 2023, 10, 964. https://doi.org/10.3390/children10060964
Hurschler Lichtsteiner S, Nideröst M, Di Brina C, Marquardt C, Wyss S, Buholzer A, Wicki W. Effectiveness of Psychomotor Therapy among Children with Graphomotor Impairment with and without DCD-Diagnosis. Children. 2023; 10(6):964. https://doi.org/10.3390/children10060964
Chicago/Turabian StyleHurschler Lichtsteiner, Sibylle, Melanie Nideröst, Carlo Di Brina, Christian Marquardt, Stefanie Wyss, Alois Buholzer, and Werner Wicki. 2023. "Effectiveness of Psychomotor Therapy among Children with Graphomotor Impairment with and without DCD-Diagnosis" Children 10, no. 6: 964. https://doi.org/10.3390/children10060964
APA StyleHurschler Lichtsteiner, S., Nideröst, M., Di Brina, C., Marquardt, C., Wyss, S., Buholzer, A., & Wicki, W. (2023). Effectiveness of Psychomotor Therapy among Children with Graphomotor Impairment with and without DCD-Diagnosis. Children, 10(6), 964. https://doi.org/10.3390/children10060964