
Comparison between Nasopharyngeal and Saliva Samples for the Detection of Respiratory Viruses in Children with Acute Lower Respiratory Tract Infections: A Pilot Study

 ,
,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population
2.3. Respiratory Specimen Collection
- Age (months), sex, and ethnicity;
- NSP, date, and result;
- Salivary swab, date, and result;
- Amount of saliva collected;
- Comorbidities;
- Asymptomatic/symptomatic;
- Presence of fever, cough, or respiratory distress;
- Need of oxygen support or not;
2.4. Pathogen Analysis
2.5. Statistical Analysis Plan
2.5.1. Sample Size Calculation
2.5.2. Statistical Analysis
3. Results
3.1. Study Population
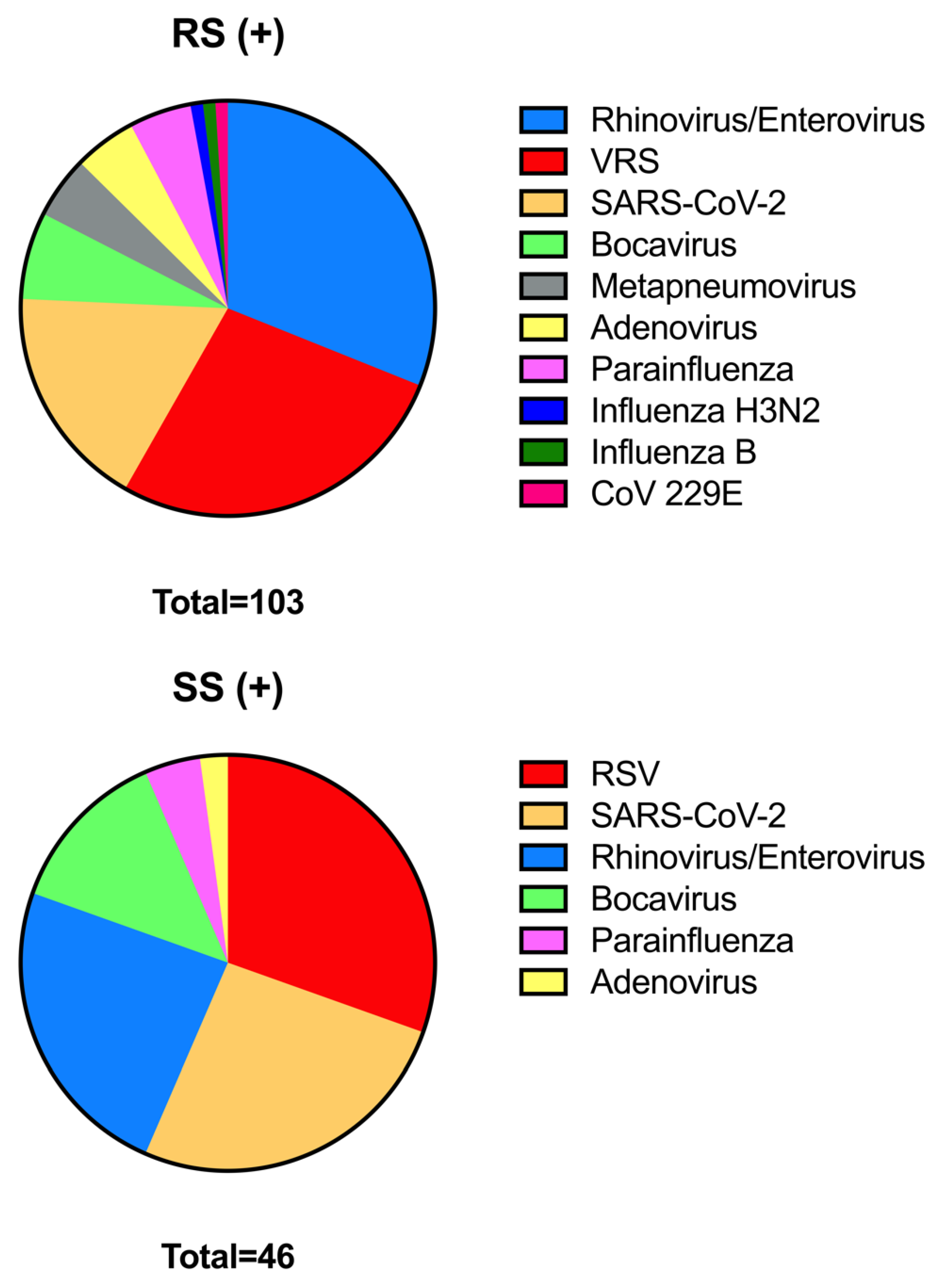
3.2. Comparison of Molecolar Results between Nasopharyngeal Swabs and Sputum Specimens
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Binns, E.; Koenraads, M.; Hristeva, L.; Flamant, A.; Baier-Grabner, S.; Loi, M.; Lempainen, J.; Osterheld, E.; Ramly, B.; Chakakala-Chaziya, J.; et al. Influenza and respiratory syncytial virus during the COVID-19 pandemic: Time for a new paradigm? Pediatr. Pulmonol. 2022, 57, 38–42. [Google Scholar] [CrossRef]
- Smith-Vaughan, H.C.; Binks, M.J.; Beissbarth, J.; Chang, A.B.; McCallum, G.B.; Mackay, I.M.; Morris, P.S.; Marsh, R.L.; Torzillo, P.J.; Wurzel, D.F.; et al. Bacteria and viruses in the nasopharynx immediately prior to onset of acute lower respiratory infections in Indigenous Australian children. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention, 14 Giugno 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/naats.html (accessed on 15 April 2023).
- Noureddine, F.Y.; Chakkour, M.; El Roz, A.; Reda, J.; Al Sahily, R.; Assi, A.; Joma, M.; Salami, H.; Hashem, S.J.; Harb, B.; et al. The Emergence of SARS-CoV-2 Variant(s) and Its Impact on the Prevalence of COVID-19 Cases in the Nabatieh Region, Lebanon. Med. Sci. 2021, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Connor, M.C.; Copeland, M.; Curran, T. Investigation of saliva, tongue swabs and buccal swabs as alternative specimen types to nasopharyngeal swabs for SARS-CoV-2 testing. J. Clin. Virol. 2021, 146, 105053. [Google Scholar] [CrossRef]
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of Saliva, Oropharyngeal Swabs, and Nasal Swabs for SARS-CoV-2 Molecular Detection: A Systematic Review and Meta-analysis. J. Clin. Microbiol. 2021, 59, e02881-20. [Google Scholar] [CrossRef]
- Camporesi, A.; Morello, R.; Ferro, V.; Pierantoni, L.; Rocca, A.; Lanari, M.; Trobia, G.L.; Sciacca, T.; Bellinvia, A.G.; De Ferrari, A.; et al. Epidemiology, Microbiology and Severity of Bronchiolitis in the First Post-Lockdown Cold Season in Three Different Geographical Areas in Italy: A Prospective, Observational Study. Children 2022, 9, 491. [Google Scholar] [CrossRef]
- Vogels, C.B.; Watkins, A.E.; Harden, C.A.; Brackney, D.E.; Shafer, J.; Wang, J.; Caraballo, C.; Kalinich, C.C.; Ott, I.M.; Fauver, J.R.; et al. SalivaDirect: A simplified and flexible platform to enhance SARS-CoV-2 testing capacity. Med 2021, 2, 263–280. [Google Scholar] [CrossRef]
- Mostafa, H.H.; Hardick, J.; Morehead, E.; Miller, J.A.; Gaydos, C.A.; Manabe, Y.C. Comparison of the analytical sensitivity of seven commonly used commercial SARS-CoV-2 automated molecular assays. J. Clin. Virol. 2020, 130, 104578. [Google Scholar] [CrossRef]
- Boers, S.A.; Melchers, W.J.G.; Peters, C.J.A.; Toonen, M.; McHugh, M.P.; Templeton, K.E.; Claas, E.C.J. Multicenter Evaluation of QIAstat-Dx Respiratory Panel V2 for Detection of Viral and Bacterial Respiratory Pathogens. J. Clin. Microbiol. 2020, 58, e01793-19. [Google Scholar] [CrossRef] [PubMed]
- Qiagen. QIAstat-Dx Respirtatroy Panel Instructions for Use (Handbook); Qiagen: Barcelona, Spain, 2019. [Google Scholar]
- Kanwar, N.; Banerjee, D.; Sasidharan, A.; Abdulhamid, A.; Larson, M.; Lee, B.; Selvarangan, R.; Liesman, R.M. Comparison of diagnostic performance of five molecular assays for detection of SARS-CoV-2. Diagn. Microbiol. Infect. Dis. 2021, 101, 115518. [Google Scholar] [CrossRef]
- Trémeaux, P.; Lhomme, S.; Abravanel, F.; Raymond, S.; Mengelle, C.; Mansuy, J.-M.; Izopet, J. Evaluation of the Aptima™ transcription-mediated amplification assay (Hologic®) for detecting SARS-CoV-2 in clinical specimens. J. Clin. Virol. 2020, 129, 104541. [Google Scholar] [CrossRef]
- Birkett, M.A.; Day, S.J. Internal pilot studies for estimating sample size. Stat. Med. 1994, 13, 2455–2463. [Google Scholar] [CrossRef]
- Guido, M.; Tumolo, M.R.; Verri, T.; Romano, A.; Serio, F.; De Giorgi, M.; De Donno, A.; Bagordo, F.; Zizza, A. Human bocavirus: Current knowledge and future challenges. World J. Gastroenterol. 2016, 22, 8684–8697. [Google Scholar] [CrossRef] [PubMed]
- Martin, E.T.; Taylor, J.; Kuypers, J.; Magaret, A.; Wald, A.; Zerr, D.; Englund, J.A. Detection of bocavirus in saliva of children with and without respiratory illness. J. Clin. Microbiol. 2009, 47, 4131–4132. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Li, Y.; Gan, F.; Du, Y.; Yao, Y. Salivary Glands: Potential Reservoirs for COVID-19 Asymptomatic Infection. J. Dent. Res. 2020, 99, 989. [Google Scholar] [CrossRef] [PubMed]
- Azzi, L.; Carcano, G.; Gianfagna, F.; Grossi, P.; Gasperina, D.D.; Genoni, A.; Fasano, M.; Sessa, F.; Tettamanti, L.; Carinci, F.; et al. Saliva is a reliable tool to detect SARS-CoV-2. J. Infect. 2020, 81, e45–e50. [Google Scholar] [CrossRef]
- Yokota, I.; Shane, P.Y.; Okada, K.; Unoki, Y.; Yang, Y.; Inao, T.; Sakamaki, K.; Iwasaki, S.; Hayasaka, K.; Sugita, J.; et al. Mass Screening of Asymptomatic Persons for Severe Acute Respiratory Syndrome Coronavirus 2 Using Saliva. Clin. Infect. Dis. 2021, 73, e559–e565. [Google Scholar] [CrossRef]
- Fukumoto, T.; Iwasaki, S.; Fujisawa, S.; Hayasaka, K.; Sato, K.; Oguri, S.; Taki, K.; Nakakubo, S.; Kamada, K.; Yamashita, Y.; et al. Efficacy of a novel SARS-CoV-2 detection kit without RNA extraction and purification. Int. J. Infect. Dis. 2020, 98, 16–17. [Google Scholar] [CrossRef]
- Kim, S.E.; Lee, J.Y.; Lee, A.; Kim, S.; Park, K.-H.; Jung, S.-I.; Kang, S.-J.; Oh, T.H.; Kim, U.J.; Lee, S.Y.; et al. Viral Load Kinetics of SARS-CoV-2 Infection in Saliva in Korean Patients: A Prospective Multi-center Comparative Study. J. Korean Med. Sci. 2020, 35, e287. [Google Scholar] [CrossRef]
- Landry, M.L.; Criscuolo, J.; Peaper, D.R. Challenges in use of saliva for detection of SARS-CoV-2 RNA in symptomatic outpatients. J. Clin. Virol. 2020, 130, 104567. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.; Rashid, F.A.; Sabri, F.S.; Jamil, N.N.; Zain, R.; Hashim, R.; Amran, F.; Kok, H.T.; Samad, M.A.; Ahmad, N. Comparing Nasopharyngeal Swab and Early Morning Saliva for the Identification of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2021, 72, e352–e356. [Google Scholar] [CrossRef]
- Williams, E.; Bond, K.; Zhang, B.; Putland, M.; Williamson, D.A. Saliva as a Noninvasive Specimen for Detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e00776-20. [Google Scholar] [CrossRef]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Warren, J.L.; Geng, B.; Muenker, M.C.; Moore, A.J.; et al. Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 1283–1286. [Google Scholar] [CrossRef]
- Jamal, A.J.; Mozafarihashjin, M.; Coomes, E.; Anceva-Sami, S.; Barati, S.; Crowl, G.; Faheem, A.; Farooqi, L.; Kandel, C.E.; Khan, S.; et al. Sensitivity of midturbinate versus nasopharyngeal swabs for the detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Infect. Control Hosp. Epidemiol. 2021, 42, 1001–1003. [Google Scholar] [CrossRef] [PubMed]
- Migueres, M.; Vellas, C.; Abravanel, F.; Da Silva, I.; Dimeglio, C.; Ferrer, V.; Raymond, S.; Mansuy, J.-M.; Izopet, J. Testing individual and pooled saliva samples for SARS-CoV-2 nucleic acid: A prospective study. Diagn. Microbiol. Infect. Dis. 2021, 101, 115478. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.; Tosif, S.; Lee, L.; Costa, A.; Bartel, C.; Last, K.; Clifford, V.; Daley, A.; Allard, N.; Orr, C.; et al. Adding saliva testing to oropharyngeal and deep nasal swab testing increases PCR detection of SARS-CoV-2 in primary care and children. Med. J. Aust. 2021, 215, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D.; Sasidharan, A.; Abdulhamid, A.; Orosco, E.M.; Watts, J.L.; E Schuster, J.; Myers, A.L.; Weddle, G.; Selvarangan, R. Diagnostic Yield of Saliva for SARS-CoV-2 Molecular Testing in Children. J. Pediatr. Infect. Dis. Soc. 2021, 10, 967–969. [Google Scholar] [CrossRef]
- Huber, M.; Schreiber, P.W.; Scheier, T.; Audigé, A.; Buonomano, R.; Rudiger, A.; Braun, D.L.; Eich, G.; Keller, D.I.; Hasse, B.; et al. High Efficacy of Saliva in Detecting SARS-CoV-2 by RT-PCR in Adults and Children. Microorganisms 2021, 9, 642. [Google Scholar] [CrossRef]
- Yee, R.; Truong, T.T.; Pannaraj, P.S.; Eubanks, N.; Gai, E.; Jumarang, J.; Turner, L.; Peralta, A.; Lee, Y.; Bard, J.D. Saliva Is a Promising Alternative Specimen for the Detection of SARS-CoV-2 in Children and Adults. J. Clin. Microbiol. 2021, 59, e02686-20. [Google Scholar] [CrossRef]
- Chong, C.Y.; Kam, K.-Q.; Li, J.; Maiwald, M.; Loo, L.H.; Nadua, K.D.; Tan, N.W.H.; Yung, C.F.; Thoon, K.C. Saliva Is Not a Useful Diagnostic Specimen in Children with Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, e3144–e3145. [Google Scholar] [CrossRef] [PubMed]
- Han, M.S.; Seong, M.-W.; Kim, N.; Shin, S.; Cho, S.I.; Park, H.; Kim, T.S.; Park, S.S.; Choi, E.H. Viral RNA Load in Mildly Symptomatic and Asymptomatic Children with COVID-19, Seoul, South Korea. Emerg. Infect. Dis. 2020, 26, 2497–2499. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, G.; Massimo, C.; Gianni, P.; Rossolini, G.M. Principi di Microbiologia Medica; Unico, Casa Editrice Ambrosiana: Rozzano, Italy, 2017; p. 928. [Google Scholar]
- Knipe, D.M.; Howley, P.M. (Eds.) Fields Virology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; Volume 1, pp. 2395–2426. [Google Scholar]
- Kim, Y.-G.; Yun, S.G.; Kim, M.Y.; Park, K.; Cho, C.H.; Yoon, S.Y.; Nam, M.H.; Lee, C.K.; Cho, Y.-J.; Lim, C.S. Comparison between Saliva and Nasopharyngeal Swab Specimens for Detection of Respiratory Viruses by Multiplex Reverse Transcription-PCR. J. Clin. Microbiol. 2016, 55, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Galar, A.; Catalán, P.; Vesperinas, L.; Miguens, I.; Muñoz, I.; García-Espona, A.; Sevillano, J.A.; Andueza, J.A.; Bouza, E.; Muñoz, P. Use of Saliva Swab for Detection of Influenza Virus in Patients Admitted to an Emergency Department. Microbiol. Spectr. 2021, 9, e0033621. [Google Scholar] [CrossRef]
- Sueki, A.; Matsuda, K.; Yamaguchi, A.; Uehara, M.; Sugano, M.; Uehara, T.; Honda, T. Evaluation of saliva as diagnostic materials for influenza virus infection by PCR-based assays. Clin. Chim. Acta 2016, 453, 71–74. [Google Scholar] [CrossRef]
- Bilder, L.; Machtei, E.E.; Shenhar, Y.; Kra-Oz, Z.; Basis, F. Salivary detection of H1N1 virus: A clinical feasibility investigation. J. Dent. Res. 2011, 90, 1136–1139. [Google Scholar] [CrossRef]
- To, K.K.W.; Yip, C.C.Y.; Lai, C.Y.W.; Wong, C.K.H.; Ho, D.T.Y.; Pang, P.K.P.; Ng, A.C.K.; Leung, K.-H.; Poon, R.W.S.; Chan, K.-H.; et al. Saliva as a diagnostic specimen for testing respiratory virus by a point-of-care molecular assay: A diagnostic validity study. Clin. Microbiol. Infect. 2019, 25, 372–378. [Google Scholar] [CrossRef]
- Robinson, J.L.; Lee, B.E.; Kothapalli, S.; Craig, W.; Fox, J.D. Use of throat swab or saliva specimens for detection of respiratory viruses in children. Clin. Infect. Dis. 2008, 46, e61–e64. [Google Scholar] [CrossRef]
- Mackie, D.A.; Pangborn, R.M. Mastication and its influence on human salivary flow and alpha-amylase secretion. Physiol. Behav. 1990, 47, 593–595. [Google Scholar] [CrossRef]
- Woda, A.; Foster, K.; Mishellany, A.; Peyron, M.A. Adaptation of healthy mastication to factors pertaining to the individual or to the food. Physiol. Behav. 2006, 89, 28–35. [Google Scholar] [CrossRef]
- Macknin, M.L.; Piedmonte, M.; Jacobs, J.; Skibinski, C. Symptoms associated with infant teething: A prospective study. Pediatrics 2000, 105 Pt 1, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.; Sørensen, C.E.; Proctor, G.B.; Carpenter, G.H. Salivary functions in mastication, taste and textural perception, swallowing and initial digestion. Oral. Dis. 2018, 24, 1399–1416. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Number of Patients | 83 |
| Gender (n, %) | |
| Male | 39 (47%) |
| Female | 44 (53%) |
| Age, months (median, IQR) | 12 (30) |
| Ethnicity (n, %) | |
| Caucasian | 68 (81.9%) |
| Asian | 8 (9.6%) |
| African | 3 (3.6%) |
| Hispanic | 4 (4.8%) |
| Swab type (n, %) | |
| Nasopharyngeal | 79 (95.2%) |
| Nasal | 4 (4.8%) |
| Comorbidities (n, %) | 17 (20.5%) |
| Isolation of more than one virus at NSP (n, %) | 17 (20.5%) |
| Isolation of more than one virus at salivar swab (n, %) | 5 (6%) |
| Salivary swab result (n, %) | |
| Positive | 41 (49.4%) |
| Negative | 42 (50.6%) |
| Paired | Samples | |
|---|---|---|
| 83 | ||
| Nasopharingeal swab | Salivary swab | |
| Rhinovirus/Enterovirus | ||
| positive | 32 (38.6%) | 11 (13.3%) |
| negative | 51 (61.4%) | 72 (86.7%) |
| RSV 1 | ||
| positive | 28 (33.7%) | 14 (16.9%) |
| negative | 55 (66.3%) | 69 (83.1%) |
| Bocavirus | ||
| positive | 7 (8.4%) | 6 (7.2%) |
| negative | 76 (91.6%) | 77 (92.8%) |
| SARS-CoV-2 | ||
| positive | 18 (21.7%) | 12 (14.5%) |
| negative | 65 (78.3%) | 71 (85.5%) |
| Influenza B | ||
| positive | 1 (1.2%) | 0 |
| negative | 82 (98.8%) | 83 (100%) |
| Adenovirus | ||
| positive | 5 (6%) | 1 (1.2%) |
| negative | 78 (94%) | 82 (98.8%) |
| CoV 2 229E | ||
| positive | 1 (1.2%) | 0 |
| negative | 82 (98.8%) | 83 (100%) |
| Metapneumovirus | ||
| positive | 5 (6%) | 0 |
| negative | 78 (94%) | 83 (100%) |
| Parainfluenza | ||
| positive | 5 (6%) | 2 (2.4%) |
| negative | 78 (94%) | 81 (97.6%) |
| Influenza H3N2 | ||
| positive | 1 (1.2%) | 0 |
| negative | 82 (98.8%) | 83 (100%) |
| PPV 1 | NPV 2 | Sensitivity | Specificity | |
|---|---|---|---|---|
| Salivary swab | 49.40% * | |||
| Rhinovirus/Enterovirus | 81.82% | 68.06% | 28.13% | 96.08% |
| RSV 3 | 92.86% | 78.26% | 46.43% | 98.18% |
| Bocavirus | 83.33% | 97.40% | 71.43% | 98.68% |
| SARS-CoV-2 | 100.00% | 91.55% | 66.67% | 100.00% |
| Influenza B | 98.80% | 0.00% | 100.00% | |
| Adenovirus | 0.00% | 93.90% | 0.00% | 98.72% |
| CoV 4 229E | 98.80% | 0.00% | 100.00% | |
| Metapneumovirus | 93.98% | 0.00% | 100.00% | |
| Parainfluenzae | 100.00% | 96.30% | 40.00% | 100.00% |
| Influenza H3N2 | 98.80% | 0.00% | 100.00% |
| Negative Salivary Swab | Positive Salivary Swab | p 1 | |
|---|---|---|---|
| N = 42 | N = 41 | ||
| Age (median, IQR) | 8.5 (15.25) | 23 (34) | 0.001 |
| Age < 12 months (n, %) | 23 (54.8%) | 15 (36.6%) | 0.097 |
| Age < 6 months (n, %) | 19 (45.2%) | 7 (17.1%) | 0.006 |
| Gender (n, %) | |||
| Male | 20 (47.6%) | 19 (46.3%) | |
| Female | 22 (52.4%) | 22 (53.7%) | 0.9 |
| Days between RS 2-SS 3 | |||
| (median, IQR) | 2 (2) | 2 (3) | 0.68 |
| Amount of saliva collected (microliters) | |||
| (median, IQR) | 0 (213) | 300 (100) | <0.001 |
| Fever (n, %) | 27 (64.3%) | 32 (78%) | 0.17 |
| Cough (n, %) | 30 (71.4%) | 35 (85.4%) | 0.12 |
| Respiratory distress (n, %) | 24 (57.1%) | 27 (65.9%) | 0.41 |
| Rhinitis (n, %) | 2 (4.8%) | 1 (2.4%) | 1 |
| Comorbidities (n, %) | 5 (11.9%) | 12 (29.3%) | 0.05 |
| Sample | Nasopharingeal Swab | |||
|---|---|---|---|---|
| Positive (+) | Negative (−) | |||
| Salivary swab | Positive (+) | 41 | 0 | 41 |
| Negative (−) | 42 | 0 | 42 | |
| 83 | 0 | 83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buonsenso, D.; Valentini, P.; Mariani, F.; Di Noi, S.; Mazza, S.; Palucci, I.; Sanguinetti, M.; Sali, M. Comparison between Nasopharyngeal and Saliva Samples for the Detection of Respiratory Viruses in Children with Acute Lower Respiratory Tract Infections: A Pilot Study. Children 2023, 10, 899. https://doi.org/10.3390/children10050899
Buonsenso D, Valentini P, Mariani F, Di Noi S, Mazza S, Palucci I, Sanguinetti M, Sali M. Comparison between Nasopharyngeal and Saliva Samples for the Detection of Respiratory Viruses in Children with Acute Lower Respiratory Tract Infections: A Pilot Study. Children. 2023; 10(5):899. https://doi.org/10.3390/children10050899
Chicago/Turabian StyleBuonsenso, Danilo, Piero Valentini, Francesco Mariani, Silvia Di Noi, Sofia Mazza, Ivana Palucci, Maurizio Sanguinetti, and Michela Sali. 2023. "Comparison between Nasopharyngeal and Saliva Samples for the Detection of Respiratory Viruses in Children with Acute Lower Respiratory Tract Infections: A Pilot Study" Children 10, no. 5: 899. https://doi.org/10.3390/children10050899
APA StyleBuonsenso, D., Valentini, P., Mariani, F., Di Noi, S., Mazza, S., Palucci, I., Sanguinetti, M., & Sali, M. (2023). Comparison between Nasopharyngeal and Saliva Samples for the Detection of Respiratory Viruses in Children with Acute Lower Respiratory Tract Infections: A Pilot Study. Children, 10(5), 899. https://doi.org/10.3390/children10050899