
The Benefit of a Retrospective Pregnancy Anamnesis in Child and Adolescent Psychiatry: The Reliability of Maternal Self-Report during Childhood Development

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Characteristics
2.2. Prenatal and Retrospective Self-Report
2.3. Statistical Analyses
3. Results
3.1. Alcohol Consumption
3.2. Smoking Behaviour
3.3. Complications during Pregnancy
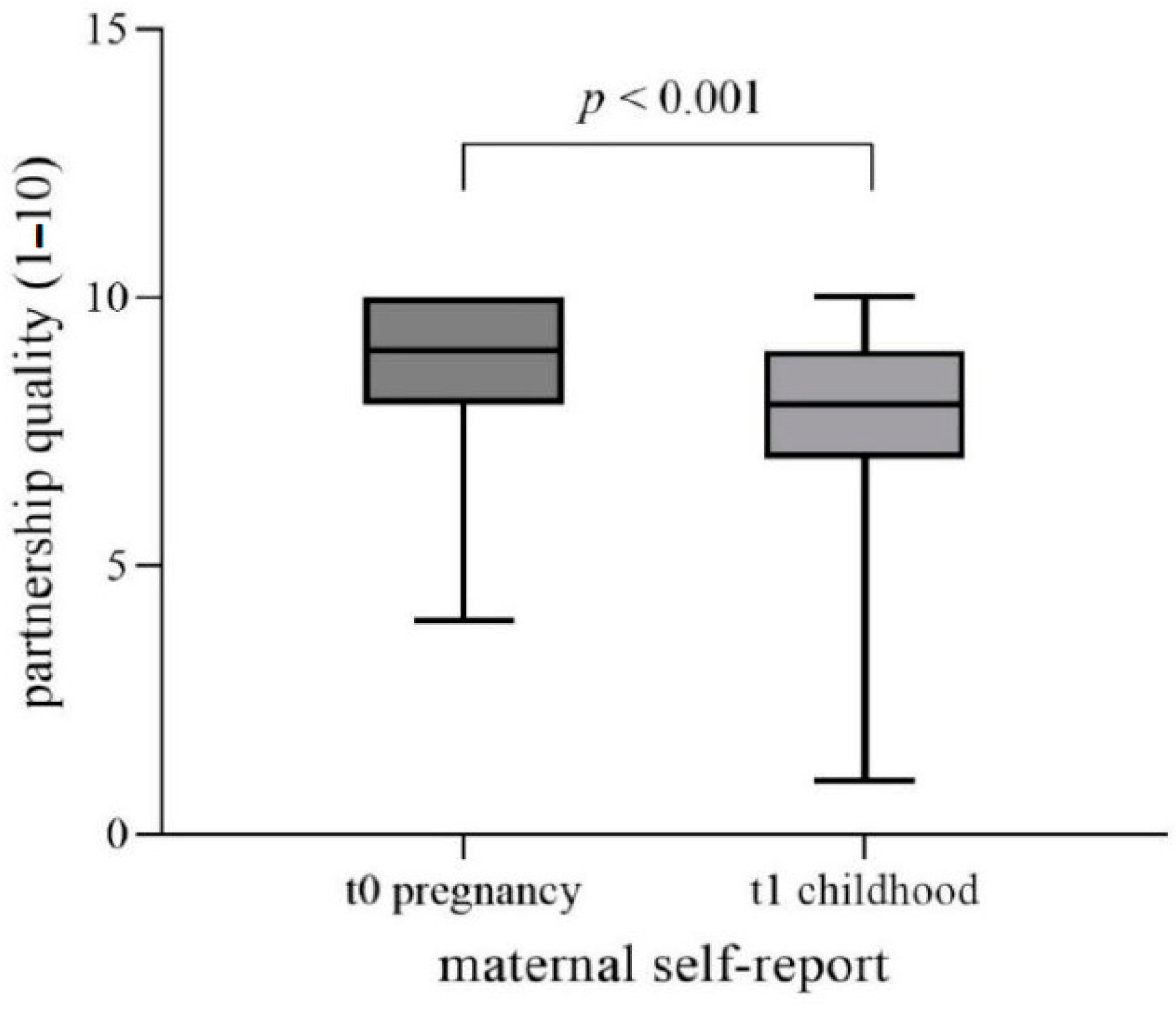
3.4. Subjective Satisfaction with Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rakers, F.; Rupprecht, S.; Dreiling, M.; Bergmeier, C.; Witte, O.W.; Schwab, M. Transfer of maternal psychosocial stress to the fetus. Neurosci. Biobehav. Rev. 2020, 117, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, I. Prä- und perinatale Aspekte kinder- und jugendpsychiatrischer Störungen. Hebamme 2011, 24, 98–103. [Google Scholar] [CrossRef]
- Graham, Y.P.; Heim, C.; Goodman, S.H.; Miller, A.H.; Nemeroff, C.B. The effects of neonatal stress on brain development: Implications for psychopathology. Dev. Psychopathol. 1999, 11, 545–565. [Google Scholar] [CrossRef] [PubMed]
- Glover, V.; O’Donnell, K.J.; O’Connor, T.G.; Fisher, J. Prenatal maternal stress, fetal programming, and mechanisms underlying later psychopathology—A global perspective. Dev. Psychopathol. 2018, 30, 843–854. [Google Scholar] [CrossRef]
- O’Donnell, K.J.; Meaney, M.J. Fetal Origins of Mental Health: The Developmental Origins of Health and Disease Hypothesis. Am. J. Psychiatry 2017, 174, 319–328. [Google Scholar] [CrossRef]
- Amgalan, A.; Andescavage, N.; Limperopoulos, C. Prenatal origins of neuropsychiatric diseases. Acta Paediatr. 2021, 110, 1741–1749. [Google Scholar] [CrossRef]
- Popova, S.; Lange, S.; Probst, C.; Gmel, G.; Rehm, J. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e290–e299. [Google Scholar] [CrossRef]
- Mattson, S.N.; Bernes, G.A.; Doyle, L.R. Fetal Alcohol Spectrum Disorders: A Review of the Neurobehavioral Deficits Associated With Prenatal Alcohol Exposure. Alcohol. Clin. Exp. Res. 2019, 43, 1046–1062. [Google Scholar] [CrossRef]
- Maschke, J.; Roetner, J.; Goecke, T.W.; Fasching, P.A.; Beckmann, M.W.; Kratz, O.; Moll, G.H.; Lenz, B.; Kornhuber, J.; Eichler, A.; et al. Prenatal Alcohol Exposure and the Facial Phenotype in Adolescents: A Study Based on Meconium Ethyl Glucuronide. Brain Sci. 2021, 11, 154. [Google Scholar] [CrossRef]
- Moder, J.E.; Ordenewitz, L.K.; Schlüter, J.A.; Weinmann, T.; Altebäumer, P.; Jung, J.; Heinen, F.; Landgraf, M.N. Fetal alcohol spectrum disorders-diagnosis, prognosis, and prevention. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 747–754. [Google Scholar] [CrossRef]
- Kalberg, W.O.; May, P.A.; Buckley, D.; Hasken, J.M.; Marais, A.S.; De Vries, M.M.; Bezuidenhout, H.; Manning, M.A.; Robinson, L.K.; Adam, M.P.; et al. Early-Life Predictors of Fetal Alcohol Spectrum Disorders. Pediatrics 2019, 144, e20182141. [Google Scholar] [CrossRef] [PubMed]
- Eichler, A.; Hudler, L.; Grunitz, J.; Grimm, J.; Raabe, E.; Goecke, T.W.; Fasching, P.A.; Beckmann, M.W.; Kratz, O.; Moll, G.H.; et al. Effects of prenatal alcohol consumption on cognitive development and ADHD-related behaviour in primary-school age: A multilevel study based on meconium ethyl glucuronide. J. Child Psychol. Psychiatry 2018, 59, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Burden, M.J.; Jacobson, J.L.; Westerlund, A.; Lundahl, L.H.; Morrison, A.; Dodge, N.C.; Klorman, R.; Nelson, C.A.; Avison, M.J.; Jacobson, S.W. An event-related potential study of response inhibition in ADHD with and without prenatal alcohol exposure. Alcohol. Clin. Exp. Res. 2010, 34, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Tiesler, C.M.; Heinrich, J. Prenatal nicotine exposure and child behavioural problems. Eur. Child Adolesc. Psychiatry 2014, 23, 913–929. [Google Scholar] [CrossRef] [PubMed]
- McGrath-Morrow, S.A.; Gorzkowski, J.; Groner, J.A.; Rule, A.M.; Wilson, K.; Tanski, S.E.; Collaco, J.M.; Klein, J.D. The Effects of Nicotine on Development. Pediatrics 2020, 145, e20191346. [Google Scholar] [CrossRef]
- Abraham, M.; Alramadhan, S.; Iniguez, C.; Duijts, L.; Jaddoe, V.W.; Den Dekker, H.T.; Crozier, S.; Godfrey, K.M.; Hindmarsh, P.; Vik, T.; et al. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS ONE 2017, 12, e0170946. [Google Scholar] [CrossRef]
- Buka, S.L.; Shenassa, E.D.; Niaura, R. Elevated risk of tobacco dependence among offspring of mothers who smoked during pregnancy: A 30-year prospective study. Am. J. Psychiatry 2003, 160, 1978–1984. [Google Scholar] [CrossRef]
- Dong, T.; Hu, W.; Zhou, X.; Lin, H.; Lan, L.; Hang, B.; Lv, W.; Geng, Q.; Xia, Y. Prenatal exposure to maternal smoking during pregnancy and attention-deficit/hyperactivity disorder in offspring: A meta-analysis. Reprod. Toxicol. 2018, 76, 63–70. [Google Scholar] [CrossRef]
- Bergman, K.; Sarkar, P.; O’Connor, T.G.; Modi, N.; Glover, V. Maternal stress during pregnancy predicts cognitive ability and fearfulness in infancy. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1454–1463. [Google Scholar] [CrossRef]
- Loomans, E.M.; van Dijk, A.E.; Vrijkotte, T.G.; van Eijsden, M.; Stronks, K.; Gemke, R.J.; Van den Bergh, B.R. Psychosocial stress during pregnancy is related to adverse birth outcomes: Results from a large multi-ethnic community-based birth cohort. Eur. J. Public Health 2013, 23, 485–491. [Google Scholar] [CrossRef]
- Talge, N.M.; Neal, C.; Glover, V.; the Early Stress, Translational Research and Prevention Science Network: Fetal and Neonatal Experience on Child and Adolescent Mental Health. Antenatal maternal stress and long-term effects on child neurodevelopment: How and why? J. Child Psychol. Psychiatry 2007, 48, 245–261. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.R.H.; van den Heuvel, M.I.; Lahti, M.; Braeken, M.; de Rooij, S.R.; Entringer, S.; Hoyer, D.; Roseboom, T.; Raikkonen, K.; King, S.; et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 2020, 117, 26–64. [Google Scholar] [CrossRef] [PubMed]
- Lautarescu, A.; Craig, M.C.; Glover, V. Prenatal stress: Effects on fetal and child brain development. Int. Rev. Neurobiol. 2020, 150, 17–40. [Google Scholar] [CrossRef]
- Kajanoja, J.; Nolvi, S.; Kantojarvi, K.; Karlsson, L.; Paunio, T.; Karlsson, H. Oxytocin receptor genotype moderates the association between maternal prenatal stress and infant early self-regulation. Psychoneuroendocrinology 2022, 138, 105669. [Google Scholar] [CrossRef] [PubMed]
- Rifkin-Graboi, A.; Meaney, M.J.; Chen, H.; Bai, J.; Hameed, W.B.; Tint, M.T.; Broekman, B.F.; Chong, Y.S.; Gluckman, P.D.; Fortier, M.V.; et al. Antenatal maternal anxiety predicts variations in neural structures implicated in anxiety disorders in newborns. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 313–321.e2. [Google Scholar] [CrossRef] [PubMed]
- DeSocio, J.E. Epigenetics, maternal prenatal psychosocial stress, and infant mental health. Arch. Psychiatr. Nurs. 2018, 32, 901–906. [Google Scholar] [CrossRef]
- Sacco, R.; Camilleri, N.; Eberhardt, J.; Umla-Runge, K.; Newbury-Birch, D. A systematic review and meta-analysis on the prevalence of mental disorders among children and adolescents in Europe. Eur. Child Adolesc. Psychiatry 2022, 1–18. [Google Scholar] [CrossRef]
- Adams, E.L.; Smith, D.; Caccavale, L.J.; Bean, M.K. Parents Are Stressed! Patterns of Parent Stress Across COVID-19. Front. Psychiatry 2021, 12, 626456. [Google Scholar] [CrossRef]
- Kölch, M.; Fegert, J.M. Chronische Tic-Störungen und Tourette-Syndrom. In Klinikmanual Kinder- und Jugendpsychiatrie und -Psychotherapie; Kölch, M., Rassenhofer, M., Fegert, J.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; pp. 169–181. [Google Scholar]
- Plener, P.L.; Fegert, J.M. Störungen des Sozialverhaltens. In Klinikmanual Kinder- und Jugendpsychiatrie und -Psychotherapie; Kölch, M., Rassenhofer, M., Fegert, J.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; pp. 25–38. [Google Scholar]
- Thomas, J.M.; Benham, A.L.; Gean, M.; Luby, J.; Minde, K.; Turner, S.; Wright, H.H. Practice parameters for the psychiatric assessment of infants and toddlers (0–36 months). American Academy of Child and Adolescent Psychiatry. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 21S–36S. [Google Scholar] [CrossRef]
- Schmidt, M.H.; Poustka, F. Multiaxiales Klassifikationsschema für Psychische Störungen des Kindes- und Jugendalters nach ICD-10: Mit einem Synoptischen Vergleich von ICD-10 und DSM-5; Hogrefe: Göttingen, Germany, 2017. [Google Scholar]
- Zero to Three. In DC: 0-5: Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood; Zero to Three: Washington, DC, USA, 2016.
- WHO. International Classification of Diseases, Eleventh Revision (ICD-11). Available online: https://icd.who.int/browse11 (accessed on 7 February 2023).
- Avila-Tang, E.; Al-Delaimy, W.K.; Ashley, D.L.; Benowitz, N.; Bernert, J.T.; Kim, S.; Samet, J.M.; Hecht, S.S. Assessing secondhand smoke using biological markers. Tob. Control 2013, 22, 164–171. [Google Scholar] [CrossRef]
- Nast, I.; Bolten, M.; Meinlschmidt, G.; Hellhammer, D.H. How to measure prenatal stress? A systematic review of psychometric instruments to assess psychosocial stress during pregnancy. Paediatr. Perinat. Epidemiol. 2013, 27, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.P.; Colton, J.; Priest, S.; Reilly, N.; Hadzi-Pavlovic, D. The antenatal risk questionnaire (ANRQ): Acceptability and use for psychosocial risk assessment in the maternity setting. Women Birth 2013, 26, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, M.; de Meer, G.; Verhulst, F.C.; Ormel, J.; Reijneveld, S.A. Limited validity of parental recall on pregnancy, birth, and early childhood at child age 10 years. J. Clin. Epidemiol. 2010, 63, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Pickett, K.E.; Kasza, K.; Biesecker, G.; Wright, R.J.; Wakschlag, L.S. Women who remember, women who do not: A methodological study of maternal recall of smoking in pregnancy. Nicotine Tob. Res. 2009, 11, 1166–1174. [Google Scholar] [CrossRef]
- Newport, D.J.; Brennan, P.A.; Green, P.; Ilardi, D.; Whitfield, T.H.; Morris, N.; Knight, B.T.; Stowe, Z.N. Maternal depression and medication exposure during pregnancy: Comparison of maternal retrospective recall to prospective documentation. BJOG 2008, 115, 681–688. [Google Scholar] [CrossRef]
- Jacobson, S.W.; Chiodo, L.M.; Sokol, R.J.; Jacobson, J.L. Validity of maternal report of prenatal alcohol, cocaine, and smoking in relation to neurobehavioral outcome. Pediatrics 2002, 109, 815–825. [Google Scholar] [CrossRef]
- Eichler, A.; Grunitz, J.; Grimm, J.; Walz, L.; Raabe, E.; Goecke, T.W.; Beckmann, M.W.; Kratz, O.; Heinrich, H.; Moll, G.H.; et al. Did you drink alcohol during pregnancy? Inaccuracy and discontinuity of women’s self-reports: On the way to establish meconium ethyl glucuronide (EtG) as a biomarker for alcohol consumption during pregnancy. Alcohol 2016, 54, 39–44. [Google Scholar] [CrossRef]
- Reulbach, U.; Bleich, S.; Knorr, J.; Burger, P.; Fasching, P.A.; Kornhuber, J.; Beckmann, M.W.; Goecke, T.W. Pre-, peri- and postpartal depression. Fortschr. Neurol. Psychiatr. 2009, 77, 708–713. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Ramos, A.M.; Marceau, K.; Neiderhiser, J.M.; De Araujo-Greecher, M.; Natsuaki, M.N.; Leve, L.D. Maternal Consistency in Recalling Prenatal Experiences at 6 Months and 8 Years Postnatal. J. Dev. Behav. Pediatr. 2020, 41, 698–705. [Google Scholar] [CrossRef]
- Hannigan, J.H.; Chiodo, L.M.; Sokol, R.J.; Janisse, J.; Ager, J.W.; Greenwald, M.K.; Delaney-Black, V. A 14-year retrospective maternal report of alcohol consumption in pregnancy predicts pregnancy and teen outcomes. Alcohol 2010, 44, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Rice, F.; Lewis, A.; Harold, G.; van den Bree, M.; Boivin, J.; Hay, D.F.; Owen, M.J.; Thapar, A. Agreement between maternal report and antenatal records for a range of pre and peri-natal factors: The influence of maternal and child characteristics. Early Hum. Dev. 2007, 83, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Czeizel, A.E.; Petik, D.; Puho, E. Smoking and alcohol drinking during pregnancy. The reliability of retrospective maternal self-reported information. Cent. Eur. J. Public Health 2004, 12, 179–183. [Google Scholar] [PubMed]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; de Pablo, G.S.; Shin, J.I.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatr. 2022, 27, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Dietz, P.; Bombard, J.; Mulready-Ward, C.; Gauthier, J.; Sackoff, J.; Brozicevic, P.; Gambatese, M.; Nyland-Funke, M.; England, L.; Harrison, L.; et al. Validation of self-reported maternal and infant health indicators in the Pregnancy Risk Assessment Monitoring System. Matern. Child Health J. 2014, 18, 2489–2498. [Google Scholar] [CrossRef]
- Castelar-Rios, M.J.; De Los Santos-Roig, M.; Robles-Ortega, H.; Diaz-Lopez, M.A.; Maldonado-Lozano, J.; Bellido-Gonzalez, M. Moderating Effect of Changes in Perceived Social Support during Pregnancy on the Emotional Health of Mothers and Fathers and on Baby’s Anthropometric Parameters at Birth. Children 2022, 9, 648. [Google Scholar] [CrossRef]
- Cheng, E.R.; Rifas-Shiman, S.L.; Perkins, M.E.; Rich-Edwards, J.W.; Gillman, M.W.; Wright, R.; Taveras, E.M. The Influence of Antenatal Partner Support on Pregnancy Outcomes. J. Womens Health 2016, 25, 672–679. [Google Scholar] [CrossRef]
- Morin, M.; Vayssiere, C.; Claris, O.; Irague, F.; Mallah, S.; Molinier, L.; Matillon, Y. Evaluation of the quality of life of pregnant women from 2005 to 2015. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 115–130. [Google Scholar] [CrossRef]
- Lagadec, N.; Steinecker, M.; Kapassi, A.; Magnier, A.M.; Chastang, J.; Robert, S.; Gaouaou, N.; Ibanez, G. Factors influencing the quality of life of pregnant women: A systematic review. BMC Pregnancy Childbirth 2018, 18, 455. [Google Scholar] [CrossRef]
- Hasan, R.; Baird, D.D.; Herring, A.H.; Olshan, A.F.; Jonsson Funk, M.L.; Hartmann, K.E. Patterns and predictors of vaginal bleeding in the first trimester of pregnancy. Ann. Epidemiol. 2010, 20, 524–531. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FRAMES t0 | FRANCES I t1 | FRANCES II t2 | ||
|---|---|---|---|---|
| M (SD)/N (%) | ||||
| Mothers | ||||
| Age [y] | 32.6 (4.7) | 40.4 (4.4) | 46.0 (4.4) | |
| BMI (prepartum) | 24.1 (5.5) | |||
| Marital status | Single Married | 194 (80.5) 47 (19.5) | 203 (85.7) 34 (14.3) | 151 (82.7) 32 (17.5) |
| Years of school attendance | >12 ≤12 | 127 (52.7) 114 (47.3) | 129 (53.5) 112 (46.5) | 112 (61.2) 71 (38.8) |
| Family income (monthly, net) | <1000 € 1000–2000 € 2000–3000 € 3000–4000 € 5000–4000 € >5000 € | 5 (2.8) 35 (19.6) 61 (34.1) 37 20.7) 23 (12.8) 18 (10.1) | 0 (0.0) 23 (9.5) 54 (22.4) 50 20.7) 48 (19.9) 66 (27.4) | 0 (0.0) 9 (4.9) 23 (12.6) 38 (20.8) 37 (20.2) 76 (41.5) |
| Fathers | ||||
| Age [y] | 35.4 (5.5) | 43.2 (5.5) | 48.7 (5.5) | |
| Children | ||||
| Age [y] | 7.7 (0.76) | 13.3 (0.34) | ||
| Sex | Female Male | 117 (48.5) 124 (51.5) | 117 (48.5) 124 (51.5) | 90 (49.2) 93 (50.8) |
| Maternal Self-Report on Prenatal… | FRAMES (t0) | FRANCES I (t1) | FRANCES II (t2) | Scale Level | Intraindividual Agreement | Dependent Group Comparison |
|---|---|---|---|---|---|---|
| Alcohol | + | + | + | Nominal | Fleiss’ κ | Cochran’s Q |
| Smoking | + | + | + | Nominal | Fleiss’ κ | Cochran’s Q |
| Complications | + | + | − | Nominal | Cohen’s κ | McNemar |
| Partnership | + | + | − | Interval | Spearman’s r | Wilcoxon |
| Satisfaction | + | + | − | Interval | Spearman’s r | Wilcoxon |
| Maternal Self-Report on Prenatal… | 3rd Trimester t0 (n = 241) FRAMES | Primary-School t1 (n = 241) FRANCES I | Adolescence t2 (n = 183) FRANCES II | Statistics | |||||
|---|---|---|---|---|---|---|---|---|---|
| p | Post-Hoc p | κ | |||||||
| N (%) | t0/t1 | t1/t2 | t0/t2 | ||||||
| Alcohol | Yes No | 46 (25.8) 132 (74.2) | 31 (17.4) 147 (82.6) | 73 (41.0) 105 (59.0) | <0.001 | 0.143 | <0.01 | 0.001 | 0.203 ** |
| Smoking | Yes No | 21 (11.9) 156 (88.1) | 29 (16.4) 148 (83.6) | 40 (22.6) 137 (77.4) | <0.001 | 0.98 | 0.01 | <0.001 | 0.719 ** |
| Complications | Yes No | 197 (84.9) 35 (15.1) | 98 (42.2) 134 (57.8) | - - | <0.001 | - | - | - | −0.051 |
| Maternal Self-Report on Prenatal… | 3rd Trimester t0 FRAMES | Primary-School t1 FRANCES I | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | Range | M | SD | Range | p | r | rs | |
| Partnership (1–10) | 8.86 | 1.19 | 6 | 7.89 | 2.05 | 9 | <0.001 | 0.49 | 0.371 ** |
| Satisfaction (1–5) | |||||||||
| 1st tri. 2nd tri. 3rd tri. | 2.50 1.91 2.23 | 1.20 0.93 0.99 | 4 4 4 | 2.28 2.06 2.32 | 1.16 1.03 1.12 | 4 4 4 | 0.003 0.017 0.256 | 0.20 0.16 0.08 | 0.544 ** 0.525 ** 0.467 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mestermann, S.; Fasching, P.A.; Beckmann, M.W.; Gerlach, J.; Kratz, O.; Moll, G.H.; Kornhuber, J.; Eichler, A.; the IMAC-Mind-Consortium. The Benefit of a Retrospective Pregnancy Anamnesis in Child and Adolescent Psychiatry: The Reliability of Maternal Self-Report during Childhood Development. Children 2023, 10, 866. https://doi.org/10.3390/children10050866
Mestermann S, Fasching PA, Beckmann MW, Gerlach J, Kratz O, Moll GH, Kornhuber J, Eichler A, the IMAC-Mind-Consortium. The Benefit of a Retrospective Pregnancy Anamnesis in Child and Adolescent Psychiatry: The Reliability of Maternal Self-Report during Childhood Development. Children. 2023; 10(5):866. https://doi.org/10.3390/children10050866
Chicago/Turabian StyleMestermann, Stefan, Peter A. Fasching, Matthias W. Beckmann, Jennifer Gerlach, Oliver Kratz, Gunther H. Moll, Johannes Kornhuber, Anna Eichler, and the IMAC-Mind-Consortium. 2023. "The Benefit of a Retrospective Pregnancy Anamnesis in Child and Adolescent Psychiatry: The Reliability of Maternal Self-Report during Childhood Development" Children 10, no. 5: 866. https://doi.org/10.3390/children10050866
APA StyleMestermann, S., Fasching, P. A., Beckmann, M. W., Gerlach, J., Kratz, O., Moll, G. H., Kornhuber, J., Eichler, A., & the IMAC-Mind-Consortium. (2023). The Benefit of a Retrospective Pregnancy Anamnesis in Child and Adolescent Psychiatry: The Reliability of Maternal Self-Report during Childhood Development. Children, 10(5), 866. https://doi.org/10.3390/children10050866