
The Development of a Screening Tool for Childcare Professionals to Detect and Refer Infant and Toddler Maltreatment and Trauma: A Tale of Four Countries

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
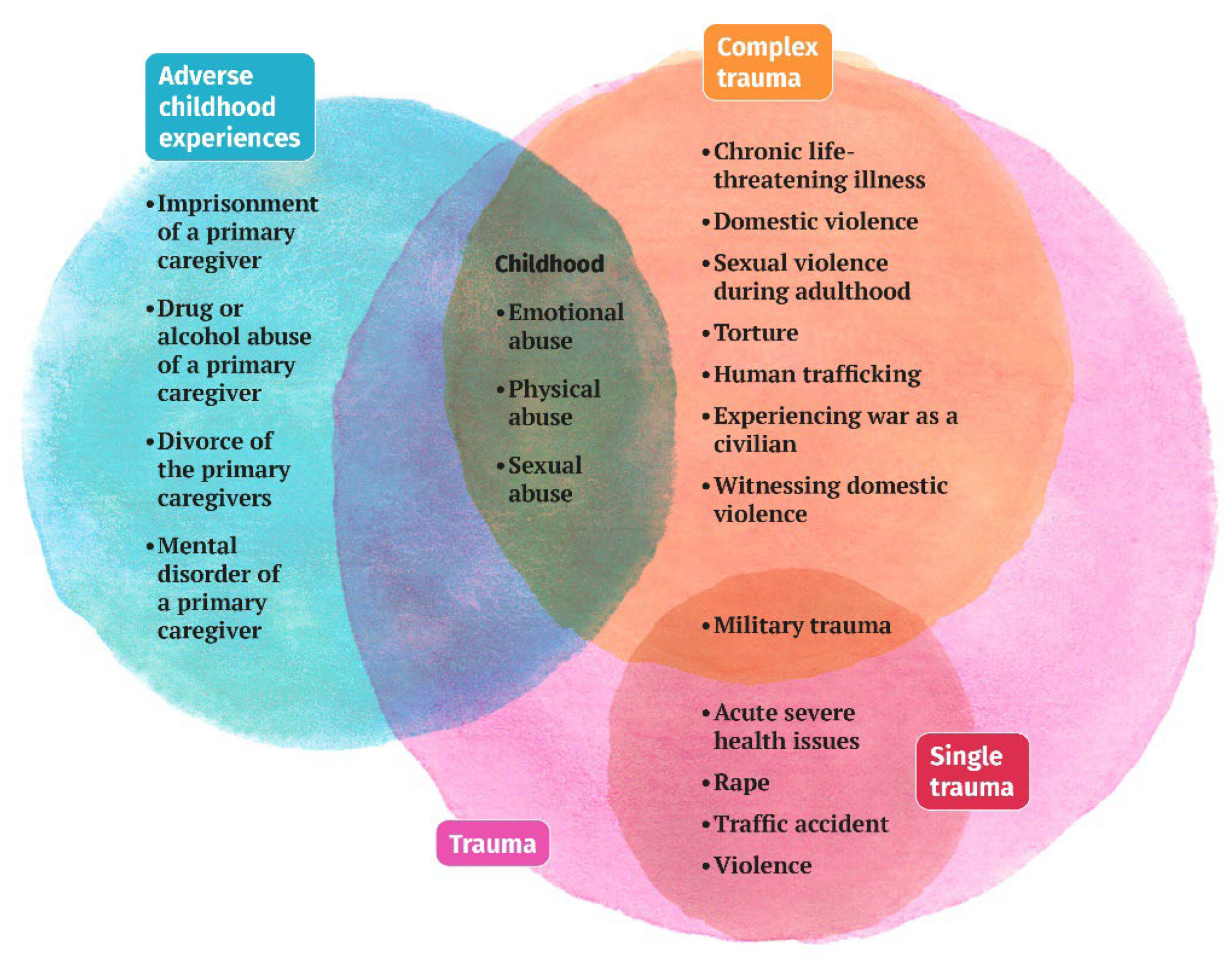
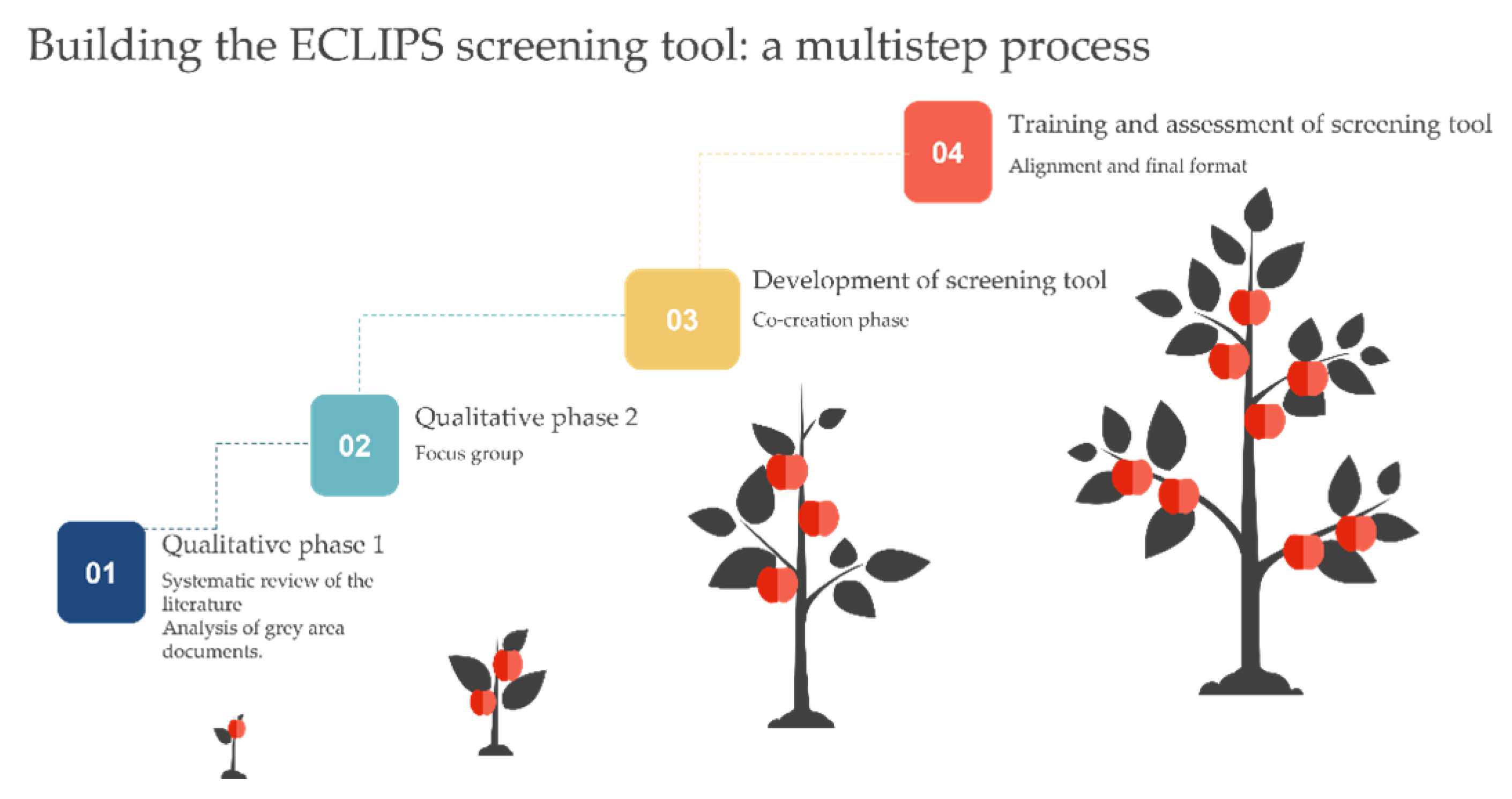
2.1. Screening Protocol Development: Design and Procedure
2.1.1. The Living Labs
- LL meetings 1 and 2, exploration stage: assessment needed concerning screening, discussion, and brainstorming about results of a previous inventory of the good practices and the insights from expert focus groups [20].
- LL meetings 3–6, co-construction stage: joint development of the screening tool
- LL meetings 7–8, piloting stage: meetings 7 and 8 took place one month after one another, during which the LLs’ childcare professionals practiced the use of the screening tool within their facilities and shared it with colleagues. Based on their experiences, both professionals and parents offered feedback on the LLs. Modifications were implemented by the researchers and led to the finalizing of the protocol.
2.1.2. Education and Testing
2.2. Measures and Data Analysis
3. Results
3.1. Outcome Co-Creation Process
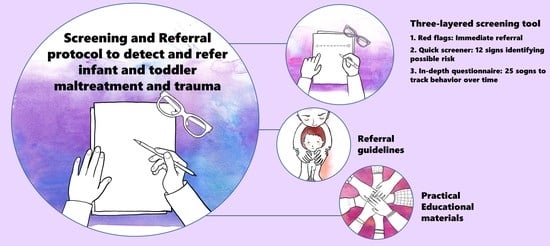
3.1.1. First Layer: The Five “Red Flags”
3.1.2. Second Layer: The “Quick Screener”
3.1.3. Third Layer: The “In-Depth Questionnaire”
3.1.4. Referral Flowchart
3.2. Outcome Training and Testing
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. ECLIPS Screening Tool Evaluation Questionnaire

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | ||||
|---|---|---|---|---|---|---|---|---|
| Completely Disagree | Disagree | Neutral | Agree | Completely agree | ||||
| 1. Trauma symptoms are visible in babies and toddlers. | 1 | 2 | 3 | 4 | 5 | |||
| 2. Trauma is not only related to physical and sexual abuse but also to psychological maltreatment and neglect. | 1 | 2 | 3 | 4 | 5 | |||
| 3. Domestic violence during infancy can have long-term effects on physical, emotional and mental health later in life. | 1 | 2 | 3 | 4 | 5 | |||
| 4. I have enough knowledge to detect signs of trauma in young children. | 1 | 2 | 3 | 4 | 5 | |||
| 5. I have enough knowledge to understand the effects of trauma on infants. | 1 | 2 | 3 | 4 | 5 | |||
| 6. I am aware of the referral procedures to follow in case of suspected abuse. | 1 | 2 | 3 | 4 | 5 | |||
| 7. Childcare professionals can play an important role in screening and referring child abuse. | 1 | 2 | 3 | 4 | 5 | |||
| 8. I found the Screening Tool to be useful. | 1 | 2 | 3 | 4 | 5 | |||
| 9. I found the Screening Tool to be user-friendly. | 1 | 2 | 3 | 4 | 5 | |||
| 10. I intend to use the Screening Tool in the future. | 1 | 2 | 3 | 4 | 5 | |||
| 11. The content of the program aligned with my expectations. | 1 | 2 | 3 | 4 | 5 | |||
| 12. I am satisfied with the content of the program. | 1 | 2 | 3 | 4 | 5 | |||
| 13. I am satisfied with the way of teaching. | 1 | 2 | 3 | 4 | 5 | |||
| 14. I am satisfied with the learning material. | 1 | 2 | 3 | 4 | 5 | |||
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Bellis, M.A.; Hughes, K.; Ford, K.; Rodriguez, G.R.; Sethi, D.; Passmore, J. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: A systematic review and meta-analysis. Lancet Public Health 2019, 4, e517–e528. [Google Scholar] [CrossRef]
- Sethi, D.; Yon, Y.; Parekh, N.; Anderson, T.; Huber, J.; Rakovac, I.; Meinck, F. European Status Report on Preventing Child Maltreatment; World Health Organisation—Regional Office for Europe: Copenhagen, Denmark, 2018; Available online: https://www.euro.who.int/__data/assets/pdf_file/0017/381140/wh12-ecm-rep-eng.pdf (accessed on 3 March 2020).
- U.S. Department of Health & Human Services (USDHHS), Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2019. 2021. Available online: https://www.acf.hhs.gov/cb/research-data-technology/statistics-research/child-maltreatment (accessed on 3 March 2020).
- U.S. Department of Health & Human Services (USDHHS), Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2020. 2022. Available online: https://www.acf.hhs.gov/cb/data-research/child-maltreatment (accessed on 3 March 2020).
- Oral, R.; Yagmur, F.; Nashelsky, M.; Turkmen, M.; Kirby, P. Fatal Abusive Head Trauma Cases: Consequence of medical staff missingmilde forms of physical abuse. Pediatr. Emerg. Care 2008, 24, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Naughton, A.M.; Maguire, S.A.; Mann, M.K.; Lumb, R.C.; Tempest, V.; Gracias, S.; Kemp, A.M. Emotional, behavioral, and developmental features indicative of neglect or emotional abuse in preschool children: A systematic review. JAMA Pediatr. 2013, 167, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Norman, R.E.; Byambaa, M.; De, R.; Butchart, A.; Scott, J.; Vos, T. The Long-Term Health Consequences of Child Physical Abuse, Emotional Abuse, and Neglect: A Systematic Review and Meta-Analysis. PLoS Med. 2012, 9, e1001349. [Google Scholar] [CrossRef]
- Treat, A.E.; Sheffield Morris, A.; Williamson, A.C.; Hays-Grudo, J.; Laurin, D. Adverse childhood experiences, parenting, and child executive function. Early Child Dev. Care 2019, 189, 926–937. [Google Scholar] [CrossRef]
- U.S. Department of Health & Human Services (USDHHS), Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. Child Maltreatment 2015. 2017. Available online: https://www.anotpertinentcf.hhs.gov/cb/research-data-technology/statistics-research/child-maltreatment (accessed on 3 March 2020).
- Baptista, J.; Silva, J.R.; Marques, S.; Martins, C.; Soares, I. Early maltreatment and current quality of relational care predict socioemotional problems among institutionalized infants and toddlers. Infant Ment. Health J. 2018, 39, 718–729. [Google Scholar] [CrossRef]
- McCrory, E.; De Brito, S.A.; Viding, E. The link between child abuse and psychopathology: A review of neurobiological and genetic research. J. R. Soc. Med. 2012, 105, 151–156. [Google Scholar] [CrossRef]
- Shonkoff, J.P.; Boyce, W.T.; Levitt, P.; Martinez, F.D.; McEwen, B. Leveraging the Biology of Adversity and Resilience to Transform Pediatric Practice. Pediatrics 2021, 147, e20193845. [Google Scholar] [CrossRef]
- Shonkoff, J.P.; Garner, A.S.; Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 2012, 129, e232–e246. [Google Scholar] [CrossRef]
- Shonkoff, J.P.; Radner, J.M.; Foote, N. Expanding the evidence base to drive more productive early childhood investment. Lancet 2017, 389, 14–16. [Google Scholar] [CrossRef]
- Perry, B.D.; Pollard, R.A.; Blakley, T.L.; Baker, W.L.; Vigilante, D. Childhood trauma, the neurobiology of adaptation, and “use-dependent” development of the brain: How “states” become “traits”. Infant Ment. Health J. 1995, 16, 271–291. [Google Scholar] [CrossRef]
- Marsac, M.L.; Kassam-Adams, N.; Hildenbrand, A.K.; Nicholls, E.; Winston, F.K.; Leff, S.S.; Fein, J. Implementing a Trauma-Informed Approach in Pediatric Health Care Networks. JAMA Pediatr. 2016, 170, 70–77. [Google Scholar] [CrossRef]
- World Health Organization. Child Maltreatment. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment (accessed on 4 April 2021).
- National Health Service Education for Scotland. Transforming Psychological Trauma: A Knowledge and Skills Framework for the Scottish Workforce. 2017. Available online: https://www.nes.scot.nhs.uk/media/rgxngvpv/nationaltraumatrainingframework-execsummary-web.pdf (accessed on 3 March 2020).
- Bisagno, E.; Cadamuro, A.; Dierickx, S.; Mosleh, D.B.; Linde-Ozola, Z.; Kandāte, A.; Varga-Sabjan, D.; Morva, D.; Laszlo, N.; Rozsa, M.; et al. A European comparison of screening and referral by childcare professionals of maltreatment in children aged 0–3: A wild goose chase or maybe not. Child Abus. Rev. 2023, e2812. [Google Scholar] [CrossRef]
- Young, J.C.; Widom, C.S. Long-term effects of child abuse and neglect on emotion processing in adulthood. Child Abus. Negl. 2014, 38, 1369–1381. [Google Scholar] [CrossRef]
- Chen, C.-J.; Chen, Y.-W.; Chang, H.-Y.; Feng, J.-Y. Screening Tools for Child Abuse Used by Healthcare Providers: A Systematic Review. J. Nurs. Res. 2022, 30, e193. [Google Scholar] [CrossRef]
- Ezpeleta, L.; Pérez-Robles, R.; Fanti, K.A.; Karveli, V.; Katsimicha, E.; Nikolaidis, G.; Hadjicharalambous, M.Z.; Hatzinikolaou, K. Development of a screening tool enabling identification of infants and toddlers at risk of family abuse and neglect: A feasibility study from three South European countries. Child Care Health Dev. 2017, 43, 75–80. [Google Scholar] [CrossRef]
- Administration for Children and Families. Child Abuse, Neglect Data Released. 2020. Available online: https://www.acf.hhs.gov/media/press/2020/child-abuse-neglect-data-released (accessed on 4 April 2021).
- Louwers, E.C.; Korfage, I.J.; Affourtit, M.J.; Ruige, M.; van den Elzen, A.P.; de Koning, H.J.; Moll, H.A. Accuracy of a screening instrument to identify potential child abuse in emergency departments. Child Abus. Negl. 2014, 38, 1275–1281. [Google Scholar] [CrossRef]
- Louwers, E.C.; Korfage, I.J.; Affourtit, M.J.; Scheewe, D.J.; van de Merwe, M.H.; Vooijs-Moulaert, A.-F.S.; van den Elzen, A.P.; Jongejan, M.H.; Ruige, M.; Manaï, B.H.; et al. Effects of Systematic Screening and Detection of Child Abuse in Emergency Departments. Pediatrics 2012, 130, 457–464. [Google Scholar] [CrossRef]
- Saini, S.M.; Hoffmann, C.R.; Pantelis, C.; Everall, I.P.; Bousman, C.A. Systematic review and critical appraisal of child abuse measurement instruments. Psychiatry Res. 2019, 272, 106–113. [Google Scholar] [CrossRef]
- Pierce, M.C.; Kaczor, K.; Aldridge, S.; O’Flynn, J.; Lorenz, D.J. Bruising Characteristics Discriminating Physical Child Abuse from Accidental Trauma. Pediatrics 2010, 125, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.C.; Kaczor, K.; Lorenz, D.J.; Bertocci, G.; Fingarson, A.K.; Makoroff, K.; Berger, R.P.; Bennett, B.; Magana, J.; Staley, S.; et al. Validation of a Clinical Decision Rule to Predict Abuse in Young Children Based on Bruising Characteristics. JAMA Netw. Open 2021, 4, e215832. [Google Scholar] [CrossRef] [PubMed]
- Essau, C.A. Guidelines for the INTOVIAN Screening Tool. 2015. Available online: https://www.intovian.eu/ (accessed on 3 March 2020).
- Chang, Y.-C.; Huang, J.-L.; Hsia, S.-H.; Lin, K.-L.; Lee, E.-P.; Chou, I.-J.; Hsin, Y.-C.; Lo, F.-S.; Wu, C.-T.; Chiu, C.-H.; et al. Child protection medical service demonstration centers in approaching child abuse and neglect in Taiwan. Medicine 2016, 95, e5218. [Google Scholar] [CrossRef] [PubMed]
- Independent Authority for Children and Adolescents; Terre des Hommes Italia; Cismai. Second National Study on Child and Adolescent Maltreatment in Italy. Findings and Perspectives. 2021. Available online: https://terredeshommes.it/comunicati/presentazione-della-ii-indagine-nazionaale-sul-maltrattamento-bambini-adolescenti-italia (accessed on 3 March 2020).
- Hoft, M.; Haddad, L. Screening Children for Abuse and Neglect: A Review of the Literature. J. Forensic Nurs. 2017, 13, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Moll, H.A. IS-058 Screening On Child Abuse In Europe. Arch. Dis. Child. 2014, 99, A18–A19. [Google Scholar] [CrossRef]
- Salinas-Miranda, A.A.; Salemi, J.L.; King, L.M.; Baldwin, J.A.; Berry, E.; Austin, D.A.; Scarborough, K.; Spooner, K.K.; Zoorob, R.J.; Salihu, H.M. Adverse childhood experiences and health-related quality of life in adulthood: Revelations from a community needs assessment. Health Qual. Life Outcomes 2015, 13, 123. [Google Scholar] [CrossRef]
- Macmillan, H.L.; Wathen, C.N. Research Brief: Interventions to Prevent Child Maltreatment. Preventing Violence across the Lifespan Research Network; PreVAiL: London, ON, Canada, 2014. [Google Scholar]
- Ballon, P. Living labs. In The International Encyclopedia of Digital Communication and Society; Mansell, R., Ang, P.H., Eds.; Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Eriksson, M.; Niitamo, V.P.; Kulkki, S. State-of-the-Art in Utilizing Living Labs Approach to User-Centric ICT Innovation—A European Approach; CDT at Luleå University of Technology: Luleå, Sweden, 2005. [Google Scholar]
- Abdoh, N.; Bernardi, E.; Mccarthy, A. Knowledge, Attitudes, and Practices of Trauma Informed Practice: A Survey of Health Care Professionals and Support Staff at Alexander Street Community; NURS Synthesis Project; University of British Columbia Library: Vancouver, Canada, 2017. [Google Scholar]
- Verdonck, E.; Groenen, A.; Van Haeken, S. Een zelfrapportage-onderzoek naar slachtofferschap van geweld bij Vlaamse scholieren: Een blik op de resultaten met een ethische reflectie. Kindvriendelijk en participatief bevragen in een stedelijke context. Tijdschrift voor Jeugd en Kinderrechten 2019, 4, 375–388. [Google Scholar]
- Callaghan, J.E.M.; Alexander, J.H.; Sixsmith, J.; Fellin, L.C. Beyond “Witnessing”: Children’s Experiences of Coercive Control in Domestic Violence and Abuse. J. Interpers. Violence 2018, 33, 1551–1581. [Google Scholar] [CrossRef]
- Arimoto, A.; Tadaka, E. Developing and Validating a New Scale to Assess Signs of Neglect of Infants and Caregivers. J. Interpers. Violence 2021, 36, 8960–8983. [Google Scholar] [CrossRef]
- Baker, L.; Cunningham, A. Inter-Parental Violence: The Pre-Schooler’s Perspective and the Educator’s Role. Early Child. Educ. J. 2009, 37, 199–207. [Google Scholar] [CrossRef]
- Harper, B.; Nwabuzor Ogbonnaya, I.; McCullough, K.C. The Effect of Intimate Partner Violence on the Psychosocial Development of Toddlers. J. Interpers. Violence 2018, 33, 2512–2536. [Google Scholar] [CrossRef]
- McTavish, J.R.; Gonzalez, A.; Santesso, N.; MacGregor, J.C.D.; McKee, C.; Macmillan, H.L. Identifying children exposed to maltreatment: A systematic review update. BMC Pediatr. 2020, 20, 113. [Google Scholar] [CrossRef]
- Afifi, T.O.; MacMillan, H.L. Resilience following Child Maltreatment: A Review of Protective Factors. Can. J. Psychiatry 2011, 56, 266–272. [Google Scholar] [CrossRef]
- Levi, B.H.; Crowell, K.; Walsh, K.; Dellasega, C. How childcare providers interpret ‘reasonable suspicion’ of child abuse. Child Youth Care Forum 2015, 44, 875–891. [Google Scholar] [CrossRef]
- Schols, M.W.A.; Serie, C.M.B.; Broers, N.J.; de Ruiter, C. Factor analysis and predictive validity of the Early Risks of Physical Abuse and Neglect Scale (ERPANS): A prospective study in Dutch public youth healthcare. Child Abus. Negl. 2019, 88, 71–83. [Google Scholar] [CrossRef]
- van der Put, C.E.; Bouwmeester-Landweer, M.B.R.; Landsmeer-Beker, E.A.; Wit, J.M.; Dekker, F.W.; Kousemaker, N.P.J.; Baartman, H.E.M. Screening for potential child maltreatment in parents of a newborn baby: The predictive validity of an Instrument for early identification of Parents at Risk for child Abuse and Neglect (IPARAN). Child Abus. Negl. 2017, 70, 160–168. [Google Scholar] [CrossRef]
- Mathews, B.; Yang, C.; Lehman, E.B.; Mincemoyer, C.; Verdiglione, N.; Levi, B.H. Educating early childhood care and education providers to improve knowledge and attitudes about reporting child maltreatment: A randomized controlled trial. PLoS ONE 2017, 12, e0177777. [Google Scholar] [CrossRef]
- Yang, C.; Panlilio, C.; Verdiglione, N.; Lehman, E.B.; Hamm, R.M.; Fiene, R.; Dore, S.; Bard, D.E.; Grable, B.; Levi, B. Generalizing findings from a randomized controlled trial to a real-world study of the iLookOut, an online education program to improve early childhood care and education providers’ knowledge and attitudes about reporting child maltreatment. PLoS ONE 2020, 15, e0227398. [Google Scholar] [CrossRef]
- Dierickx, S.; Bisagno, E.; Varga-Sabján, D.; Morva, D.; Linde-Ozola, Z.; László, N.; Cadamuro, A.; Mosleh, D.B.; Rózsa, M.; De Fazio, G.L.; et al. Trauma-informed care to support children exposed to child abuse in childcare organizations: A qualitative comparison of four European countries. Child Abus. Rev. 2023, e2821. [Google Scholar] [CrossRef]






| PP | T0 | T1 | T2 |
|---|---|---|---|
| UCLL (Belgium) | 17 | 12 | 17 |
| UNIMORE (Italy) | 30 | 26 | 30 |
| Pressley Ridge (Hungary) | 27 | 27 | 27 |
| Centrs Dardedze (Latvia) | 26 | 30 | 22 |
| Total sample | 100 | 95 | 74 |
| Country | Time | Knowledge | Attitude | Screening | Training | ||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | ||
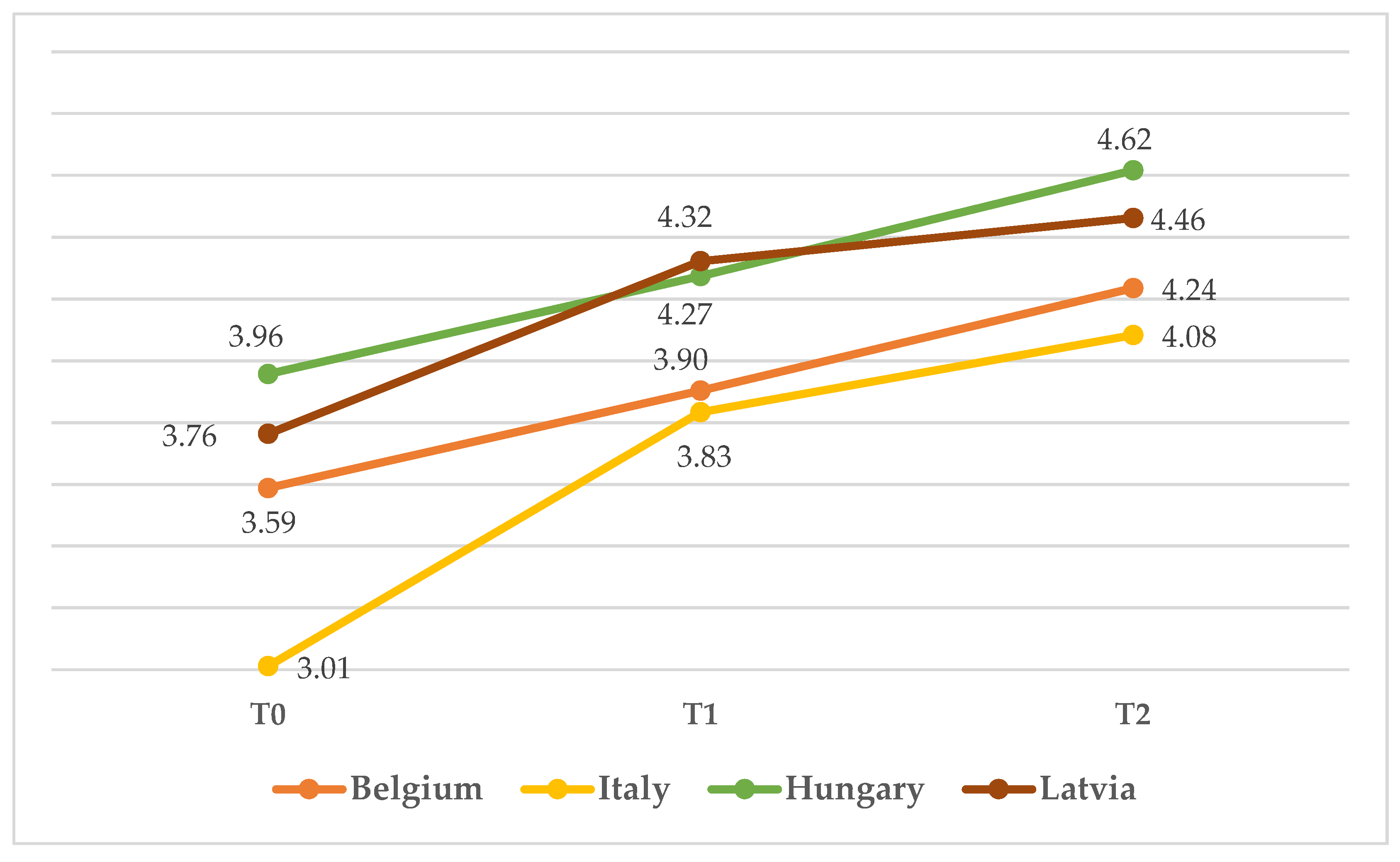
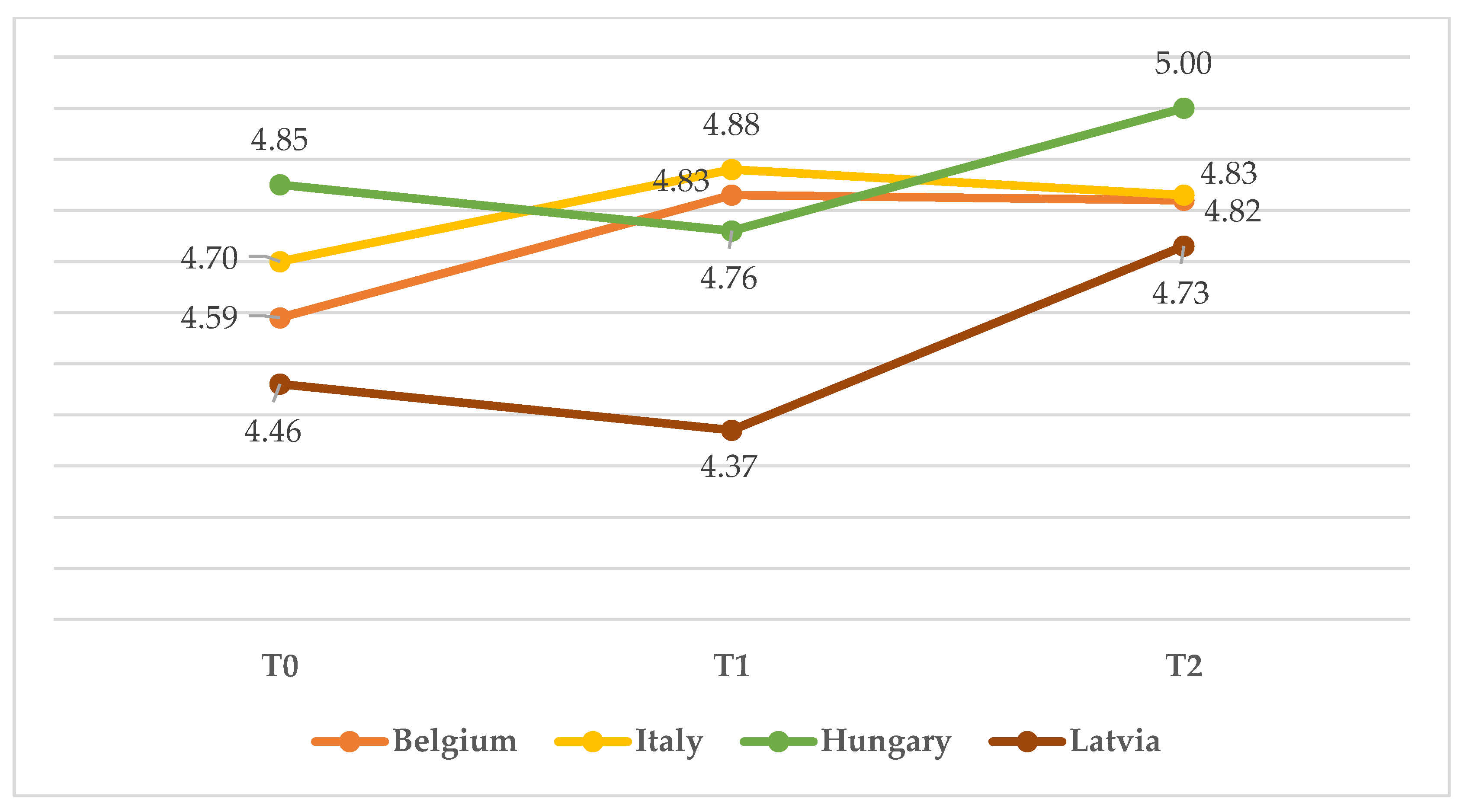
| Belgium | T0 | 3.59 | 0.37 | 4.59 | 0.51 | - | - | - | - |
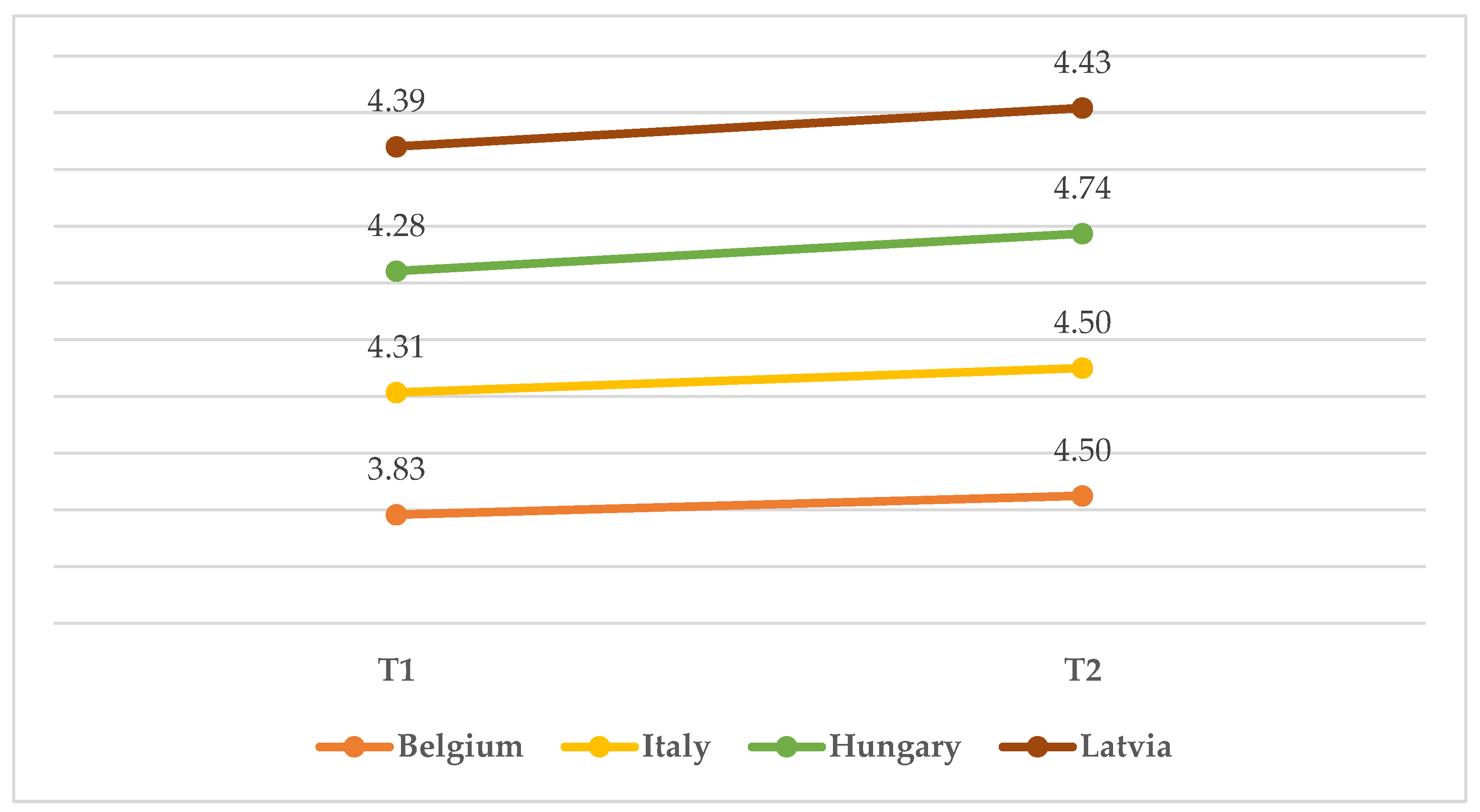
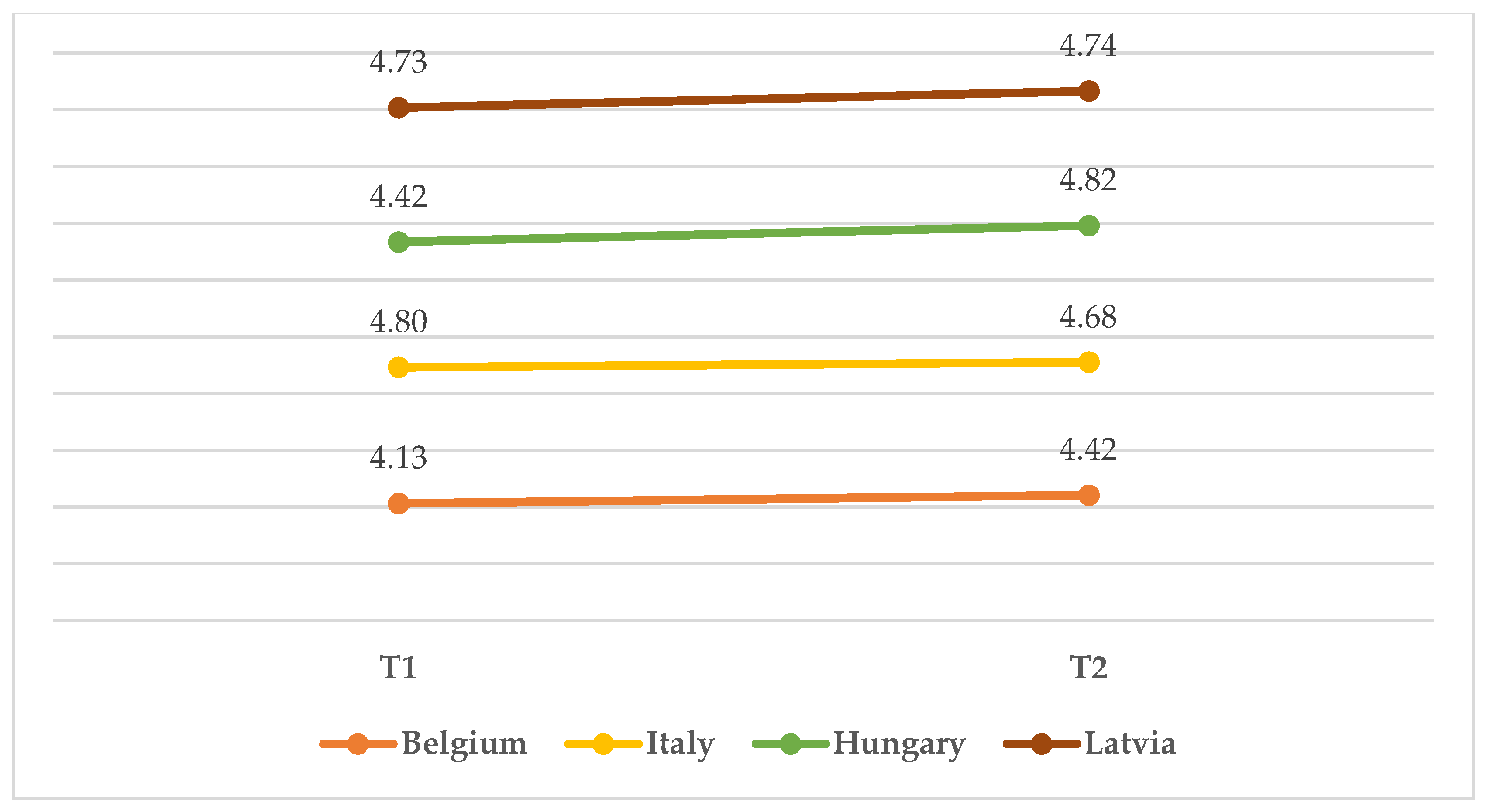
| T1 | 3.90 | 0.39 | 4.83 | 0.39 | 3.83 | 1.14 | 4.13 | 0.58 | |
| T2 | 4.24 | 0.24 | 4.82 | 0.39 | 4.50 | 0.54 | 4.423 | 0.38 | |
| Italy | T0 | 3.01 | 0.56 | 4.70 | 0.47 | - | - | - | - |
| T1 | 3.83 | 0.37 | 4.88 | 0.33 | 4.31 | 0.60 | 4.80 | 0.35 | |
| T2 | 4.08 | 0.37 | 4.83 | 0.38 | 4.50 | 0.58 | 4.68 | 0.53 | |
| Hungary | T0 | 3.96 | 0.44 | 4.85 | 0.36 | - | - | - | - |
| T1 | 4.27 | 0.44 | 4.76 | 0.53 | 4.28 | 0.61 | 4.42 | 0.56 | |
| T2 | 4.62 | 0.29 | 5.00 | 0.00 | 4.74 | 0.60 | 4.82 | 0.36 | |
| Latvia | T0 | 3.76 | 0.51 | 4.46 | 0.51 | - | - | - | - |
| T1 | 4.32 | 0.44 | 4.37 | 0.45 | 4.39 | 0.51 | 4.73 | 0.40 | |
| T2 | 4.46 | 0.30 | 4.73 | 0.55 | 4.43 | 0.59 | 4.74 | 0.44 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bisagno, E.; Cadamuro, A.; Serafine, D.; Dima, B.M.; Anne, G.; Zane, L.-O.; Annija, K.; Dóra, V.-S.; Dorottya, M.; Noémi, L.; et al. The Development of a Screening Tool for Childcare Professionals to Detect and Refer Infant and Toddler Maltreatment and Trauma: A Tale of Four Countries. Children 2023, 10, 858. https://doi.org/10.3390/children10050858
Bisagno E, Cadamuro A, Serafine D, Dima BM, Anne G, Zane L-O, Annija K, Dóra V-S, Dorottya M, Noémi L, et al. The Development of a Screening Tool for Childcare Professionals to Detect and Refer Infant and Toddler Maltreatment and Trauma: A Tale of Four Countries. Children. 2023; 10(5):858. https://doi.org/10.3390/children10050858
Chicago/Turabian StyleBisagno, Elisa, Alessia Cadamuro, Dierickx Serafine, Bou Mosleh Dima, Groenen Anne, Linde-Ozola Zane, Kandāte Annija, Varga-Sabján Dóra, Morva Dorottya, László Noémi, and et al. 2023. "The Development of a Screening Tool for Childcare Professionals to Detect and Refer Infant and Toddler Maltreatment and Trauma: A Tale of Four Countries" Children 10, no. 5: 858. https://doi.org/10.3390/children10050858
APA StyleBisagno, E., Cadamuro, A., Serafine, D., Dima, B. M., Anne, G., Zane, L.-O., Annija, K., Dóra, V.-S., Dorottya, M., Noémi, L., Monika, R., Andrea, G., Giovanna Laura, D. F., & Johanna Maria Catharina, B. (2023). The Development of a Screening Tool for Childcare Professionals to Detect and Refer Infant and Toddler Maltreatment and Trauma: A Tale of Four Countries. Children, 10(5), 858. https://doi.org/10.3390/children10050858