
Neighborhood Socioeconomic Characteristics Associated with the COVID-19 Incidence in Elementary School Children: An Ecological Study in Osaka City, Japan



Abstract
1. Introduction
2. Materials and Methods
2.1. Target
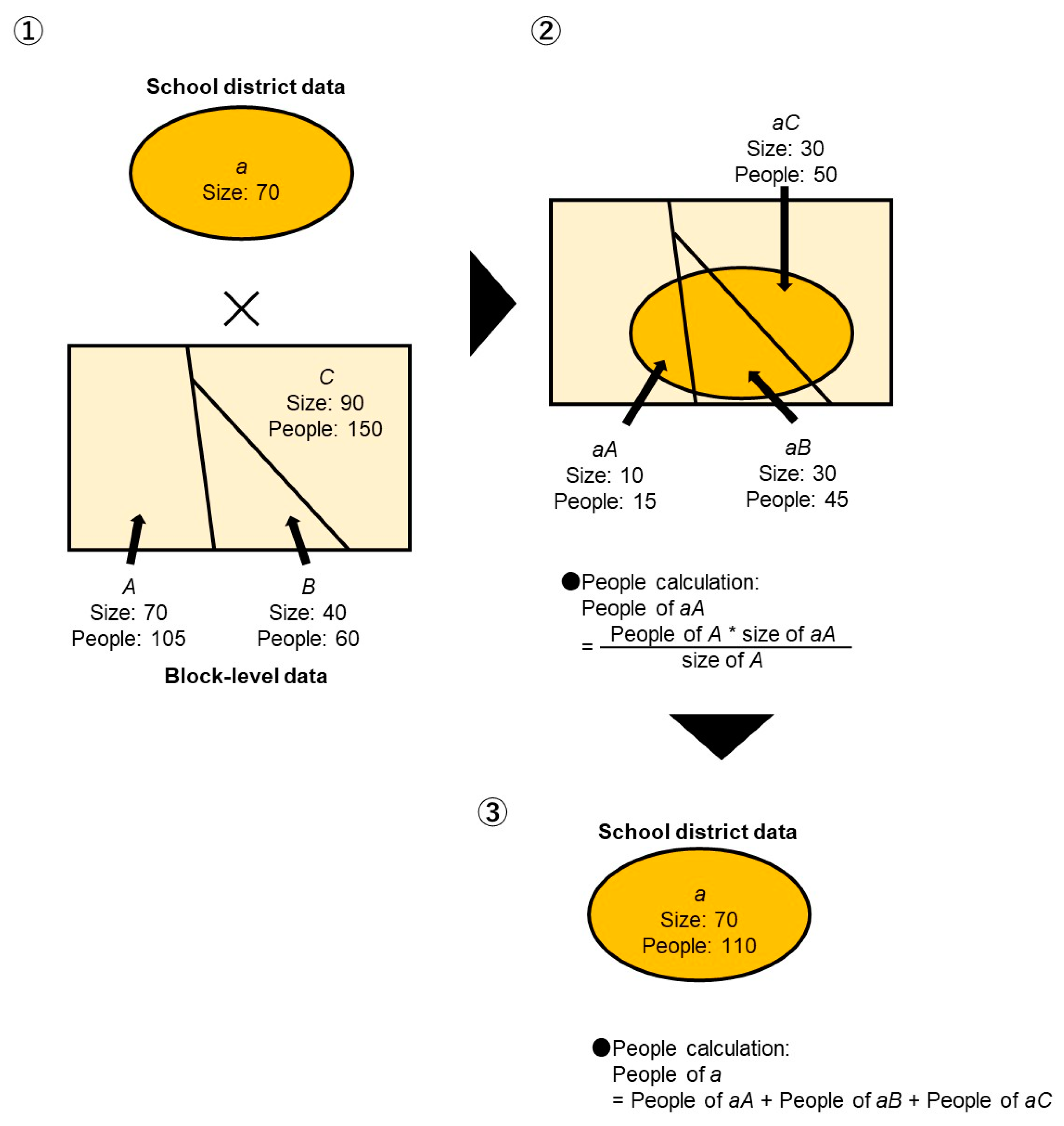
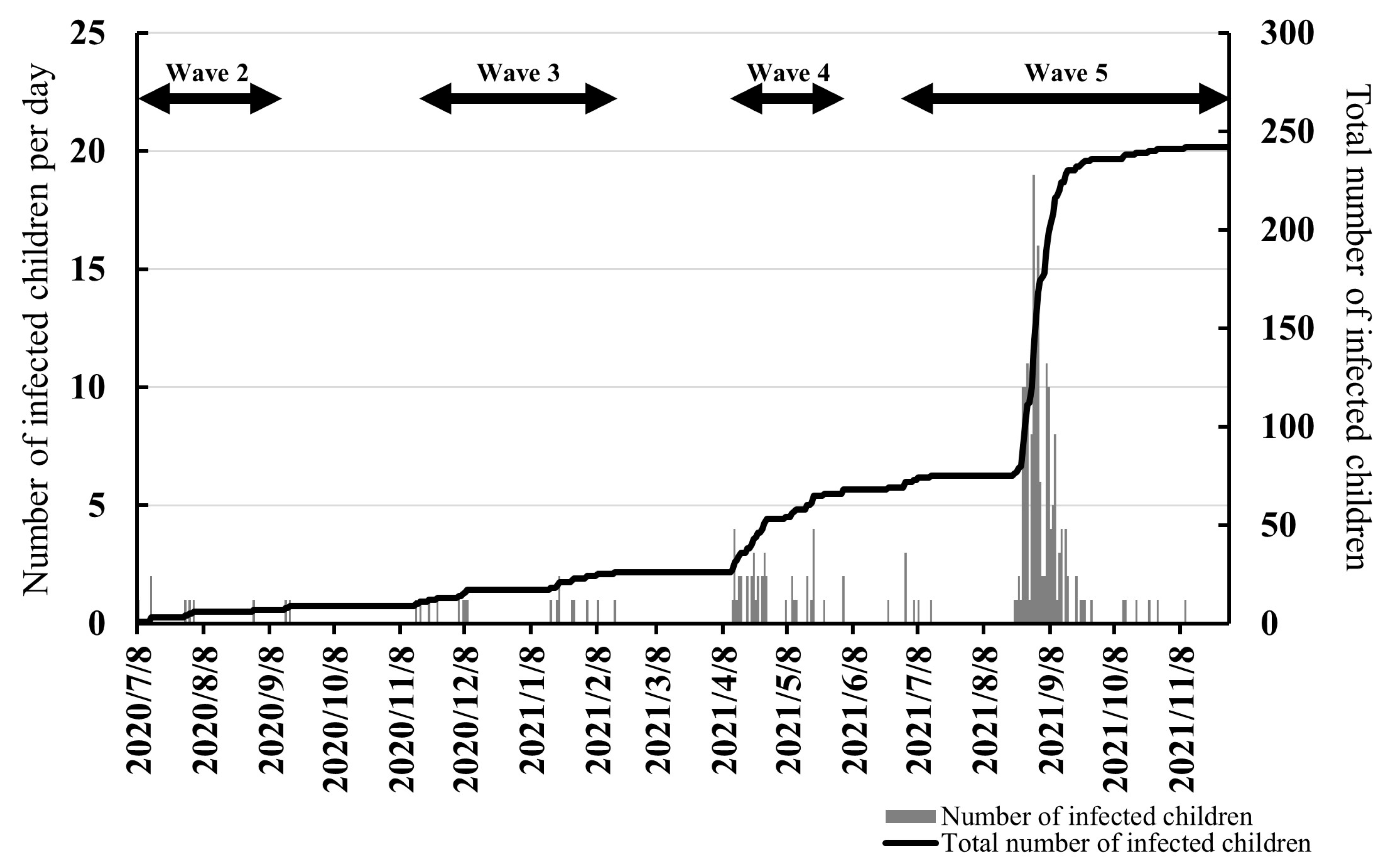
2.2. Number of Children with COVID-19 and the Total Number of Children
2.3. Investigation of Neighborhood Socioeconomic Characteristics
2.4. Proportion of Individuals Employed in Industries with Frequent Close Contact with the Public
2.5. College Graduation Rate
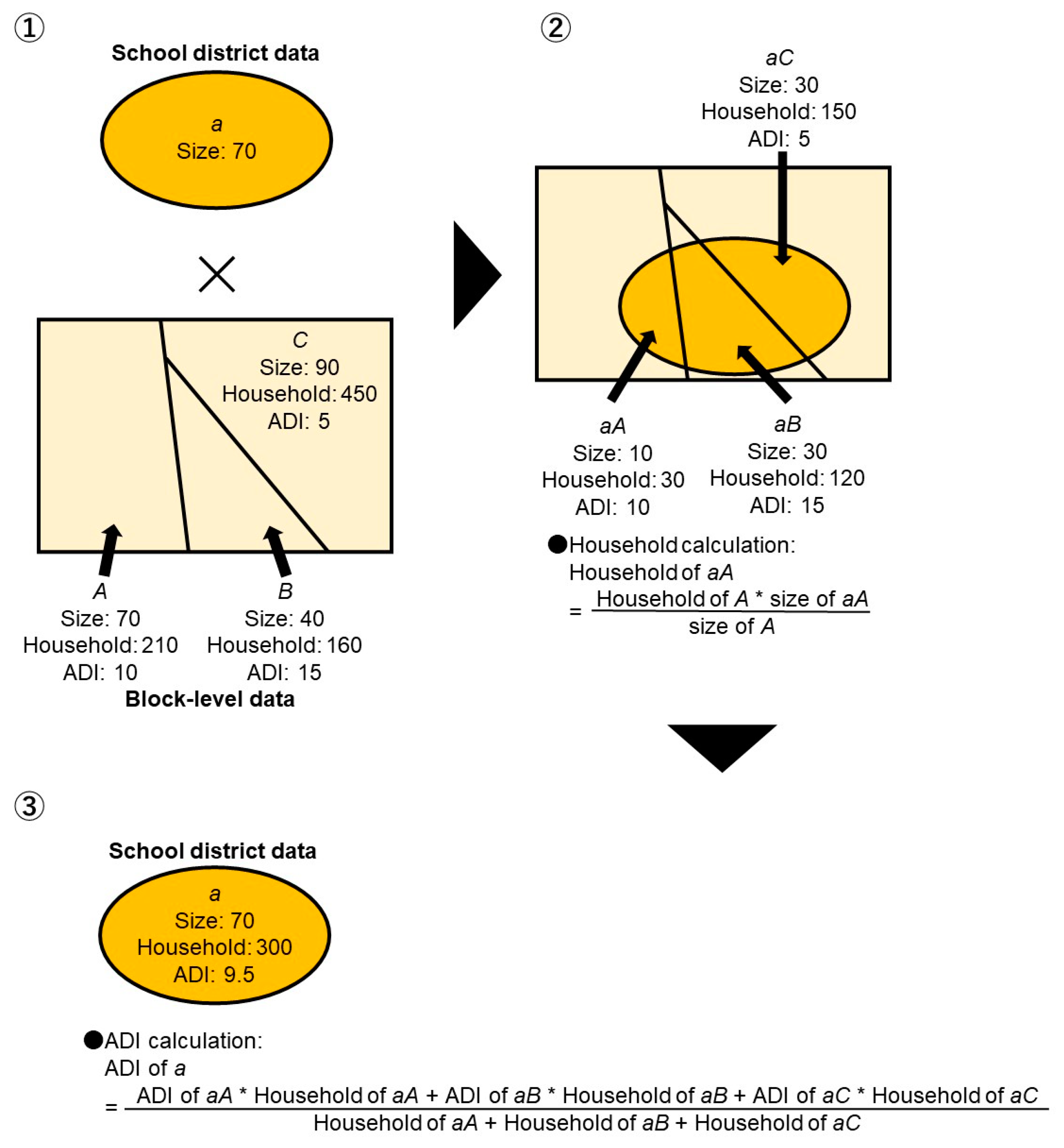
2.6. Area Deprivation Index (ADI)
2.7. Covariates
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 15 January 2022).
- Ministry of Health, Labour and Welfare, Visualizing the Data: Information on COVID-19 Infections. 2022. Available online: https://covid19.mhlw.go.jp/en/ (accessed on 10 March 2022).
- Osaka Prefectural Center for Infectious Diseases, COVID-19. Available online: http://www.iph.pref.osaka.jp/infection/disease/corona.html (accessed on 25 April 2023). (In Japanese).
- Barceló, M.A.; Saez, M. Methodological Limitations in Studies Assessing the Effects of Environmental and Socioeconomic Variables on the Spread of COVID-19: A Systematic Review. Environ. Sci. Eur. 2021, 33, 108. [Google Scholar] [CrossRef]
- Magesh, S.; John, D.; Li, W.T.; Li, Y.; Mattingly-app, A.; Jain, S.; Chang, E.Y.; Ongkeko, W.M. Disparities in COVID-19 Outcomes by Race, Ethnicity, and Socioeconomic Status. JAMA Netw. Open 2021, 4, 34147. [Google Scholar] [CrossRef] [PubMed]
- Khanijahani, A.; Iezadi, S.; Gholipour, K.; Azami-Aghdash, S.; Naghibi, D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int. J. Equity Health 2021, 20, 248. [Google Scholar] [CrossRef]
- Benita, F.; Rebollar-Ruelas, L.; Gaytán-Alfaro, E.D. What Have We Learned about Socioeconomic Inequalities in the Spread of COVID-19? A Systematic Review. Sustain. Cities Soc. 2022, 86, 104158. [Google Scholar] [CrossRef]
- Alidadi, M.; Sharifi, A. Effects of the Built Environment and Human Factors on the Spread of COVID-19: A Systematic Literature Review. Sci. Total Environ. 2022, 850, 158056. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Hosozawa, M.; Hasegawa, A.; Okubo, Y.; Sampei, M.; Sawada, N.; Piedvache, A.; Morisaki, N.; Hangai, M.; Tanaka, K.; et al. The Coronavirus Disease 2019 Pandemic and the Rights of the Child in Japan. Pediatr. Int. 2021, 64, e14913. [Google Scholar] [CrossRef] [PubMed]
- Martins-Filho, P.R.; Quintans-Júnior, L.J.; de Souza Araújo, A.A.; Sposato, K.B.; Souza Tavares, C.S.; Gurgel, R.Q.; Fontes Leite, D.C.; de Paiva, S.M.; Santos, H.P.; Santos, V.S. Socio-Economic Inequalities and COVID-19 Incidence and Mortality in Brazilian Children: A Nationwide Register-Based Study. Public Health 2021, 190, 4–6. [Google Scholar] [CrossRef]
- Society at a Glance 2019: OECD Social Indicators—OECD iLibrary. Available online: https://www.oecd-ilibrary.org/docserver/soc_glance-2019-en.pdf?expires=1555274574&id=id&accname=guest&checksum=638B78794EFD743B54BF58C7707D0038 (accessed on 29 June 2021).
- Yoshikawa, Y.; Kawachi, I. Association of Socioeconomic Characteristics with Disparities in COVID-19 Outcomes in Japan. JAMA Netw. Open 2021, 4, e2117060. [Google Scholar] [CrossRef] [PubMed]
- Osaka City Hall, Estimated Population (as of the 1st of Each Month) and Population Change. 2023. Available online: https://www.city.osaka.lg.jp/toshikeikaku/page/0000541634.html/ (accessed on 25 April 2023). (In Japanese).
- Osaka City Hall, Status of Application of Public Assistance, etc. Available online: https://www.city.osaka.lg.jp/fukushi/page/0000086901.html/ (accessed on 24 May 2022). (In Japanese).
- Ministry of Health, Labor and Welfare, Results of the National Survey on the Actual Conditions of the Homeless (Approximate Survey). Available online: https://www.mhlw.go.jp/content/12003000/000769666.pdf/2021 (accessed on 25 April 2023). (In Japanese).
- Osaka City Hall, Suspended Classes at Schools Due to Novel Coronavirus Infection. 2022. Available online: https://www.city.osaka.lg.jp/kyoiku/page/0000509375.html/ (accessed on 24 May 2022). (In Japanese).
- Osaka City Hall, Fiscal 2020 School Status Survey (as of 1 May 2021). Available online: https://www.city.osaka.lg.jp/kyoiku/page/0000511944.html/ (accessed on 24 May 2022). (In Japanese).
- Oishi, K.; Aoki, T.; Harada, T.; Tanaka, C.; Tanaka, S.; Tanaka, H.; Fukuda, K.; Kamikawa, Y.; Tsuji, N.; Komura, K.; et al. Association of Neighborhood Food Environment and Physical Activity Environment with Obesity: A Large-Scale Cross-Sectional Study of Fifth- to Ninth-Grade Children in Japan. INQUIRY J. Health Care Organ. Provis. Financ. 2021, 58, 004695802110556. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Aoki, T.; Oishi, K.; Harada, T.; Tanaka, C.; Tanaka, S.; Tanaka, H.; Fukuda, K.; Kamikawa, Y.; Tsuji, N.; et al. Neighborhood-Level Socioeconomic Factors Moderate the Association between Physical Activity and Relative Age Effect: A Cross-Sectional Survey Study with Japanese Adolescents. BMC Public Health 2022, 22, 1656. [Google Scholar] [CrossRef]
- Geo-K, L.L.C. School District (Elementary and Junior High School District Polygon and Point Database). 2018. Available online: https://www.gisdata-store.biz/product/1264/ (accessed on 10 November 2022). (In Japanese).
- Statistics Bureau of Japan, Population Census. 2015. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&toukei=00200521&tstat=000001080615/ (accessed on 15 January 2022).
- Statistics Bureau of Japan, Population Census. 2010. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&toukei=00200521&tstat=000001039448/ (accessed on 15 January 2022).
- Nakaya, T. Evaluating socio-economic inequalities in cancer mortality by using areal statistics in Japan: A note on the relation between municipal cancer mortality and areal deprivation index. Proc. Inst. Stat. Math. 2011, 59, 239–265. (In Japanese) [Google Scholar]
- Nakaya, T.; Honjo, K.; Hanibuchi, T.; Ikeda, A.; Iso, H.; Inoue, M.; Sawada, N.; Tsugane, S. Associations of All-Cause Mortality with Census-Based Neighbourhood Deprivation and Population Density in Japan: A Multilevel Survival Analysis. PLoS ONE 2014, 9, e97802. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Yoshioka, T.; Nakaya, T.; Hanibuchi, T.; Okano, H.; Ikezawa, S.; Tsuno, K.; Murayama, H.; Tabuchi, T. Urbanization level and neighborhood deprivation, not COVID-19 case numbers by residence area, are associated with severe psychological distress and new-onset suicidal ideation during the COVID-19 pandemic. J. Affect. Disord. 2021, 287, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, A.; Fukui, K.; Sato, T.; Kikuchi, H.; Inoue, S.; Kondo, N.; Nakaya, T.; Ito, Y. Geographical socioeconomic inequalities in healthy life expectancy in Japan, 2010-2014: An ecological study. Lancet Reg. Health West Pac. 2021, 14, 100204. [Google Scholar] [CrossRef]
- Osaka City Hall, 2016 Census Results by Elementary District. 2016. Available online: https://www.city.osaka.lg.jp/toshikeikaku/page/0000341916.html/ (accessed on 10 November 2022). (In Japanese).
- Ministry of Land, Infrastructure, Transport and Tourism, National Land Information Download Service. Available online: https://nlftp.mlit.go.jp/ksj/gml/datalist/KsjTmplt-P11.html/ (accessed on 29 June 2021). (In Japanese).
- Ministry of Land, Infrastructure, Transport and Tourism, National Land Information Download Service. Available online: https://nlftp.mlit.go.jp/ksj/gml/datalist/KsjTmplt-N05-v1_3.html/ (accessed on 29 June 2021). (In Japanese).
- Osaka Prefectural Government, List of Medical Treatment and Testing Institution (All Medical Institutions). 2022. Available online: https://pref-osaka.viewer.kintoneapp.com/public/0513c2014b31535d76ce0b6d4a6516e1399e3ae432a81f7b1c400569491589dc#/ (accessed on 15 January 2022). (In Japanese).
- Bui, D.P.; McCaffrey, K.; Friedrichs, M.; LaCross, N.; Lewis, N.M.; Sage, K.; Barbeau, B.; Vilven, D.; Rose, C.; Braby, S.; et al. Racial and Ethnic Disparities among COVID-19 Cases in Workplace Outbreaks by Industry Sector—Utah, 6 March 6–5 June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1133–1138. [Google Scholar] [CrossRef]
- Al-Kuwari, M.G.; Al-Nuaimi, A.A.; Abdulmajeed, J.; Semaan, S.; Al-Romaihi, H.E.; Kandy, M.C.; Swamy, S. COVID-19 Infection across Workplace Settings in Qatar: A Comparison of COVID-19 Positivity Rates of Screened Workers from March 1st until July 31st, 2020. J. Occup. Med. Toxicol. 2021, 16, 21. [Google Scholar] [CrossRef]
- Japan Tourism Agency, Go to Travel Campaign. 2020. Available online: https://www.e-stat.go.jp/stat-search?page=1&toukei=00601020&kikan=00601 (accessed on 10 November 2022). (In Japanese).
- Anzai, A.; Nishiura, H. “Go To Travel” Campaign and Travel-Associated Coronavirus Disease 2019 Cases: A Descriptive Analysis, July–August 2020. J. Clin. Med. 2021, 10, 398. [Google Scholar] [CrossRef]
- Kanamori, R.; Kawakami, Y.; Nojiri, S.; Miyazawa, S.; Kuroki, M.; Nishizaki, Y. Changes in social environment due to the state of emergency and Go To campaign during the COVID-19 pandemic in Japan: An ecological study. PLoS ONE 2022, 17, e0267395. [Google Scholar] [CrossRef]
- Uchida, M. Changes in numbers of COVID-19 cases among residents of sightseeing resort areas before and during the “Go to Travel” campaign: Descriptive epidemiology in Gunma Prefecture. Jpn. J. Infect. Dis. 2021, 74, 554–559. [Google Scholar] [CrossRef]
- Mutambudzi, M.; Niedwiedz, C.; Macdonald, E.B.; Leyland, A.; Mair, F.; Anderson, J.; Celis-Morales, C.; Cleland, J.; Forbes, J.; Gill, J.; et al. Occupation and risk of severe COVID-19: Prospective cohort study of 120 075 UK Biobank participants. Occup. Environ. Med. 2020, 78, 307–314. [Google Scholar] [CrossRef]
- Buchan, S.A.; Smith, P.M.; Warren, C.; Murti, M.; Mustard, C.; Kim, J.H.; Menon, S.; Brown, K.A.; van Ingen, T.; Smith, B.T. Incidence of outbreak-associated COVID-19 cases by industry in Ontario, Canada, 1 April 2020–31 March 2021. Occup. Environ. Med. 2022, 79, 403–411. [Google Scholar] [CrossRef]
- Hawkins, R.B.; Charles, E.J.; Mehaffey, J.H. Socio-economic status and COVID-19–related cases and fatalities. Public Health 2020, 189, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, Y.; Doba, N.; Butler, J.P.; Paasche-Orlow, M.K. Health literacy and physical and psychological wellbeing in Japanese adults. Patient Educ. Couns. 2009, 75, 411–417. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare, Preliminary Results of the 3rd Antibody Retention Survey. 2022. Available online: https://www.mhlw.go.jp/content/10900000/000898612.pdf/ (accessed on 27 April 2023). (In Japanese).
- Prime Minister’s Office of Japan and His Cabinet, COVID-19 Vaccines. 2023. Available online: https://www.kantei.go.jp/jp/headline/kansensho/vaccine.html/ (accessed on 27 April 2023). (In Japanese).
- Ministry of Health, Labor and Welfare, Preliminary Results of the 4th Antibody Retention Survey. 2022. Available online: https://www.mhlw.go.jp/content/000945078.pdf/ (accessed on 27 April 2023). (In Japanese).
- Fazel, M.; Puntis, S.; White, S.R.; Townsend, A.; Mansfield, K.L.; Viner, R.; Herring, J.; Polland, A.J.; Freeman, D. Willingness of children and adolescents to have a COVID-19 vaccination: Results of a large whole schools survey in England. EClinicalMedicine 2021, 40, 101144. [Google Scholar] [CrossRef] [PubMed]
- Scharff, A.Z.; Paulsen, M.; Schaefer, P.; Tanisik, F.; Sugianto, R.I.; Stanislawski, N.; Blume, H.; Schmidt, B.M.W.; Heiden, S.; Stiesch, M.; et al. Students’ age and parental level of education influence COVID-19 vaccination hesitancy. Eur. J. Pediatr. 2022, 181, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Lee, H.; Azuine, R.E. Marked disparities in COVID-19 vaccination among US children and adolescents by racial/ethnic, socioeconomic, geographic, and health characteristics, United States, December 2021–April 2022. Int. J. MCH AIDS 2022, 11, e598. [Google Scholar] [CrossRef]
- Japan Pediatric Society, COVID-19 pediatric Cases in Japan. 2022. Available online: https://www.coreregistry.jp/CoreRegistry_COVID19_CRF_Dashboard/Home/DashBoardviewer/ (accessed on 27 April 2023). (In Japanese).




{kind=link}
{kind=link}
{kind=link}
| Model | Objective Variable | Explanatory Variable | Covariate | Offset Term |
|---|---|---|---|---|
| Model 1 | The number of COVID-19-infected children | Input one socioeconomic characteristic at a time | None | The number of school children |
| Model 2 | The number of COVID-19-infected children | Input one socioeconomic characteristic at a time | Adjusted for population density, number of people in the household, number of public transportation, number of facilities for older adults, and number of medical treatment and testing institutions | The number of school children |
| Model 3 | The number of COVID-19-infected children | Input all socioeconomic characteristics simultaneously | None | The number of school children |
| Model 4 | The number of COVID-19-infected children | Input all socioeconomic characteristics simultaneously | Adjusted for population density, number of people in the household, number of public transportation, number of facilities for older adults, and number of medical treatment and testing institutions | The number of school children |
| Variables | Mean ± SD |
|---|---|
| Number of children with COVID-19 in Wave 2 | 0.03 ± 0.18 |
| Number of children with COVID-19 in Wave 3 | 0.06 ± 0.25 |
| Number of children with COVID-19 in Wave 4 | 0.15 ± 0.48 |
| Number of children with COVID-19 in Wave 5 | 0.62 ± 0.92 |
| Total number of children with COVID-19 | 0.86 ± 1.15 |
| School population | 402.01 ± 218.97 |
| Employment in the transportation and postal services industry (%) | 5.61 ± 2.63 |
| Employment in the wholesale and retail trade industry (%) | 16.17 ± 1.57 |
| Employment in the accommodation and food services industry (%) | 6.64 ± 1.21 |
| Employment in the health care and social assistance industry (%) | 10.74 ± 2.03 |
| College graduation rate (%) | 20.59 ± 8.31 |
| ADI | 6.79 ± 1.13 |
| Population density (10,000 people/km2) | 1.56 ± 0.62 |
| Number of people in the household (people/family) | 7.99 ± 9.36 |
| Density of public transportation (/10,000 people) | 1.94 ± 0.25 |
| Density of facilities for older adults (/10,000 people) | 1.19 ± 1.34 |
| Density of medical treatment and testing institutions (/10,000 people) | 1.22 ± 1.38 |
| Explanatory Variables | Model 1 a | Model 2 b | Model 3 c | Model 4 d | |||||
|---|---|---|---|---|---|---|---|---|---|
| IRR | (95% CI) | IRR | (95% CI) | IRR | (95% CI) | IRR | (95% CI) | ||
| Total | Employment in the transportation and postal services industry (%) | 0.97 | (0.91–1.04) | 0.99 | (0.92–1.07) | 0.92 | (0.84–1.01) | 0.93 | (0.84–1.03) |
| Employment in the wholesale and retail trade industry (%) | 1.22 *** | (1.11–1.35) | 1.18 *** | (1.07–1.31) | 1.19 *** | (1.08–1.31) | 1.17 ** | (1.06–1.29) | |
| Employment in the accommodation and food services industry (%) | 1.03 | (0.90–1.18) | 1.10 | (0.93–1.30) | 1.11 | (0.96–1.29) | 1.06 | (0.89–1.26) | |
| Employment in the health care and social assistance industry (%) | 1.07 | (1.00–1.15) | 1.05 | (0.97–1.14) | 1.09 * | (1.01–1.18) | 1.08 | (0.99–1.18) | |
| College graduation rate (%) | 0.99 | (0.98–1.01) | 0.98 | (0.96–1.00) | 0.95 * | (0.91–0.99) | 0.95 * | (0.91–0.99) | |
| ADI | 0.98 | (0.85–1.12) | 1.07 | (0.91–1.25) | 0.79 | (0.59–1.05) | 0.83 | (0.59–1.14) | |
| Wave 2 | Employment in the transportation and postal services industry (%) | 1.07 | (0.81–1.34) | 0.92 | (0.65–1.23) | 0.82 | (0.54–1.17) | 0.69 | (0.41–1.06) |
| Employment in the wholesale and retail trade industry (%) | 0.86 | (0.54–1.34) | 0.91 | (0.53–1.44) | 0.89 | (0.56–1.35) | 0.91 | (0.56–1.34) | |
| Employment in the accommodation and food services industry (%) | 1.47 | (0.88–2.17) | 2.88 ** | (1.44–5.88) | 1.65 | (0.91–2.99) | 2.85 ** | (1.33–6.43) | |
| Employment in the health care and social assistance industry (%) | 0.89 | (0.64–1.22) | 0.83 | (0.54–1.21) | 0.98 | (0.62–1.50) | 0.89 | (0.54–1.44) | |
| College graduation rate (%) | 0.92 | (0.83–1.01) | 0.94 | (0.83–1.04) | 0.78 * | (0.60–0.98) | 0.90 | (0.68–1.13) | |
| ADI | 1.33 | (0.75–2.00) | 1.33 | (0.63–2.51) | 0.37 | (0.09–1.24) | 0.80 | (0.16–3.04) | |
| Wave 3 | Employment in the transportation and postal services industry (%) | 1.05 | (0.85–1.24) | 1.08 | (0.86–1.30) | 1.27 | (0.97–1.60) | 1.22 | (0.89–1.64) |
| Employment in the wholesale and retail trade industry (%) | 1.35 * | (0.99–1.80) | 1.39 * | (1.01–1.85) | 1.28 | (0.96–1.68) | 1.32 | (0.97–1.76) | |
| Employment in the accommodation and food services industry (%) | 1.07 | (0.68–1.57) | 1.03 | (0.59–1.68) | 1.02 | (0.60–1.70) | 0.99 | (0.54–1.71) | |
| Employment in the health care and social assistance industry (%) | 0.81 | (0.63–1.02) | 0.76 | (0.56–1.01) | 0.89 | (0.67–1.15) | 0.90 | (0.63–1.24) | |
| College graduation rate (%) | 1.04 | (0.99–1.09) | 1.02 | (0.96–1.08) | 1.01 | (0.89–1.14) | 1.00 | (0.85–1.16) | |
| ADI | 0.53 * | (0.30–0.88) | 0.61 | (0.31–1.12) | 0.41 | (0.15–1.16) | 0.47 | (0.10–1.89) | |
| Wave 4 | Employment in the transportation and postal services industry (%) | 0.94 | (0.78–1.12) | 0.98 | (0.78–1.20) | 0.81 | (0.61–1.04) | 0.83 | (0.61–1.09) |
| Employment in the wholesale and retail trade industry (%) | 1.38 ** | (1.06–1.85) | 1.34 * | (1.03–1.79) | 1.41 ** | (1.07–1.90) | 1.34 * | (1.02–1.80) | |
| Employment in the accommodation and food services industry (%) | 1.18 | (0.83–1.65) | 1.16 | (0.76–1.76) | 1.15 | (0.78–1.68) | 1.05 | (0.66–1.63) | |
| Employment in the health care and social assistance industry (%) | 0.97 | (0.57–1.19) | 0.98 | (0.79–1.23) | 0.97 | (0.78–1.20) | 1.00 | (0.78–1.27) | |
| College graduation rate (%) | 0.98 | (0.93–1.03) | 0.96 | (0.91–1.02) | 0.92 | (0.82–1.03) | 0.91 | (0.80–1.03) | |
| ADI | 1.05 | (0.73–1.46) | 1.09 | (0.74–1.58) | 0.92 | (0.43–1.75) | 0.86 | (0.37–1.77) | |
| Wave 5 | Employment in the transportation and postal services industry (%) | 0.97 | (0.90–1.04) | 0.98 | (0.90–1.07) | 0.91 | (0.82–1.01) | 0.94 | (0.83–1.05) |
| Employment in the wholesale and retail trade industry (%) | 1.19 ** | (1.06–1.33) | 1.16 ** | (1.03–1.30) | 1.16 ** | (1.04–1.29) | 1.15 * | (1.03–1.29) | |
| Employment in the accommodation and food services industry (%) | 0.98 | (0.83–1.13) | 1.04 | (0.85–1.26) | 1.08 | (0.91–1.29) | 1.02 | (0.83–1.25) | |
| Employment in the health care and social assistance industry (%) | 1.13 ** | (1.04–1.22) | 1.12 * | (1.02–1.22) | 1.15 ** | (1.05–1.25) | 1.16 ** | (1.05–1.28) | |
| College graduation rate (%) | 0.99 | (0.97–1.01) | 0.98 | (0.96–1.01) | 0.95 * | (0.91–1.00) | 0.94 * | (0.90–0.99) | |
| ADI | 0.99 | (0.85–1.16) | 1.08 | (0.90–1.29) | 0.80 | (0.57–1.11) | 0.80 | (0.54–1.16) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oishi, K.; Mori, T.; Nakaya, T.; Ishii, K. Neighborhood Socioeconomic Characteristics Associated with the COVID-19 Incidence in Elementary School Children: An Ecological Study in Osaka City, Japan. Children 2023, 10, 822. https://doi.org/10.3390/children10050822
Oishi K, Mori T, Nakaya T, Ishii K. Neighborhood Socioeconomic Characteristics Associated with the COVID-19 Incidence in Elementary School Children: An Ecological Study in Osaka City, Japan. Children. 2023; 10(5):822. https://doi.org/10.3390/children10050822
Chicago/Turabian StyleOishi, Kan, Takaaki Mori, Tomoki Nakaya, and Kojiro Ishii. 2023. "Neighborhood Socioeconomic Characteristics Associated with the COVID-19 Incidence in Elementary School Children: An Ecological Study in Osaka City, Japan" Children 10, no. 5: 822. https://doi.org/10.3390/children10050822
APA StyleOishi, K., Mori, T., Nakaya, T., & Ishii, K. (2023). Neighborhood Socioeconomic Characteristics Associated with the COVID-19 Incidence in Elementary School Children: An Ecological Study in Osaka City, Japan. Children, 10(5), 822. https://doi.org/10.3390/children10050822