
The Incidence of Clubfoot in the Czech Republic: A Nationwide Epidemiological Study from 2000 to 2014

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Incidence of Clubfoot in the Czech Republic
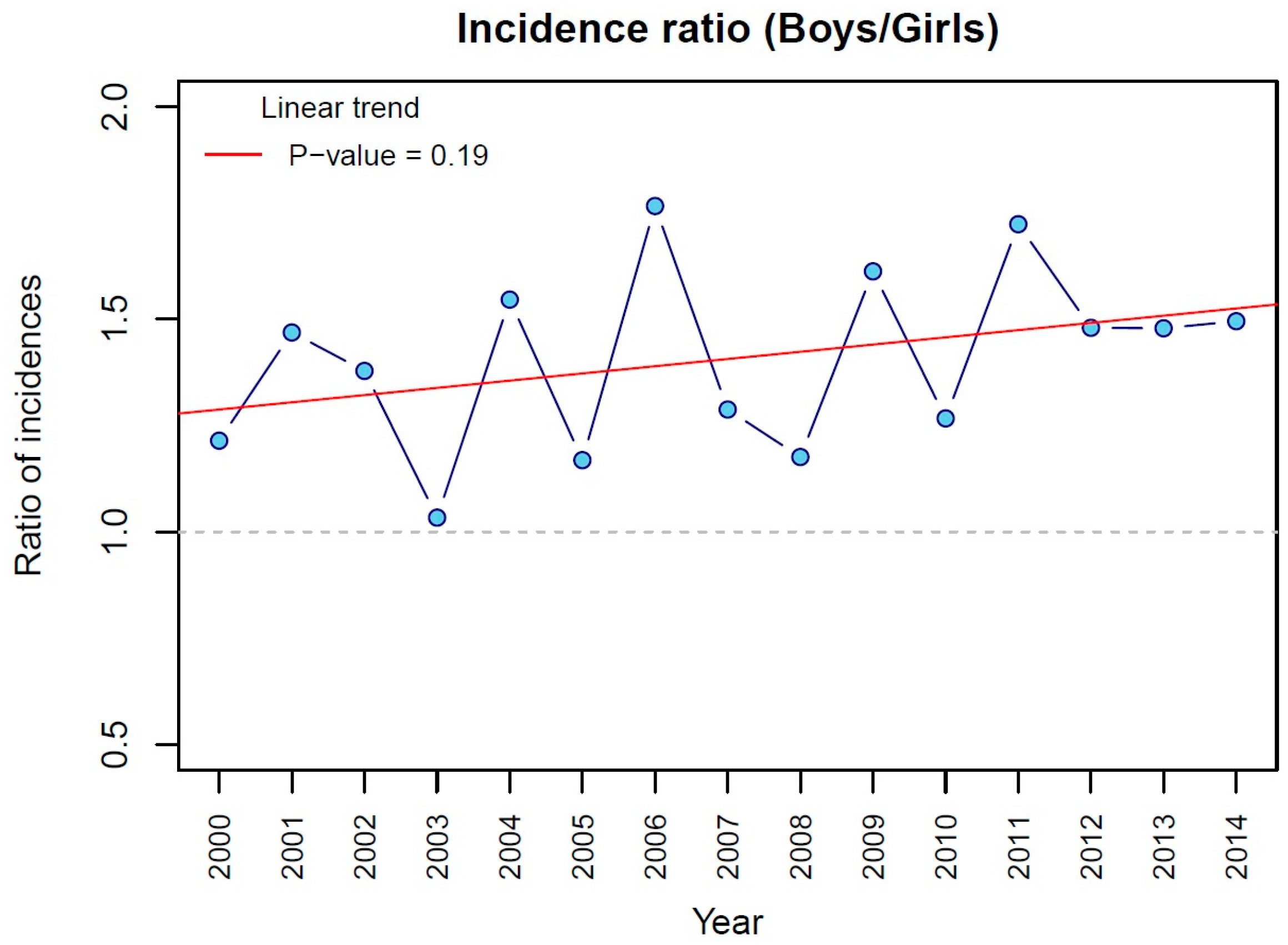
3.2. Incidence of Clubfoot According to Sex
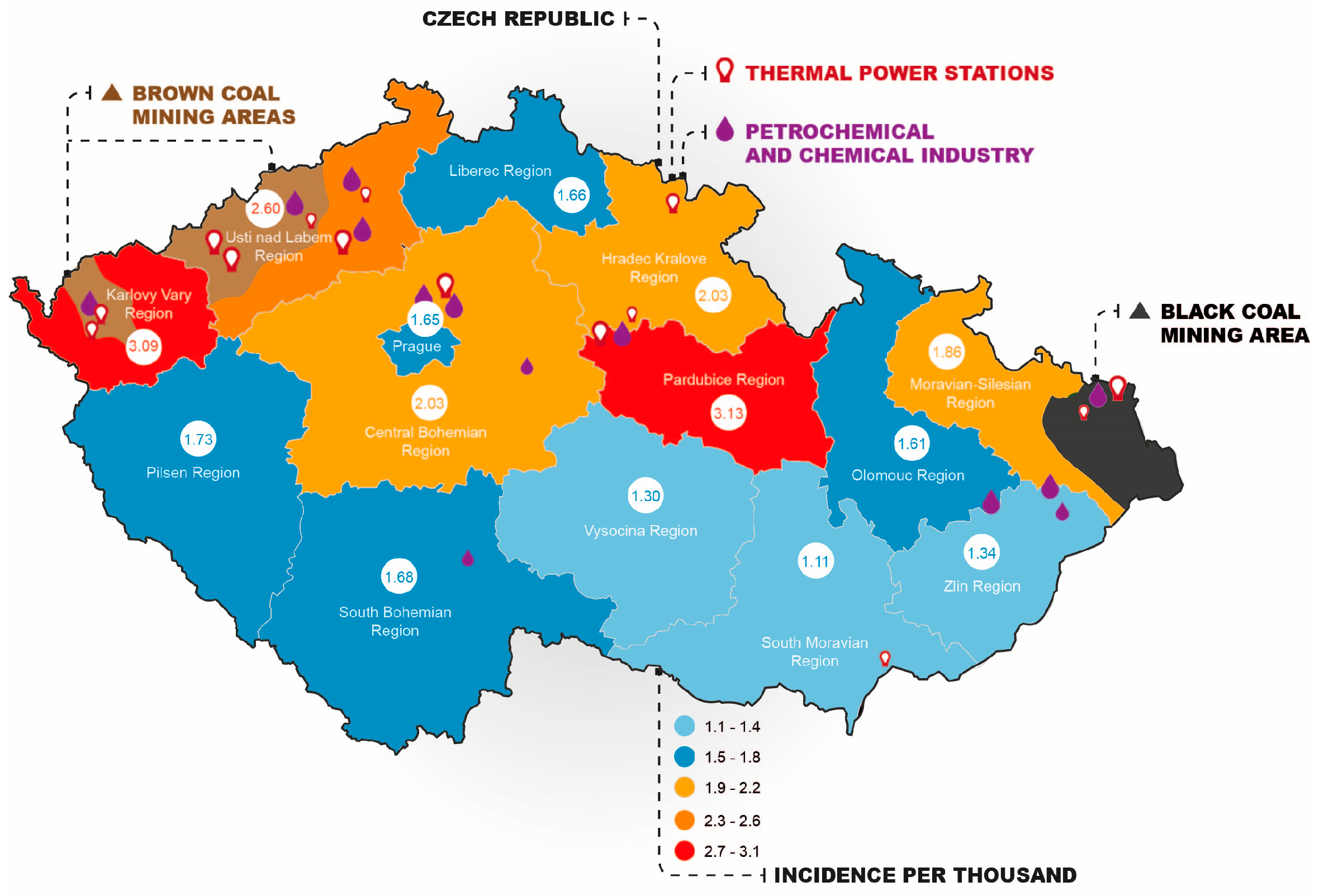
3.3. Incidence of Clubfoot According to Geographical Distribution
4. Discussion
4.1. Incidence over Time
4.2. Boys vs. Girls
4.3. Geographical Distribution
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barker, S.; Chesney, D.; Miedzybrodzka, Z.; Maffulli, N. Current Issues Edited by Genetics and Epidemiology of Idiopathic Congenital Talipes Equinovarus. J. Pediatr. Orthop. 2003, 23, 265–272. [Google Scholar] [CrossRef]
- Dobbs, M.B.; Gurnett, C.A. Update on Clubfoot: Etiology and Treatment. Clin. Orthop. Relat. Res. 2009, 467, 1146–1153. [Google Scholar] [CrossRef]
- Pavone, V.; Chisari, E.; Vescio, A.; Lucenti, L.; Sessa, G.; Testa, G. The Etiology of Idiopathic Congenital Talipes Equinovarus: A Systematic Review. J. Orthop. Surg. Res. 2018, 13, 206. [Google Scholar] [CrossRef] [PubMed]
- Kancherla, V.; Romitti, P.A.; Caspers, K.M.; Puzhankara, S.; Morcuende, J.A. Epidemiology of Congenital Idiopathic Talipes Equinovarus in Iowa, 1997–2005. Am. J. Med. Genet. Part A 2010, 152, 1695–1700. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, P.J.; Gray, K. Update on Clubfoot. J. Paediatr. Child Health 2013, 49, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Keret, D.; Ezra, E.; Lokiec, F.; Hayek, S.; Segev, E.; Wientroub, S. Efficacy of Prenatal Ultrasonography in Confirmed Club Foot. J. Bone Jt. Surg.—Ser. B 2002, 84, 1015–1019. [Google Scholar] [CrossRef]
- Shabtai, L.; Specht, S.C.; Herzenberg, J.E. Worldwide Spread of the Ponseti Method for Clubfoot. World J. Orthop. 2014, 5, 585–590. [Google Scholar] [CrossRef]
- López-Carrero, E.; Castillo-López, J.M.; Medina-Alcantara, M.; Domínguez-Maldonado, G.; Garcia-Paya, I.; Jiménez-Cebrián, A.M. Effectiveness of the Ponseti Method in the Treatment of Clubfoot: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3714. [Google Scholar] [CrossRef]
- Herzenberg, J.E.; Radler, C.; Bor, N. Ponseti versus Traditional Methods of Casting for Idiopathic Clubfoot. J. Pediatr. Orthop. 2002, 22, 517–521. [Google Scholar] [CrossRef]
- Dobbs, M.B.; Nunley, R.; Schoenecker, P.L. Long-Term Follow-up of Patients with Clubfeet Treated with Extensive Soft-Tissue Release. J. Bone Jt. Surg. 2006, 88, 2536. [Google Scholar] [CrossRef]
- Balasankar, G.; Luximon, A.; Al-Jumaily, A. Current Conservative Management and Classification of Club Foot: A Review. J. Pediatr. Rehabil. Med. 2016, 9, 257–264. [Google Scholar] [CrossRef]
- Dobbs, M.; Garg, S. Use of the Ponseti Method for Recurrent Clubfoot Following Posteromedial Release. Indian J. Orthop. 2008, 42, 68. [Google Scholar] [CrossRef]
- Gurnett, C.A.; Boehm, S.; Connolly, A.; Reimschisel, T.; Dobbs, M.B. Impact of Congenital Talipes Equinovarus Etiology on Treatment Outcomes. Dev. Med. Child Neurol. 2008, 50, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, M.B.; Rudzki, J.R.; Purcell, D.B.; Walton, T.; Porter, K.R.; Gurnett, C.A. Factors Predictive of Outcome after Use of the Ponseti Method for the Treatment of Idiopathic Clubfeet. J. Bone Jt. Surg.—Ser. A 2004, 86, 22–27. [Google Scholar] [CrossRef]
- Dobbs, M.B.; Morcuende, J.A.; Gurnett, C.A.; Ponseti, I.V. Treatment of Idiopathic Clubfoot: An Historical Review. Iowa Orthop. J. 2000, 20, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Ponseti, I.V.; Campos, J. The Classic: Observations on Pathogenesis and Treatment of Congenital Clubfoot. Clin. Orthop. Relat. Res. 2009, 467, 1124–1132. [Google Scholar] [CrossRef]
- Ponseti, I.V.; Smoley, E.N. The Classic: Congenital Club Foot: The Results of Treatment. Clin. Orthop. Relat. Res. 2009, 467, 1133–1145. [Google Scholar] [CrossRef]
- Mosca, V.S. Clubfoot Pathoanatomy—Biomechanics of Deformity Correction: A Narrative Review. Ann. Transl. Med. 2021, 9, 1096. [Google Scholar] [CrossRef]
- Dobbs, M.B.; Gurnett, C.A. The 2017 ABJS Nicolas Andry Award: Advancing Personalized Medicine for Clubfoot Through Translational Research. Clin. Orthop. Relat. Res. 2017, 475, 1716–1725. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, E.; Gorgolini, G. Clubfoot Pathology in Fetus and Pathogenesis. A New Pathogenetic Theory Based on Pathology, Imaging Findings and Biomechanics-a Narrative Review. Ann. Transl. Med. 2021, 9, 1095–1115. [Google Scholar] [CrossRef]
- Farrell, S.A.; Summers, A.M.; Dallaire, L.; Singer, J.; Johnson, J.A.M.; Wilson, R.D. Club Foot, an Adverse Outcome of Early Amniocentesis: Disruption or Deformation? J. Med. Genet. 1999, 36, 843–846. [Google Scholar] [PubMed]
- Nikkilä, A.; Valentin, L.; Thelin, A.; Jörgensen, C. Early Amniocentesis and Congenital Foot Deformities. Fetal Diagn. Ther. 2002, 17, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, K.C.; Meyer, R.E.; Kotch, J. Maternal Smoking and the Risk for Clubfoot in Infants. Birth Defects Res. Part A—Clin. Mol. Teratol. 2008, 82, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Dodwell, E.; Risoe, P.; Wright, J. Factors Associated With Increased Risk of Clubfoot: A Norwegian National Cohort Analysis. J. Pediatr. Orthop. 2015, 35, e104–e109. [Google Scholar] [CrossRef]
- Honein, M.A.; Paulozzi, L.J.; Moore, C.A. Family History, Maternal Smoking, and Clubfoot: An Indication of a Gene-Environment Interaction. Am. J. Epidemiol. 2000, 152, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Skelly, A.C.; Holt, V.L.; Mosca, V.S.; Alderman, B.W. Talipes Equinovarus and Maternal Smoking: A Population-Based Case-Control Study in Washington State. Teratology 2002, 66, 91–100. [Google Scholar] [CrossRef]
- Wang, H.; Barisic, I.; Loane, M.; Addor, M.C.; Bailey, L.M.; Gatt, M.; Klungsoyr, K.; Mokoroa, O.; Nelen, V.; Neville, A.J.; et al. Congenital Clubfoot in Europe: A Population-Based Study. Am. J. Med. Genet. Part A 2019, 179, 595–601. [Google Scholar] [CrossRef]
- ÚZIS ČR. Vrozené Vady u Narozených v Roce 2011; ÚZIS ČR: Prague, Czech Republic, 2013; ISBN 978-80-7472-088-8.
- ÚZIS ČR. MKN-10: Mezinárodní Klasifikace Nemocí a Přidružených Zdravotních Problémů, 10th ed.; ÚZIS ČR: Prague, Czech Republic, 2020.
- Pavone, V.; Bianca, S.; Grosso, G.; Pavone, P.; Mistretta, A.; Longo, M.R.; Marino, S.; Sessa, G. Congenital Talipes Equinovarus: An Epidemiological Study in Sicily. Acta Orthop. 2012, 83, 294–298. [Google Scholar] [CrossRef]
- Krogsgaard, M.R.; Jensen, P.K.; Kjær, I.; Husted, H.; Lorentzen, J.; Hvass-Christensen, B.; Christensen, S.B.; Larsen, K.; Sonne-Holm, S. Increasing Incidence of Club Foot with Higher Population Density: Incidence and Geographical Variation in Denmark over a 16-Year Period—An Epidemiological Study of 936,525 Births. Acta Orthop. 2006, 77, 839–846. [Google Scholar] [CrossRef]
- Wallander, H.; Hovelius, L.; Michaelsson, K. Incidence of Congenital Clubfoot in Sweden. Acta Orthop. 2006, 77, 847–852. [Google Scholar] [CrossRef]
- Wallander, H.M. Congenital Clubfoot: Aspects on Epidemiology, Residual Deformity and Patient Reported Outcome. Acta Orthop. 2010, 81, 339. [Google Scholar] [CrossRef]
- Engesæter, L.B. Increasing Incidence of Clubfoot: Changes in the Genes or the Environment? Acta Orthop. 2006, 77, 837–838. [Google Scholar] [CrossRef] [PubMed]
- Paton, R.W.; Fox, A.E.; Foster, A.; Fehily, M. Incidence and Aetiology of Talipes Equino-Varus with Recent Population Changes. Acta Orthop. Belg. 2010, 76, 86–89. [Google Scholar] [PubMed]
- Carey, M.; Bower, C.; Mylvaganam, A.; Rouse, I. Talipes Equinovarus in Western Australia. Paediatr. Perinat. Epidemiol. 2003, 17, 187–194. [Google Scholar] [CrossRef]
- Moorthi, R.N.; Hashmi, S.S.; Langois, P.; Canfield, M.; Waller, D.K.; Hecht, J.T. Idiopathic Talipes Equinovarus (ITEV) (Clubfeet) in Texas. Am. J. Med. Genet. 2005, 132A, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Byron-Scott, R.; Sharpe, P.; Hasler, C.; Cundy, P.; Hirte, C.; Chan, A.; Scott, H.; Baghurst, P.; Haan, E. A South Australian Population-Based Study of Congenital Talipes Equinovarus. Paediatr. Perinat. Epidemiol. 2005, 19, 227–237. [Google Scholar] [CrossRef]
- Barker, S.L.; Macnicol, M.F. Seasonal Distribution of Idiopathic Congenital Talipes Equinovarus in Scotland. J. Pediatr. Orthop. Part B 2002, 11, 129–133. [Google Scholar]
- ÚZIS ČR. Vrozené Vady u Narozených v Roce 2011—Aktuální Informace č. 47/2013; ÚZIS ČR: Prague, Czech Republic, 2013.
- Parker, S.E.; Mai, C.T.; Strickland, M.J.; Olney, R.S.; Rickard, R.; Marengo, L.; Wang, Y.; Hashmi, S.S.; Meyer, R.E. Multistate Study of the Epidemiology of Clubfoot. Birth Defects Res. Part A—Clin. Mol. Teratol. 2009, 85, 897–904. [Google Scholar] [CrossRef]
- Sípek, A.; Gregor, V.; Sípek, A.; Horácek, J.; Vencálek, O.; Langhammer, P.; Petrzílková, L.; Wiesnerová, J. [Birth Defects in Births in the Czech Republic Regions in 1994–2007]. TT—Vrozené Vady u Narozených Detí v Jednotlivých Krajích Ceské Republiky v Období Let 1994–2007. Ces. Gynekol. 2010, 75, 15–40. [Google Scholar]
- Pinto, J.P.; Stevens, R.K.; Willis, R.D.; Kellogg, R.; Mamane, Y.; Novak, J.; Šantroch, J.; Beneš, I.; Leniček, J.; Bureš, V. Czech Air Quality Monitoring and Receptor Modeling Study. Environ. Sci. Technol. 1998, 32, 843–854. [Google Scholar] [CrossRef]
- Hůnová, I. Ambient Air Quality in the Czech Republic: Past and Present. Atmosphere 2020, 11, 214. [Google Scholar] [CrossRef]
- Renner, E. The Black Triangle Area—Fit for Europe? Numerical Air Quality Studies for the Black Triangle Area. Ambio 2002, 31, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Cardy, A.H.; Barker, S.; Chesney, D.; Sharp, L.; Maffulli, N.; Miedzybrodzka, Z. Pedigree Analysis and Epidemiological Features of Idiopathic Congenital Talipes Equinovarus in the United Kingdom: A Case-Control Study. BMC Musculoskelet. Disord. 2007, 8, 62. [Google Scholar] [CrossRef] [PubMed]
- Ragothaman, A.; Anderson, W.A. Air Quality Impacts of Petroleum Refining and Petrochemical Industries. Environments 2017, 4, 66. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | No. of Children with Clubfoot | No. of Children Born Alive | Incidence per Thousand |
|---|---|---|---|
| 2000 | 205 | 90,910 | 2.3 |
| 2001 | 194 | 90,715 | 2.1 |
| 2002 | 150 | 92,786 | 1.6 |
| 2003 | 182 | 93,685 | 1.9 |
| 2004 | 161 | 97,664 | 1.6 |
| 2005 | 183 | 102,211 | 1.8 |
| 2006 | 173 | 105,831 | 1.6 |
| 2007 | 213 | 114,632 | 1.9 |
| 2008 | 235 | 119,570 | 2.0 |
| 2009 | 217 | 118,348 | 1.8 |
| 2010 | 241 | 117,153 | 2.1 |
| 2011 | 217 | 108,673 | 2.0 |
| 2012 | 232 | 108,576 | 2.1 |
| 2013 | 189 | 106,751 | 1.8 |
| 2014 | 165 | 109,860 | 1.5 |
| Total | 2957 | 1,577,365 | 1.9 (95% CI 1.8–2.0) |
| Boys | 1755 | 809,676 | 2.2 (95% CI 2.0–2.3) |
| Girls | 1202 | 767,689 | 1.6 (95% CI 1.4–1.7) |
| Year | Boys Incidence per Thousand | Girls Incidence per Thousand |
|---|---|---|
| 2000 | 2.5 | 2.0 |
| 2001 | 2.5 | 1.7 |
| 2002 | 1.9 | 1.4 |
| 2003 | 2.0 | 1.9 |
| 2004 | 2.0 | 1.3 |
| 2005 | 1.9 | 1.6 |
| 2006 | 2.1 | 1.2 |
| 2007 | 2.1 | 1.6 |
| 2008 | 2.1 | 1.8 |
| 2009 | 2.3 | 1.4 |
| 2010 | 2.3 | 1.8 |
| 2011 | 2.5 | 1.5 |
| 2012 | 2.5 | 1.7 |
| 2013 | 2.1 | 1.4 |
| 2014 | 1.8 | 1.2 |
| Total | 2.2 (95% CI 2.0–2.3) | 1.6 (95% CI 1.4–1.7) |
| Region | Native Births | Clubfoot Children | Incidence in Total | Incidence Boys | Incidence Girls | |
|---|---|---|---|---|---|---|
| 1. | Prague | 187,934 | 310 | 1.6 (1.4–1.9) | 2.1 (1.8–2.5) | 1.1 (0.9–1.4) |
| 2. | Central Bohemian | 194,935 | 396 | 2.0 (1.9–2.2) | 2.4 (2.1–2.7) | 1.6 (1.4–1.9) |
| 3. | South Bohemian | 95,003 | 160 | 1.7 (1.5–1.9) | 2.1 (1.8–2.3) | 1.3 (1.0–1.6) |
| 4. | Plzeň | 83,432 | 144 | 1.7 (1.4–2.1) | 1.9 (1.4–2.4) | 1.5 (1.0–2.0) |
| 5. | Karlovy Vary | 45,936 | 142 | 3.1 (2.4–3.8) | 3.2 (2.2–4.1) | 3.0 (2.0–4.0) |
| 6. | Ústí nad Labem | 130,558 | 340 | 2.6 (2.2–3.0) | 3.0 (2.6–3.5) | 2.2 (1.7–2.6) |
| 7. | Liberec | 68,136 | 113 | 1.7 (1.3–2.0) | 1.9 (1.3–2.4) | 1.4 (1.0–1.8) |
| 8. | Hradec Králové | 82,579 | 168 | 2.0 (1.6–2.4) | 2.5 (2.0–2.9) | 1.6 (1.0–2.2) |
| 9. | Pardubice | 77,365 | 242 | 3.1 (2.5–3.8) | 3.1 (2.6–3.7) | 3.1 (2.2–4.0) |
| 10. | Vysočina | 76,164 | 99 | 1.3 (1.1–1.5) | 1.6 (1.3–1.9) | 1.0 (0.6–1.4) |
| 11. | South Moravian | 174,288 | 194 | 1.1 (0.9–1.3) | 1.2 (1.0–1.5) | 1.0 (0.8–1.2) |
| 12. | Olomouc | 94,688 | 152 | 1.6 (1.3–1.9) | 1.7 (1.3–2.2) | 1.5 (1.2–1.8) |
| 13. | Zlín | 84,051 | 113 | 1.3 (1.1–1.6) | 1.6 (1.3–2.0) | 1.0 (0.8–1.3) |
| 14. | Moravian-Silesian | 182,296 | 339 | 1.9 (1.6–2.1) | 2.1 (1.8–2.4) | 1.6 (1.2–1.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janatová, K.; Nováková, T.; Lopot, F. The Incidence of Clubfoot in the Czech Republic: A Nationwide Epidemiological Study from 2000 to 2014. Children 2023, 10, 714. https://doi.org/10.3390/children10040714
Janatová K, Nováková T, Lopot F. The Incidence of Clubfoot in the Czech Republic: A Nationwide Epidemiological Study from 2000 to 2014. Children. 2023; 10(4):714. https://doi.org/10.3390/children10040714
Chicago/Turabian StyleJanatová, Klára, Tereza Nováková, and František Lopot. 2023. "The Incidence of Clubfoot in the Czech Republic: A Nationwide Epidemiological Study from 2000 to 2014" Children 10, no. 4: 714. https://doi.org/10.3390/children10040714
APA StyleJanatová, K., Nováková, T., & Lopot, F. (2023). The Incidence of Clubfoot in the Czech Republic: A Nationwide Epidemiological Study from 2000 to 2014. Children, 10(4), 714. https://doi.org/10.3390/children10040714