
Retrocardiac Pneumomediastinum: Description of an Unusual Case and Review of Literature
 , and
, and
Abstract
1. Introduction
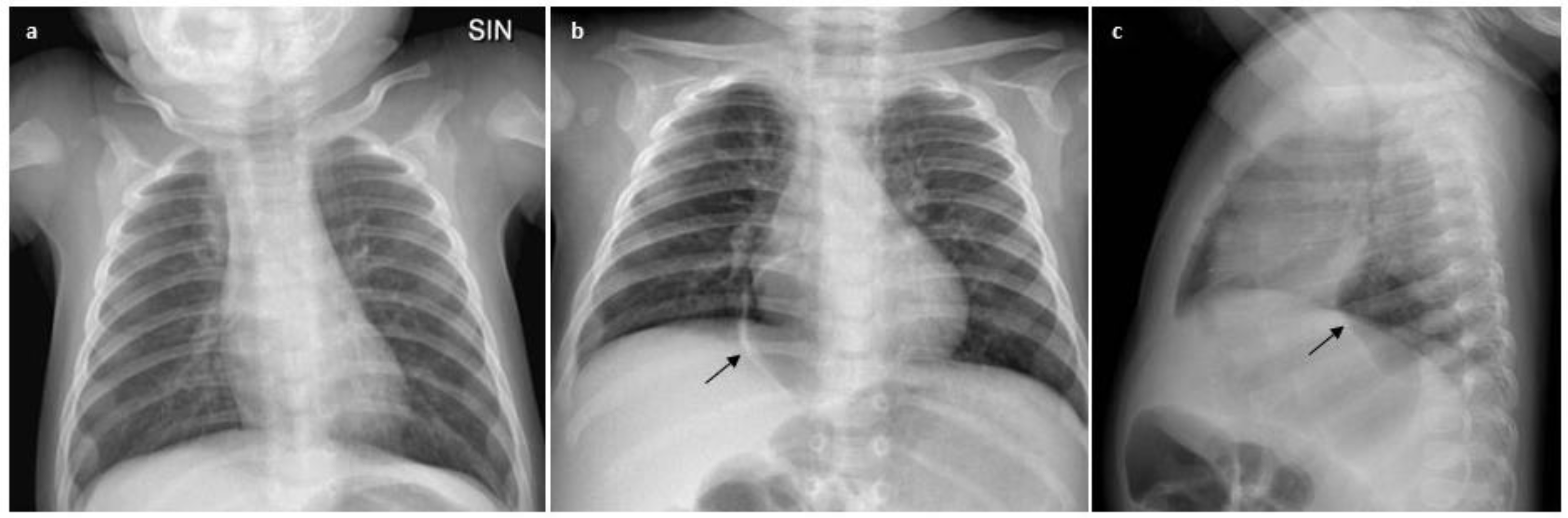
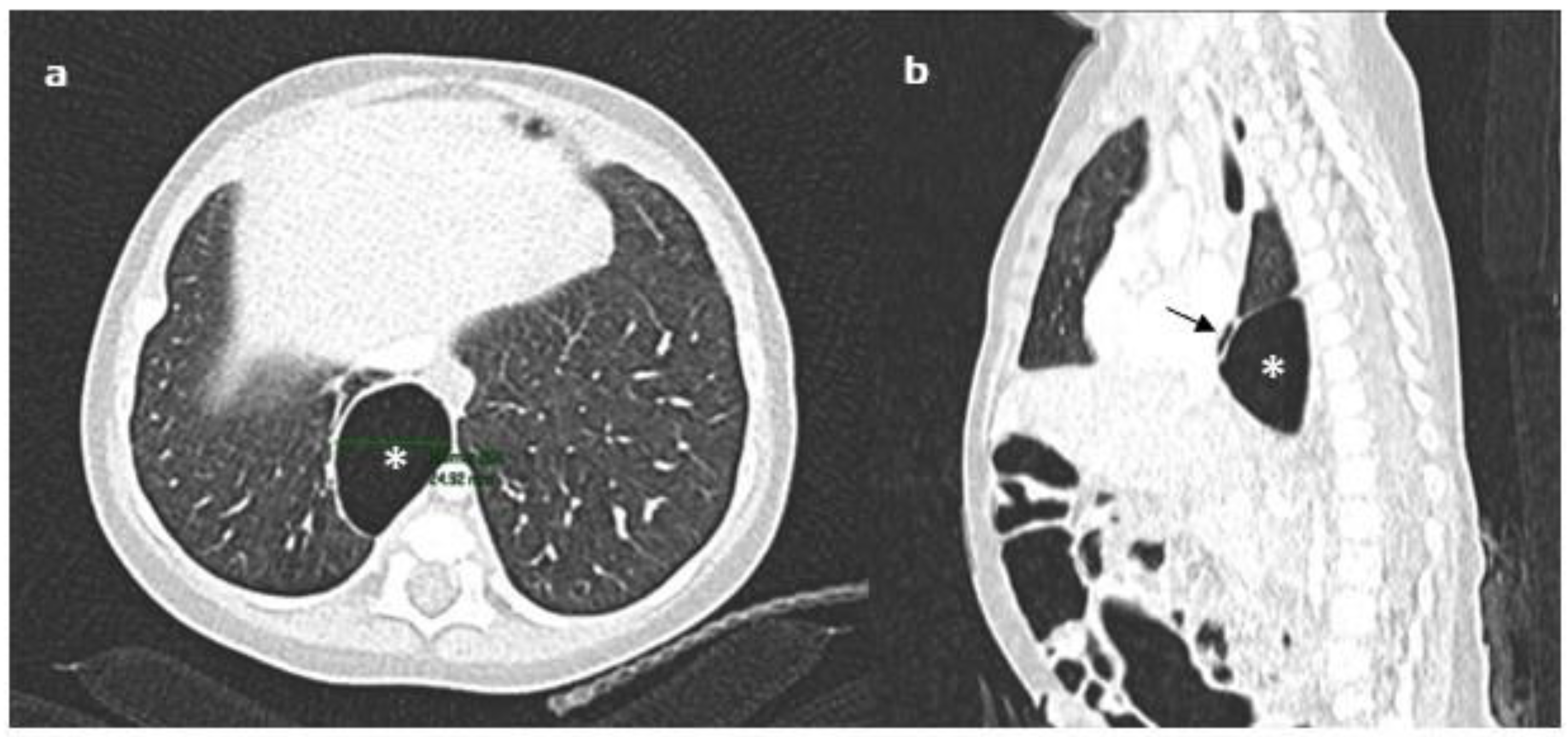
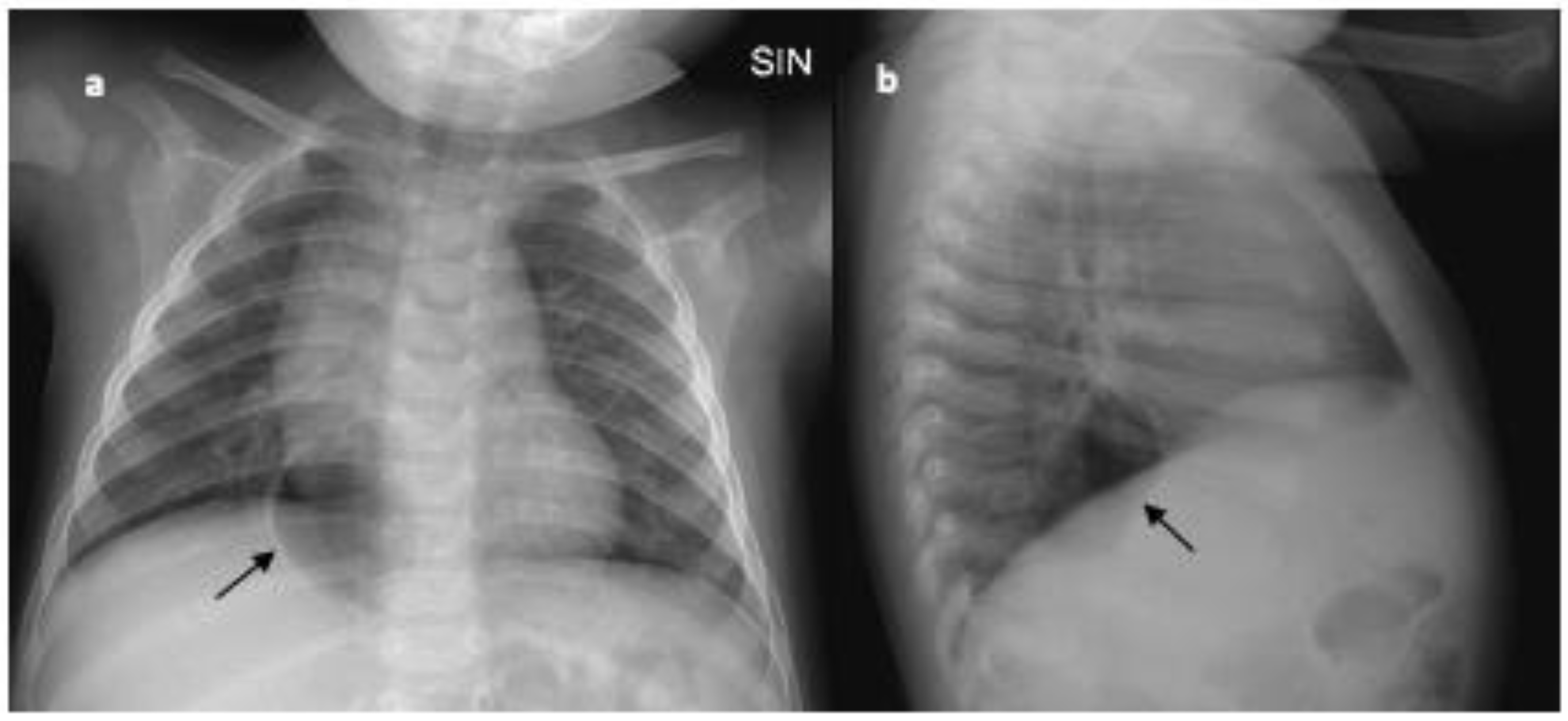
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leinert, J.L.; Perez Ortiz, A.; Rafat, N. Spontaneous Pneumomediastinum in Children with Viral Infections: Report of Three Cases Related to Rhinovirus or Respiratory Syncytial Virus Infection. Children 2022, 9, 1040. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.; Uvaise, M.; Canet-Tarres, A.; Lillie, J. Spontaneous Massive Pneumomediastinum in a Previously Well Infant with COVID-19. Pediatrics 2021, 148, e2021051904. [Google Scholar] [CrossRef] [PubMed]
- Monaco, F.; Barone, M.; Manfredi, V.G.; Marando, R.; Nunnari, F.; David, A.; Monaco, M.; Cascio, A. Pneumomediastinum as a complication of critical pertussis. Clin. Respir. J. 2016, 10, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Kouritas, V.K.; Papagiannopoulos, K.; Lazaridis, G.; Baka, S.; Mpoukovinas, I.; Karavasilis, V.; Lampaki, S.; Kioumis, I.; Pitsiou, G.; Papaiwannou, A.; et al. Pneumomediastinum. J. Thorac. Dis. 2015, 7 (Suppl. S1), S44–S49. [Google Scholar]
- Noorbakhsh, K.A.; Williams, A.E.; Langham, J.J.W.; Wu, L.; Krafty, R.T.; Furtado, A.D.; Zuckerbraun, N.S.; Manole, M.D. Management and Outcomes of Spontaneous Pneumomediastinum in Children. Pediatr. Emerg. Care 2021, 37, e1051–e1056. [Google Scholar] [CrossRef]
- Hassan, H.; Ferguson, L. Spontaneous Pneumomediastinum in a Healthy Pediatric Patient. Cureus 2021, 13, e17847. [Google Scholar] [CrossRef]
- Alahmari, A.K.; Alhelali, A.A.; Alahmari, A.K.; Ahmed, N.J.; Alkathiri, A.A.; Ardi, K.T.; Baali, M.H.; Mubarki, M.H.; Alhamoud, M.A. Pneumothorax/pneumomediastinum as a complication of foreign body inhalation in 3 pediatric patients: A case series. Medicine 2022, 101, e31073. [Google Scholar] [CrossRef]
- Ma, L.; Yin, M.; Yang, X.L.; Xu, W. Risk factors for air leakage during invasive mechanical ventilation in pediatric intensive care units. Eur. J. Med. Res. 2022, 27, 218. [Google Scholar] [CrossRef]
- Hauri-Hohl, A.; Baenziger, O.; Frey, B. Pneumomediastinum in the neonatal and paediatric intensive care unit. Eur. J. Pediatr. 2008, 167, 415–418. [Google Scholar] [CrossRef]
- Cagle, K.J. Pneumomediastinum in the neonate. Neonatal Netw. 2014, 33, 275–282. [Google Scholar] [CrossRef]
- Volberg, F.M.; Everett, C.J.; Brill, P.W. Radiologic features of inferior pulmonary ligament air collections in neonates with respiratory distress. Radiology 1979, 130, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Bowen, A.; Quattromani, F.L. Infraazygous pneumomediastinum in the newborn. AJR Am. J. Roentgenol. 1980, 135, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Morrison, S.C.; Fletcher, B.D. Infra-azygous pneumomediastinum versus pulmonary ligament air collection: CT evaluation. Pediatr. Radiol. 1985, 15, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Purohit, D.M.; Lorenzo, R.L.; Smith, C.D.; Bradford, B.F. Bronchial laceration in a newborn with persistent posterior pneumomediastinum. J. Pediatr. Surg. 1985, 20, 82–85. [Google Scholar] [CrossRef]
- Amodio, J.B.; Berdon, W.E.; Abramson, S.J.; Oh, K.S.; Oudjhane, K.; Wung, J.T. Retrocardiac pneumomediastinum in association with tracheal and esophageal perforations. Pediatr. Radiol. 1986, 16, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, D.L.; Cordell, C.E.; Jadeja, N. Retrocardiac pneumomediastinum: Radiographic finding and clinical implications. Pediatrics 1990, 85, 92–97. [Google Scholar] [CrossRef]
- Pollack, A.; Lask, P.; Kassner, E.G.; Wood, B.P. Radiological case of the month. Retrocardiac pneumomediastinum. Am. J. Dis. Child. 1992, 146, 831–832. [Google Scholar]
- Newman, B.; Oh, K.S. Iatrogenic tracheobronchial perforation in infants. J. Thorac. Imaging. 1994, 9, 269–272. [Google Scholar] [CrossRef]
- Kyle, A.; Veldtman, G.; Stanton, M.; Weeden, D.; Baral, V. Barotrauma-associated posterior tension pneumomediastinum, a rare cause of cardiac tamponade in a ventilated neonate: A case report and review of the literature. Acta Paediatr. 2012, 101, e142–e144. [Google Scholar] [CrossRef]
- Beckstrom, A.C.; Ricca, R.L.; Gow, K.W.; McAdams, R.M. Persistent posterior pneumomediastinum in a neonate. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2012, 54, 441–442. [Google Scholar] [CrossRef]
- Ponkowski, M.J.; Yadav, B.; Meagher, E.; Ho, A.; Vellody, R. Minimally invasive treatment of retrocardiac tension pneumomediastinum in an extremely low birth weight infant. Pediatr. Radiol. 2020, 50, 1624–1628. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, D.; Meyer, K.M.; Thompson, A.R.; Speck, K.E. Pediatric pneumomediastinum: Symptom-based management. J. Pediatr. Surg. 2023, 58, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.J.; Liao, C.H.; Shen, T.C. Bronchogenic cyst. QJM Mon. J. Assoc. Physicians 2018, 111, 905. [Google Scholar] [CrossRef] [PubMed]
- Hermelijn, S.M.; Elders, B.B.L.J.; Ciet, P.; Wijnen, R.M.H.; Tiddens, H.A.W.M.; Schnater, J.M. A clinical guideline for structured assessment of CT-imaging in congenital lung abnormalities. Paediatr. Respir. Rev. 2021, 37, 80–88. [Google Scholar] [CrossRef]
- Hegde, S.; Prodhan, P. Serious air leak syndrome complicating high-flow nasal cannula therapy: A report of 3 cases. Pediatrics 2013, 131, e939–e944. [Google Scholar] [CrossRef]
- Baudin, F.; Gagnon, S.; Crulli, B.; Proulx, F.; Jouvet, P.; Emeriaud, G. Modalities and Complications Associated with the Use of High-Flow Nasal Cannula: Experience in a Pediatric ICU. Respir. Care 2016, 61, 1305–1310. [Google Scholar] [CrossRef]
- Hishikawa, K.; Goishi, K.; Fujiwara, T.; Kaneshige, M.; Ito, Y.; Sago, H. Pulmonary air leak associated with CPAP at term birth resuscitation. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F382–F387. [Google Scholar] [CrossRef]
- Hung, S.C.; Hsu, H.C.; Chang, S.C. Cerebral air embolism complicating bilevel positive airway pressure therapy. Eur. Respir. J. 1998, 12, 235–237. [Google Scholar] [CrossRef]
- Hazkani, I.; Siong, T.C.; Hill, R.; Dautel, J.; Patel, M.D.; Vaughn, W.; Patzer, R.; Raol, N. The safety of respiratory positive pressure support immediately following pediatric tonsillectomy. Int. J. Pediatr. Otorhinolaryngol. 2023, 167, 111487. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | N. Preterm/Term Patients | Total Patients’ n. | Primary Cause | Symptoms | Treatment | Outcomes |
|---|---|---|---|---|---|---|
| Volberg, 1979 [11] | 12 pt 2 t | 14 | 14 IMV | RD | n.a. | n.a. |
| Bowen, 1980 [12] | 6 pt | 6 | 6 IMV | RD | n.a. | 2 Dead 3 Alive 1 n.a. |
| Morrison, 1985 [13] | 1 t | 1 | 1 IMV | RD | Conservative | Alive |
| Purohit, 1985 [14] | n.a. | 1 | n.a. | RD | Conservative | Alive |
| Amodio, 1986 [15] | 2 pt | 2 | n.a. | n.a. | n.a. | n.a. |
| Rosenfeld, 1990 [16] | 13 pt 1 t | 14 | 1 IMV 12 HMD 1 HL 1 MA | RD | n.a. | 6 Dead 8 Alive |
| Pollack, 1992 [17] | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. |
| Newman, 1994 [18] | 4 pt | 4 | IMV | RD | 2 Drainage 2 Conservative | 2 Dead 2 Alive |
| Kyle, 2011 [19] | 1 pt | 1 | IMV | RD | Drainage | Alive |
| Beckstrom, 2012 [20] | 1 pt | 1 | IMV | RD | Drainage | Alive |
| Ponkowski, 2020 [21] | 1 pt | 1 | IMV | RD | Drainage | Alive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porcaro, F.; Onofri, A.; Allegorico, A.; Tomà, P.; Cutrera, R. Retrocardiac Pneumomediastinum: Description of an Unusual Case and Review of Literature. Children 2023, 10, 649. https://doi.org/10.3390/children10040649
Porcaro F, Onofri A, Allegorico A, Tomà P, Cutrera R. Retrocardiac Pneumomediastinum: Description of an Unusual Case and Review of Literature. Children. 2023; 10(4):649. https://doi.org/10.3390/children10040649
Chicago/Turabian StylePorcaro, Federica, Alessandro Onofri, Annalisa Allegorico, Paolo Tomà, and Renato Cutrera. 2023. "Retrocardiac Pneumomediastinum: Description of an Unusual Case and Review of Literature" Children 10, no. 4: 649. https://doi.org/10.3390/children10040649
APA StylePorcaro, F., Onofri, A., Allegorico, A., Tomà, P., & Cutrera, R. (2023). Retrocardiac Pneumomediastinum: Description of an Unusual Case and Review of Literature. Children, 10(4), 649. https://doi.org/10.3390/children10040649