

The Use of Automated Atrial CMR Measures and a Novel Atrioventricular Coupling Index for Predicting Risk in Repaired Tetralogy of Fallot
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Data
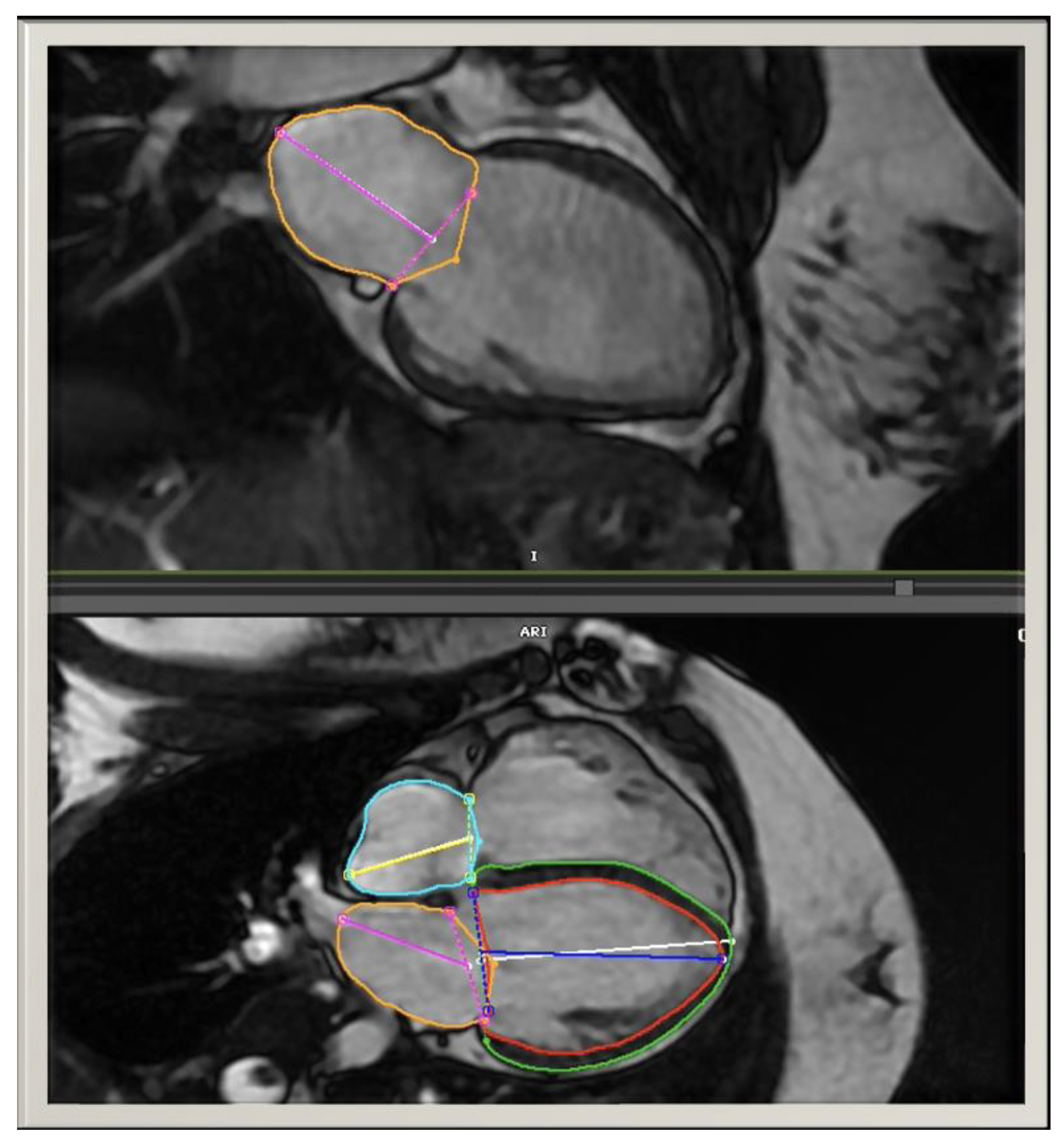
2.3. CMR
2.4. Risk Scores
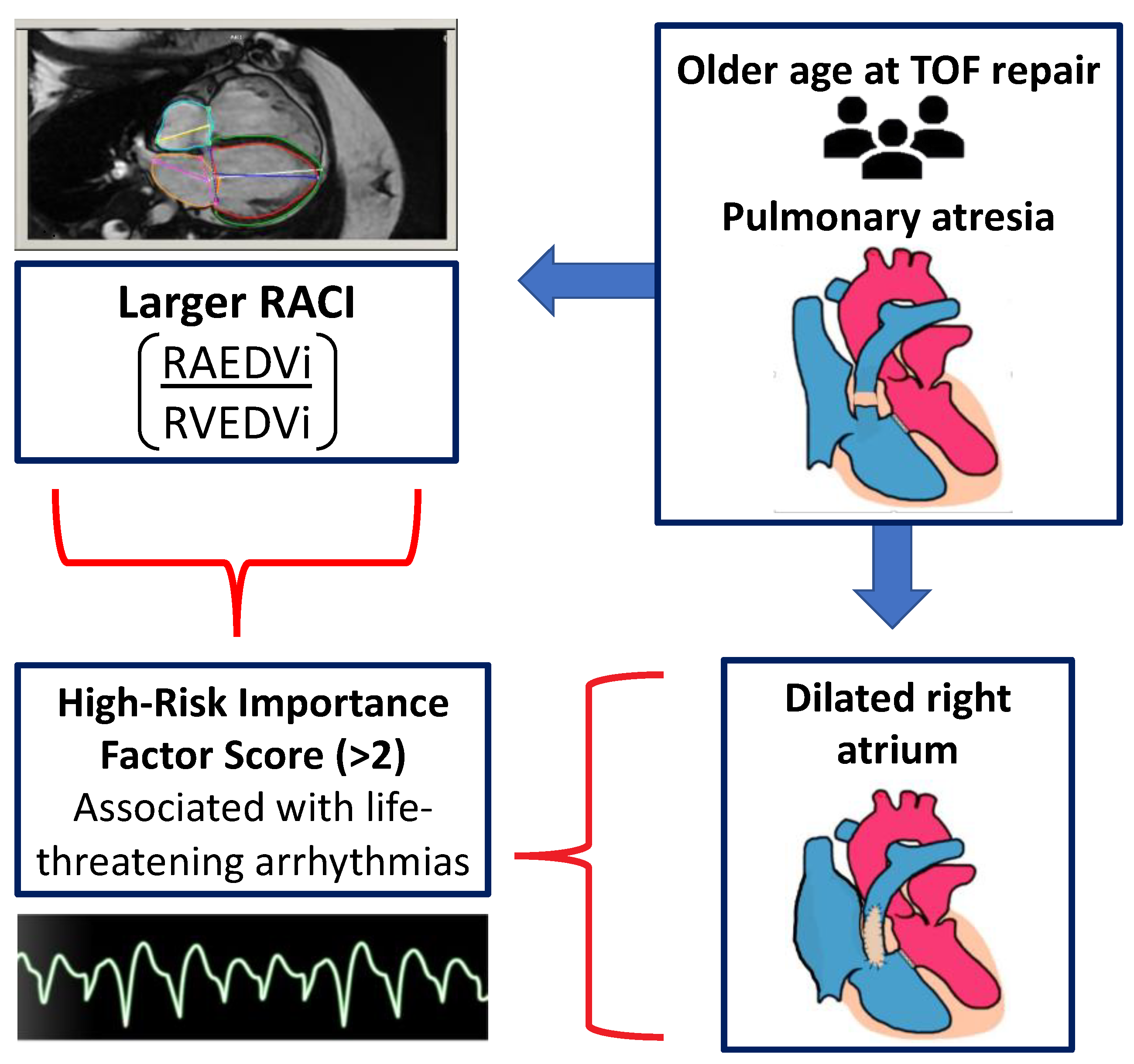
2.5. Right Atrioventricular Coupling Index
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Associations between Atrial CMR Measurements and Patient Characteristics
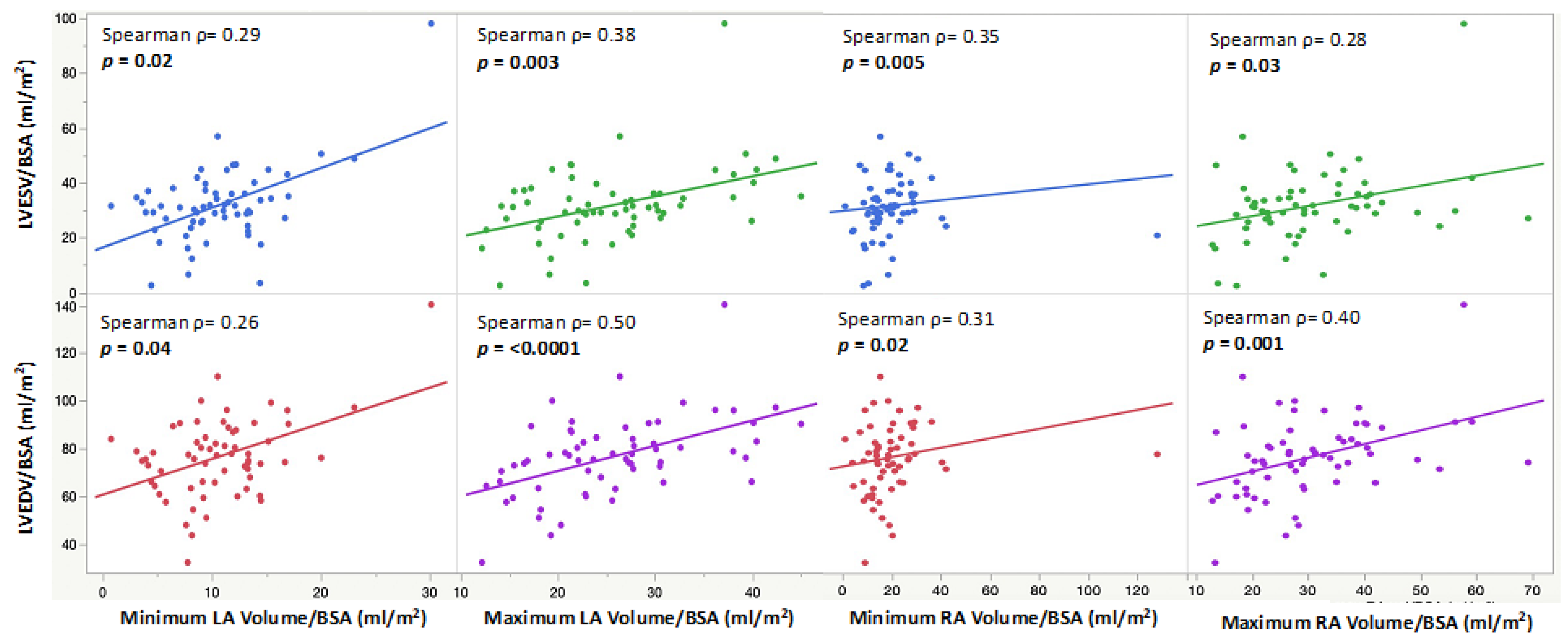
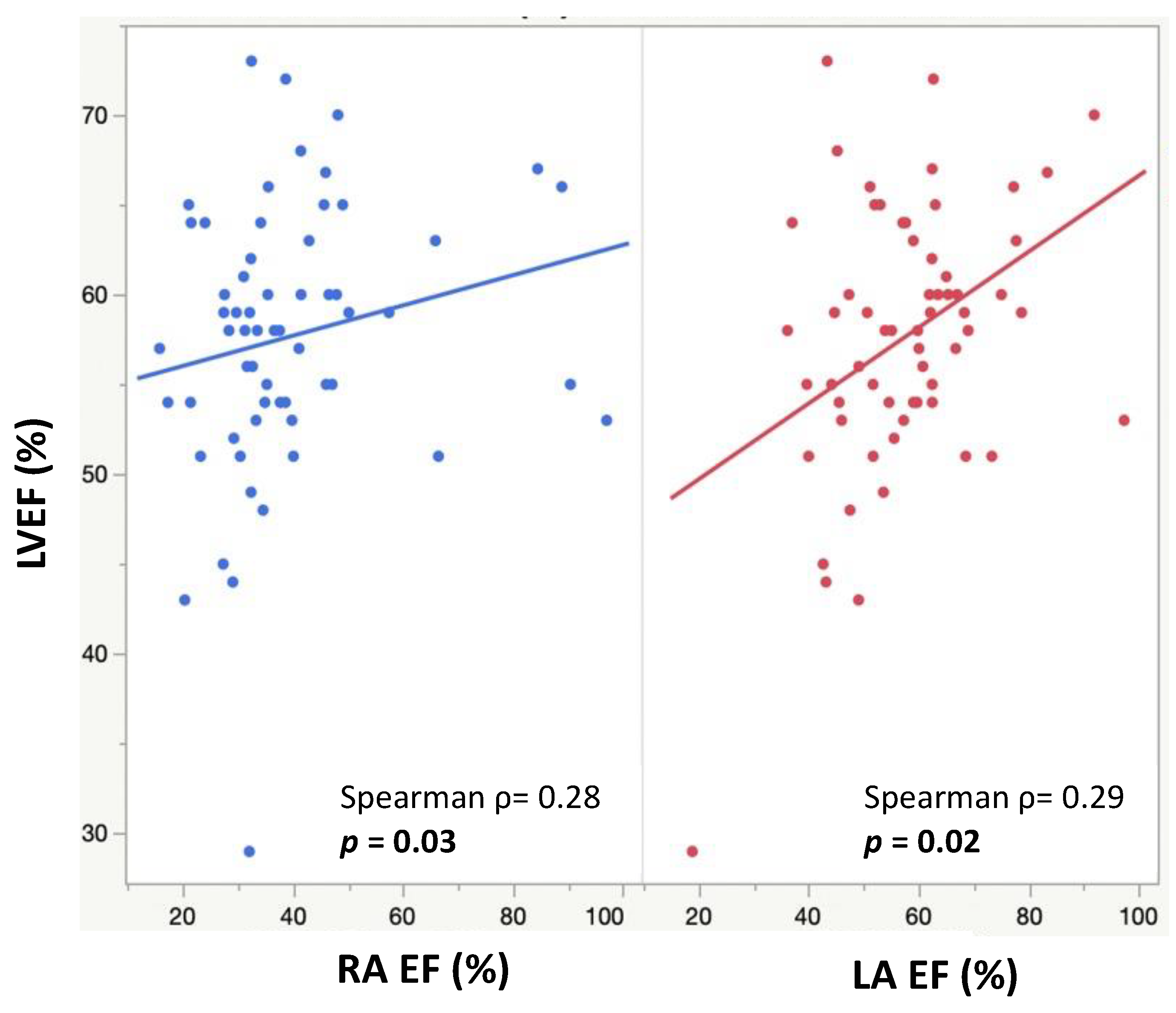
3.3. Associations between Atrial CMR Measurements and Ventricular CMR Parameters
3.4. Risk Scores
3.5. Effects of PVR on Atrial Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nollert, G.; Fischlein, T. Long-term results of total repair of tetralogy of Fallot in adulthood: 35 years follow-up in 104 patients corrected at the age of 18 or older. Thorac. Cardiovasc. Surg. 1997, 45, 178–181. [Google Scholar] [CrossRef]
- Geva, T.; Sandweiss, B.M. Factors associated with impaired clinical status in long-term survivors of tetralogy of Fallot repair evaluated by magnetic resonance imaging. J. Am. Coll Cardiol. 2004, 43, 1068–1074. [Google Scholar] [CrossRef]
- Marelli, A.J.; Ionescu-Ittu, R. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation 2014, 130, 749–756. [Google Scholar] [CrossRef]
- Hickey, E.J.; Veldtman, G. Late risk of outcomes for adults with repaired tetralogy of Fallot from an inception cohort spanning four decades. Eur. J. Cardiothorac. Surg. 2009, 35, 156–164; Discussion 64. [Google Scholar] [CrossRef]
- Geva, T. Indications and timing of pulmonary valve replacement after tetralogy of Fallot repair. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card Surg. Annu. 2006, 9, 11–22. [Google Scholar] [CrossRef]
- Valente, A.M.; Gauvreau, K. Contemporary predictors of death and sustained ventricular tachycardia in patients with repaired tetralogy of Fallot enrolled in the INDICATOR cohort. Heart 2014, 100, 247–253. [Google Scholar] [CrossRef]
- Panesar, D.K.; Burch, M. Assessment of Diastolic Function in Congenital Heart Disease. Front. Cardiovasc. Med. 2017, 4, 5. [Google Scholar] [CrossRef]
- Khairy, P.; Harris, L. Implantable cardioverter-defibrillators in tetralogy of Fallot. Circulation 2008, 117, 363–370. [Google Scholar] [CrossRef]
- Cameli, M.; Lisi, M. Left atrial deformation analysis by speckle tracking echocardiography for prediction of cardiovascular outcomes. Am. J. Cardiol. 2012, 110, 264–269. [Google Scholar] [CrossRef]
- Mawad, W.; Friedberg, M.K. The continuing challenge of evaluating diastolic function by echocardiography in children: Developing concepts and newer modalities. Curr. Opin. Cardiol. 2017, 32, 93–100. [Google Scholar] [CrossRef]
- Atallah, J.; Gonzalez Corcia, M.C. Ventricular Arrhythmia and Life-Threatening Events in Patients With Repaired Tetralogy of Fallot. Am. J. Cardiol. 2020, 132, 126–132. [Google Scholar] [CrossRef]
- Pezel, T.; Ambale Venkatesh, B. Left Atrioventricular Coupling Index to Predict Incident Heart Failure: The Multi-Ethnic Study of Atherosclerosis. Front. Cardiovasc. Med. 2021, 8, 704611. [Google Scholar] [CrossRef]
- Pezel, T.; Venkatesh, B.A. Left Atrioventricular Coupling Index as a Prognostic Marker of Cardiovascular Events: The MESA Study. Hypertension 2021, 78, 661–671. [Google Scholar] [CrossRef]
- Pezel, T.; Ambale-Venkatesh, B. Change in Left Atrioventricular Coupling Index to Predict Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA). Radiology 2022, 303, 317–326. [Google Scholar] [CrossRef]
- Ait Ali, L.; Lurz, P. Implications of atrial volumes in surgical corrected Tetralogy of Fallot on clinical adverse events. Int. J. Cardiol. 2019, 283, 107–111. [Google Scholar] [CrossRef]
- Kawel-Boehm, N.; Hetzel, S.J. Reference ranges (“normal values”) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 87. [Google Scholar] [CrossRef]
- Possner, M.; Tseng, S.Y. Risk Factors for Mortality and Ventricular Tachycardia in Patients With Repaired Tetralogy of Fallot: A Systematic Review and Meta-analysis. Can. J. Cardiol. 2020, 36, 1815–1825. [Google Scholar] [CrossRef]
- Arya, S.; Kovach, J. Arrhythmias and sudden death among older children and young adults following tetralogy of Fallot repair in the current era: Are previously reported risk factors still applicable? Congenit. Heart Dis. 2014, 9, 407–414. [Google Scholar] [CrossRef]
- Riesenkampff, E.; Mengelkamp, L. Integrated analysis of atrioventricular interactions in tetralogy of Fallot. Am. J. Physiol. Heart Circ. Physiol. 2010, 299, H364–H371. [Google Scholar] [CrossRef]
- Abd El Rahman, M.; Raedle-Hurst, T. Assessment of inter-atrial, inter-ventricular, and atrio-ventricular interactions in tetralogy of Fallot patients after surgical correction. Insights from two-dimensional speckle tracking and three-dimensional echocardiography. Cardiol. Young 2015, 25, 1254–1262. [Google Scholar] [CrossRef]
- Abhayaratna, W.P.; Fatema, K. Left atrial reservoir function as a potent marker for first atrial fibrillation or flutter in persons > or = 65 years of age. Am. J. Cardiol. 2008, 101, 1626–1629. [Google Scholar] [CrossRef]
- Wijesekera, V.A.; Raju, R. Sequential Right and Left Ventricular Assessment in Posttetralogy of Fallot Patients with Significant Pulmonary Regurgitation. Congenit. Heart Dis. 2016, 11, 606–614. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Complete TOF Repair (years) | 0.5 (0.4, 1.0) |
| Age at CMR (years) | 16.4 (12.9, 18.7) |
| Sex | |
| Male | 37 (59%) |
| Female | 26 (41%) |
| TOF Diagnosis | |
| Pulmonary Atresia | 16 (25%) |
| Pulmonary Stenosis | 47 (75%) |
| History of BTT Shunt | |
| Yes | 9 (14%) |
| No | 54 (86%) |
| History of Pulmonary Valve Replacement | |
| Yes | 31 (49%) |
| No | 32 (51%) |
| QRS Duration on EKG | 134.0 (108.0, 149.0) |
| CMR Data † | |
| LV End-Diastolic Volume (mL/m2) | 76.2 (66.3, 85.9) |
| LV End-Systolic Volume (mL/m2) | 31.2 (26.0, 36.5) |
| LV Ejection Fraction (%) | 58.0 (54.0, 63.0) |
| RV End-Diastolic Volume (mL/m2) | 119.1 (95.5, 138.3) |
| RV End-Systolic Volume (mL/m2) | 61.3 (49.0, 73.2) |
| RV Ejection Fraction (%) | 49.0 (44.0, 53.0) |
| Pulmonary Regurgitation Fraction (%) | 39.0 (19.0, 51.5) |
| Minimum LA Volume (mL/m2) | 10.4 (8.0, 13.3) |
| Maximum LA Volume (mL/m2) | 24.4 (20.0, 30.2) |
| LA Ejection Fraction (%) | 59.0 (49.1, 64.3) |
| Minimum RA Volume (mL/m2) | 18.5 (12.6, 23.4) |
| Maximum RA Volume (mL/m2) | 27.8 (22.0, 37.4) |
| RA Ejection Fraction (%) | 34.9 (30.7, 45.8) |
| RA Coupling Index (%) | 15.0 (10.5, 22.1) |
| Minimum LA Volume (mL/m2) | Maximum LA Volume (mL/m2) | LA Ejection Fraction (%) | Minimum RA Volume (mL/m2) | Maximum RA Volume (mL/m2) | RA Ejection Fraction (%) | RA Coupling Index (%) | |
|---|---|---|---|---|---|---|---|
| CMR Parameters | |||||||
| LV End-Diastolic Volume (mL/m2) | 0.26, 0.04 ‡ | 0.50, <0.0001 ‡ | 0.18, NS | 0.31, 0.02 ‡ | 0.40, 0.001 ‡ | 0.09, NS | 0.17, NS |
| LV End-Systolic Volume (mL/m2) | 0.29, 0.02 ‡ | 0.38, 0.003 ‡ | 0.01, NS | 0.35, 0.005 ‡ | 0.28, 0.03 ‡ | −0.24, NS | 0.24, NS |
| LV Ejection Fraction (%) | −0.18, NS | 0.03, NS | 0.29, 0.02 ‡ | −0.12, NS | 0.03, NS | 0.28, 0.03 c | 0.04, NS |
| RV End-Diastolic Volume (mL/m2) | 0.00, NS | 0.08, NS | 0.05, NS | −0.06, NS | −0.04, NS | 0.06, NS | |
| RV End-Systolic Volume (mL/m2) | 0.07, NS | 0.05, NS | −0.12, NS | 0.03, NS | −0.01, NS | −0.02, NS | −0.36, 0.004 ‡ |
| RV Ejection Fraction (%) | −0.07, NS | 0.13, NS | 0.30, 0.02‡ | −0.09, NS | 0.06, NS | 0.15, NS | −0.01, NS |
| Pulmonary Regurgitation Fraction (%) | −0.13, NS | −0.16, NS | −0.03, NS | −0.21, NS | −0.24, NS | 0.03, NS | −0.45, 0.0002 ‡ |
| Minimum LA Volume (mL/m2) | 0.62, <0.0001 ‡ | −0.61, <0.0001 ‡ | −0.30, 0.02 ‡ | 0.30, 0.02 ‡ | |||
| Maximum LA Volume (mL/m2) | 0.12, NS | −0.01, NS | 0.37, 0.003 ‡ | ||||
| LA Ejection Fraction (%) | −0.03, NS | ||||||
| Minimum RA Volume (mL/m2) | 0.37, 0.003 ‡ | 0.50, <0.0001 ‡ | −0.01, NS | 0.78, <0.0001 ‡ | −0.46, 0.0002 ‡ | ||
| Maximum RA Volume (mL/m2) | 0.22, NS | 0.57, <0.0001 ‡ | 0.24, NS | 0.03, NS | 0.63, <0.0001 ‡ | ||
| RA Ejection Fraction (%) | 0.38, 0.002 ‡ | −0.42, 0.0007 ‡ | |||||
| Age at Complete TOF repair | 0.23, NS | 0.25, NS | −0.03, NS | 0.17, NS | 0.26, 0.04 ‡ | −0.04, NS | 0.27, 0.03 ‡ |
| Age at CMR | 0.34, 0.006 ‡ | 0.32, 0.01 ‡ | −0.11, NS | 0.36, 0.005 ‡ | 0.38, 0.002 ‡ | 0.01, NS | 0.40, 0.001 ‡ |
| N | LA Ejection Fraction (%) | Minimum RA Volume (mL/m2) | Maximum RA Volume (mL/m2) | RA Ejection Fraction (%) | RA Coupling Index (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (25th %ile, 75th %ile) | p-Value * | Median (25th %ile, 75th %ile) | p-Value * | Median (25th %ile, 75th %ile) | p-Value * | Median (25th %ile, 75th %ile) | p-Value * | Median (25th %ile, 75th %ile) | p-Value * | ||
| TOF Diagnosis | NS | 0.03 * | NS | NS | 0.02 * | ||||||
| Pulmonary Atresia | 16 | 56.8 (45.7, 66.5) | 20.6 (16.3, 29.1) | 31.0 (27.7, 40.9) | 32.2 (25.2, 40.7) | 22.8 (15.1, 27.0) | |||||
| Pulmonary Stenosis | 47 | 59.0 (49.1, 63.5) | 14.76 (12.0, 23.2) | 26.8 (20.4, 42.2) | 35.5 (31.6, 47.1) | 13.2 (9.8, 18.8) | |||||
| History of BTT Shunt | NS | NS | NS | NS | NS | ||||||
| Yes | 9 | 59.7 (50.1, 62.4) | 24.8 (13.0, 32.4) | 37.1 (25.3, 50.6) | 38.6 (26.4, 41.2) | 19.5 (8.9, 28.6) | |||||
| No | 54 | 58.3 (47.7, 65.8) | 16.6 (12.4, 22.7) | 27.6 (20.5, 35.7) | 34.3 (30.8, 46.1) | 14.9 (10.6, 22.1) | |||||
| History of PVR | |||||||||||
| Yes: Pre-CMR | 6 | 56.3 (50.3, 67.1) | NS† | 32.8 (12.2, 41.0) | NS † | 54.9 (29.6, 61.7) | 0.03 *,† | 44.7 (34.2, 53.2) | NS† | 33.2 (12.9, 48.9) | NS † |
| Yes: Post-CMR | 25 | 57.3 (46.6, 62.4) | 0.03 *,‡ | 16.7 (10.8, 20.3) | NS ‡ | 27.5 (19.8, 35.1) | NS ‡ | 35.2 (30.5, 44.4) | NS‡ | 12.1 (7.7, 16.9) | NS ‡ |
| No | 32 | 60.4 (47.9, 71.6) | 17.7 (12.8, 23.3) | 27.7 (20.9, 37.2) | 33.8 (29.5, 44.6) | 17.0 (10.9, 22.8) | |||||
| Importance Factor Score | RV-Independent Score | |||||
|---|---|---|---|---|---|---|
| ≤2 | >2 | p-Value ‡ | ≤2 | >2 | p-Value ‡ | |
| CMR Parameters | ||||||
| Minimum LA Volume (mL/m2) | 10.3 (7.8, 13.1) | 11.2 (7.9, 14.0) | NS | 10.4 (7.8, 13.1) | 10.3 (7.9, 14.4) | NS |
| Maximum LA Volume (mL/m2) | 24.8 (19.2, 30.3) | 24.4 (20.1, 30.3) | NS | 23.8 (19.2, 30.0) | 25.6 (20.1, 30.7) | NS |
| LA Ejection Fraction (%) | 59.5 (51.0, 65.7) | 53.6 (44.9, 62.4) | NS | 59.4 (51.0, 65.1) | 53.6 (46.3, 64.7) | NS |
| Minimum RA Volume (mL/m2) | 16.6 (11.3, 23.2) | 19.8 (14.3, 28.9) | 0.04 ‡ | 15.4 (11.3, 22.7) | 20.6 (14.7, 28.9) | 0.02 ‡ |
| Maximum RA Volume (mL/m2) | 27.2 (19.9, 36.5) | 29.0 (22.8, 40.8) | NS | 26.8 (19.9, 35.7) | 30.8 (24.7, 41.6) | NS |
| RA Ejection Fraction (%) | 35.2 (31.2, 47.3) | 33.3 (28.7, 40.0) | NS | 35.3 (31.2, 47.3) | 33.3 (28.7, 41.2) | NS |
| RA Coupling Index (%) | 13.5 (9.9, 19.6) | 18.6 (11.8, 26.8) | 0.03 ‡ | 13.1 (9.8, 18.9) | 19.5 (13.4, 26.8) | 0.02 ‡ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunsaulus, M.; Bueno, A.; Bright, C.; Snyder, K.; Das, N.; Dobson, C.; DeBrunner, M.; Christopher, A.; Hoskoppal, A.; Follansbee, C.; et al. The Use of Automated Atrial CMR Measures and a Novel Atrioventricular Coupling Index for Predicting Risk in Repaired Tetralogy of Fallot. Children 2023, 10, 400. https://doi.org/10.3390/children10020400
Gunsaulus M, Bueno A, Bright C, Snyder K, Das N, Dobson C, DeBrunner M, Christopher A, Hoskoppal A, Follansbee C, et al. The Use of Automated Atrial CMR Measures and a Novel Atrioventricular Coupling Index for Predicting Risk in Repaired Tetralogy of Fallot. Children. 2023; 10(2):400. https://doi.org/10.3390/children10020400
Chicago/Turabian StyleGunsaulus, Megan, Alejandra Bueno, Carley Bright, Katelyn Snyder, Nikkan Das, Craig Dobson, Mark DeBrunner, Adam Christopher, Arvind Hoskoppal, Christopher Follansbee, and et al. 2023. "The Use of Automated Atrial CMR Measures and a Novel Atrioventricular Coupling Index for Predicting Risk in Repaired Tetralogy of Fallot" Children 10, no. 2: 400. https://doi.org/10.3390/children10020400
APA StyleGunsaulus, M., Bueno, A., Bright, C., Snyder, K., Das, N., Dobson, C., DeBrunner, M., Christopher, A., Hoskoppal, A., Follansbee, C., Arora, G., Olivieri, L., & Alsaied, T. (2023). The Use of Automated Atrial CMR Measures and a Novel Atrioventricular Coupling Index for Predicting Risk in Repaired Tetralogy of Fallot. Children, 10(2), 400. https://doi.org/10.3390/children10020400