
Pediatric Anesthesia Providers’ Perspective on the Real-Life Implementation of the Philips Visual Patient Avatar: A Qualitative Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Approval and Consent
2.2. Study Design
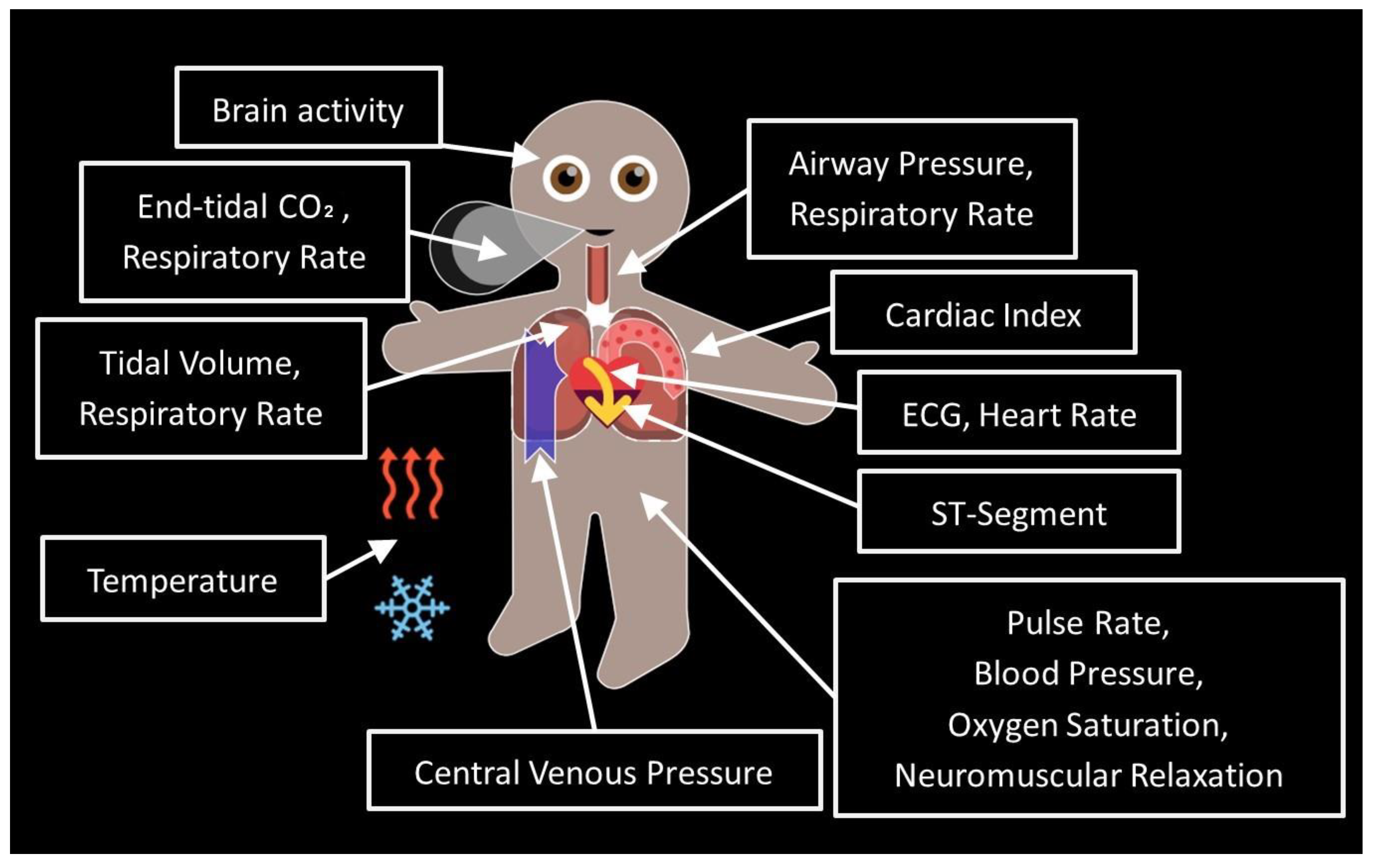
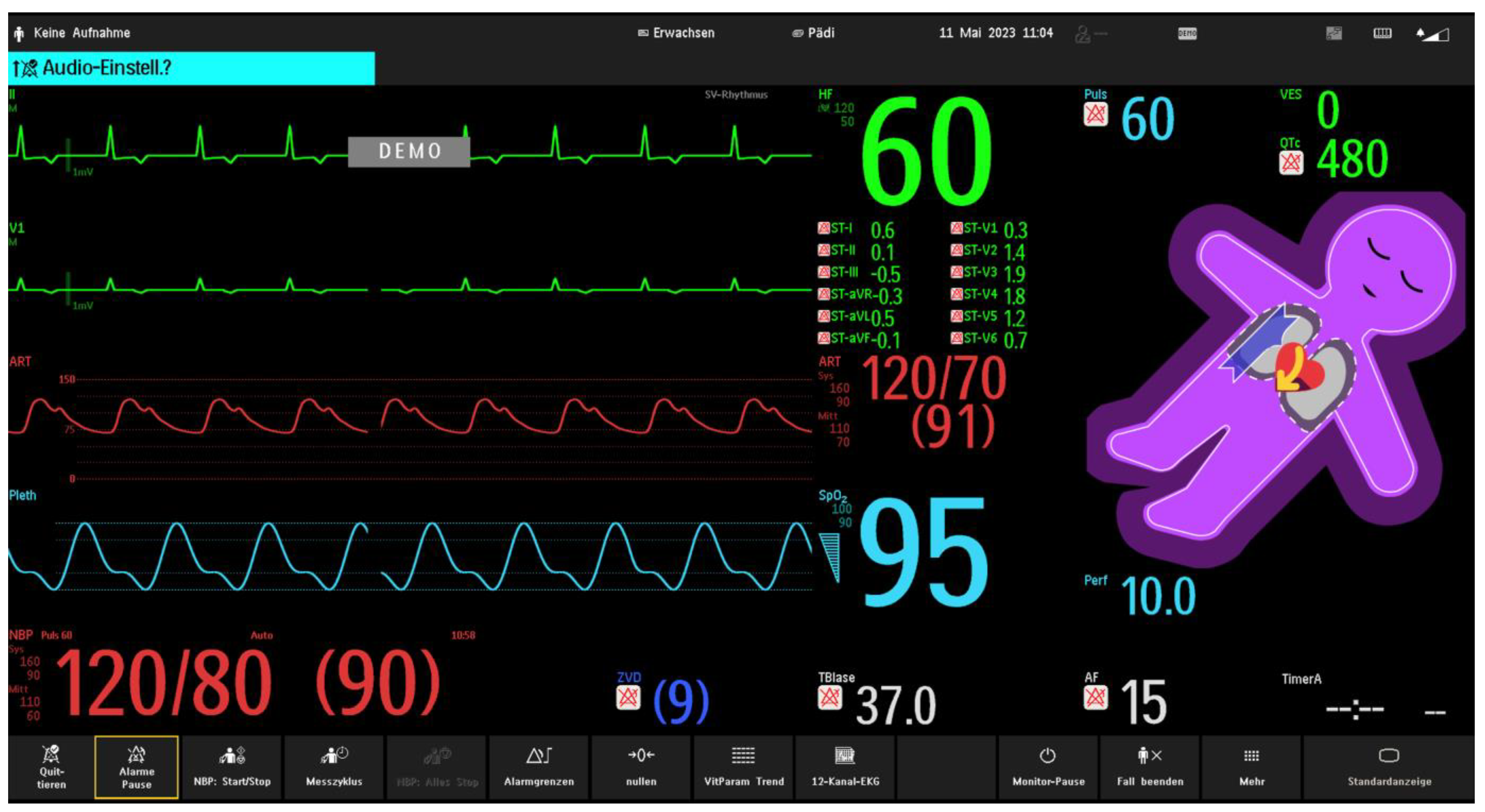
2.3. The Visual Patient Avatar in the Study Center
2.4. Reflexivity
2.5. Data Collection
2.6. Data Analysis
2.6.1. Open-Ended Questions
2.6.2. Demographic Data
3. Results
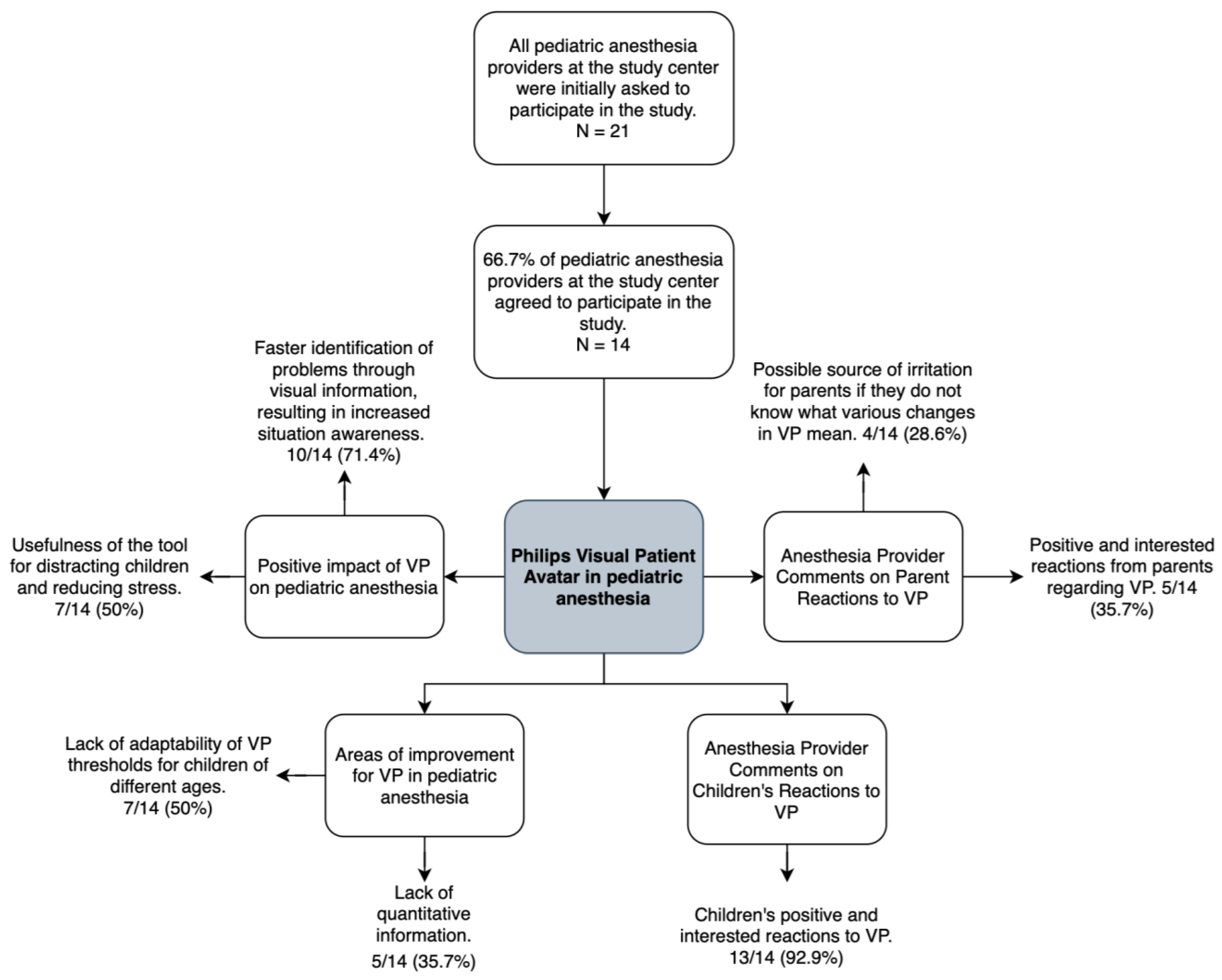
3.1. Participant Characteristics
3.2. The Positive Impact of Visual Patient Avatar on Pediatric Anesthesia from Anesthesia Providers’ Perspective
3.2.1. Faster Identification of Problems through Visual Information, Resulting in Increased Situation Awareness
“Even faster problem recognition, especially when the child’s temperature or oxygen saturation drops.”(Participant 2)
“From the position on the patient’s head, e.g., during anesthesia induction (standing far from the monitor), changes in the vital parameters can be quickly recognized.”(Participant 3)
“Visual Patient Avatar is good for situation awareness, e.g., if a lot of attention is taken up with the distraction of the child at the beginning of the induction, a good picture of the overall situation can be formed by a quick look at the Visual Patient Avatar. The focus is directly drawn to the problem if there is one.”(Participant 9)
3.2.2. Usefulness of the Tool for Distracting Children and Reducing Stress
“Visual Patient Avatar offers the possibility of distracting children during certain procedures.”(Participant 2)
“Visual Patient is a good tool to entertain the child, exciting to look at, and attracts attention through flashing and colors. It is also good for explaining individual monitoring parameters to the child.”(Participant 9)
3.3. Areas for Improvement of Visual Patient Avatar from Anesthesia Providers’ Perspective
3.3.1. Lack of Adaptability of the Visual Patient Avatar Thresholds for Children of Different Age Groups
“There should be more profiles of Visual Patient Avatar for different age groups in pediatric anesthesia because with the standard pediatric profile, the alarms do not always fit with very small children or even older children, and it then alarms wrongly and distracts.”(Participant 9)
“The very high pediatric heart rate is visually distracting in Visual Patient Avatar.”(Participant 3)
3.3.2. Lack of Quantitative Information
“In a critical situation, I would not pay much attention to visualizations. You need numbers for that.”
3.4. Anesthesia Providers’ Comments on Children’s Reactions to Visual Patient Avatar
“Children react very positively to Visual Patient Avatar: curious, find it exciting or even funny.”(Participant 9)
“Children like Visual Patient Avatar: its sympathetic appearance, friendly impression.”(Participant 1)
“Children definitely benefit from Visual Patient Avatar: you can explain the process to them better, and it also has an entertainment value.”(Participant 6)
3.5. Anesthesia Providers’ Comments on Parents’ Reactions to Visual Patient Avatar
“I experience it in Caesarean sections: the patient and the partner react very positively to Visual Patient Avatar; so I imagine that parents in pediatric anesthesia settings would also respond positively.”(Participant 3)
“Parents might be irritated, possibly worried, if everything flashes quickly or Visual Patient Avatar turns purple.”(Participant 9)
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hashimoto, D.A.; Witkowski, E.; Gao, L.; Meireles, O.; Rosman, G. Artificial Intelligence in Anesthesiology: Current Techniques, Clinical Applications, and Limitations. Anesthesiology 2020, 132, 379–394. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Drews, F.A. Patient monitors in critical care: Lessons for improvement. In Advances in Patient Safety: New Directions and Alternative Approaches (Performance and Tools); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008; Volume 3. [Google Scholar]
- Tscholl, D.W.; Rossler, J.; Said, S.; Kaserer, A.; Spahn, D.R.; Nothiger, C.B. Situation Awareness-Oriented Patient Monitoring with Visual Patient Technology: A Qualitative Review of the Primary Research. Sensors 2020, 20, 2112. [Google Scholar] [CrossRef] [PubMed]
- Radziwill, N.M. Designing for Situation Awareness: An Approach to User-Centered Design, 2nd ed.; CRC Press Inc.: Boca Raton, FL, USA, 2011. [Google Scholar]
- Oury, J.D.; Ritter, F.E.; Oury, J.D.; Ritter, F.E. How User-Centered Design Supports Situation Awareness for Complex Interfaces. In Building Better Interfaces for Remote Autonomous Systems: An Introduction for Systems Engineers; Human–Computer Interaction Series, Vanderdonckt, J., Liao, Q.V., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Katz, D. Gestalt psychology: Its nature and significance. Psychol. Bull. 1950, 48, 177–180. [Google Scholar]
- Wagemans, J.; Elder, J.H.; Kubovy, M.; Palmer, S.E.; Peterson, M.A.; Singh, M.; von der Heydt, R. A century of Gestalt psychology in visual perception: I. Perceptual grouping and figure–ground organization. Psychol. Bull. 2012, 138, 1172. [Google Scholar] [CrossRef] [PubMed]
- Croskerry, P. Clinical cognition and diagnostic error: Applications of a dual process model of reasoning. Adv. Health Sci. Educ. 2009, 14, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D. Thinking, Fast and Slow; Macmillan: New York, NY, USA, 2011. [Google Scholar]
- Roche, T.R.; Said, S.; Braun, J.; Maas, E.J.C.; Machado, C.; Grande, B.; Kolbe, M.; Spahn, D.R.; Nothiger, C.B.; Tscholl, D.W. Avatar-based patient monitoring in critical anaesthesia events: A randomised high-fidelity simulation study. Br. J. Anaesth. 2021, 126, 1046–1054. [Google Scholar] [CrossRef]
- Reader, T.W.; Flin, R.; Mearns, K.; Cuthbertson, B.H. Team situation awareness and the anticipation of patient progress during ICU rounds. BMJ Qual. Saf. 2011, 20, 1035–1042. [Google Scholar] [CrossRef]
- Schulz, C.M.; Endsley, M.R.; Kochs, E.F.; Gelb, A.W.; Wagner, K.J. Situation awareness in anesthesia: Concept and research. Anesthesiology 2013, 118, 729–742. [Google Scholar] [CrossRef]
- Schulz, C.M.; Burden, A.; Posner, K.L.; Mincer, S.L.; Steadman, R.; Wagner, K.J.; Domino, K.B. Frequency and Type of Situational Awareness Errors Contributing to Death and Brain Damage: A Closed Claims Analysis. Anesthesiology 2017, 127, 326–337. [Google Scholar] [CrossRef]
- Schulz, C.M.; Krautheim, V.; Hackemann, A.; Kreuzer, M.; Kochs, E.F.; Wagner, K.J. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2016, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Bergauer, L.; Braun, J.; Roche, T.R.; Meybohm, P.; Hottenrott, S.; Zacharowski, K.; Raimann, F.J.; Rivas, E.; López-Baamonde, M.; Ganter, M.T.; et al. Avatar-based patient monitoring for intensive care units improves information transfer, diagnostic confidence and decreases perceived workload—A computer-based, multicentre comparison study. Sci. Rep. 2023, 13, 5908. [Google Scholar] [CrossRef] [PubMed]
- Mindray. Products. Available online: https://www.mindray.com/uk/products (accessed on 16 November 2023).
- Kheterpal, S.; Shanks, A.; Tremper, K.K. Impact of a Novel Multiparameter Decision Support System on Intraoperative Processes of Care and Postoperative Outcomes. Anesthesiology 2018, 128, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Sathishkumar, S.; Lai, M.; Picton, P.; Kheterpal, S.; Morris, M.; Shanks, A.; Ramachandran, S.K. Behavioral Modification of Intraoperative Hyperglycemia Management with a Novel Real-time Audiovisual Monitor. Anesthesiology 2015, 123, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Drews, F.A.; Westenskow, D.R. The right picture is worth a thousand numbers: Data displays in anesthesia. Hum. Factors 2006, 48, 59–71. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Weiss, M.; Handschin, L.; Spahn, D.R.; Nothiger, C.B. User perceptions of avatar-based patient monitoring: A mixed qualitative and quantitative study. BMC Anesthesiol. 2018, 18, 188. [Google Scholar] [CrossRef] [PubMed]
- Sowb, Y.A.; Loeb, R.G. Cognitive analysis of intraoperative critical events: A problem-driven approach to aiding clinician’s performance. J. Cogn. Technol. Work. 2002, 4, 109–119. [Google Scholar] [CrossRef]
- Sowb, Y.A.; Loeb, R.G.; Roth, E.M. Cognitive modeling of intraoperative critical events. In Proceedings of the IEEE Meeting on Systems, Man, and Cybernetics, San Diego, CA, USA, 11–14 October 1998; pp. 2533–2538. [Google Scholar]
- Patel, V.L.; Arocha, J.F.; Kaufman, D.R. Medical cognition. In Handbook of Applied Cognition; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 1999. [Google Scholar]
- Cooke, N.J. Knowledge elicitation. In Handbook of Applied Cognition; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 1999. [Google Scholar]
- Olmos-Vega, F.M.; Stalmeijer, R.E.; Varpio, L.; Kahlke, R. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med. Teach. 2022, 7, 1–11. [Google Scholar] [CrossRef]
- Hendra, R.; Hill, A. Rethinking Response Rates: New Evidence of Little Relationship between Survey Response Rates and Nonresponse Bias. Eval. Rev. 2018, 43, 307–330. [Google Scholar] [CrossRef]
- Elston, D.M. Participation bias, self-selection bias, and response bias. J. Am. Acad. Dermatol. 2021. ahead of print. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Virginia, B.; Victoria, C. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar]
- Fortier, M.A.; Del Rosario, A.M.; Martin, S.R.; Kain, Z.N. Perioperative anxiety in children. Pediatr. Anesth. 2010, 20, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Kain, Z.N.; Mayes, L.C.; Caldwell-Andrews, A.A.; Karas, D.E.; McClain, B.C. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics 2006, 118, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Wright, K.D.; Stewart, S.H.; Finley, G.A.; Buffett-Jerrott, S.E. Prevention and intervention strategies to alleviate preoperative anxiety in children: A critical review. Behav. Modif. 2007, 31, 52–79. [Google Scholar] [CrossRef]
- Kain, Z.N.; Mayes, L.C.; O’Connor, T.Z.; Cicchetti, D.V. Preoperative anxiety in children. Predictors and outcomes. Arch. Pediatr. Adolesc. Med. 1996, 150, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Schneuer, F.J.; Bentley, J.P.; Davidson, A.J.; Holland, A.J.; Badawi, N.; Martin, A.J.; Skowno, J.; Lain, S.J.; Nassar, N. The impact of general anesthesia on child development and school performance: A population-based study. Pediatr. Anesth. 2018, 28, 528–536. [Google Scholar] [CrossRef]
- O’Leary, J.D.; Janus, M.; Duku, E.; Wijeysundera, D.N.; To, T.; Li, P.; Maynes, J.T.; Faraoni, D.; Crawford, M.W. Influence of Surgical Procedures and General Anesthesia on Child Development Before Primary School Entry among Matched Sibling Pairs. JAMA Pediatr. 2019, 173, 29–36. [Google Scholar] [CrossRef]
- McCann, M.E.; Soriano, S.G. Does general anesthesia affect neurodevelopment in infants and children? BMJ 2019, 367, l6459. [Google Scholar] [CrossRef]
- Grabowski, J.; Goldin, A.; Arthur, L.G.; Beres, A.L.; Guner, Y.S.; Hu, Y.Y.; Kawaguchi, A.L.; Kelley-Quon, L.I.; McAteer, J.P.; Miniati, D.; et al. The effects of early anesthesia on neurodevelopment: A systematic review. J. Pediatr. Surg. 2021, 56, 851–861. [Google Scholar] [CrossRef]
- Atieno, O.P. An analysis of the strengths and limitation of qualitative and quantitative research paradigms. Probl. Educ. 21st Century 2009, 13, 13–38. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Participants (n = 14) | |
|---|---|
| Sex | |
| Female | 5 (35.7%) |
| Male | 9 (64.3%) |
| Participant age in years, median (IQR) | 42 (38–45) |
| Anesthesia experience in years, median (IQR) | 11 (6–14) |
| Role | |
| Certified nurse anesthetist | 4 (28.6%) |
| Resident 1–2 years of training (limits: 1 year to 2 years) | 1 (7.1%) |
| Resident 3–5 years of training (limits: 3 to 5 years) | 1 (7.1%) |
| Resident with >5 years of experience (limits: 6 years to end of residency) | 3 (21.4%) |
| Staff anesthesiologist | 5 (35.7%) |
| Educational material consulted | |
| Quick guide only | 4 (28.6%) |
| Tutorial video only | 0 |
| Both | 3 (21.4%) |
| None | 7 (50.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lunkiewicz, J.; Fries, D.; Milovanovic, P.; Noethiger, C.B.; Tscholl, D.W.; Gasciauskaite, G. Pediatric Anesthesia Providers’ Perspective on the Real-Life Implementation of the Philips Visual Patient Avatar: A Qualitative Study. Children 2023, 10, 1841. https://doi.org/10.3390/children10121841
Lunkiewicz J, Fries D, Milovanovic P, Noethiger CB, Tscholl DW, Gasciauskaite G. Pediatric Anesthesia Providers’ Perspective on the Real-Life Implementation of the Philips Visual Patient Avatar: A Qualitative Study. Children. 2023; 10(12):1841. https://doi.org/10.3390/children10121841
Chicago/Turabian StyleLunkiewicz, Justyna, Daniel Fries, Petar Milovanovic, Christoph B. Noethiger, David W. Tscholl, and Greta Gasciauskaite. 2023. "Pediatric Anesthesia Providers’ Perspective on the Real-Life Implementation of the Philips Visual Patient Avatar: A Qualitative Study" Children 10, no. 12: 1841. https://doi.org/10.3390/children10121841
APA StyleLunkiewicz, J., Fries, D., Milovanovic, P., Noethiger, C. B., Tscholl, D. W., & Gasciauskaite, G. (2023). Pediatric Anesthesia Providers’ Perspective on the Real-Life Implementation of the Philips Visual Patient Avatar: A Qualitative Study. Children, 10(12), 1841. https://doi.org/10.3390/children10121841