
Risk Behaviors among Migrant Adolescents in Italy

 , , ,
, , ,  ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
- Current smoking. Smoking habit was assessed by asking participants how many days they had smoked cigarettes in the past 30 days. Responses ranged from 0 to every day. Under HBSC protocol, if the answer was at least one day, participants were considered current smokers [1].
- Current weekly drinking. Students were asked how many days they had drunk in the last 30 days. Responses ranged from “Never” to “Every day” and were dichotomized into “at least weekly” (i.e., weekly or daily) vs. “monthly, rarely or never” [1].
- Drunkenness. Adolescents responded to the question, “Have you ever had so much alcohol that you were really drunk?” The response options were “No, never” (1), “Yes, once” (2), “Yes, 2–3 times’’ (3), “Yes, 4–10 times” (4), and “Yes, more than 10 times” (5). Students were considered having this risk behavior if they reported getting drunk at least twice in their lifetime [1].
- Binge drinking. This risky behavior has been investigated in the Italian national HBSC survey since 2010. The binge drinking category asks students to indicate whether they had drunk five or more glasses of alcohol on a single occasion in the past 12 months. Responses were dichotomized into “Yes, at least once” (i.e., binge drunk once or more times) and “No, never” [46].
- Cannabis use. Participants were asked if they had ever taken cannabis in their lifetime, with response options ranging from “Never” to “30 days or more”. Adolescents were considered cannabis users when they answered that they had taken cannabis for at least 3 days in their lifetime [1].
- Multiple substance use. Students reporting two or more among current cigarette smoking, alcohol consumption, and cannabis consumption were considered multiple substance users [47].
- At-risk or problem gambling. The 12-item South Oaks Gambling Screen-Revised for Adolescents (SOGS-RA), which is the most used screening tool for assessing problem gambling in adolescents, was administered. The scoring was: 0–1, “No problem gambling”; 2–3, “At-risk gambling”; and 4 or more, “Problem gambling”. Those categories were then dichotomized into “At risk-problematic gambling” and “No problem gambling”, as in literature, at-risk and problem gamblers seem to exhibit similar characteristics [22,48,49,50,51].
- Gender. Participants were asked to indicate whether they were a boy or a girl.
- Generation of migration. Adolescents were classified as “natives” if both parents were born in Italy, otherwise, they were considered migrants. Specifically, they were classified as “first-generation immigrants” if they were born abroad and at least one parent was born abroad, or as “second-generation immigrants” if they were born in Italy and at least one parent was born abroad [52].
- Area of origin. Based on the country of birth of the mother (or, if missing or born in Italy, on the country of birth of the father), the ethnic background was categorized into three different areas: “Western Countries”, “Eastern European Countries”, and “non-Western/non-European Countries” [52,53].
- “Western Countries”: European Union (EU)—14 countries (member states prior to May 2004), and United Kingdom, Switzerland, Norway and Iceland. It also includes United States, Canada, Australia, and New Zealand, all classified by the International Monetary Fund as advanced economies countries [54];
- “Eastern European countries”: EU—13 countries (new member states joining the EU after May 2004), plus Albania, Bosnia, Macedonia, Moldavia, Serbia, and Ukraine [54];
- “Non-Western/non-European countries”: countries in Africa, South or Central America, and Asia. As immigrant youth from non-Western/non-European countries showed numerous similarities with the other migrants’ area groups, they were combined into a single group.
- Peer substance use-related variables. The HBSC questionnaire asked for the number of friends who smoke, drink alcohol, or take cannabis. For each of the three substances, a variable was created categorizing the number of friends using those substances into three levels: none/a few, some, many/all [1].
- Support-related variables. Referring to the 2017/18 HBSC Research Protocol [1], family and social support items were used to create the following variables: high family support, high friends support, high teachers support, and high classmates support”.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Inchley, J.; Currie, C.; Cosma, A.; Samdal, O. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2017/18 Survey; CAHRU: St Andrews, UK, 2018. [Google Scholar]
- Inchley, J.; Currie, D.; Budisavljevic, S.; Torbjørn, T.; Jåstad, A.; Cosma, A.; Kelly, C.; Arnarsson, Á.; Samdal, O. Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada; International Report. Key Data; Regional Office for Europe, World Health Organization: Geneva, Switzerland, 2020; Volume 2, ISBN 978-92-890-5501-7. [Google Scholar]
- Inchley, J.; Currie, D.; Vieno, A.; Torsheim, T.; Ferreira-Borges, C.; Weber, M.M.; Barnekow, V.; Breda, J. Adolescent Alcohol-Related Behaviours: Trends and Inequalities in the WHO European Region, 2002–2014: Observations from the Health Behaviour in School-Aged Children (HBSC) WHO Collaborative Cross-National Study; Regional Office for Europe, World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-890-5349-5.
- Marshall, E.J. Adolescent Alcohol Use: Risks and Consequences. Alcohol. Alcohol. 2014, 49, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Dick, B.; Ferguson, B.J. Health for the World’s Adolescents: A Second Chance in the Second Decade. J. Adolesc. Health 2015, 56, 3–6. [Google Scholar] [CrossRef] [PubMed]
- van Dorp, M.; Boon, A.; Spijkerman, R.; Los, L. Substance Use Prevalence Rates among Migrant and Native Adolescents in Europe: A Systematic Review. Drug Alcohol. Rev. 2021, 40, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Molinaro, S.; Canale, N.; Vieno, A.; Lenzi, M.; Siciliano, V.; Gori, M.; Santinello, M. Country- and Individual-Level Determinants of Probable Problematic Gambling in Adolescence: A Multi-Level Cross-National Comparison. Addiction 2014, 109, 2089–2097. [Google Scholar] [CrossRef]
- Walsh, S.D.; Sela, T.; De Looze, M.; Craig, W.; Cosma, A.; Harel-Fisch, Y.; Boniel-Nissim, M.; Malinowska-Cieślik, M.; Vieno, A.; Molcho, M.; et al. Clusters of Contemporary Risk and Their Relationship to Mental Well-Being Among 15-Year-Old Adolescents Across 37 Countries. J. Adolesc. Health 2020, 66, S40–S49. [Google Scholar] [CrossRef]
- DuRant, R.H.; Smith, J.A.; Kreiter, S.R.; Krowchuk, D.P. The Relationship between Early Age of Onset of Initial Substance Use and Engaging in Multiple Health Risk Behaviors among Young Adolescents. Arch. Pediatr. Adolesc. Med. 1999, 153, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Busch, V.; Van Stel, H.F.; Schrijvers, A.J.P.; de Leeuw, J.R.J. Clustering of Health-Related Behaviors, Health Outcomes and Demographics in Dutch Adolescents: A Cross-Sectional Study. BMC Public Health 2013, 13, 1118. [Google Scholar] [CrossRef]
- Dumith, S.C.; Muniz, L.C.; Tassitano, R.M.; Hallal, P.C.; Menezes, A.M.B. Clustering of Risk Factors for Chronic Diseases among Adolescents from Southern Brazil. Prev. Med. 2012, 54, 393–396. [Google Scholar] [CrossRef]
- Poulin, C.; Graham, L. The Association between Substance Use, Unplanned Sexual Intercourse and Other Sexual Behaviours among Adolescent Students. Addiction 2001, 96, 607–621. [Google Scholar] [CrossRef]
- Assanangkornchai, S.; Li, J.; McNeil, E.; Saingam, D. Clusters of Alcohol and Drug Use and Other Health-Risk Behaviors among Thai Secondary School Students: A Latent Class Analysis. BMC Public Health 2018, 18, 1272. [Google Scholar] [CrossRef]
- Molinaro, S.; Benedetti, E.; Scalese, M.; Bastiani, L.; Fortunato, L.; Cerrai, S.; Canale, N.; Chomynova, P.; Elekes, Z.; Feijão, F.; et al. Prevalence of Youth Gambling and Potential Influence of Substance Use and Other Risk Factors throughout 33 European Countries: First Results from the 2015 ESPAD Study. Addiction 2018, 113, 1862–1873. [Google Scholar] [CrossRef]
- Charrier, L.; Berchialla, P.; Dalmasso, P.; Borraccino, A.; Lemma, P.; Cavallo, F. Cigarette Smoking and Multiple Health Risk Behaviors: A Latent Class Regression Model to Identify a Profile of Young Adolescents. Risk Anal. 2019, 39, 1771–1782. [Google Scholar] [CrossRef]
- Calado, F.; Alexandre, J.; Griffiths, M.D. Prevalence of Adolescent Problem Gambling: A Systematic Review of Recent Research. J. Gambl. Stud. 2017, 33, 397–424. [Google Scholar] [CrossRef]
- Bastiani, L.; Gori, M.; Colasante, E.; Siciliano, V.; Capitanucci, D.; Jarre, P.; Molinaro, S. Complex Factors and Behaviors in the Gambling Population of Italy. J. Gambl. Stud. 2013, 29, 1–13. [Google Scholar] [CrossRef]
- Buja, A.; Lion, C.; Scioni, M.; Vian, P.; Genetti, B.; Vittadello, F.; Sperotto, M.; Simeoni, E.; Baldo, V. SOGS-RA Gambling Scores and Substance Use in Adolescents. J. Behav. Addict. 2017, 6, 425–433. [Google Scholar] [CrossRef] [PubMed]
- McPherson, K.E.; Kerr, S.; Morgan, A.; McGee, E.; Cheater, F.M.; McLean, J.; Egan, J. The Association between Family and Community Social Capital and Health Risk Behaviours in Young People: An Integrative Review. BMC Public Health 2013, 13, 971. [Google Scholar] [CrossRef] [PubMed]
- Velleman, R.D.B.; Templeton, L.J.; Copello, A.G. The Role of the Family in Preventing and Intervening with Substance Use and Misuse: A Comprehensive Review of Family Interventions, with a Focus on Young People. Drug Alcohol. Rev. 2005, 24, 93–109. [Google Scholar] [CrossRef]
- Constante, K.; Huntley, E.D.; Si, Y.; Schillinger, E.; Wagner, C.; Keating, D.P. Conceptualizing Protective Family Context and Its Effect on Substance Use: Comparisons across Diverse Ethnic-Racial Youth. Subst. Abus. 2021, 42, 796–805. [Google Scholar] [CrossRef]
- Canale, N.; Vieno, A.; Griffiths, M.D.; Borraccino, A.; Lazzeri, G.; Charrier, L.; Lemma, P.; Dalmasso, P.; Santinello, M. A Large-Scale National Study of Gambling Severity among Immigrant and Non-Immigrant Adolescents: The Role of the Family. Addict. Behav. 2017, 66, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Brechwald, W.A.; Prinstein, M.J. Beyond Homophily: A Decade of Advances in Understanding Peer Influence Processes. J. Res. Adolesc. 2011, 21, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Choy, B.; Arunachalam, K.; Gupta, S.; Taylor, M.; Lee, A. Systematic Review: Acculturation Strategies and Their Impact on the Mental Health of Migrant Populations. Public Health Pract. 2021, 2, 100069. [Google Scholar] [CrossRef] [PubMed]
- Sirin, S.R.; Choi, E.; Sin, E.J. Meta-Analysis on the Relation Between Acculturation and Alcohol Use Among Immigrant Youth. J. Adolesc. Health 2022, 70, 361–377. [Google Scholar] [CrossRef] [PubMed]
- McCabe, B.E.; Stenzel, H.; Li, Q.; Cervantes, R.C.; Gonzalez-Guarda, R.M. Multidimensional Acculturation, Acculturative Stress and Alcohol or Drug Use of Adult Latinx Immigrants. J. Psychoact. Drugs 2021, 53, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Kulis, S.; Marsiglia, F.F.; Nieri, T. Perceived Ethnic Discrimination versus Acculturation Stress: Influences on Substance Use among Latino Youth in the Southwest. J. Health Soc. Behav. 2009, 50, 443–459. [Google Scholar] [CrossRef]
- Okamoto, J.; Ritt-Olson, A.; Soto, D.; Baezconde-Garbanati, L.; Unger, J.B. Perceived Discrimination and Substance Use among Latino Adolescents. Am. J. Health Behav. 2009, 33, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.B.; Schwartz, S.J.; Huh, J.; Soto, D.W.; Baezconde-Garbanati, L. Acculturation and Perceived Discrimination: Predictors of Substance Use Trajectories from Adolescence to Emerging Adulthood among Hispanics. Addict. Behav. 2014, 39, 1293–1296. [Google Scholar] [CrossRef] [PubMed]
- Donati, M.A.; Primi, C.; Mazzarese, M.; Sanson, F.; Leone, L. Immigrant Status and Problem-Gambling Severity in Adolescents: Evidence for Moderation by Sensation Seeking. Addict. Behav. 2020, 107, 106395. [Google Scholar] [CrossRef] [PubMed]
- Ellenbogen, S.; Gupta, R.; Derevensky, J.L. A Cross-Cultural Study of Gambling Behaviour among Adolescents. J. Gambl. Stud. 2007, 23, 25–39. [Google Scholar] [CrossRef]
- Salas-Wright, C.P.; Vaughn, M.G.; Schwartz, S.J.; Córdova, D. An “Immigrant Paradox” for Adolescent Externalizing Behavior? Evidence from a National Sample. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 27–37. [Google Scholar] [CrossRef]
- Chun, H.; Mobley, M. The “Immigrant Paradox” Phenomenon: Assessing Problem Behaviors and Risk Factors among Immigrant and Native Adolescents. J. Prim. Prev. 2014, 35, 339–356. [Google Scholar] [CrossRef]
- Tilley, J.L.; Huey, S.J.; Farver, J.M.; Lai, M.H.C.; Wang, C.X. The Immigrant Paradox in the Problem Behaviors of Youth in the United States: A Meta-Analysis. Child. Dev. 2021, 92, 502–516. [Google Scholar] [CrossRef] [PubMed]
- Bui, H.N. Racial and Ethnic Differences in the Immigrant Paradox in Substance Use. J. Immigr. Minor. Health 2013, 15, 866–881. [Google Scholar] [CrossRef]
- Hamilton, H.A.; Noh, S.; Adlaf, E.M. Adolescent Risk Behaviours and Psychological Distress across Immigrant Generations. Can. J. Public Health 2009, 100, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Bacio, G.A.; Mays, V.M.; Lau, A.S. Drinking Initiation and Problematic Drinking among Latino Adolescents: Explanations of the Immigrant Paradox. Psychol. Addict. Behav. 2013, 27, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Westphal, J.R.; Rush, J.A.; Stevens, L.; Johnson, L.J. Gambling Behavior of Louisiana Students in Grades 6 through 12. Psychiatr. Serv. 2000, 51, 96–99. [Google Scholar] [CrossRef]
- Delfabbro, P.; Lahn, J.; Grabosky, P. Further Evidence Concerning the Prevalence of Adolescent Gambling and Problem Gambling in Australia: A Study of the ACT. Int. Gambl. Stud. 2005, 5, 209–228. [Google Scholar] [CrossRef]
- Italian Ministry of Education, University and Research. Gli Alunni Con Cittadinanza Non Italiana A.S. 2017/2018. July 2019. Available online: https://www.miur.gov.it/documents/20182/250189/Notiziario+Stranieri+1718.pdf/78ab53c4-dd30-0c0f-7f40-bf22bbcedfa6?version%3D1.2%26t%3D1562937526726 (accessed on 27 October 2023).
- McHugh, R.K.; Votaw, V.R.; Sugarman, D.E.; Greenfield, S.F. Sex and Gender Differences in Substance Use Disorders. Clin. Psychol. Rev. 2018, 66, 12–23. [Google Scholar] [CrossRef]
- Kuhn, C. Emergence of Sex Differences in the Development of Substance Use and Abuse during Adolescence. Pharmacol. Ther. 2015, 153, 55–78. [Google Scholar] [CrossRef] [PubMed]
- Buja, A.; Sperotto, M.; Genetti, B.; Vian, P.; Vittadello, F.; Simeoni, E.; Zampieri, C.; Baldo, V. Adolescent Gambling Behavior: A Gender Oriented Prevention Strategy Is Required? Ital. J. Pediatr. 2022, 48, 113. [Google Scholar] [CrossRef]
- Claesdotter-Knutsson, E.; André, F.; Fridh, M.; Delfin, C.; Håkansson, A.; Lindström, M. Gender Differences and Associated Factors Influencing Problem Gambling in Adolescents in Sweden: Cross-Sectional Investigation. JMIR Pediatr. Parent. 2022, 5, e35207. [Google Scholar] [CrossRef]
- Lazzeri, G.; Vieno, A.; Charrier, L.; Spinelli, A.; Ciardullo, S.; Pierannunzio, D.; Galeone, D.; Nardone, P. The Methodology of the Italian Health Behaviour in School-Aged Children (HBSC) 2018 Study and Its Development for the next Round. J. Prev. Med. Hyg. 2021, 62, E926–E933. [Google Scholar] [CrossRef]
- Wechsler, H.; Isaac, N. “Binge” Drinkers at Massachusetts Colleges. Prevalence, Drinking Style, Time Trends, and Associated Problems. JAMA 1992, 267, 2929–2931. [Google Scholar] [CrossRef]
- Költő, A.; Cosma, A.; Young, H.; Moreau, N.; Pavlova, D.; Tesler, R.; Thorsteinsson, E.B.; Vieno, A.; Saewyc, E.M.; Nic Gabhainn, S. Romantic Attraction and Substance Use in 15-Year-Old Adolescents from Eight European Countries. Int. J. Environ. Res. Public Health 2019, 16, 3063. [Google Scholar] [CrossRef]
- Winters, K.C.; Stinchfield, R.D.; Kim, L.G. Monitoring Adolescent Gambling in Minnesota. J. Gambl. Stud. 1995, 11, 165–183. [Google Scholar] [CrossRef] [PubMed]
- Blinn-Pike, L.; Worthy, S.L.; Jonkman, J.N. Adolescent Gambling: A Review of an Emerging Field of Research. J. Adolesc. Health 2010, 47, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Chiesi, F.; Donati, M.A.; Galli, S.; Primi, C. The Suitability of the South Oaks Gambling Screen–Revised for Adolescents (SOGS-RA) as a Screening Tool: IRT-Based Evidence. Psychol. Addict. Behav. 2013, 27, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Edgren, R.; Castrén, S.; Jokela, M.; Salonen, A.H. At-Risk and Problem Gambling among Finnish Youth: The Examination of Risky Alcohol Consumption, Tobacco Smoking, Mental Health and Loneliness as Gender-Specific Correlates. Nord. Stud. Alcohol. Drugs 2016, 33, 61–80. [Google Scholar] [CrossRef]
- Borraccino, A.; Charrier, L.; Berchialla, P.; Lazzeri, G.; Vieno, A.; Dalmasso, P.; Lemma, P. Perceived Well-Being in Adolescent Immigrants: It Matters Where They Come From. Int. J. Public Health 2018, 63, 1037–1045. [Google Scholar] [CrossRef]
- Dalmasso, P.; Borraccino, A.; Lazzeri, G.; Charrier, L.; Berchialla, P.; Cavallo, F.; Lemma, P. Being a Young Migrant in Italy: The Effect of Perceived Social Support in Adolescence. J. Immigr. Minor. Health 2018, 20, 1044–1052. [Google Scholar] [CrossRef]
- Eurostat Glossary: EU Enlargements. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:EU_enlargements (accessed on 27 October 2023).
- Lehtonen, R.; Pahkinen, E. Practical Methods for Design and Analysis of Complex Surveys, 2nd ed.; John Wiley & Sons, Inc.: Chichester, UK, 2004; ISBN 978-0-470-84769-5. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- Khlat, M.; Legleye, S.; Bricard, D. Migration-Related Changes in Smoking among Non-Western Immigrants in France. Eur. J. Public Health 2019, 29, 453–457. [Google Scholar] [CrossRef]
- Al-Ansari, B.; Thow, A.-M.; Day, C.A.; Conigrave, K.M. Extent of Alcohol Prohibition in Civil Policy in Muslim Majority Countries: The Impact of Globalization. Addiction 2016, 111, 1703–1713. [Google Scholar] [CrossRef]
- Inter-American Drug Abuse Control Commission (CICAD); Secretariat for Multidimensional Security (SMS). Report on Drug Use in the Americas 2019; Organization of American States (OAS): Washington, DC, USA, 2019; ISBN 978-0-8270-6793-6. [Google Scholar]
- Malisauskaite, G.; Klein, A. Drinking under Communism: Why Do Alcohol Consumption Habits in Eastern Europe Differ from the West in the Long-Run? J. Comp. Econ. 2018, 46, 821–837. [Google Scholar] [CrossRef]
- Yakovlev, E. Alcoholism and Mortality in Eastern Europe. IZA World Labor. 2021. [Google Scholar] [CrossRef]
- Charrier, L.; Comoretto, R.I.; Bersia, M.; Dalmasso, P.; Koumantakis, E.; Borraccino, A.; Baban, A.; Berchialla, P.; Lemma, P. Who Stays, Who Moves on and the Host Population: A Picture of Adolescents’ Perceived Well-Being and Risk Behaviours. Int. J. Environ. Res. Public Health 2023, 20, 5902. [Google Scholar] [CrossRef] [PubMed]
- Vaičiūnas, T.; Žemaitaitytė, M.; Lange, S.; Štelemėkas, M.; Oja, L.; Petkevičienė, J.; Kowalewska, A.; Pudule, I.; Piksööt, J.; Šmigelskas, K. Trends in Adolescent Substance Use: Analysis of HBSC Data for Four Eastern European Countries, 1994–2018. Int. J. Environ. Res. Public Health 2022, 19, 15457. [Google Scholar] [CrossRef] [PubMed]
- Curtis, P.; Thompson, J.; Fairbrother, H. Migrant Children within Europe: A Systematic Review of Children’s Perspectives on Their Health Experiences. Public Health 2018, 158, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Sarasa-Renedo, A.; Sordo, L.; Pulido, J.; Guitart, A.; González-González, R.; Hoyos, J.; Bravo, M.J.; Barrio, G. Effect of Immigration Background and Country-of-Origin Contextual Factors on Adolescent Substance Use in Spain. Drug Alcohol. Depend. 2015, 153, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Abebe, D.S.; Hafstad, G.S.; Brunborg, G.S.; Kumar, B.N.; Lien, L. Binge Drinking, Cannabis and Tobacco Use Among Ethnic Norwegian and Ethnic Minority Adolescents in Oslo, Norway. J. Immigr. Minor. Health 2015, 17, 992–1001. [Google Scholar] [CrossRef]
- Tabri, N.; Will Shead, N.; Wohl, M.J.A. Me, Myself, and Money II: Relative Deprivation Predicts Disordered Gambling Severity via Delay Discounting, Especially Among Gamblers Who Have a Financially Focused Self-Concept. J. Gambl. Stud. 2017, 33, 1201–1211. [Google Scholar] [CrossRef]
- Freund, E.A.; Morris, I.L. Gambling and Income Inequality in the States. Policy Stud. J. 2006, 34, 265–276. [Google Scholar] [CrossRef]
- Kim, W.; Kim, I.; Nochajski, T.H. Predictors of Gambling Behaviors in Filipino Americans Living in Honolulu or San Francisco. J. Gambl. Stud. 2012, 28, 297–314. [Google Scholar] [CrossRef]
- Scull, S.; Woolcock, G. Problem Gambling in Non-English Speaking Background Communities in Queensland, Australia: A Qualitative Exploration. Int. Gambl. Stud. 2005, 5, 29–44. [Google Scholar] [CrossRef]
- Hawkins, J.D.; Catalano, R.F.; Miller, J.Y. Risk and Protective Factors for Alcohol and Other Drug Problems in Adolescence and Early Adulthood: Implications for Substance Abuse Prevention. Psychol. Bull. 1992, 112, 64–105. [Google Scholar] [CrossRef]
- Huff, A.J.; Luzingu, J.K.; Valdez, E.S.; Brady, B.; Bell, M. Does High Family Support Protect against Substance Use in Adolescents Who Perceive High Disordered Neighborhood Stress, Border Community and Immigration Stress or Normalization of Drug Trafficking at the US-Mexico Border? Analysis of the BASUS Survey. J. Migr. Health 2023, 7, 100164. [Google Scholar] [CrossRef]
- Ventura, A.S.; Bagley, S.M. To Improve Substance Use Disorder Prevention, Treatment and Recovery: Engage the Family. J. Addict. Med. 2017, 11, 339–341. [Google Scholar] [CrossRef]
- Kumpfer, K.L.; Alvarado, R.; Whiteside, H.O. Family-Based Interventions for Substance Use and Misuse Prevention. Subst. Use Misuse 2003, 38, 1759–1787. [Google Scholar] [CrossRef]
- Algan, Y.; Bisin, A.; Manning, A.; Verdier, T. (Eds.) Cultural Integration of Immigrants in Europe; Oxford University Press: Oxford, UK; New York, NY, USA, 2012; ISBN 978-0-19-966009-4. [Google Scholar]
- Prado, G.; Huang, S.; Schwartz, S.J.; Maldonado-Molina, M.M.; Bandiera, F.C.; de la Rosa, M.; Pantin, H. What Accounts for Differences in Substance Use among U.S.-Born and Immigrant Hispanic Adolescents?: Results from a Longitudinal Prospective Cohort Study. J. Adolesc. Health 2009, 45, 118–125. [Google Scholar] [CrossRef]
- Groves, R.M. Nonresponse Rates and Nonresponse Bias in Household Surveys. Public Opin. Q. 2006, 70, 646–675. [Google Scholar] [CrossRef]
- Zlobina, A.; Basabe, N.; Paez, D.; Furnham, A. Sociocultural Adjustment of Immigrants: Universal and Group-Specific Predictors. Int. J. Intercult. Relat. 2006, 30, 195–211. [Google Scholar] [CrossRef]
- Borges, G.; Rafful, C.; Benjet, C.; Tancredi, D.J.; Saito, N.; Aguilar-Gaxiola, S.; Medina-Mora, M.E.; Breslau, J. Mexican Immigration to the US and Alcohol and Drug Use Opportunities: Does It Make a Difference in Alcohol and/or Drug Use? Drug Alcohol. Depend. 2012, 125 (Suppl. S1), S4–S11. [Google Scholar] [CrossRef]


{kind=link}
| BOYS | GIRLS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AREA OF ORIGIN | AREA OF ORIGIN | |||||||||
| Italy | W | EE | nW/nE | Total | Italy | W | EE | nW/nE | Total | |
| N = 7862 | N = 477 | N = 474 | N = 532 | N = 9345 | N = 7953 | N = 496 | N = 493 | N = 507 | N = 9449 | |
| Current smoking | 26.8% | 26.2% | 24.3% | 25.6% | 26.6% | 32.7% | 34.1% | 31.8% | 27.2% | 32.4% |
| Current alcohol consumption | 29.4% | 31.1% | 24.1% | 17.6% | 28.5% | 20.2% | 22.1% | 15.2% | 12.8% | 19.6% |
| Drunkenness | 20.4% | 21.0% | 23.4% | 16.3% | 20.3% | 18.4% | 21.7% | 20.2% | 15.6% | 18.5% |
| Binge drinking | 27.2% | 27.4% | 24.0% | 19.6% | 26.6% | 21.5% | 24.7% | 22.7% | 20.2% | 21.7% |
| Cannabis | 16.9% | 17.7% | 17.6% | 20.6% | 17.1% | 12.0% | 15.4% | 13.7% | 13.6% | 12.3% |
| Multiple substance use | 27.4% | 27.5% | 30.6% | 27.3% | 27.5% | 28.4% | 31.5% | 28.6% | 23.7% | 28.3% |
| At risk/problem gambling | 17.4% | 16.6% | 21.6% | 25.8% | 17.9% | 6.8% | 7.6% | 15.2% | 7.6% | 7.2% |
| Has friends who smoke | ||||||||||
| None/Few | 37.2% | 30.6% | 37.9% | 42.0% | 37.1% | 31.6% | 28.3% | 29.2% | 32.9% | 31.4% |
| Some | 34.0% | 37.3% | 30.5% | 28.1% | 33.8% | 31.2% | 33.7% | 27.1% | 32.2% | 31.2% |
| Many/All | 28.8% | 32.2% | 31.6% | 30.0% | 29.2% | 37.2% | 38.0% | 43.6% | 34.8% | 37.4% |
| Has friends who drink alcohol | ||||||||||
| None/Few | 27.6% | 24.4% | 30.7% | 33.3% | 27.8% | 25.6% | 23.4% | 23.7% | 27.1% | 25.5% |
| Some | 33.1% | 33.7% | 31.8% | 27.0% | 32.8% | 32.4% | 33.1% | 30.2% | 30.9% | 32.3% |
| Many/All | 39.3% | 41.9% | 37.6% | 39.6% | 39.4% | 42.0% | 43.5% | 46.0% | 42.0% | 42.3% |
| Has friends who take cannabis | ||||||||||
| None/Few | 71.0% | 69.9% | 71.1% | 64.8% | 70.7% | 70.7% | 67.8% | 67.3% | 68.6% | 70.3% |
| Some | 17.0% | 17.6% | 14.0% | 16.7% | 16.9% | 17.4% | 19.0% | 18.6% | 17.6% | 17.6% |
| Many/All | 12.0% | 12.5% | 14.9% | 18.6% | 12.5% | 11.9% | 13.2% | 14.2% | 13.8% | 12.1% |
| Peer support | 60.7% | 62.9% | 52.6% | 48.7% | 59.8% | 70.1% | 69.9% | 60.0% | 62.4% | 69.2% |
| Family support | 71.5% | 70.8% | 69.1% | 56.3% | 70.5% | 66.1% | 66.3% | 49.9% | 54.0% | 64.6% |
| Teacher support | 49.7% | 50.1% | 48.8% | 46.1% | 49.5% | 45.3% | 43.6% | 43.6% | 46.7% | 45.2% |
| Classmates support | 76.3% | 76.0% | 71.4% | 70.2% | 75.7% | 65.2% | 65.7% | 55.7% | 57.3% | 64.3% |
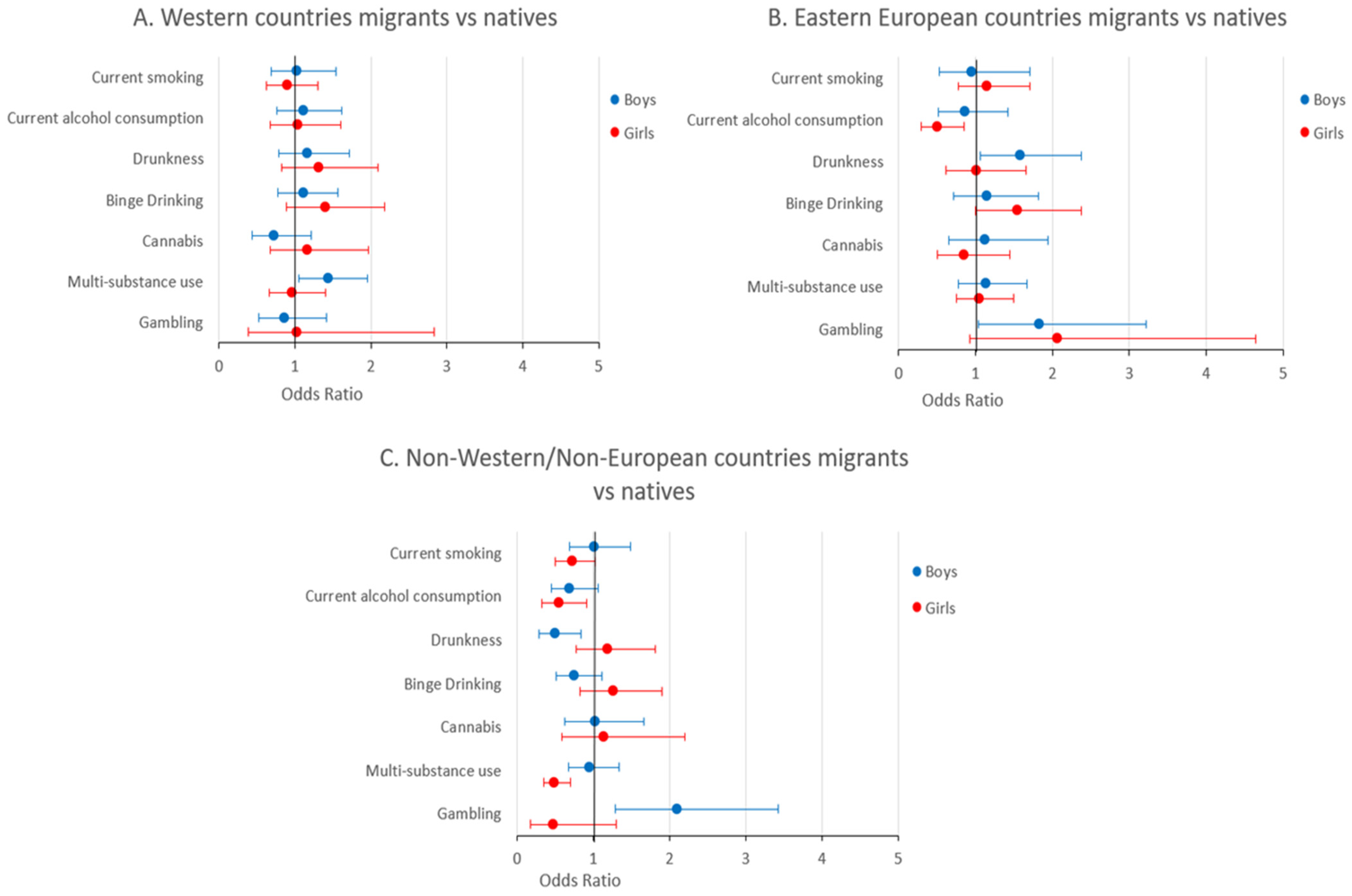
| Country/Region of Birth | Current Smoking § | Current Alcohol Consumption § | Drunkenness § | Binge Drinking § | Cannabis § | Multiple Substance Use ^ | At-Risk or Problem Gambling ^ |
|---|---|---|---|---|---|---|---|
| BOYS | |||||||
| Italy (native-born) | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Western Countries | 1.03 (0.69–1.54) | 1.11 (0.76–1.61) | 1.16 (0.79–1.71) | 1.11 (0.78–1.57) | 0.73 (0.44–1.21) | 1.44 (1.05–1.96) | 0.86 (0.53–1.42) |
| Eastern European Countries | 0.95 (0.53–1.70) | 0.86 (0.52–1.42) | 1.58 (1.06–2.37) | 1.15 (0.72–1.82) | 1.12 (0.65–1.94) | 1.14 (0.78–1.67) | 1.83 (1.04–3.22) |
| Non-Western/Non-European Countries | 1.01 (0.69–1.49) | 0.69 (0.45–1.06) | 0.50 (0.29–0.84) | 0.75 (0.51–1.11) | 1.03 (0.63–1.66) | 0.95 (0.68–1.34) | 2.10 (1.29–3.42) |
| GIRLS | |||||||
| Italy (native-born) | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Western Countries | 0.90 (0.62–1.30) | 1.04 (0.67–1.60) | 1.32 (0.83–2.09) | 1.40 (0.89–2.18) | 1.16 (0.68–1.97) | 0.96 (0.66–1.40) | 1.03 (0.38–2.83) |
| Eastern European Countries | 1.15 (0.77–1.70) | 0.50 (0.29–0.85) | 1.01 (0.61–1.66) | 1.54 (1.00–2.37) | 0.85 (0.50–1.45) | 1.05 (0.75–1.49) | 2.07 (0.93–4.64) |
| Non-Western/Non-European Countries | 0.72 (0.50–1.03) | 0.55 (0.33–0.91) | 1.19 (0.78–1.81) | 1.26 (0.83–1.90) | 1.14 (0.59–2.20) | 0.49 (0.35–0.70) | 0.48 (0.17–1.30) |
| Country/Region of Birth | Generation | Current Smoking § | Current Alcohol Consumption § | Drunkenness § | Binge Drinking § | Cannabis § | Multiple Substance Use ^ | At-Risk or Problem Gambling ^ |
|---|---|---|---|---|---|---|---|---|
| BOYS | ||||||||
| Italy (native-born) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Western Countries | First | 0.60 (0.17–2.13) | 1.13 (0.32–4.05) | 1.10 (0.29–4.13) | 0.54 (0.15–2.00) | 0.22 (0.03–1.58) | 0.86 (0.24–3.02) | 1.33 (0.35–5.02) |
| Second | 1.06 (0.69–1.62) | 1.11 (0.75–1.63) | 1.16 (0.78–1.73) | 1.14 (0.80–1.63) | 0.77 (0.46–1.27) | 1.47 (1.07–2.02) | 0.84 (0.50–1.42) | |
| Eastern European Countries | First | 1.32 (0.48–3.68) | 1.18 (0.53–2.66) | 2.08 (1.01–4.32) | 1.00 (0.52–1.93) | 1.81 (0.74–4.45) | 1.30 (0.73–2.31) | 1.52 (0.72–3.18) |
| Second | 0.79 (0.42–1.48) | 0.71 (0.39–1.31) | 1.35 (0.80–2.28) | 1.27 (0.75–2.17) | 0.82 (0.42–1.59) | 1.04 (0.65–1.66) | 2.04 (0.98–4.21) | |
| Non-Western/Non-European Countries | First | 0.46 (0.18–1.17) | 1.08 (0.45–2.55) | 0.58 (0.20–1.66) | 0.74 (0.37–1.47) | 1.22 (0.51–2.92) | 0.99 (0.54–1.81) | 2.76 (1.02–7.43) |
| Second | 1.23 (0.78–1.93) | 0.59 (0.36–0.98) | 0.48 (0.27–0.85) | 0.75 (0.47–1.22) | 0.97 (0.56–1.65) | 0.94 (0.63–1.40) | 1.92 (1.08–3.42) | |
| GIRLS | ||||||||
| Italy (native-born) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Western Countries | First | 0.74 (0.18–3.05) | 0.36 (0.06–2.02) | 1.54 (0.41–5.83) | 0.69 (0.18–2.63) | 3.60 (0.85–15.2) | 0.58 (0.15–2.23) | NA * |
| Second | 0.90 (0.62–1.32) | 1.07 (0.69–1.67) | 1.31 (0.82–2.10) | 1.43 (0.91–2.27) | 1.09 (0.63–1.89) | 0.99 (0.67–1.45) | 1.10 (0.40–2.98) | |
| Eastern European Countries | First | 0.88 (0.51–1.52) | 0.33 (0.15–0.73) | 0.93 (0.44–1.95) | 2.05 (1.04–4.02) | 0.98 (0.49–1.99) | 0.88 (0.52–1.48) | 1.31 (0.38–4.54) |
| Second | 1.33 (0.79–2.24) | 0.61 (0.32–1.16) | 1.05 (0.58–1.91) | 1.26 (0.74–2.13) | 0.79 (0.39–1.60) | 1.18 (0.75–1.86) | 2.46 (0.95–6.39) | |
| Non-Western/Non-European Countries | First | 1.16 (0.57–2.37) | 0.49 (0.16–1.55) | 1.69 (0.68–4.18) | 2.71 (1.26–5.84) | 1.18 (0.34–4.09) | 0.62 (0.31–1.25) | 4.38 (1.26–15.3) |
| Second | 0.64 (0.43–0.95) | 0.57 (0.33–0.97) | 1.07 (0.66–1.75) | 0.95 (0.60–1.49) | 1.13 (0.57–2.24) | 0.46 (0.30–0.70) | 0.06 (0.02–0.20) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koumantakis, E.; Comoretto, R.I.; Dalmasso, P.; Bersia, M.; Lemma, P.; Lazzeri, G.; Nardone, P.; Vieno, A.; Galeotti, T.; Berchialla, P.; et al. Risk Behaviors among Migrant Adolescents in Italy. Children 2023, 10, 1816. https://doi.org/10.3390/children10111816
Koumantakis E, Comoretto RI, Dalmasso P, Bersia M, Lemma P, Lazzeri G, Nardone P, Vieno A, Galeotti T, Berchialla P, et al. Risk Behaviors among Migrant Adolescents in Italy. Children. 2023; 10(11):1816. https://doi.org/10.3390/children10111816
Chicago/Turabian StyleKoumantakis, Emanuele, Rosanna Irene Comoretto, Paola Dalmasso, Michela Bersia, Patrizia Lemma, Giacomo Lazzeri, Paola Nardone, Alessio Vieno, Tommaso Galeotti, Paola Berchialla, and et al. 2023. "Risk Behaviors among Migrant Adolescents in Italy" Children 10, no. 11: 1816. https://doi.org/10.3390/children10111816
APA StyleKoumantakis, E., Comoretto, R. I., Dalmasso, P., Bersia, M., Lemma, P., Lazzeri, G., Nardone, P., Vieno, A., Galeotti, T., Berchialla, P., & Charrier, L. (2023). Risk Behaviors among Migrant Adolescents in Italy. Children, 10(11), 1816. https://doi.org/10.3390/children10111816