
Atopic Dermatitis in Italian Pre-School Children: Literature Review of Epidemiological Data with a Focus on Disease Prevalence and Severity

 ,
,
Abstract
:1. Introduction
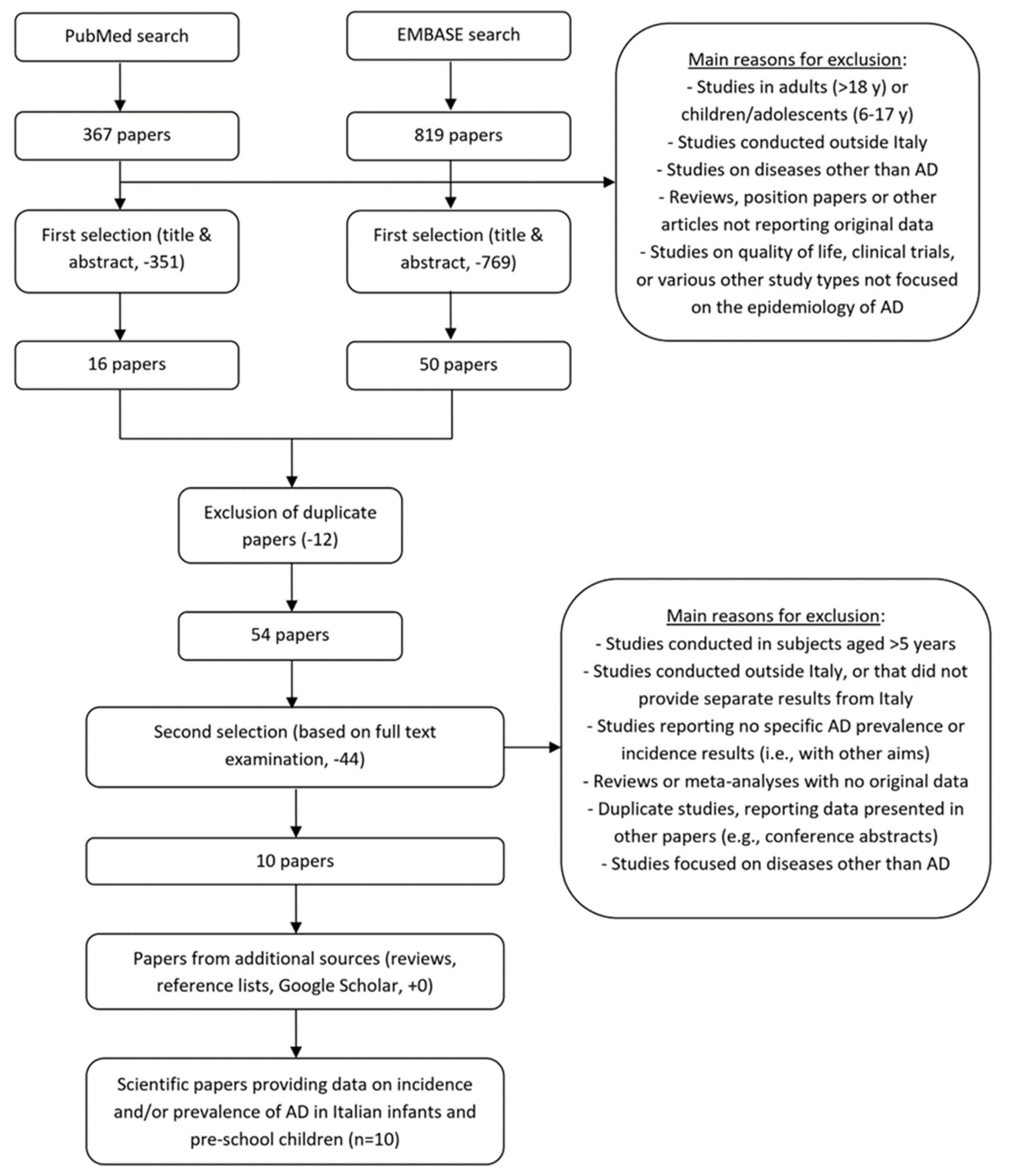
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laughter, M.R.; Maymone, M.B.C.; Mashayekhi, S.; Arents, B.W.M.; Karimkhani, C.; Langan, S.M.; Dellavalle, R.P.; Flohr, C. The global burden of atopic dermatitis: Lessons from the Global Burden of Disease Study 1990–2017. Br. J. Dermatol. 2021, 184, 304–309. [Google Scholar] [CrossRef]
- Stander, S. Atopic Dermatitis. N. Engl. J. Med. 2021, 384, 1136–1143. [Google Scholar] [CrossRef]
- Williams, H.C. Clinical practice. Atopic dermatitis. N. Engl. J. Med. 2005, 352, 2314–2324. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Illi, S.; von Mutius, E.; Lau, S.; Nickel, R.; Gruber, C.; Niggemann, B.; Wahn, U.; Multicenter Allergy Study, G. The natural course of atopic dermatitis from birth to age 7 years and the association with asthma. J. Allergy Clin. Immunol. 2004, 113, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Lewis-Jones, S. Quality of life and childhood atopic dermatitis: The misery of living with childhood eczema. Int. J. Clin. Pract. 2006, 60, 984–992. [Google Scholar] [CrossRef]
- Monti, F.; Agostini, F.; Gobbi, F.; Neri, E.; Schianchi, S.; Arcangeli, F. Quality of life measures in Italian children with atopic dermatitis and their families. Ital. J. Pediatr. 2011, 37, 59. [Google Scholar] [CrossRef]
- Barbarot, S.; Auziere, S.; Gadkari, A.; Girolomoni, G.; Puig, L.; Simpson, E.L.; Margolis, D.J.; de Bruin-Weller, M.; Eckert, L. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy 2018, 73, 1284–1293. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Barbarot, S.; Gadkari, A.; Simpson, E.L.; Weidinger, S.; Mina-Osorio, P.; Rossi, A.B.; Brignoli, L.; Saba, G.; Guillemin, I.; et al. Atopic dermatitis in the pediatric population: A cross-sectional, international epidemiologic study. Ann. Allergy Asthma Immunol. 2021, 126, 417–428.e2. [Google Scholar] [CrossRef]
- Agosti, M.; Vegni, C.; Gangi, S.; Benedetti, V.; Marini, A. Allergic manifestations in very low-birthweight infants: A 6-year follow-up. Acta Paediatr. Suppl. 2003, 91, 44–47. [Google Scholar] [CrossRef]
- Indinnimeo, L.; Porta, D.; Forastiere, F.; De Vittori, V.; De Castro, G.; Zicari, A.M.; Tancredi, G.; Melengu, T.; Duse, M. Prevalence and risk factors for atopic disease in a population of preschool children in Rome: Challenges to early intervention. Int. J. Immunopathol. Pharmacol. 2016, 29, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Cipriani, S.; Zinetti, C.; Chatenoud, L.; Frigerio, L.; Amuso, G.; Ciammella, M.; Di Landro, A.; Naldi, L. Perinatal factors and the risk of atopic dermatitis: A cohort study. Pediatr. Allergy Immunol. 2014, 25, 43–50. [Google Scholar] [CrossRef]
- Peroni, D.G.; Piacentini, G.L.; Bodini, A.; Rigotti, E.; Pigozzi, R.; Boner, A.L. Prevalence and risk factors for atopic dermatitis in preschool children. Br. J. Dermatol. 2008, 158, 539–543. [Google Scholar] [CrossRef] [PubMed]
- El Hachem, M.; Naldi, L.; Neri, I.; Pedone, M.P.; Fanelli, F.; Galeone, C. Atopic dermatitis in schoolchildren and adolescents: A critical review of Italian epidemiological data and systemic treatments. Ital. J. Dermatol. Venereol. 2021, 156, 650–658. [Google Scholar] [CrossRef]
- Cantarutti, A.; Donà, D.; Visentin, F.; Borgia, E.; Scamarcia, A.; Cantarutti, L.; Peruzzi, E.; Egan, C.G.; Villa, M.; Giaquinto, C. Epidemiology of Frequently Occurring Skin Diseases in Italian Children from 2006 to 2012: A Retrospective, Population-Based Study. Pediatr. Dermatol. 2015, 32, 668–678. [Google Scholar] [CrossRef]
- Fortes, C.; Mastroeni, S.; Mannooranparampil, T.J.; Di Lallo, D. Pre-natal folic acid and iron supplementation and atopic dermatitis in the first 6 years of life. Arch. Dermatol. Res. 2019, 311, 361–367. [Google Scholar] [CrossRef]
- Fuertes, E.; Sunyer, J.; Gehring, U.; Porta, D.; Forastiere, F.; Cesaroni, G.; Vrijheid, M.; Guxens, M.; Annesi-Maesano, I.; Slama, R.; et al. Associations between air pollution and pediatric eczema, rhinoconjunctivitis and asthma: A meta-analysis of European birth cohorts. Environ. Int. 2020, 136, 105474. [Google Scholar] [CrossRef]
- Parmes, E.; Pesce, G.; Sabel, C.E.; Baldacci, S.; Bono, R.; Brescianini, S.; D’Ippolito, C.; Hanke, W.; Horvat, M.; Liedes, H.; et al. Influence of residential land cover on childhood allergic and respiratory symptoms and diseases: Evidence from 9 European cohorts. Environ. Res. 2020, 183, 108953. [Google Scholar] [CrossRef]
- Stazi, M.A.; Sampogna, F.; Montagano, G.; Grandolfo, M.E.; Couilliot, M.F.; Annesi-Maesano, I. Early life factors related to clinical manifestations of atopic disease but not to skin-prick test positivity in young children. Pediatr. Allergy Immunol. 2002, 13, 105–112. [Google Scholar] [CrossRef]
- Ruggiero, G.; Gelmetti, C.; Adamo, M.C.; Baldessarri, D.; Bonfanti, R.; Brero, P.; Calzaretti, R.; Candelori, G.; Danesi, R.; D’Amanti, V.; et al. Atopic dermatitis (AD) management in an Italian pediatric clinic. G. Ital. Dermatol. Venereol. 2012, 147, 71–81. [Google Scholar]
- Galli, E.; Maiello, N.; Cipriani, F.; La Grutta, S.; Fasola, S.; Carello, R.; Caminiti, L.; Licari, A.; Landi, M.; Di Mauro, D.; et al. Atopic dermatitis phenotypes in preschool and school-age children: A latent class analysis. J. Investig. Allergol. Clin. Immunol. 2020, 30, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Shaw, T.E.; Currie, G.P.; Koudelka, C.W.; Simpson, E.L. Eczema prevalence in the United States: Data from the 2003 National Survey of Children’s Health. J. Investig. Dermatol. 2011, 131, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Odhiambo, J.A.; Williams, H.C.; Clayton, T.O.; Robertson, C.F.; Asher, M.I.; Group, I.P.T.S. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J. Allergy Clin. Immunol. 2009, 124, 1251–1258.e23. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Robertson, C.; Stewart, A.; Ait-Khaled, N.; Anabwani, G.; Anderson, R.; Asher, I.; Beasley, R.; Bjorksten, B.; Burr, M.; et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the International Study of Asthma and Allergies in Childhood. J. Allergy Clin. Immunol. 1999, 103, 125–138. [Google Scholar] [CrossRef]
- Draaisma, E.; Garcia-Marcos, L.; Mallol, J.; Sole, D.; Perez-Fernandez, V.; Brand, P.L.; Group, E.S. A multinational study to compare prevalence of atopic dermatitis in the first year of life. Pediatr. Allergy Immunol. 2015, 26, 359–366. [Google Scholar] [CrossRef]
- Bylund, S.; Kobyletzki, L.B.; Svalstedt, M.; Svensson, Å. Prevalence and Incidence of Atopic Dermatitis: A Systematic Review. Acta Derm. Venereol. 2020, 100, adv00160. [Google Scholar] [CrossRef]
- Spuls, P.I.; Gerbens, L.A.A.; Simpson, E.; Apfelbacher, C.J.; Chalmers, J.R.; Thomas, K.S.; Prinsen, C.A.C.; von Kobyletzki, L.B.; Singh, J.A.; Williams, H.C.; et al. Patient-Oriented Eczema Measure (POEM), a core instrument to measure symptoms in clinical trials: A Harmonising Outcome Measures for Eczema (HOME) statement. Br. J. Dermatol. 2017, 176, 979–984. [Google Scholar] [CrossRef]
- Emerson, R.M.; Charman, C.R.; Williams, H.C. The Nottingham Eczema Severity Score: Preliminary refinement of the Rajka and Langeland grading. Br. J. Dermatol. 2000, 142, 288–297. [Google Scholar] [CrossRef]
- Huang, E.; Ong, P.Y. Severe Atopic Dermatitis in Children. Curr. Allergy Asthma Rep. 2018, 18, 35. [Google Scholar] [CrossRef]
- Ricci, G.; Bendandi, B.; Bellini, F.; Patrizi, A.; Masi, M. Atopic dermatitis: Quality of life of young Italian children and their families and correlation with severity score. Pediatr. Allergy Immunol. 2007, 18, 245–249. [Google Scholar] [CrossRef]
- McAleer, M.A.; Flohr, C.; Irvine, A.D. Management of difficult and severe eczema in childhood. BMJ 2012, 345, e4770. [Google Scholar] [CrossRef] [PubMed]
- Proudfoot, L.E.; Powell, A.M.; Ayis, S.; Barbarot, S.; Baselga Torres, E.; Deleuran, M.; Fölster-Holst, R.; Gelmetti, C.; Hernández-Martin, A.; Middelkamp-Hup, M.A.; et al. The European treatment of severe atopic eczema in children taskforce (TREAT) survey. Br. J. Dermatol. 2013, 169, 901–909. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Source | Period | Area | Study Design | Study Population | Type of Diagnosis | Notes |
|---|---|---|---|---|---|---|
| Agosti et al., 2003 [10] | 1994–2000 | Milan-Varese | Birth cohort | Population-based (hospital newborns) | Arata Criteria | |
| Cantarutti et al., 2015 [15] | 2006–2012 | Italy | Retrospective cohort | Primary care patients | Diagnosis of AD registered by a paediatrician | |
| Fortes et al., 2019 [16] | NR | Rome | Birth cohort | Population-based (hospital newborns) | UK Diagnostic Criteria | Study not focused on AD incidence/prevalence, but it reports such results |
| Fuertes et al., 2020 [17] | 2003–2008 | Rome (within an international study) | Birth cohort | Population-based (hospital newborns) | Based on 2 ISAAC questions (itchy rash and localisation, in the previous 12 months) | Study not focused on AD incidence/prevalence, but it reports such results |
| Indinnimeo et al., 2016 [11] | NR | Rome | Cross-sectional survey | Population-based | AD in the last 12 months (ISAAC), self-reported by parents | |
| Parazzini et al., 2014 [12] | 2007–2010 | Bergamo | Birth cohort | Population-based (hospital newborns) | UK Working Party diagnostic criteria and diagnosis by a paediatrician or dermatologist, reported by parents | Study not focused on AD incidence/prevalence, but it reports such results |
| Parmes et al., 2020 [18] | 2009–2014 | Italy (within an international study) | Birth cohort | Population-based (hospital newborns) | Itchy rash that comes and goes or diagnosis of AD by a clinician | Study not focused on AD incidence/prevalence, but it reports such results |
| Peroni et al., 2008 [13] | NR | Verona | Cross-sectional survey | Population-based |
| |
| Silverberg et al., 2021 [9] | 2018–2019 | Italy | Web survey | Population-based |
| |
| Stazi et al., 2002 [19] | 1993–1994 | Basilicata | Cross-sectional survey | Population-based | AD diagnosed by a clinician |
| Source | N | Age Considered | Lifetime Prevalence | Period (12 mo) Prevalence | Notes |
|---|---|---|---|---|---|
| Agosti et al., 2003 [10] | 98 | 0–6 years | 33.7% over the entire 6-year period | NR | Data for full-term children. Results of children with very low birth weight were excluded |
| Cantarutti et al., 2015 [15] | ≈55,000 (0 y: 10,000; 1–4 y: 45,000) |
| NR |
| Year-by-year results, for the period from 2006 to 2012 Approximate results, as they were derived from two figures |
| Fortes et al., 2019 [16] | 344 | 0–6 years | 7.8% over the entire 6-year period | NR | Among the diagnostic criteria is ‘onset of AD before the age of 2 years’ |
| Fuertes et al., 2020 [17] | 581 | 4 years | NR | 13.3% | Only data from the Italian GASPII cohort were reported |
| Indinnimeo et al., 2016 [11] | 494 | 3–5 | NR | 11.8% | |
| Parazzini et al., 2014 [12] | 796 | 0–1 year |
| NR | |
| Parmes et al., 2020 [18] | 274 | 0–3 years | 17.8% over the entire 3-year period | NR | Other Italian cohorts in the study were excluded because most of the children were of school age |
| Peroni et al., 2008 [13] | 1402 | 3–5 | 20.9% over the entire 3–5 year period (based on symptoms) |
| |
| Silverberg et al., 2021 [9] | 1547 | 6 months to <6 years | NR |
| The study reports information on the severity of AD, based on PGA and POEM |
| Stazi et al., 2002 [19] | 201 | 3 months to 5 years | 8.0% | NR |
| All Studies | Only Recent Studies (≥2010) | |||||||
|---|---|---|---|---|---|---|---|---|
| Epidemiological Measurement | No. of Studies | No. of Measures | Range | Median | No. of Studies | No. of Measures | Range | Median |
| Lifetime prevalence | 6 | 6 | 7.8–33.7% | 19.3% | 2 | 2 | 7.8–17.8% | 12.8% |
| Period prevalence, 12 months | 5 | 8 b | 4.0–42.2% b | 14.3% | 3 | 5 b | 4.0–42.2% b | 11.8% |
| Incidence rate (/100 py) | 1 | 2 b | 2.5–9.0 b | 5.7 | 1 | 2 b | 2.5–9.0 b | 5.7 |
| Source | Area | Study Design | No. Enrolled | Severity Measurement | Indicator/Level | Result |
|---|---|---|---|---|---|---|
| Ruggiero et al., 2012 [20] | Italy, 16 regions involved | Survey of family paediatricians | 437 | Simple question on the case history of each paediatrician | % of cases evaluated as: | |
| 68.9% | |||||
| 23.3% | |||||
| 7.8% | |||||
| Galli et al., 2020 [21] | Italy, 9 cities | Cross-sectional, paediatric or allergy centre patients | 206 at pre-school age | SCORAD | % of cases with SCORAD: | |
| 64% | |||||
| 25% | |||||
| 11% | |||||
| Silverberg et al., 2021 [9] | Italy (within an international study conducted in 18 countries) | Cross-sectional, web-survey | 1547, of which 132 with AD diagnosed by a clinician | POEM and PtGA | % of cases with POEM: | |
| 52.2% | |||||
| 38.7% | |||||
| 8.4% | |||||
| % of cases with PtGA: | ||||||
| 54.2% | |||||
| 34.3% | |||||
| 10.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neri, I.; Galeone, C.; Pelucchi, C.; Ronci, G.; Matruglio, P.; Pedone, M.P.; Galli, E. Atopic Dermatitis in Italian Pre-School Children: Literature Review of Epidemiological Data with a Focus on Disease Prevalence and Severity. Children 2023, 10, 1629. https://doi.org/10.3390/children10101629
Neri I, Galeone C, Pelucchi C, Ronci G, Matruglio P, Pedone MP, Galli E. Atopic Dermatitis in Italian Pre-School Children: Literature Review of Epidemiological Data with a Focus on Disease Prevalence and Severity. Children. 2023; 10(10):1629. https://doi.org/10.3390/children10101629
Chicago/Turabian StyleNeri, Iria, Carlotta Galeone, Claudio Pelucchi, Gianluca Ronci, Paolo Matruglio, Maria Paola Pedone, and Elena Galli. 2023. "Atopic Dermatitis in Italian Pre-School Children: Literature Review of Epidemiological Data with a Focus on Disease Prevalence and Severity" Children 10, no. 10: 1629. https://doi.org/10.3390/children10101629
APA StyleNeri, I., Galeone, C., Pelucchi, C., Ronci, G., Matruglio, P., Pedone, M. P., & Galli, E. (2023). Atopic Dermatitis in Italian Pre-School Children: Literature Review of Epidemiological Data with a Focus on Disease Prevalence and Severity. Children, 10(10), 1629. https://doi.org/10.3390/children10101629