
Impact of Delayed Time to Antibiotics in Medical and Surgical Necrotizing Enterocolitis
 ,
,
Abstract
1. Introduction
2. Materials and Methods
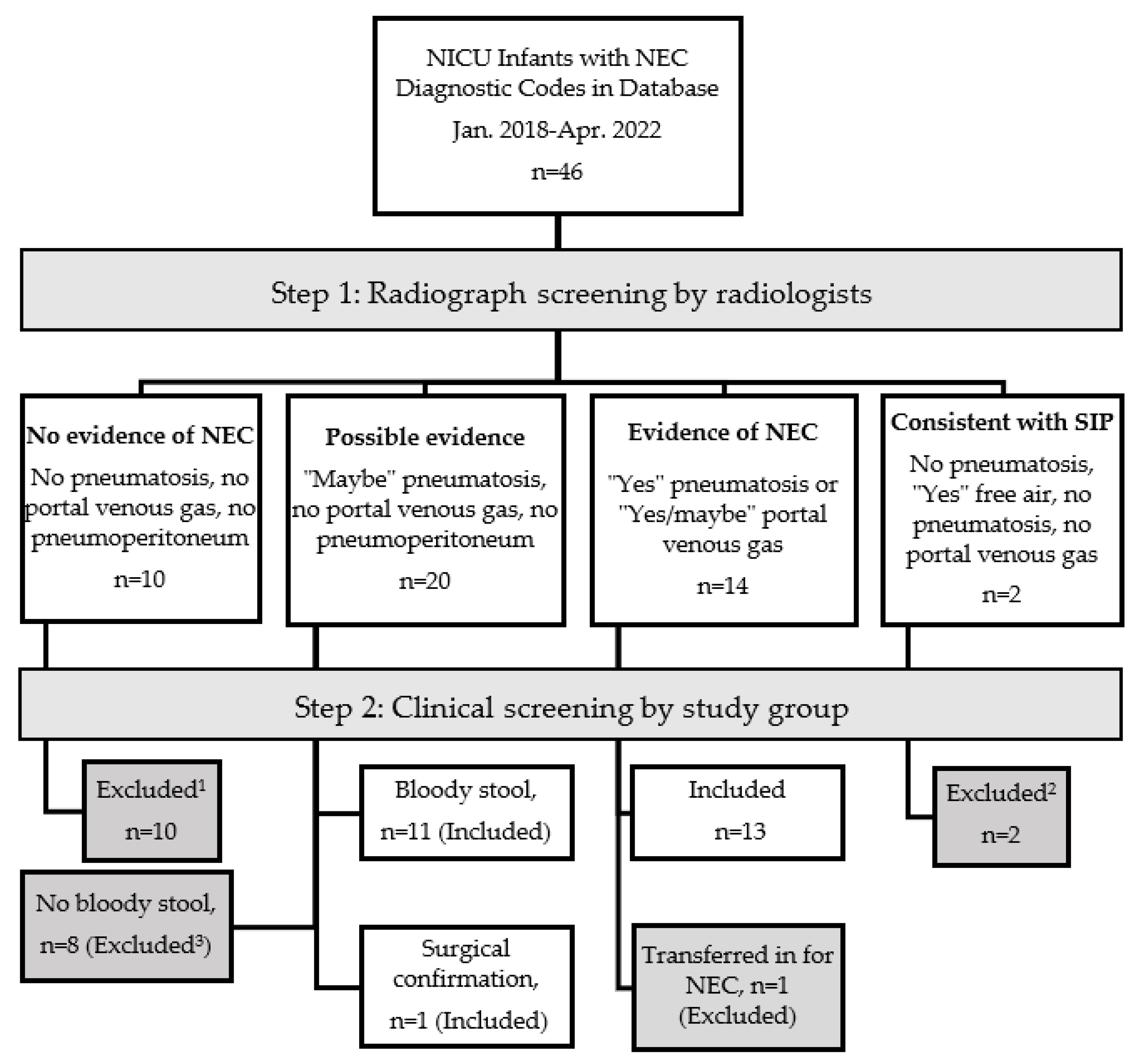
2.1. Study Design and Population
2.2. Independent Radiographic Review
2.3. Electronic Medical Record Review
2.4. Statistics
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nanthakumar, N.N.; Fusunyan, R.D.; Sanderson, I.; Walker, W.A. Inflammation in the developing human intestine: A possible pathophysiologic contribution to necrotizing enterocolitis. Proc. Natl. Acad. Sci. USA 2000, 97, 6043–6048. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.W.; Nasr, T.R.; Stoll, B.J. Necrotizing enterocolitis: Recent scientific advances in pathophysiology and prevention. Seminars in Perinatology 2008, 23, 70–82. [Google Scholar] [CrossRef]
- Neu, J.; Walker, W.A. Necrotizing enterocolitis. New Engl. J. Med. 2011, 364, 255–264. [Google Scholar] [CrossRef]
- Patel, R.M.; Ferguson, J.; McElroy, S.J.; Khashu, M.; Caplan, M.S. Defining necrotizing enterocolitis: Current difficulties and future opportunities. Pediatr. Res. 2020, 88, 10–15. [Google Scholar] [CrossRef]
- Han, S.M.; Hong, C.R.; Knell, J.; Edwards, E.M.; Morrow, K.A.; Soll, R.F.; Modi, B.P.; Horbar, J.D.; Jaksic, T. Trends in incidence and outcomes of necrotizing enterocolitis over the last 12 years: A multicenter cohort analysis. J. Pediatr. Surg. 2020, 55, 998–1001. [Google Scholar] [CrossRef] [PubMed]
- Pammi, M.; Cope, J.; Tarr, P.I.; Warner, B.B.; Morrow, A.L.; Mai, V.; Gregory, K.E.; Kroll, J.S.; McMurtry, V.; Ferris, M.J. Intestinal dysbiosis in preterm infants preceding necrotizing enterocolitis: A systematic review and meta-analysis. Microbiome 2017, 5, 5. [Google Scholar] [CrossRef]
- Wang, Y.; Hoenig, J.D.; Malin, K.J.; Qamar, S.; Petrof, E.O.; Sun, J.; Antonopoulos, D.A.; Chang, E.B.; Claud, E.C. 16S rRNA gene-based analysis of fecal microbiota from preterm infants with and without necrotizing enterocolitis. ISME J. 2009, 3, 944–954. [Google Scholar] [CrossRef] [PubMed]
- Piena-Spoel, M.; Albers, M.J.; ten Kate, J.; Tibboel, D. Intestinal permeability in newborns with necrotizing enterocolitis and controls: Does the sugar absorption test provide guidelines for the time to (re-) introduce enteral nutrition? J. Pediatr. Surg. 2001, 36, 587–592. [Google Scholar] [CrossRef]
- Sodhi, C.; Richardson, W.; Gribar, S.; Hackam, D.J. The development of animal models for the study of necrotizing enterocolitis. Dis. Model. Mech. 2008, 1, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Grishin, A.; Papillon, S.; Bell, B.; Wang, J.; Ford, H.R. The role of the intestinal microbiota in the pathogenesis of necrotizing enterocolitis. In Seminars in Pediatric Surgery; WB Saunders: Philadelphia, PA, USA, 2013; pp. 69–75. [Google Scholar]
- Bulle, E.B.; Peake, S.L.; Finnis, M.; Bellomo, R.; Delaney, A.; Investigators, A.; Investigators, A.; Committee, A.W.; Peake, S.; Delaney, A. Time to antimicrobial therapy in septic shock patients treated with an early goal-directed resuscitation protocol: A post-hoc analysis of the ARISE trial. Emerg. Med. Australas. 2021, 33, 409–417. [Google Scholar] [CrossRef]
- Gaieski, D.F.; Mikkelsen, M.E.; Band, R.A.; Pines, J.M.; Massone, R.; Furia, F.F.; Shofer, F.S.; Goyal, M. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit. Care Med. 2010, 38, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Londono, J.; Nino, C.; Archila, A.; Valencia, M.; Cardenas, D.; Perdomo, M.; Moncayo, G.; Vargas, C.; Vallejo, C.E.; Hincapie, C. Antibiotics has more impact on mortality than other early goal-directed therapy components in patients with sepsis: An instrumental variable analysis. J. Crit. Care 2018, 48, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.L.; Fitzgerald, J.C.; Balamuth, F.; Alpern, E.R.; Lavelle, J.; Chilutti, M.; Grundmeier, R.; Nadkarni, V.M.; Thomas, N.J. Delayed antimicrobial therapy increases mortality and organ dysfunction duration in pediatric sepsis. Crit. Care Med. 2014, 42, 2409. [Google Scholar] [CrossRef]
- Wasserman, R.C. Electronic medical records (EMRs), epidemiology, and epistemology: Reflections on EMRs and future pediatric clinical research. Acad. Pediatr. 2011, 11, 280–287. [Google Scholar] [CrossRef]
- Challis, P.; Larsson, L.; Stoltz Sjöström, E.; Serenius, F.; Domellöf, M.; Elfvin, A. Validation of the diagnosis of necrotising enterocolitis in a Swedish population-based observational study. Acta Paediatr. 2019, 108, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Selewski, D.T.; Cornell, T.T.; Heung, M.; Troost, J.P.; Ehrmann, B.J.; Lombel, R.M.; Blatt, N.B.; Luckritz, K.; Hieber, S.; Gajarski, R. Validation of the KDIGO acute kidney injury criteria in a pediatric critical care population. Intensive Care Med. 2014, 40, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Neu, J. Necrotizing enterocolitis: The search for a unifying pathogenic theory leading to prevention. Pediatr. Clin. 1996, 43, 409–432. [Google Scholar]
- Uauy, R.D.; Fanaroff, A.A.; Korones, S.B.; Phillips, E.A.; Phillips, J.B.; Wright, L.L.; members of the National Institute of Child Health and Human Development Neonatal Research Network. Necrotizing enterocolitis in very low birth weight infants: Biodemographic and clinical correlates. J. Pediatr. 1991, 119, 630–638. [Google Scholar] [CrossRef]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1. [Google Scholar] [CrossRef]
- Bell, M.J.; Ternberg, J.L.; Bower, R.J. The microbial flora and antimicrobial therapy of neonatal peritonitis. J. Pediatr. Surg. 1980, 15, 569–573. [Google Scholar] [CrossRef]
- Faix, R.G.; Polley, T.Z.; Grasela, T.H. A randomized, controlled trial of parenteral clindamycin in neonatal necrotizing enterocolitis. J. Pediatr. 1988, 112, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Scheifele, D.W.; Ginter, G.L.; Olsen, E.; Fussell, S.; Pendray, M. Comparison of two antibiotic regimens for neonatal necrotizing enterocolitis. J. Antimicrob. Chemother. 1987, 20, 421–429. [Google Scholar] [CrossRef]
- Gill, E.M.; Jung, K.; Qvist, N.; Ellebæk, M.B. Antibiotics in the medical and surgical treatment of necrotizing enterocolitis. A systematic review. BMC Pediatr. 2022, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Zarychanski, R.; Light, B.; Parrillo, J.; Maki, D.; Simon, D.; Laporta, D.; Lapinsky, S.; Ellis, P.; Mirzanejad, Y. Early combination antibiotic therapy yields improved survival compared with monotherapy in septic shock: A propensity-matched analysis. Crit. Care Med. 2010, 38, 1773–1785. [Google Scholar] [CrossRef]
- MacArthur, R.D.; Miller, M.; Albertson, T.; Panacek, E.; Johnson, D.; Teoh, L.; Barchuk, W. Adequacy of early empiric antibiotic treatment and survival in severe sepsis: Experience from the MONARCS trial. Clin. Infect. Dis. 2004, 38, 284–288. [Google Scholar] [CrossRef]
- Brindley, P.G.; Zhu, N.; Sligl, W. Best evidence in critical care medicine Early antibiotics and survival from septic shock: It’s about time. Can. J. Anesth. J. Can. D’anesthésie 2006, 53, 1157–1160. [Google Scholar] [CrossRef]
- El-Kady, S.; Petel, D.; Baird, R. Inter-rater agreement in the evaluation of abdominal radiographs for necrotizing enterocolitis. J. Pediatr. Surg. 2014, 49, 733–735. [Google Scholar] [CrossRef] [PubMed]
- Gephart, S.M.; Gordon, P.V.; Penn, A.H.; Gregory, K.E.; Swanson, J.R.; Maheshwari, A.; Sylvester, K. Changing the paradigm of defining, detecting, and diagnosing NEC: Perspectives on Bell’s stages and biomarkers for NEC. In Seminars in Pediatric Surgery; WB Saunders: Philadelphia, PA, USA, 2018; pp. 3–10. [Google Scholar]
- Al-Hamad, S.; Hackam, D.J.; Goldstein, S.D.; Huisman, T.A.G.M.; Darge, K.; Hwang, M. Contrast-enhanced ultrasound and near-infrared spectroscopy of the neonatal bowel: Novel, bedside, noninvasive, and radiation-free imaging for early detection of necrotizing enterocolitis. Am. J. Perinatol. 2018, 35, 1358–1365. [Google Scholar] [CrossRef]
- Hwang, M.; Tierradentro-García, L.O.; Dennis, R.A.; Anupindi, S.A. The role of ultrasound in necrotizing enterocolitis. Pediatric Radiology 2021, 52, 1–14. [Google Scholar] [CrossRef]
- Llanos, A.R.; Moss, M.E.; Pinzòn, M.C.; Dye, T.; Sinkin, R.A.; Kendig, J.W. Epidemiology of neonatal necrotising enterocolitis: A population-based study. Paediatr. Perinat. Epidemiol. 2002, 16, 342–349. [Google Scholar] [CrossRef]
- Pineda, L.C.; Hornik, C.P.; Seed, P.C.; Cotten, C.M.; Laughon, M.M.; Bidegain, M.; Clark, R.H.; Brian Smith, P. Association between positive urine cultures and necrotizing enterocolitis in a large cohort of hospitalized infants. Early Hum. Dev. 2015, 91, 583–586. [Google Scholar] [CrossRef]
- Ortigoza, E.B.; Cagle, J.; Brown, L.S.; Mansi, S.; Gosser, S.P.; Montgomery, A.D.; Foresman, Z.; Boren, M.L.; Pettit, P.S.; Thompson, T.D. Tachygastria in Preterm Infants: A Longitudinal Cohort Study. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Sitek, A.; Seliga-Siwecka, J.; Płotka, S.; Grzeszczyk, M.K.; Seliga, S.; Włodarczyk, K.; Bokiniec, R. Artificial intelligence in the diagnosis of necrotising enterocolitis in newborns. Pediatr. Res. 2022. [Google Scholar] [CrossRef]
- Nora, D.; Salluh, J.; Martin-Loeches, I.; Povoa, P. Biomarker-guided antibiotic therapy—Strengths and limitations. Ann. Transl. Med. 2017, 5, 208. [Google Scholar] [CrossRef] [PubMed]
- Schmit, X.; Vincent, J.L. The time course of blood C-reactive protein concentrations in relation to the response to initial antimicrobial therapy in patients with sepsis. Infection 2008, 36, 213–219. [Google Scholar] [CrossRef]
- Maheshwari, A. Role of platelets in neonatal necrotizing enterocolitis. Pediatr. Res. 2021, 89, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Ververidis, M.; Kiely, E.; Spitz, L.; Drake, D.; Eaton, S.; Pierro, A. The clinical significance of thrombocytopenia in neonates with necrotizing enterocolitis. J. Pediatr. Surg. 2001, 36, 799–803. [Google Scholar] [CrossRef]
- Kim, Y.I.; Joo, J.Y.; Jung, Y.H.; Choi, C.W.; Kim, B.I.; Yang, H.R. Differentiation of food protein-induced enterocolitis syndrome misleading to necrotizing enterocolitis. Ann. Allergy Asthma Immunol. 2022, 128, 193–198. [Google Scholar] [CrossRef]
- Murch, S.H. Cow’s-Milk Protein as a Specific Immunological Trigger of Necrotising Enterocolitis—Or Food Protein–induced Enterocolitis Syndrome in Disguise? J. Pediatr. Gastroenterol. Nutr. 2013, 56, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.; Schanler, R.J.; Kim, J.H.; Patel, A.L.; Trawöger, R.; Kiechl-Kohlendorfer, U.; Chan, G.M.; Blanco, C.L.; Abrams, S.; Cotten, C.M. An exclusively human milk-based diet is associated with a lower rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products. J. Pediatr. 2010, 156, 562–567.e561. [Google Scholar] [CrossRef]
- Cacho, N.T.; Parker, L.A.; Neu, J. Necrotizing enterocolitis and human milk feeding: A systematic review. Clin. Perinatol. 2017, 44, 49–67. [Google Scholar] [CrossRef] [PubMed]
- Lucas, A.; Cole, T.J. Breast milk and neonatal necrotising enterocolitis. Lancet 1990, 336, 1519–1523. [Google Scholar] [CrossRef] [PubMed]
- Mangalapally, N.; Patel, S.; Vlk, A.M.; Capriolo, C.; Schofield, E.E.; Davis, N.L. Outcomes of Donor Breast Milk and Prolacta Use in an Urban Level IV Neonatal Intensive Care Unit. Pediatrics 2022, 149, 289. [Google Scholar]



{kind=link}
{kind=link}
| Demographics 1 | All NEC N = 25 | Medical n = 16 | Surgical n = 9 | p-Value |
|---|---|---|---|---|
| Gestational age (wk) | 28.5 ± 4.2 | 28.9 ± 4.3 | 29.6 ± 4.1 | 0.34 |
| Birth Weight (g) | 1184 ± 787 | 1132 ± 880 | 1277 ± 625 | 0.095 |
| Sex, male | 14 (56) | 8 | 6 | 0.35 |
| Multiples | 5 (20) | 2 | 3 | 0.54 |
| Congenital anomalies | 3 (12) | 1 | 2 | 0.91 |
| Maternal Age (y) | 31 ± 7 | 31 ± 7 | 31 ± 8 | 0.92 |
| Race Black White Other Not given | 12 (48) 8 (32) 2 (8) 2 (8) | 8 5 1 1 | 4 3 1 1 | 0.44 |
| Ethnicity, Hispanic | 1 (4) | 1 | 0 | |
| Insurance Medicaid Private Other | 3 (12) 18 (72) 4 (16) | 1 12 3 | 2 6 1 | 0.46 |
| Factors at Diagnosis 1 | All NEC N = 25 | Medical n = 16 | Surgical n = 9 | p-Value |
|---|---|---|---|---|
| Delivery Type, (c/s) | 16 (65) | 11 (69) | 5 (55) | 0.51 |
| Maternal diabetes | 7 (28) | 4 (25) | 3 (33) | 0.50 |
| Maternal obesity | 8 (32) | 4 (25) | 4 (44) | 0.51 |
| Pre-eclampsia | 6 (24) | 4 (25) | 2 (22) | 0.88 |
| Covid19 | 1 (4) | 0 | 1 (11) | 0.17 |
| Chorioamnionitis | 1 (4) | 1 (6) | 0 | 0.44 |
| Maternal abx | 14 (56) | 10 (62) | 4 (44) | 0.38 |
| Antenatal Steroids Complete Partial None | 12 (48) 6 (24) 7 (28) | 5 3 1 (6) | 7 3 6 | 0.38 |
| PPROM | 7 (28) | 4 (25) | 3 (33) | 0.66 |
| IUGR | 6 (24) | 4 (25) | 2 (22) | 0.88 |
| All NEC 1 N = 25 | Medical n = 16 | Surgical n = 9 | p-Value | |
|---|---|---|---|---|
| Weight | 1420 ± 889 | 1476 ± 1017 | 1321 ± 640 | 0.60 |
| Age (d) | 24 ± 21 | 29 ± 24 | 16 ± 12 | 0.17 |
| Other Studies | ||||
| Abdominal US | 6 (24) | 4 (25) | 2 (22) | 0.8 |
| Liver US | 5 (20) | 4 (25) | 1 (11) | 0.36 |
| Lab Values | ||||
| CRP (day 0) mg/L | 2.5 ± 3.1 | 2.3 ± 2.9 | 2.9 ± 3.6 | 0.69 |
| CRP (day 1) mg/L | 5.7 ± 4.0 | 6.4 ± 4.6 | 3.7 ± 1.4 | 0.10 |
| CRP (day 2) mg/L | 6.5 ± 4.8 | 6.1 ± 4.6 | 7.2 ± 5.6 | 0.69 |
| Platelets (day 0) 109/L | 308 ± 145 | 331 ±148 | 266 ± 137 | 0.28 |
| Platelets (day 1) 109/L | 261 ± 156 | 302 ±162 | 142 ± 104 | 0.06 |
| Platelets (day 2) 109/L | 212 ± 165 | 250 ± 182 | 107 ± 40.3 | 0.07 |
| Inotropes 2 | 8 (32) | 1 (6) | 7 (78) | <0.001 |
| Intubation 3 | 16 (64) | 7 (43) | 9 (100) | 0.005 |
| AKI (by KDIGO) | 3 (12) | 1 (6) | 2 (22) | 0.23 |
| Central access | 3 (12) | 3 (19) | 0 | 0.23 |
| PDA (n = 23 ECHOs) | 3 (21) | 2 (17) | 1 (11) | 0.83 |
| Positive blood cultures | 5 (20) | 2 (13) | 3 (33) | 0.21 |
| Diet Any formula Unfortified HM Fortified HM (HMF) | 5 (20) | 4 (25) 3 (15) 9 (45) | 1(11) 0 8 (100) | 0.62 0.24 |
| Antibiotics | All NEC N = 25 | Medical n = 16 | Surgical n = 9 | p-Value |
|---|---|---|---|---|
| Time to any antibiotic 1 (min) | 151 ± 96 | 122 ± 58 | 204 ± 129 | 0.049 |
| Time to vancomycin (min) | 160 ± 93 | 131 ± 67 | 210 ± 115 | 0.032 |
| Time to piperacillin-tazobactam (min) | 143 ± 93 | 112 ± 56 | 198 ± 176 | 0.15 |
| Outcomes | All NEC n = 25 |
|---|---|
| Discharge Home | 18 (72) |
| Death | 5 (20) |
| Transferred to another facility | 2 (8) |
| NEC Totalis 1 | 3 (13) |
| Any bronchopulmonary dysplasia | 16 (64) |
| Severe bronchopulmonary dysplasia 2 | 10 (40) |
| All Radiologists (3 Raters) | Interpretation of Agreement | |
|---|---|---|
| All studies (N = 46) | 0.657 (0.585–0.730) | Substantial |
| ICC by findings | ||
| Pneumatosis | 0.454 (0.336–0.573) | Moderate |
| Portal venous gas | 0.629 (0.492–0.765) | Substantial |
| Pneumoperitoneum | 0.719 (0.589–0.879) | Substantial |
| ICC by Certainty | ||
| No NEC | 0.739 (0.642–0.843) | Substantial |
| Maybe NEC | 0.412 (0.316–0.508) | Moderate |
| Definitely NEC | 0.763 (0.666–0.859) | Substantial |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chetta, K.E.; Vincent, K.G.; Fanning, B.; Klumb, A.B.; Chetta, J.A.; Rohrer, A.M.; Spence, L.H.; Hill, J.G. Impact of Delayed Time to Antibiotics in Medical and Surgical Necrotizing Enterocolitis. Children 2023, 10, 160. https://doi.org/10.3390/children10010160
Chetta KE, Vincent KG, Fanning B, Klumb AB, Chetta JA, Rohrer AM, Spence LH, Hill JG. Impact of Delayed Time to Antibiotics in Medical and Surgical Necrotizing Enterocolitis. Children. 2023; 10(1):160. https://doi.org/10.3390/children10010160
Chicago/Turabian StyleChetta, Katherine E., Katherine G. Vincent, Bresney Fanning, Ashley B. Klumb, Justin A. Chetta, Allison M. Rohrer, Leslie H. Spence, and Jeanne G. Hill. 2023. "Impact of Delayed Time to Antibiotics in Medical and Surgical Necrotizing Enterocolitis" Children 10, no. 1: 160. https://doi.org/10.3390/children10010160
APA StyleChetta, K. E., Vincent, K. G., Fanning, B., Klumb, A. B., Chetta, J. A., Rohrer, A. M., Spence, L. H., & Hill, J. G. (2023). Impact of Delayed Time to Antibiotics in Medical and Surgical Necrotizing Enterocolitis. Children, 10(1), 160. https://doi.org/10.3390/children10010160