


Breaking Barriers to Rapid Whole Genome Sequencing in Pediatrics: Michigan’s Project Baby Deer

 ,
,  , ,
, ,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
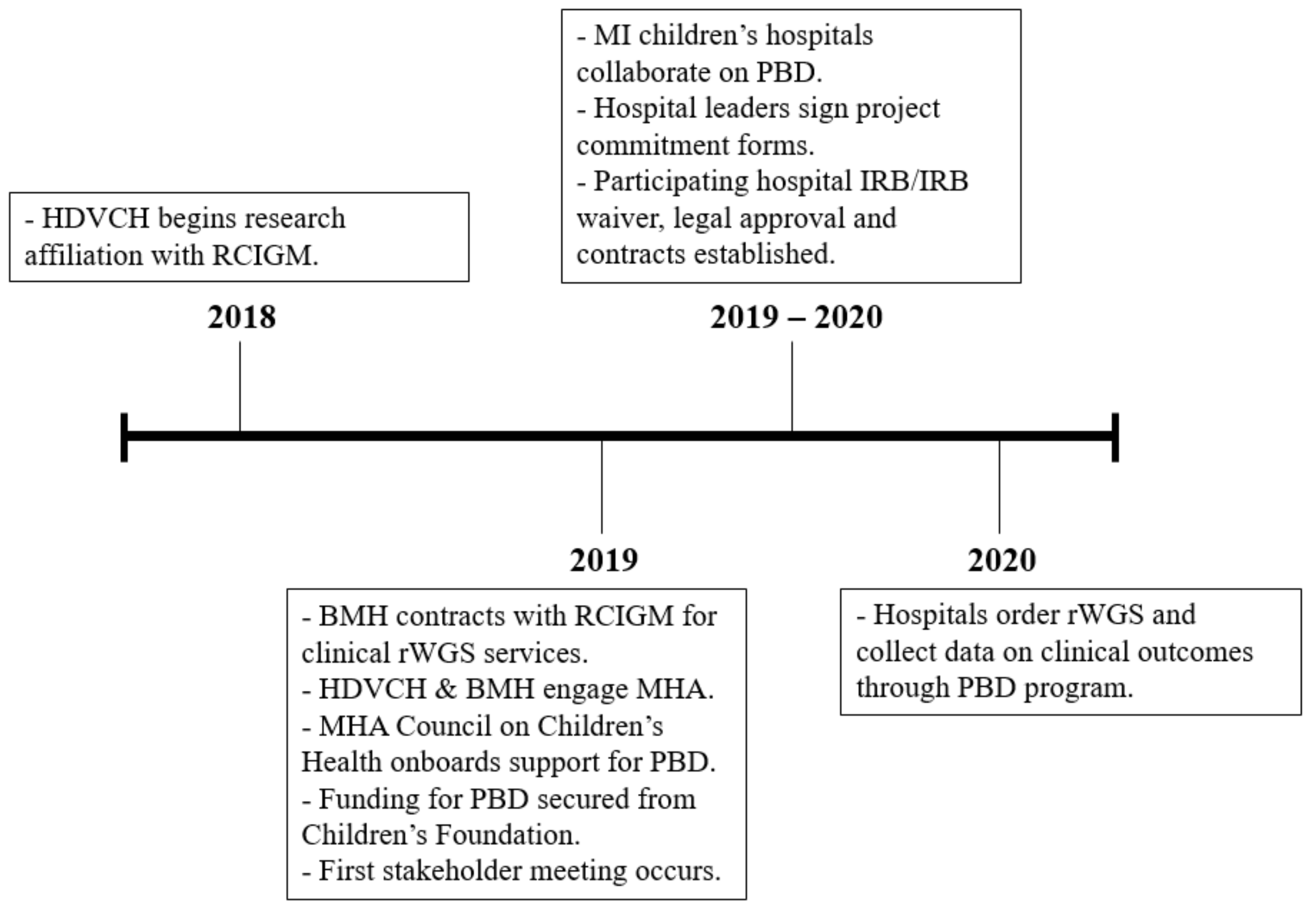
2.1. Exploration
2.2. Preparation
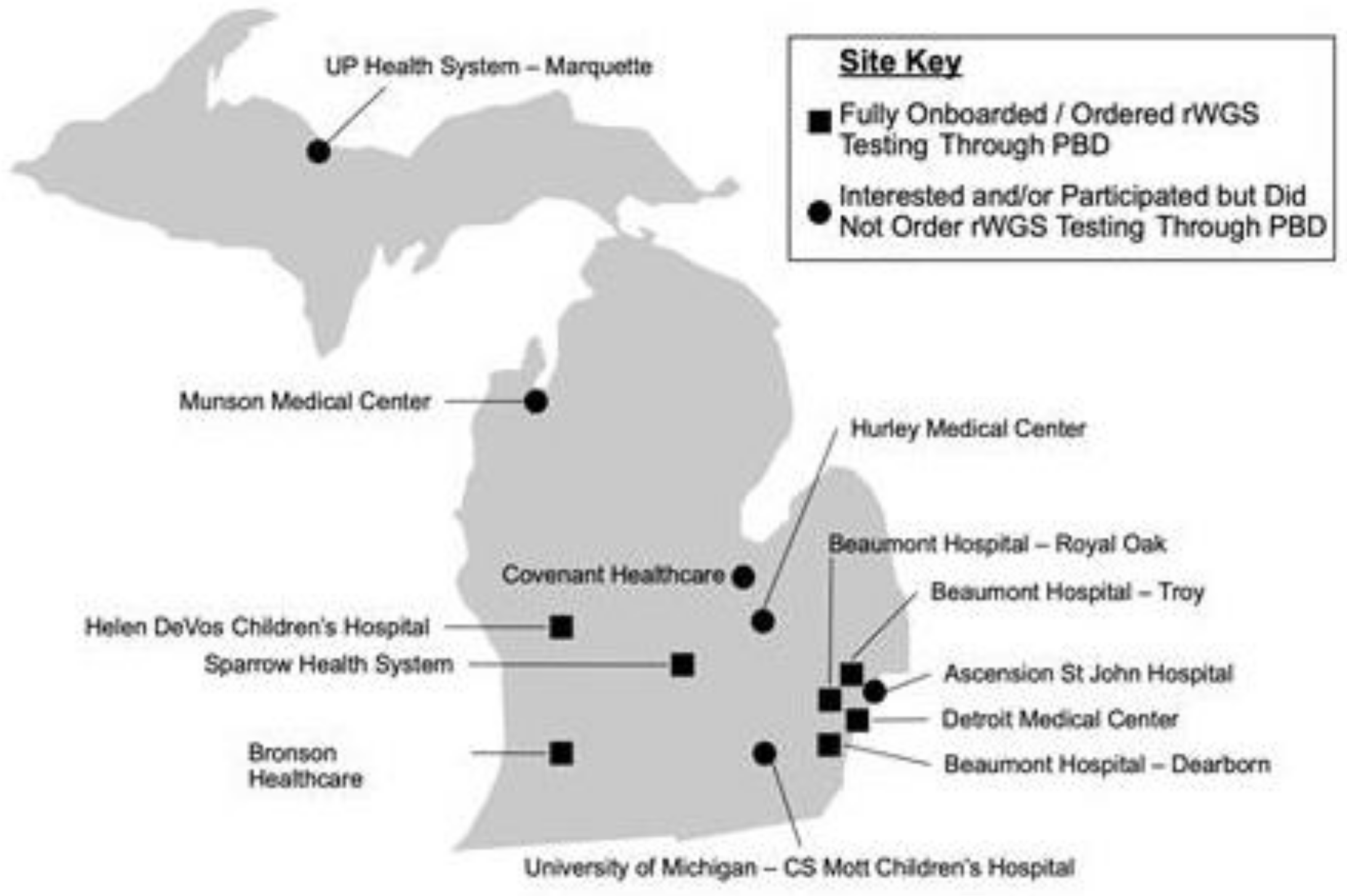
2.3. Implementation
3. Results
3.1. Clinical Impact
3.2. Economic Impact
3.3. Family Impact
3.4. Policy Impact
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lavelle, T.A.; Feng, X.; Keisler, M.; Cohen, J.T.; Neumann, P.J.; Prichard, D.; Schroeder, B.E.; Salyakina, D.; Espinal, P.S.; Weidner, S.B.; et al. Cost-effectiveness of exome and genome sequencing for children with rare and undiagnosed conditions. Genet. Med. 2022, 24, 1349–1361, Erratum in Genet Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.M.; Stark, Z.; Farnaes, L.; Tan, T.Y.; White, S.M.; Dimmock, D.; Kingsmore, S.F. Meta-analysis of the diagnostic and clinical utility of genome and exome sequencing and chromosomal microarray in children with suspected genetic diseases. NPJ Genom. Med. 2018, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- The NICUSeq Study Group; Krantz, I.D.; Medne, L.; Weatherly, J.M.; Wild, K.T.; Biswas, S.; Devkota, B.; Hartman, T.; Brunelli, L.; Fishler, K.P.; et al. Effect of whole-genome sequencing on the clinical management of acutely ill infants with suspected genetic disease: A randomized clinical trial. JAMA Pediatr. 2021, 1, 1218–1226, Erratum in JAMA Pediatr. 2021, 1, 1295. [Google Scholar] [CrossRef]
- Farnaes, L.; Hildreth, A.; Sweeney, N.M.; Clark, M.M.; Chowdhury, S.; Nahas, S.; Cakici, J.A.; Benson, W.; Kaplan, R.H.; Kronick, R.; et al. Rapid whole-genome sequencing decreases infant morbidity and cost of hospitalization. NPJ Genom. Med. 2018, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Dimmock, D.P.; Clark, M.M.; Gaughran, M.; Cakici, J.A.; Caylor, S.A.; Clarke, C.; Feddock, M.; Chowdhury, S.; Salz, L.; Cheung, C.; et al. An RCT of rapid genomic sequencing among seriously ill infants results in high clinical utility, changes in management, and low perceived harm. Am. J. Hum. Genet. 2020, 107, 942–952. [Google Scholar] [CrossRef] [PubMed]
- Kingsmore, S.F.; Cakici, J.A.; Clark, M.M.; Gaughran, M.; Feddock, M.; Batalov, S.; Bainbridge, M.N.; Carroll, J.; Caylor, S.A.; Clarke, C.; et al. A randomized, controlled trial of the analytic and diagnostic performance of singleton and trio, rapid genome and exome sequencing in ill infants. Am. J. Hum. Genet. 2019, 105, 719–733. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Kang, W.; Wang, Y.; Zhuang, D.; Chen, L.; Li, L.; Su, Y.; Pan, X.; Wei, Q.; Tang, Z.; et al. Application of full-spectrum rapid clinical genome sequencing improves diagnostic rate and clinical outcomes in critically ill infants in the China Neonatal Genomes Project. Crit. Care Med. 2021, 49, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Petrikin, J.E.; Cakici, J.A.; Clark, M.M.; Willig, L.K.; Sweeney, N.M.; Farrow, E.G.; Saunders, C.J.; Thiffault, I.; Miller, N.A.; Zellmer, L.; et al. The NSIGHT1-randomized controlled trial: Rapid whole-genome sequencing for accelerated etiologic diagnosis in critically ill infants. NPJ Genom. Med. 2018, 3, 6. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Lu, Y.; Dong, X.; Lu, G.; Cheng, G.; Qian, Y.; Ni, Q.; Zhang, P.; Yang, L.; Wu, B.; et al. Optimized trio genome sequencing (OTGS) as a first-tier genetic test in critically ill infants: Practice in China. Hum. Genet. 2020, 139, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Elliott, A.M.; du Souich, C.; Lehman, A.; Guella, I.; Evans, D.M.; Candido, T.; Tooman, L.; Armstrong, L.; Clarke, L.; Gibson, W.; et al. RAPIDOMICS: Rapid genome-wide sequencing in a neonatal intensive care unit-successes and challenges. Eur. J. Pediatr. 2019, 178, 1207–1218. [Google Scholar] [CrossRef] [PubMed]
- Franck, L.S.; Kriz, R.M.; Rego, S.; Garman, K.; Hobbs, C.; Dimmock, D. Implementing rapid whole-genome sequencing in critical care: A qualitative study of facilitators and barriers to new technology adoption. J. Pediatr. 2021, 237, 237–243.e2. [Google Scholar] [CrossRef] [PubMed]
- Dimmock, D.; Caylor, S.; Waldman, B.; Benson, W.; Ashburner, C.; Carmichael, J.L.; Carroll, J.; Cham, E.; Chowdhury, S.; Cleary, J.; et al. Project Baby Bear: Rapid precision care incorporating rWGS in 5 California children’s hospitals demonstrates improved clinical outcomes and reduced costs of care. Am. J. Hum. Genet. 2021, 108, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Rady Institute for Genomics Medicine. Genomics 101 Courses. Available online: https://radygenomics.org/education/genomics-101/ (accessed on 5 November 2022).
- Franck, L.S.; Scheurer-Monaghan, A.; Bupp, C.P.; Fakhoury, J.D.; Hoffmann, T.J.; Deshpandey, M.; Arenchild, M.; Dimmock, D.P. Healthcare professionals’ attitudes toward rapid whole genome sequencing in pediatric acute care. Children 2022, 9, 357. [Google Scholar] [CrossRef]
- Project Baby Deer. Rapid Whole Genome Sequencing. Available online: https://radygenomics.org/wp-content/uploads/2022/03/Project-Baby-Deer_UpdateandEcoSavings_Flyer.pdf (accessed on 5 November 2022).
- United States Census Bureau. Quick Facts: Michigan. Available online: https://www.census.gov/quickfacts/MI (accessed on 5 November 2022).
- Rady Children’s Hospital. Project Baby Bear Final Report. Available online: https://radygenomics.org/wp-content/uploads/2021/04/PBB-Final-Report_07.14.20.pdf (accessed on 5 November 2022).
- Michigan Department of Health and Human Services. Clinical Lab Fee Schedule. January 2022. Available online: https://www.michigan.gov/mdhhs/-/media/Project/Websites/mdhhs/Folder50/Folder7/Clinical_Lab-_012022-pdf.pdf?rev=9e1b1896ef9547f48afabebe283866b3 (accessed on 5 November 2022).
- Michigan Department of Health and Human Services. Coverage of Rapid Whole Genome Sequencing (rWGS) Testing. 17 August 2021. Available online: https://www.michigan.gov/documents/mdhhs/MSA_21-33_732848_7.pdf (accessed on 5 November 2022).
- Michigan Health and Hospital Association. About the Keystone Center. Available online: https://www.mha.org/mha-keystone-center-patient-safety-organization/about-the-mha-keystone-center/ (accessed on 5 November 2022).
- Smedley, D.; Smith, K.R.; Martin, A.; Thomas, E.A.; McDonagh, E.M.; Cipriani, V.; Ellingford, J.M.; Arno, G.; Tucci, A.; Vandrovcova, J.; et al. 100,000 Genomes pilot on rare-disease diagnosis in health care—Preliminary report. N. Engl. J. Med. 2021, 385, 1868–1880. [Google Scholar] [CrossRef] [PubMed]
- Medi-Cal Update. Inpatient Services. Bulletin 573. June 2022. Available online: https://files.medi-cal.ca.gov/pubsdoco/bulletins/artfull/ips202206.aspx (accessed on 5 November 2022).
- Minnesota Department of Human Services. Laboratory and Pathology Tests. Revised 4 April 2022. Available online: https://www.dhs.state.mn.us/main/idcplg?IdcService=GET_DYNAMIC_CONVERSION&RevisionSelectionMethod=LatestReleased&dDocName=DHS16_144353 (accessed on 5 November 2022).
- Louisiana SB 154. Provides for Health Insurance Coverage of Genetic Testing for Critically Ill Infants with No Diagnosis. (1/1/23). Available online: https://legiscan.com/LA/text/SB154/2022 (accessed on 5 November 2022).
- Maryland Department of Health. Whole Genome Sequencing (WGS) Clinical Criteria. Whole Genome Clinical Criteria. Available online: https://health.maryland.gov/mmcp/Documents/Whole%20Genome%20Clinical%20Criteria.pdf#search=Whole%20Genome%20Sequencing%20Clinical%20Criteria (accessed on 5 November 2022).
- Oregon Health Authority. Prioritized list of Health Services. 1 January 2023. Available online: https://www.oregon.gov/oha/HPA/DSI-HERC/PrioritizedList/1-1-2022PrioritizedListofHealthServices.pdf (accessed on 5 November 2022).
- Wojcik, M.H.; Fraiman., Y.S. Further considerations on the value of whole-genome sequencing in critically ill infants. JAMA Pediatr. 2022, 176, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.B.; Quittner, A.L.; Brown, M.; Li-Rosi, A.M. Understanding access to genomics in an ethnically diverse south Florida population: A comparison of demographics in odyssey and rapid whole genome sequencing programs. J. Genet. Couns. 2020, 29, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Chad, L.; Anderson, J.; Cagliero, D.; Hayeems, R.Z.; Ly, L.G.; Szuto, A. Rapid genetic testing in pediatric and neonatal critical care: A scoping review of emerging ethical issues. Hosp. Pediatr. 2022, 12, e347–e359. [Google Scholar] [CrossRef] [PubMed]
- Cakici, J.A.; Dimmock, D.P.; Caylor, S.A.; Gaughran, M.; Clarke, C.; Triplett, C.; Clark, M.M.; Kingsmore, S.F.; Bloss, C.S. A prospective study of parental perceptions of rapid whole-genome and -exome sequencing among seriously ill infants. Am. J. Hum. Genet. 2020, 107, 953–962. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
Inclusion Criteria:
|
| Exclusion Criteria: Patients whose clinical course is entirely explained by:
|
| Minimum genome-wide sequencing standards: Given the data on the effects of turnaround time on economic impact and the clear yield of several specific tests, genomic sequencing could be sent to any laboratory that offered a complete test of all coding and non-coding sequences of clinically relevant genes, high resolution copy number (to single exon) for all OMIM morbid genes, mitochondrial (mt)DNA coverage, SMN1/2 copy number analysis and a consistent mean and median turnaround time of less than 3 days. |
| Onboarded Sites. | Site Type | Genetics on Site | NICU/PICU Admissions per Year (Estimated) | Date of Initial rWGS Test Sent |
|---|---|---|---|---|
| Beaumont Hospital- Dearborn | Community | No | NICU-759 No PICU | January 2021 |
| Beaumont Hospital- Royal Oak | Community/Hybrid | No | NICU-1311 PICU-610 | December 2020 |
| Beaumont Hospital- Troy | Community | No | NICU-572 No PICU | June 2021 |
| Bronson Methodist Hospital | Community/Hybrid | No | NICU-600 PICU-700 | August 2020 |
| Detroit Medical Center/ Hutzel Women’s Hospital | Free standing children’s hospital | Yes | NICU-1200 PICU-2100 | May 2020 |
| Helen DeVos Children’s Hospital | Free standing children’s hospital | Yes | NICU-1600 PICU-1319 | November 2020 |
| Sparrow Health System | Community/Hybrid | Yes | NICU-800 PICU-455 | November 2020 |
| Pilot Site | Children Who Received rWGS | Children Diagnosed (Diagnostic Rate) | Children Whose Care Changed (Change in Management Rate) |
|---|---|---|---|
| Beaumont Health, Dearborn | 3 | 2 (67%) | 2 (67%) |
| Beaumont Health, Royal Oak | 6 | 0 (0%) | 0 (0%) |
| Beaumont Health, Troy | 1 | 1 (100%) | 0 (0%) |
| Bronson Methodist Hospital | 15 | 6 (40%) | 7 (47%) |
| Children’s Hospital of Michigan | 10 | 4 (40%) | 1 (10%) |
| Helen DeVos Children’s Hospital | 45 | 18 (40%) | 11 (25%) |
| Sparrow Hospital | 9 | 4 (44%) | 3 (33%) |
| Totals | 89 | 35 (39%) | 24 (27%) |
| Total Cases in Cohort | 89 |
| Total Genomes Sequenced (proband + comparator) | 140 |
| Average Cost per Case * | $7563.86 |
| Change in Management Surveys Completed | 64 |
| Midpoint of Estimated Range of Avoided Days | 154.5 |
| Avg Savings Per Avoided Inpatient Day | $4854.47 |
| Gross Savings (n = 64) | $750,015.32 |
| Net Savings (n = 64) | $265,928.53 |
| Net Savings Per Patient | $4155.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bupp, C.P.; Ames, E.G.; Arenchild, M.K.; Caylor, S.; Dimmock, D.P.; Fakhoury, J.D.; Karna, P.; Lehman, A.; Meghea, C.I.; Misra, V.; et al. Breaking Barriers to Rapid Whole Genome Sequencing in Pediatrics: Michigan’s Project Baby Deer. Children 2023, 10, 106. https://doi.org/10.3390/children10010106
Bupp CP, Ames EG, Arenchild MK, Caylor S, Dimmock DP, Fakhoury JD, Karna P, Lehman A, Meghea CI, Misra V, et al. Breaking Barriers to Rapid Whole Genome Sequencing in Pediatrics: Michigan’s Project Baby Deer. Children. 2023; 10(1):106. https://doi.org/10.3390/children10010106
Chicago/Turabian StyleBupp, Caleb P., Elizabeth G. Ames, Madison K. Arenchild, Sara Caylor, David P. Dimmock, Joseph D. Fakhoury, Padmani Karna, April Lehman, Cristian I. Meghea, Vinod Misra, and et al. 2023. "Breaking Barriers to Rapid Whole Genome Sequencing in Pediatrics: Michigan’s Project Baby Deer" Children 10, no. 1: 106. https://doi.org/10.3390/children10010106
APA StyleBupp, C. P., Ames, E. G., Arenchild, M. K., Caylor, S., Dimmock, D. P., Fakhoury, J. D., Karna, P., Lehman, A., Meghea, C. I., Misra, V., Nolan, D. A., O’Shea, J., Sharangpani, A., Franck, L. S., & Scheurer-Monaghan, A. (2023). Breaking Barriers to Rapid Whole Genome Sequencing in Pediatrics: Michigan’s Project Baby Deer. Children, 10(1), 106. https://doi.org/10.3390/children10010106