
Effects of Epoxyeicosatrienoic Acid-Enhancing Therapy on the Course of Congestive Heart Failure in Angiotensin II-Dependent Rat Hypertension: From mRNA Analysis towards Functional In Vivo Evaluation

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Heart Failure Model, Exclusion Criteria
2.3. Detailed Experimental Design
2.3.1. Series 1: Assessment of Kidney mRNA Expression in the Early Phase of ACF-Induced HF
- Sham-operated HanSD rats
- Sham-operated TGR
- ACF TGR
2.3.2. Series 2: Assessment of RAS, SNS and CYP Metabolites and Enzymes in the Early Phase of ACF-Induced HF
2.3.3. Series 3 and 6: Effects of Treatment with EET-A or ACEi, Alone or Combined, on the Survival Rate and Albuminuria, and Effects of 20-Weeks’ Treatment on Basal Cardiac Function Assessed by Echocardiography and by Pressure-Volume Analysis
- Sham-operated HanSD rats (initial n = 20)
- Sham-operated TGR (initial n = 21)
- ACF TGR + water (i.e., untreated) (initial n = 32)
- ACF TGR + EET-A (initial n = 32)
- ACF TGR + ACEi (initial n = 32)
- ACF TGR + EET-A + ACEi (initial n = 33)
2.3.4. Series 4: Effects of 2-Weeks’ Treatment with EET-A and ACEi, Alone or Combined, on Basal Cardiac Function Assessed by Echocardiography and by Pressure-Volume Analyses
- Sham-operated HanSD rats
- Sham-operated TGR
- ACF TGR + water
- ACF TGR + EET-A
- ACF TGR + ACEi
- ACF TGR + EET-A + ACEi
2.3.5. Series 5: Effects of 2-Weeks’ Treatment with EET-A and ACEi, Alone or Combined, on Renal Hemodynamics and Excretory Function
- Sham-operated HanSD rats
- Sham-operated TGR
- ACF TGR + water
- ACF TGR + EET-A
- ACF TGR + ACEi
- ACF TGR + EET-A + ACEi
2.4. Statement of Ethics
2.5. Statistical Analysis
3. Results
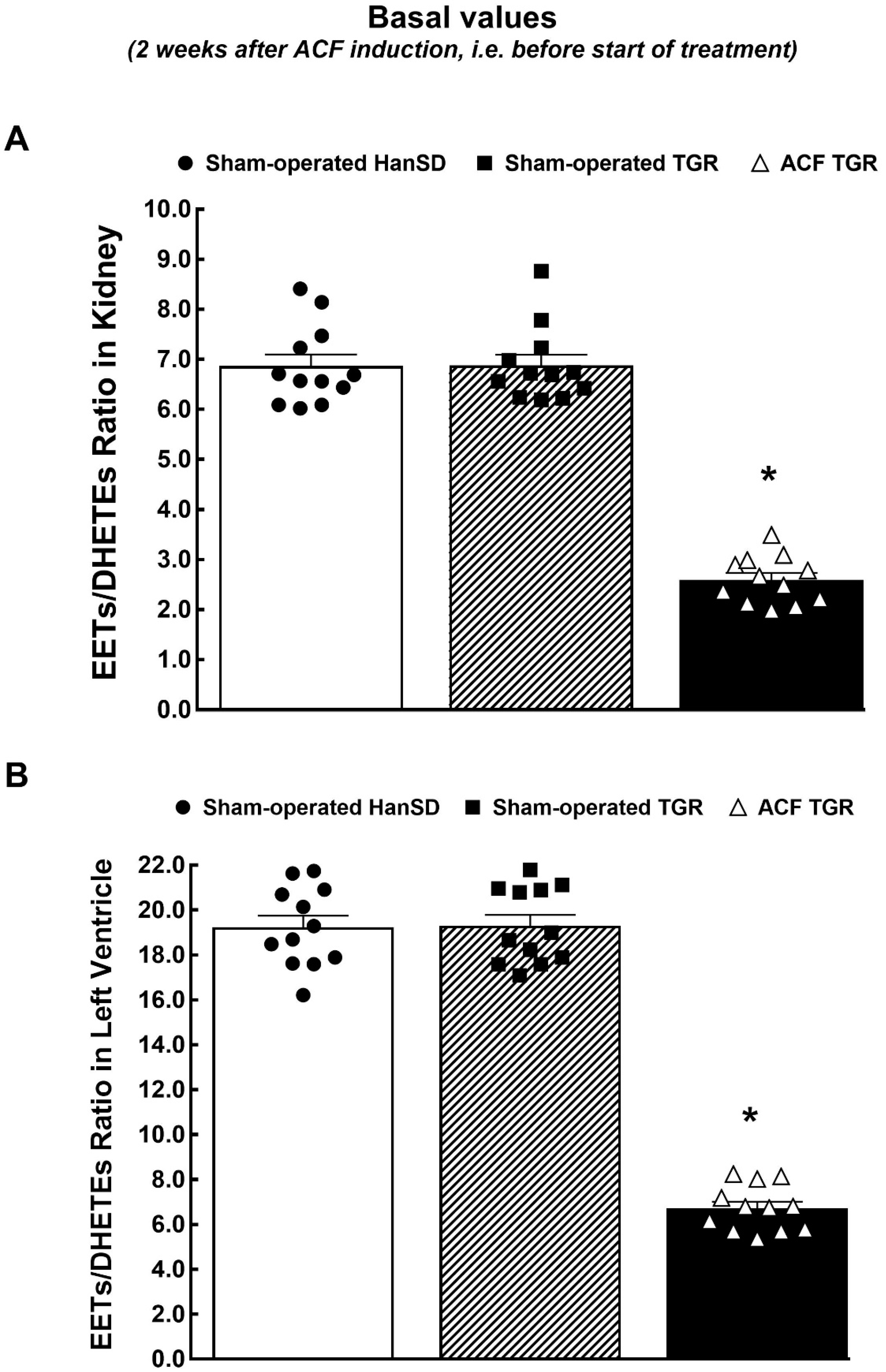
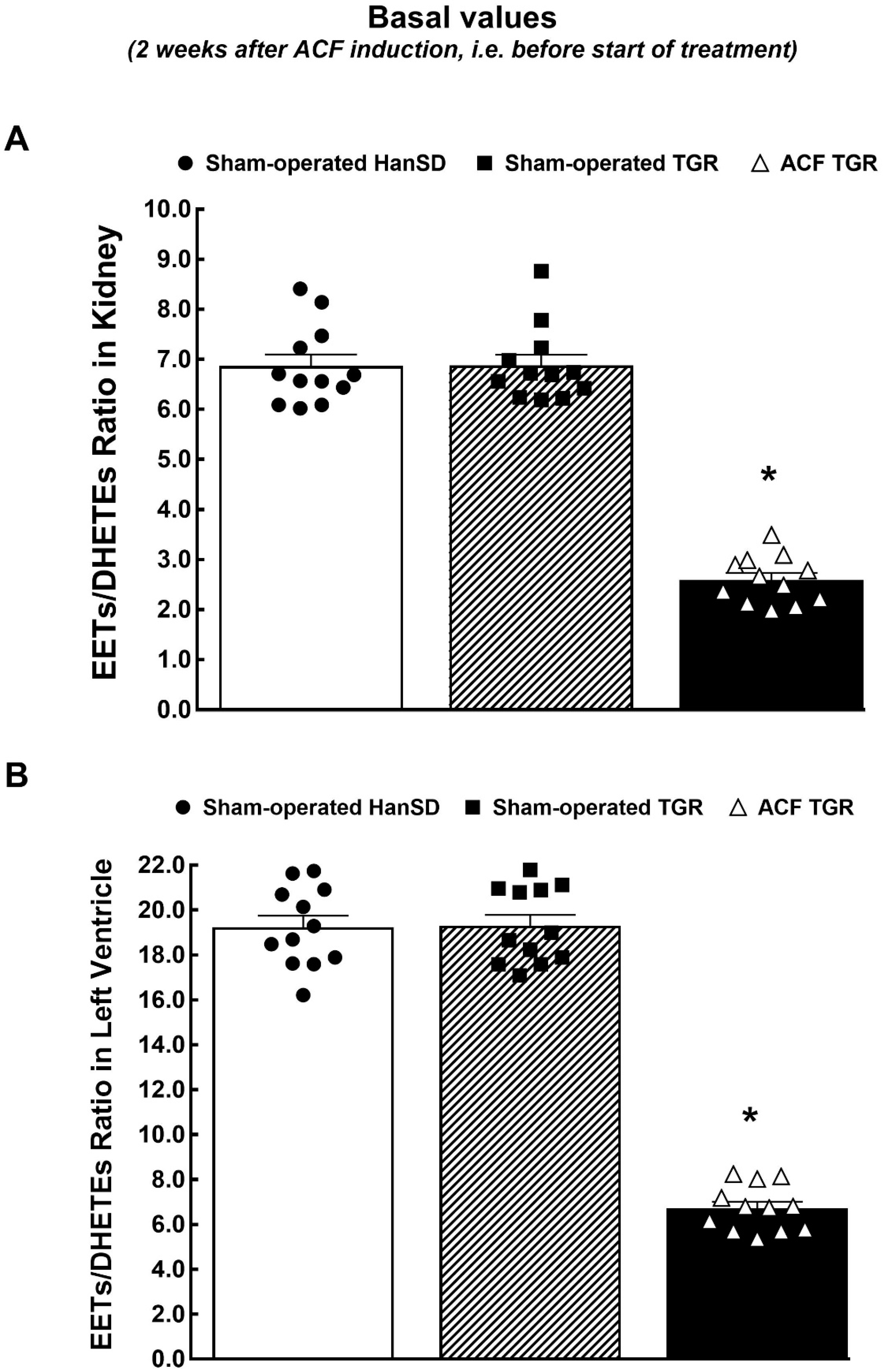
3.1. Series 1 and 2: Assessment of Kidney mRNA Expression and RAS, SNS and CYP Active Agents, Metabolites and Enzymes in the Early Phase of ACF-Induced HF in the Early Phase of ACF-Induced HF
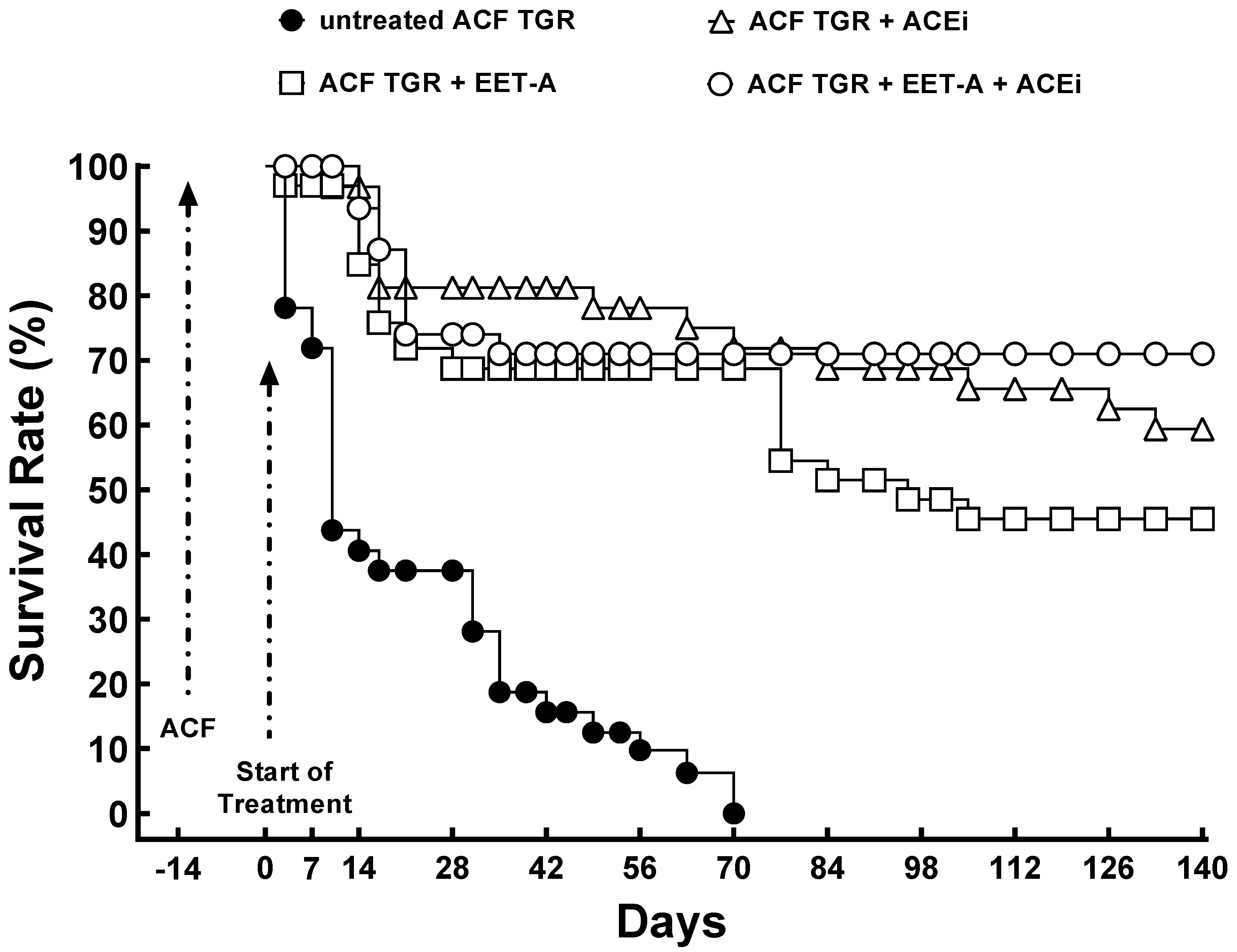
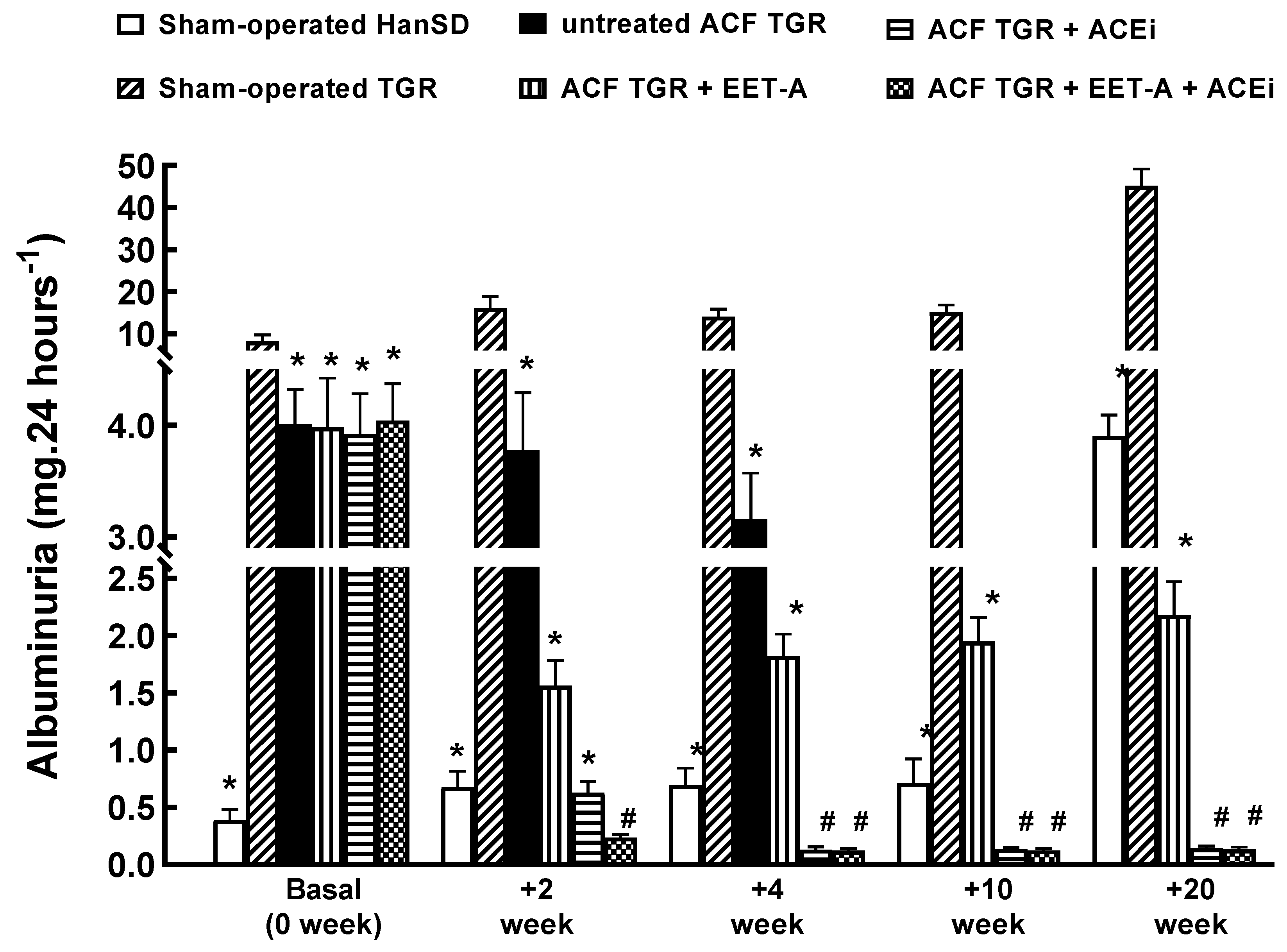
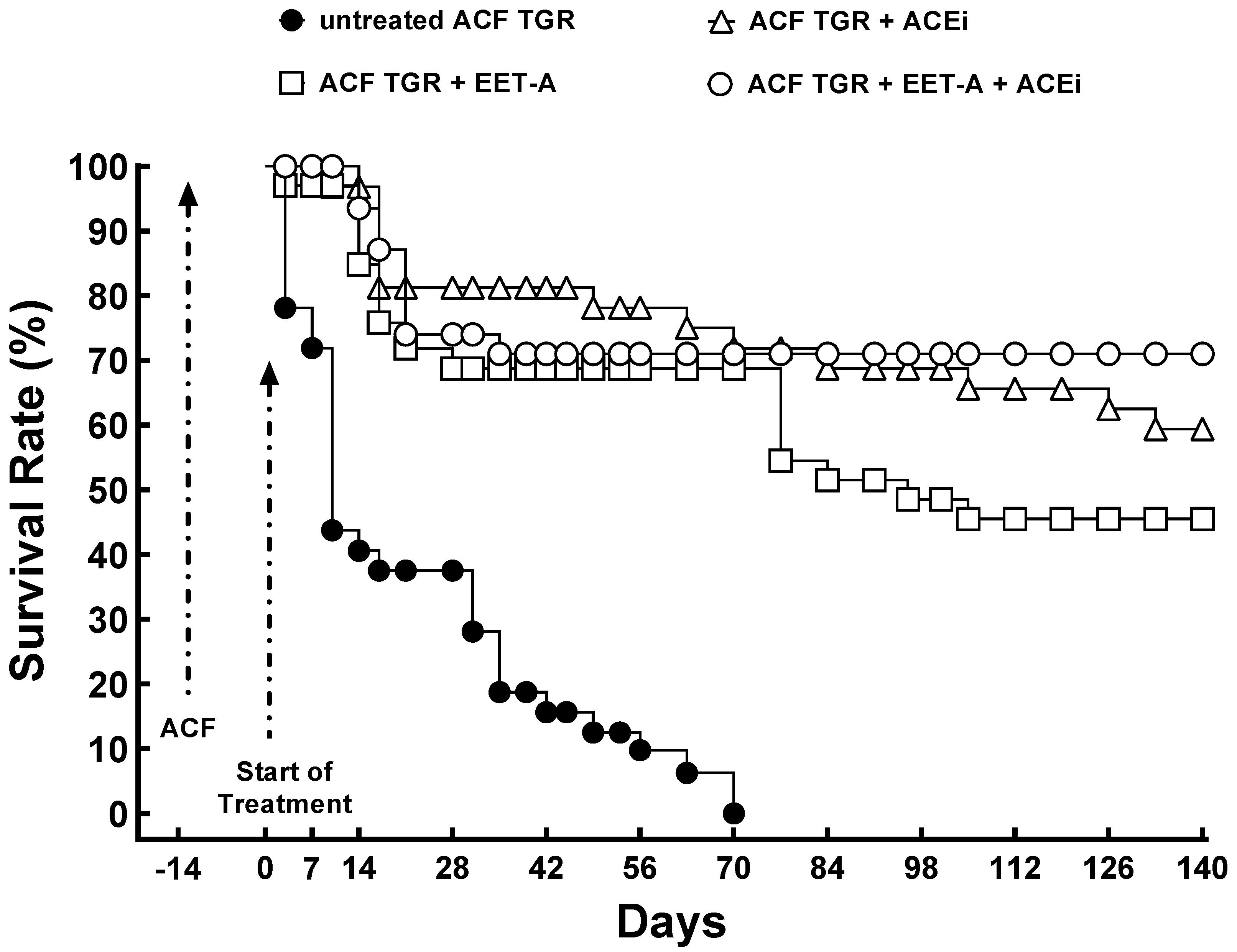
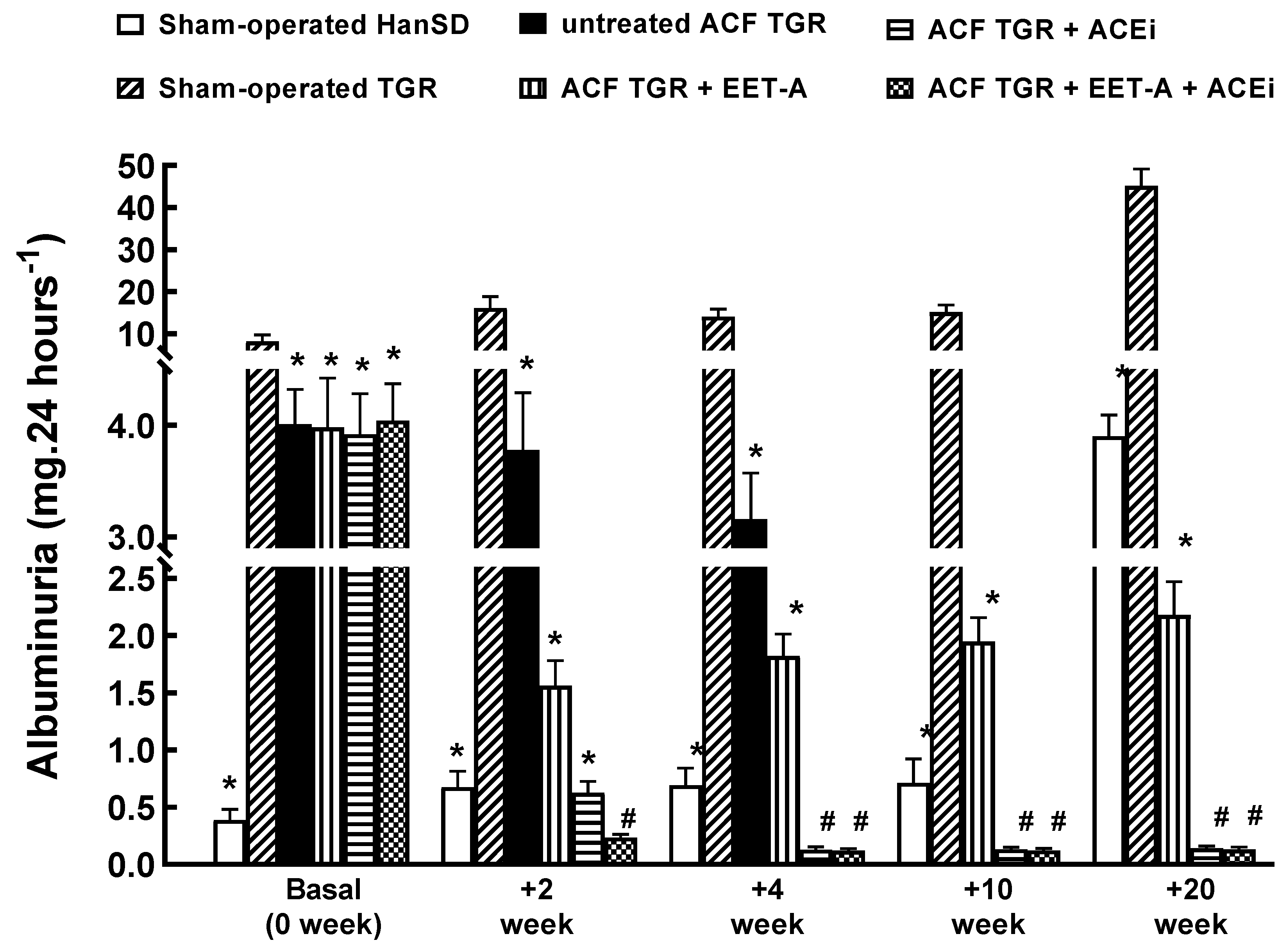
3.2. Series 3: Effects of Single Treatment with EET-A or ACEi or with a Combination Thereof on the Survival Rate and Albuminuria
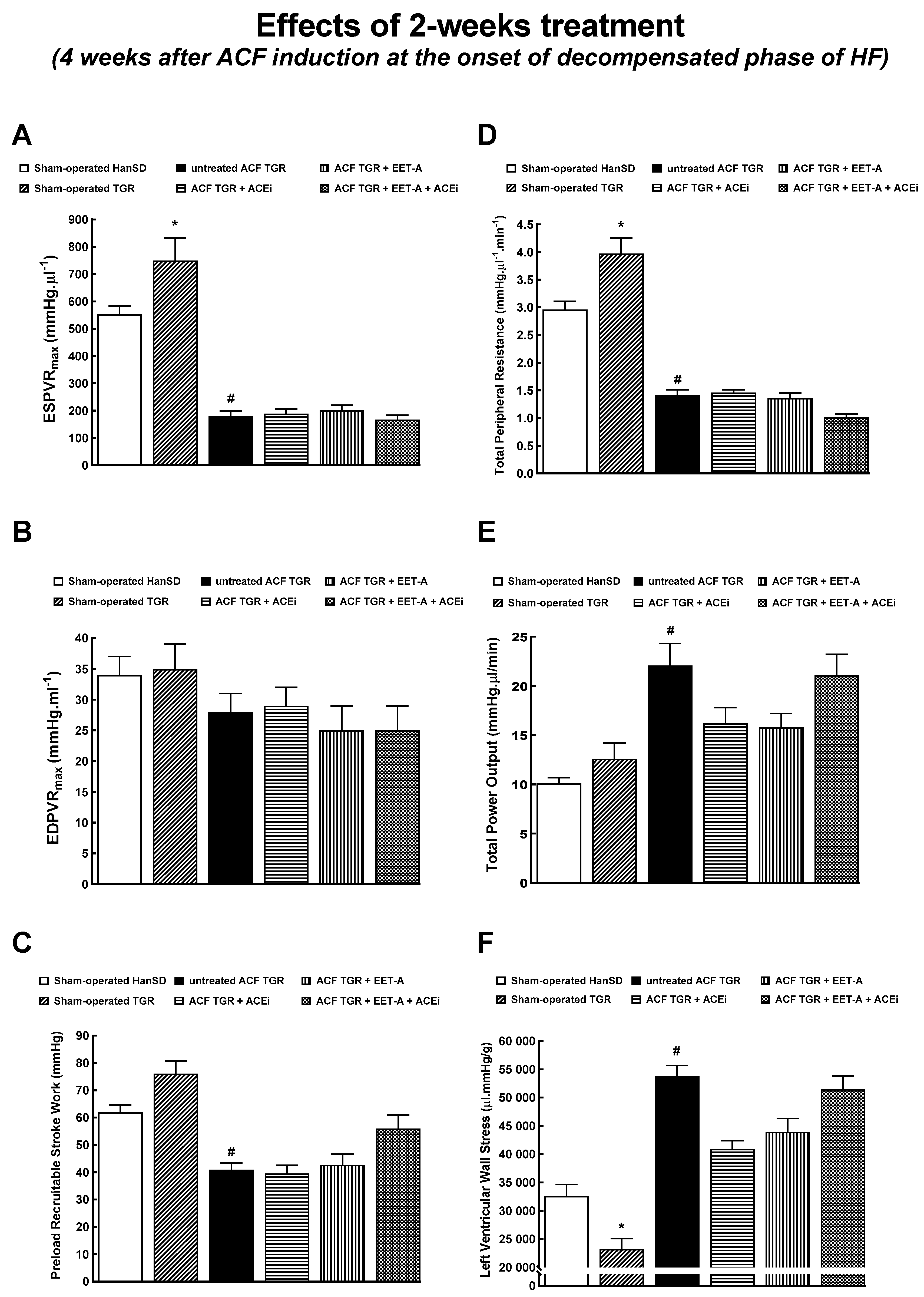
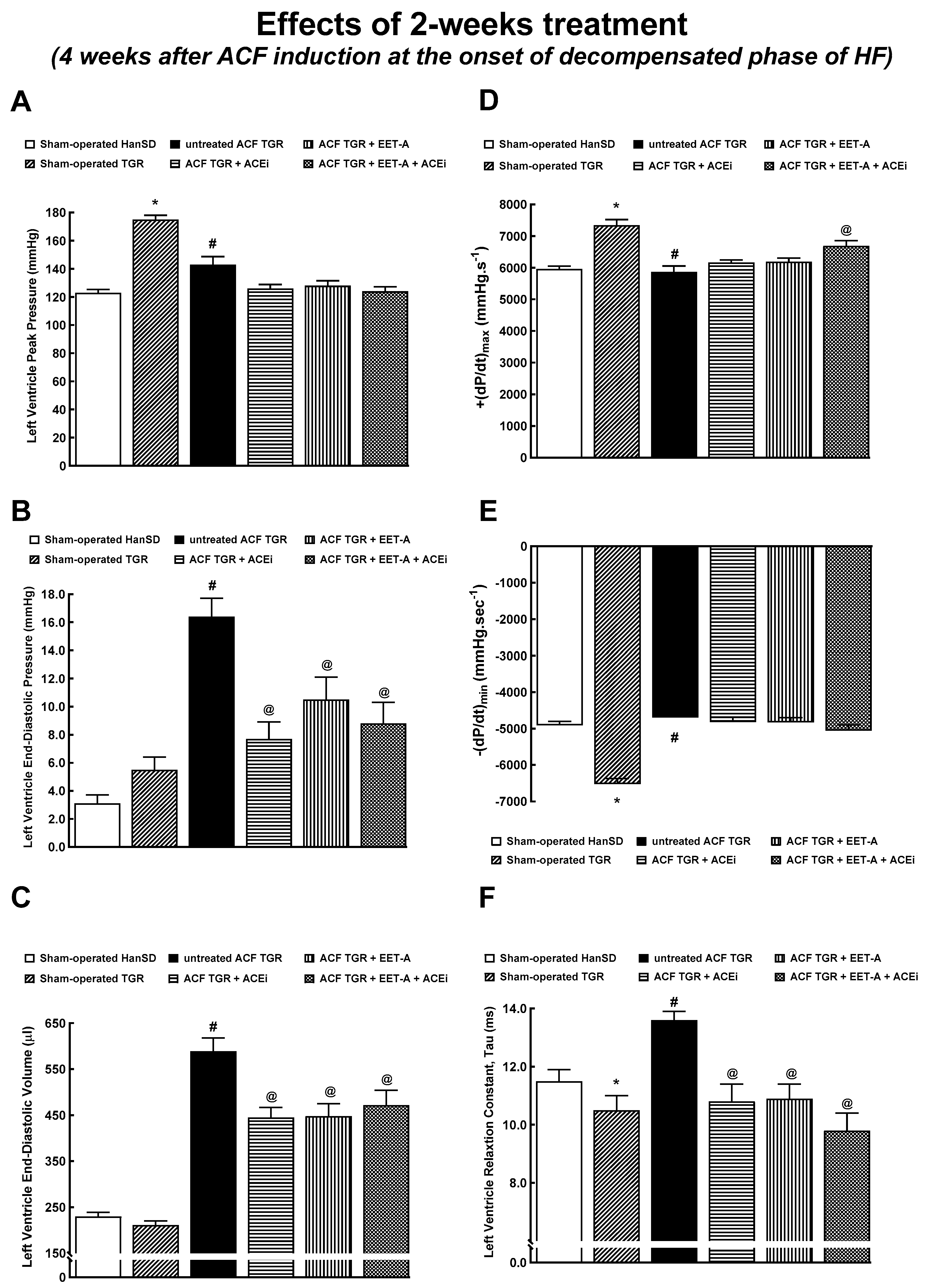
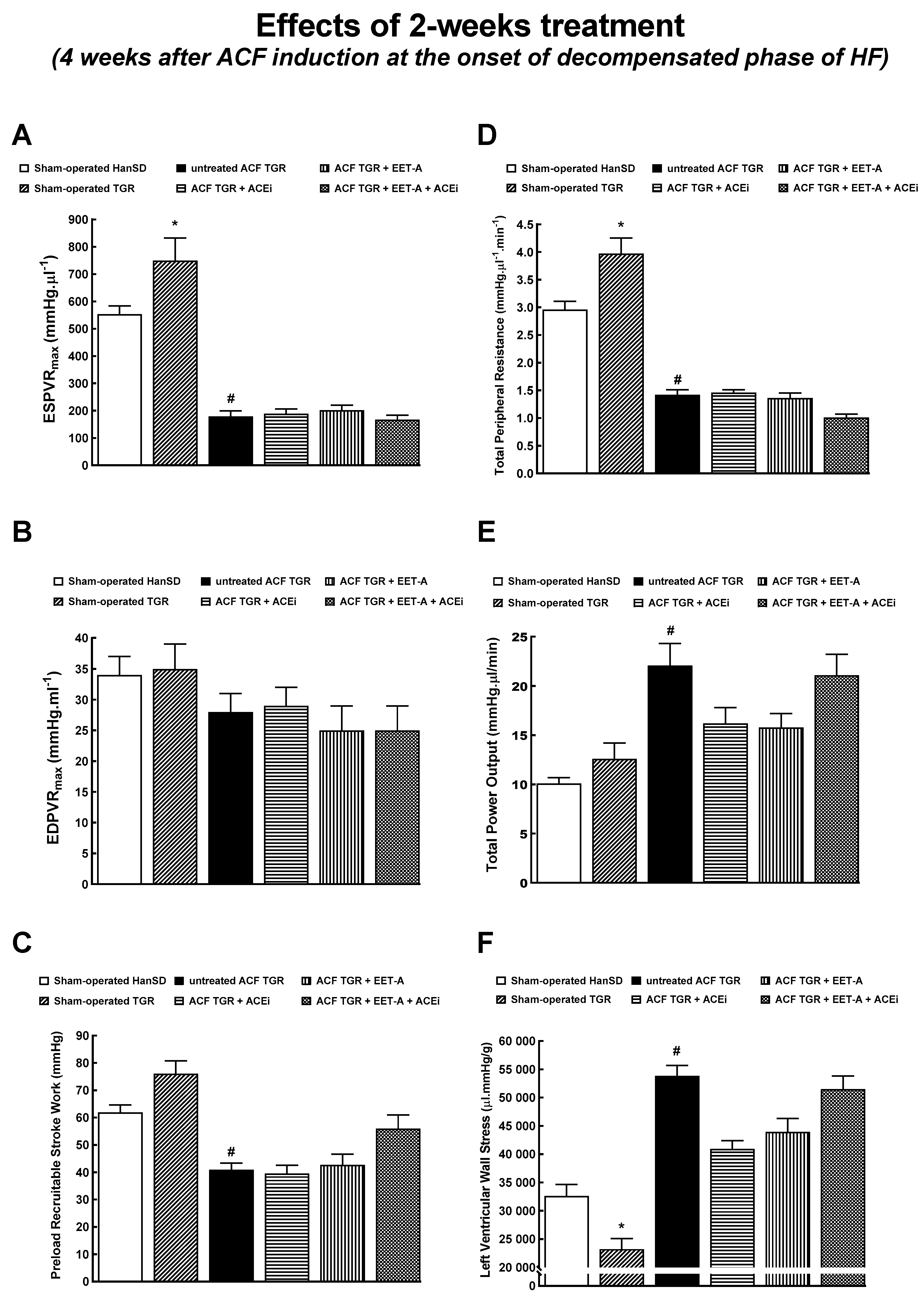
3.3. Series 4: Effects of 2-Weeks’ Treatment with EET-A or ACEi, Alone or Combined, on Basal Cardiac Function Assessed by Echocardiography and by Pressure-Volume Analysis
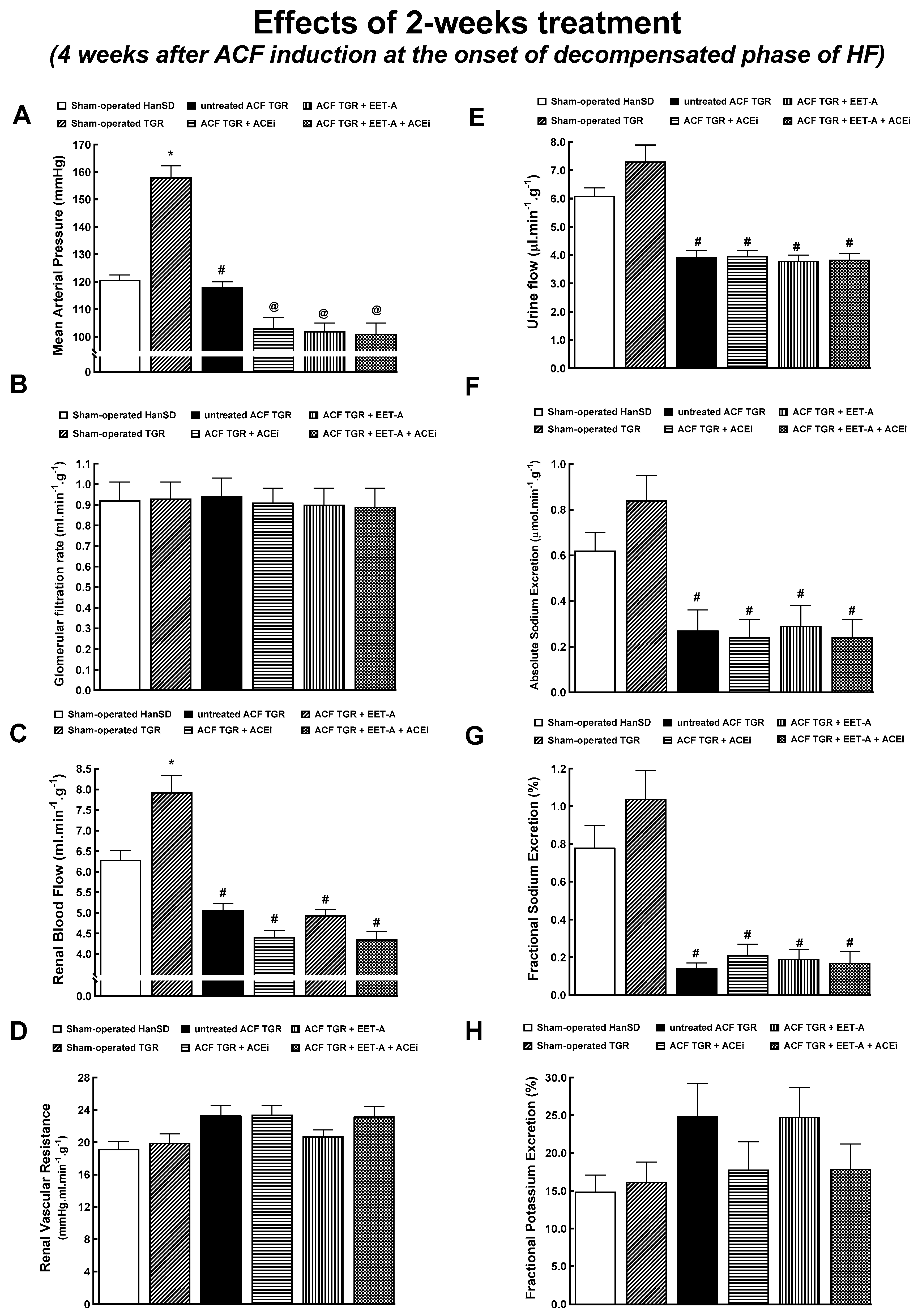
3.4. Series 5: Effects of 2-Weeks’ Treatment with EET-A or ACEi, Alone or Combined, on Renal Hemodynamics and Excretory Function
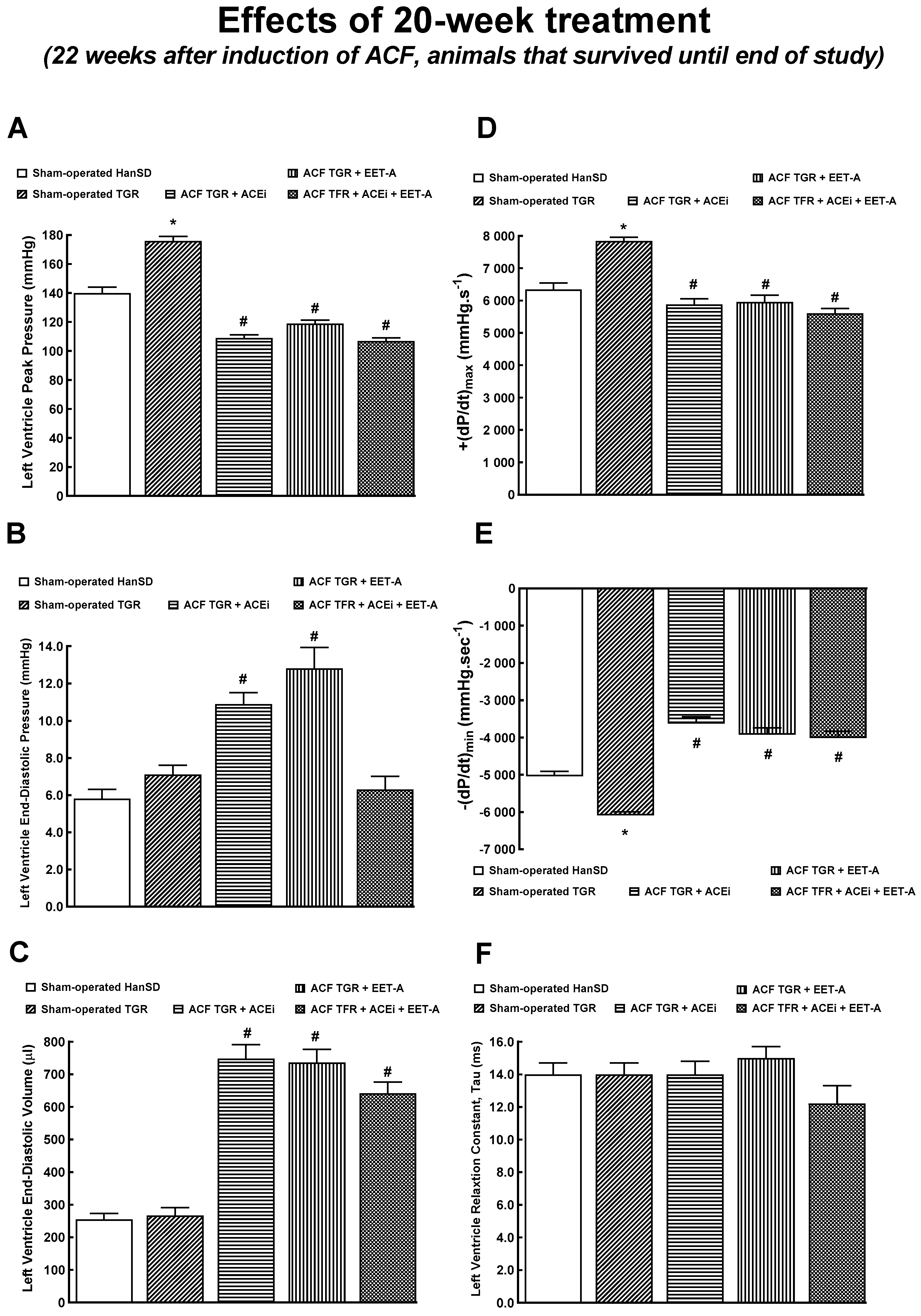
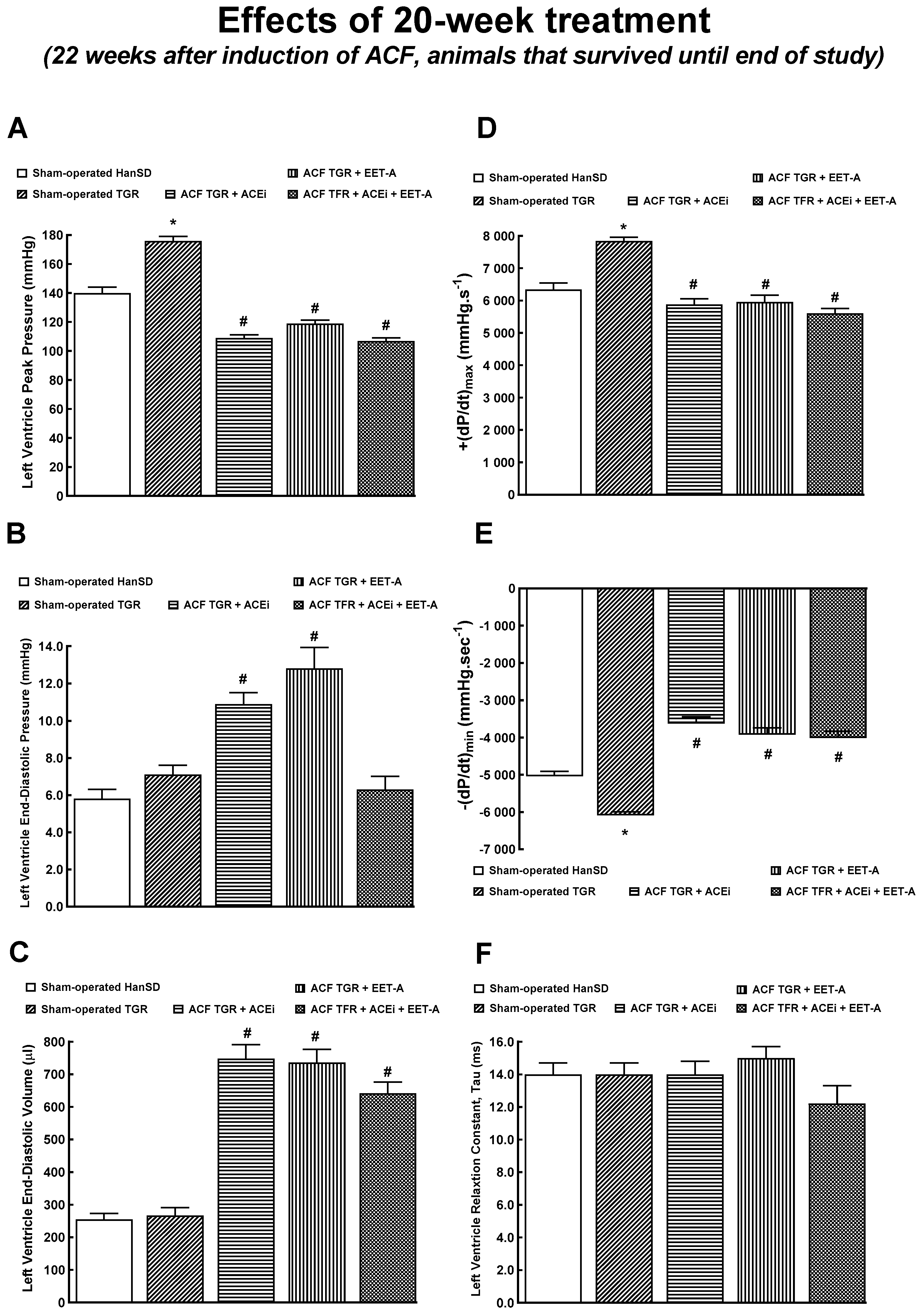
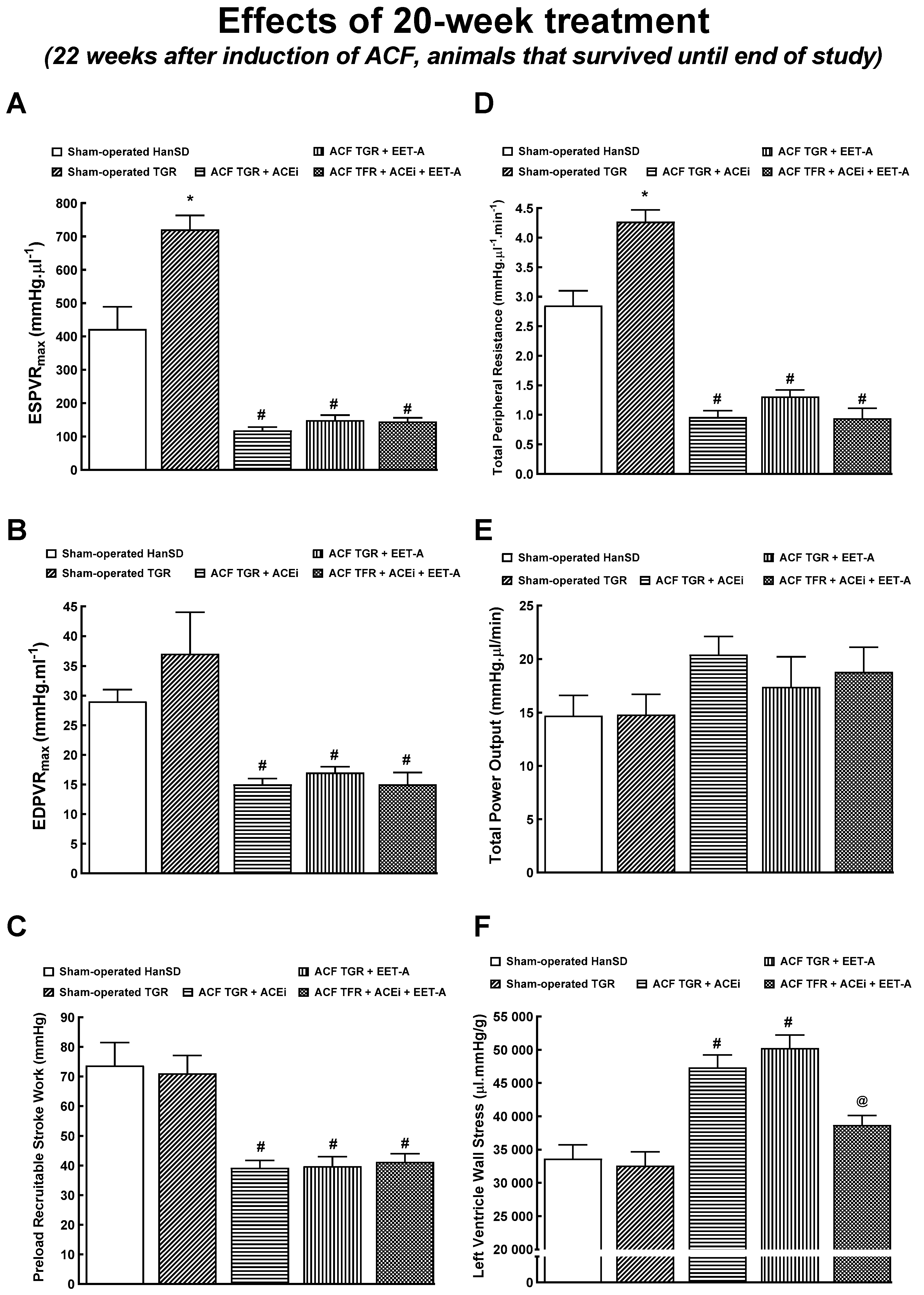
3.5. Series 6: Effects of 20-Weeks’ Treatment with EET-A or ACEi, Alone or Combined, on Basal Cardiac Function Assessed by Echocardiography and by Pressure-Volume Analyses
4. Discussion
4.1. Activity of the Neurohormonal Systems in ACF-Induced Heart Failure
4.2. Effects of the Treatment Regimens on the Survival Rate
4.3. Mechanisms of the Beneficial Actions of the Treatments
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AA | arachidonic acid |
| ACE | angiotensin-converting enzyme |
| ACEi | angiotensin-converting enzyme inhibitor |
| ACE2 | angiotensin-converting enzyme type 2 |
| ACF | aorto-caval fistula |
| ANG II | angiotensin II |
| ANG 1-7 | angiotensin 1-7 |
| AT1A | angiotensin II type 1 receptor subtype A |
| AT2 | angiotensin II type 2 receptor |
| CKD | chronic kidney disease |
| CYP | cytochrome P-450 enzyme |
| CYP2C23 | cytochrome P-450 enzyme subfamily 2C23 |
| CYP4A1 | cytochrome P-450 enzyme subfamily 4A1 |
| (+dP/dt)max | maximum rates of pressure rise |
| (−dP/dt)max | maximum rates of pressure fall |
| DHETEs | dihydroxyeicosatrienoic acids |
| EET-A | 14,15-epoxyeicosatrienoic acid analog |
| EETs | epoxyeicosatrienoic acids |
| EDPVR | end-diastolic pressure-volume relationship |
| ESPVR | end-systolic pressure-volume relationship |
| FHH | fawn-hooded hypertensive rats |
| FHL | fawn-hooded low-pressure rats |
| GFR | glomerular filtration rate |
| HanSD | normotensive, transgene-negative, Hannover Sprague-Dawley rats |
| HF | heart failure |
| IKEM | Institute for Clinical and Experimental Medicine |
| LV | left ventricle |
| MAP | mean arterial pressure |
| mRNA | messenger ribonucleic acid |
| NE | norepinephrine |
| PRSW | preload recruitable stroke work |
| RAS | renin-angiotensin system |
| RBF | renal blood flow |
| RDN | renal denervation |
| RSNA | renal sympathetic nerve activity |
| RV | right ventricle |
| sEH | soluble epoxide hydrolase |
| SHR | spontaneously hypertensive rats |
| TGR | Ren2 renin transgenic, hypertensive rats |
| TPR | total peripheral resistance |
| 20-HETE | 20-hydroxyeicosatrienoic acid |
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanaatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart disease and stroke statistics—2017 update: A report from the American heart association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Hein, A.; Scialla, J.; Edmonston, D.; Cooper, L.B.; DeVore, A.D.; Mentz, R.J. Medical management of heart failure with reduced ejection fraction in patients with advanced renal disease. JACC Heart Fail. 2019, 7, 371–382. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.S.; Cunningham, J.W.; Ferreira, J.P.; Zannad, F.; Packer, M.; Fonarow, G.C.; McMurray, J.J.V.; Solomon, S.D. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: A comparative analysis of three randomised controlled trials. Lancet 2020, 396, 121–128. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckman, M.; et al. EMPEROR reduced trial investigators cardiovascular and renal outcomes with empagli-flozin in heart failure. N. Eng. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.P.; Ibrahim, N.E.; Januzzi, J.J. Heart failure with reduced ejection fraction. JAMA 2020, 324, 488–504. [Google Scholar] [CrossRef] [PubMed]
- Imig, J.D. Epoxyeicosanoids in Hypertension. Physiol. Res. 2019, 68, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Elmarakby, A.A. Reno-protective mechanisms of epoxyeicosatrienoic acids in cardiovascular disease. Am. J. Physiol. Integr. Comp. Physiol. 2012, 302, R321–R330. [Google Scholar] [CrossRef] [Green Version]
- Fan, F.; Roman, R.J. Effect of cytochrome P450 metabolites of arachidonic acid in nephrology. J. Am. Soc. Nephrol. 2017, 28, 2845–2855. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, K.L.; Endo, T.; Darwesh, A.M.; Samokhvalov, V.; Seubert, J.M. Cytochrome P450-derived eicosanoids and heart function. Pharmacol. Ther. 2017, 179, 47–83. [Google Scholar] [CrossRef] [PubMed]
- Sporková, A.; Reddy, R.M.; Falck, J.R.; Imig, J.D.; Kopkan, L.; Sadowski, J.; Červenka, L. Interlobular arteries from 2-kidney, 1-clip Goldblatt hypertensive ras´ exhibit-impaired vasodilatory response to epoxyeicosatrienoic acids. Am. J. Med. Sci. 2016, 351, 513–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangawwami, J.; Bhalla, V.; Blair, J.E.A.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezeu, K.; Molitch, M.; Mullens, W.; et al. Cardiorenal syndrome: Classification, pathophysiology, diagnosis, and treatment strategies. Circulation 2019, 139, e840–e878. [Google Scholar]
- Messerli, F.H.; Rimoldi, S.F.; Bangalore, S. The transition from hypertension to heart failure. JACC Heart Fail. 2017, 5, 543–551. [Google Scholar] [CrossRef]
- Dube, P.; Weber, K.T. Congestive heart failure: Pathophysiologic consequences of neurohormonal activation and the potential for recovery: Part I. Am. J. Med. Sci. 2011, 342, 348–351. [Google Scholar] [CrossRef]
- Packer, M. The neurohormonal hypothesis: A theory to explain the mechanism of disease progression in heart failure. J. Am. Coll. Cardiol. 1992, 20, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Pavo, N.; Prausmüller, S.; Spinka, G.; Goliasch, G.; Bartko, P.E.; Wurm, R.; Arfsten, H.; Strunk, G.; Poglitsch, M.; Domenig, O.; et al. Myocardial angiotensin metabolism in end-stage heart failure. J. Am. Coll. Cardiol. 2021, 77, 1731–1743. [Google Scholar] [CrossRef]
- Fleming, I. The pharmacology of the cytochrome P450 epoxygenase/soluble epoxide hydrolase axis in the vasculature and cardiovascular disease. Pharmacol. Rev. 2014, 66, 1106–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.H.; Schwartzman, M.L.; Roman, R.J. Altered renal P-450 metabolism of arachidonic acid in Dahl salt-sensitive rats. Am. J. Physiol. Integr. Comp. Physiol. 1994, 267, R579–R589. [Google Scholar] [CrossRef]
- Kaergel, E.; Muller, D.N.; Honeck, H.; Theuer, J.; Shagdarsuren, E.; Mullally, A.; Luft, F.; Schunck, W.-H. P450-dependent arachidonic acid metabolism and angiotensin II–induced renal damage. Hypertens 2002, 40, 273–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falck, J.R.; Kodela, R.; Manne, R.; Atcha, R.; Puli, N.; Dubasi, N. 14,15-Epoxyeicosa-5,8,11-trienoic acid (14,15-EET) surro-gates containing epoxide bioisosteres: Influence upon vascular relaxation and soluble epoxide hydrolase inhibition. J. Med. Chem. 2009, 52, 5069–5075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imig, J.D.; Elmarakby, A.; Nithipatikom, K.; Wei, S.; Capdevila, J.H.; Tuniki, V.R.; Sangras, B.; Anjaiah, S.; Manthati, V.L.; Reddy, D.S.; et al. Development of epoxyeicosatrienoic acid analogs with in vivo anti-hypertensive actions. Front. Physiol. 2010, 1, 157. [Google Scholar] [CrossRef] [Green Version]
- Hrdlička, J.; Neckář, J.; Papoušek, F.; Husková, Z.; Kikerlová, S.; Vaňourková, Z.; Vernerová, Z.; Akat, F.; Vašinová, J.; Hammock, B.D.; et al. Epoxyeicosatrienoic acid-based therapy attenuates the progression of postischemic heart failure in normotensive sprague-dawley but not in hypertensive Ren-2 transgenic Rats. Front. Pharmacol. 2019, 10, 159. [Google Scholar] [CrossRef] [Green Version]
- Neckář, J.; Khan, M.A.H.; Gross, G.J.; Cyprová, M.; Hrdlička, J.; Kvasilová, A.; Falck, J.R.; Campbell, W.B.; Sedláková, L.; Škutová, Š.; et al. Epoxyeicosatrienoic acid analog EET-B at-tenuates post-myocardial infarction remodeling in spontaneously hypertensive rats. Clin. Sci. 2019, 133, 939–951. [Google Scholar] [CrossRef]
- Imig, J.D.; Khan, M.A.H.; Burkhan, A.; Chen, G.; Adebesin, A.M.; Falck, J.R. Kidney-targeting epoxyeicosatrienoic acid ana-log, EET-F01, reduces inflammation, oxidative stress, and cisplatin-induced nephrotoxicity. Int. J. Mol. Sci. 2021, 22, 2793. [Google Scholar] [CrossRef] [PubMed]
- Walkowska, A.; Červenka, L.; Imig, J.D.; Falck, J.R.; Sadowski, J.; Kompanowska-Jezierska, E. Early Renal Vasodilator and Hypotensive Action of Epoxyeicosatrienoic Acid Analog (EET-A) and 20-HETE Receptor Blocker (AAA) in Spontaneously Hypertensive Rats. Front. Physiol. 2021, 12. [Google Scholar] [CrossRef]
- Garcia, R.; Diebold, S. Simple, rapid, and effective method of producing aorto-caval shunts in the rat. Cardiovasc. Res. 1990, 24, 430–432. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Segev, R.; Francis, B.; Abu-Saleh, N.; Awad, H.; Lazarovich, A.; Kabala, A.; Aronson, D.; Abassi, Z. Cardiac and renal distribution of ACE and ACE-2 in rats with heart failure. Acta Histochem. 2014, 116, 1342–1349. [Google Scholar] [CrossRef] [PubMed]
- Abassi, Z.; Goltsman, I.; Karram, T.; Winaver, J.; Hoffman, A. Aortocaval Fistula in Rat: A Unique Model of Volume-Overload Congestive Heart Failure and Cardiac Hypertrophy. J. Biomed. Biotechnol. 2011, 2011, 729497. [Google Scholar] [CrossRef] [Green Version]
- Brower, G.; Levick, S.; Janicki, J.S. Differential Effects of Prevention and Reversal Treatment with Lisinopril on Left Ventricular Remodelling in a Rat Model of Heart Failure. Hear. Lung Circ. 2015, 24, 919–924. [Google Scholar] [CrossRef] [Green Version]
- Kala, P.; Sedláková, L.; Škaroupková, P.; Kopkan, L.; Vaňourková, Z.; Táborský, M.; Nishiyama, A.; Hwang, S.H.; Hammock, B.D.; Sadowski, J.; et al. Effect of Angiotensin-Converting Enzyme Blockade, Alone or Combined With Blockade of Soluble Epoxide Hydrolase, on the Course of Congestive Heart Failure and Occurrence of Renal Dysfunction in Ren-2 Transgenic Hypertensive Rats With Aorto-Caval Fistula. Physiol. Res. 2017, 67, 401–415. [Google Scholar] [CrossRef]
- Honetschlagerová, Z.; Gawrys, O.; Jíchová, Š.; Škaroupková, P.; Kikerlová, S.; Vaňourková, Z.; Husková, Z.; Melenovský, V.; Kom-panowska-Jezierska, E.; Sadowski, J.; et al. Renal sympathetic denervation at-tenuates congestive heart failure in angiotensin II-dependent hypertension: Studies with Ren-2 transgenic hypertensive rats with aorto-caval fistula. Kidney Blood Press. Res. 2021, 46, 95–113. [Google Scholar] [PubMed]
- Honetschlagerová, Z.; Škaroupková, P.; Kikerlová, S.; Husková, Z.; Maxová, H.; Melenovský, V.; Kompanowska-Jezierska, E.; Sadowski, J.; Gawrys, O.; Kujal, P.; et al. Effects of renal sympathetic denervation on the course of congestive heart failure combined with chronic kidney disease: Insight from studies with fawn-hooded hypertensive rats with volume overload induced using aorto-caval fistula. Clin. Exp. Hypertens. 2021, 43, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Houser, S.R.; Margulies, K.B.; Murphy, A.M.; Spinale, F.G.; Francis, G.S.; Prabhu, S.D. Animal models of heart failure: A sci-entific statement from the American Heart Association. Circ. Res. 2012, 111, 131–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riehle, C.; Bauersachs, J. Small animal models of heart failure. Cardiovasc. Res. 2019, 115, 1838–1849. [Google Scholar] [CrossRef] [PubMed]
- Mullins, J.J.; Peters, J.F.; Ganten, D. Fulminant hypertension in transgenic rats harbouring the mouse Ren-2 gene. Nat. Cell Biol. 1990, 344, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Husková, Z.; Kramer, H.J.; Vaňourková, Z.; Červenka, L. Effects of changes in sodium balance on plasma and kidney angio-tensin II levels in anesthetized and conscious Ren-2 transgenic rats. J. Hypertens. 2006, 24, 517–527. [Google Scholar] [CrossRef]
- Červenka, L.; Melenovský, V.; Husková, Z.; Škaroupková, P.; Nishiyama, A.; Sadowski, J. Inhibition of soluble epoxide hydrolase counteracts the development of renal dysfunction and progression of congestive heart failure in Ren-2 transgenic hyperten-sive rats with aorto-caval fistula. Clin. Exp. Pharmacol. Physiol. 2015, 42, 795–807. [Google Scholar] [CrossRef]
- Jíchová, Š.; Kopkan, L.; Husková, Z.; Doleželová, Š.; Neckář, J.; Kujal, P.; Verenerová, Z.; Kramer, H.J.; Sadowski, J.; Kom-panowska-Jezierska, E.; et al. Epoxyeicosatrienoic acid analog attenuates the develop-ment of malignant hypertension, but does not reverse it once established: A study in Cyp1a1-Ren-2 transgenic rats. J. Hypertens. 2016, 34, 2008–2025. [Google Scholar] [CrossRef] [Green Version]
- Červenka, L.; Husková, Z.; Kopkan, L.; Kikerlová, S.; Sedláková, L.; Vaňourková, Z.; Alánová, P.; Kolář, F.; Hammock, B.D.; Hwang, S.H.; et al. Two pharmacological epoxyeicosatrienoic ac-id-enhancing therapies are effectively antihypertensive and reduce the severity of ischemic arrhythmias in rats with angio-tensin II-dependent hypertension. J. Hypertens. 2018, 3, 1326–1341. [Google Scholar] [CrossRef]
- Gawrys, O.; Husková, Z.; Baranowska, I.; Walkowska, A.; Sadowski Kikerlová, S.; Vaňourková, Z.; Honetschlagerová, Z.; Ška-roupková, P.; Červenka, L.; Falck, J.; et al. Combined treatment with epoxyeicosatrienoic acid an-alog and 20-hydroxyeicosatetraenoic acid antagonist provides substantial hypotensive effect in spontaneously hypertensive rats. J. Hypertens. 2020, 38, 1802–1810. [Google Scholar] [CrossRef]
- Kala, P.; Červenka, L.; Škaroupková, P.; Táborský, M.; Kompanowska-Jezierska, E.; Sadowski, J. Sex-linked differences in the mor-tality in Ren-2 transgenic hypertensive rats with aorto-caval fistula: Effects of treatment with angiotensin-converting enzyme alone and combined with inhibitor of soluble epoxide hydrolase. Physiol. Res. 2019, 68, 589–601. [Google Scholar] [CrossRef] [PubMed]
- Hillege, H.L.; Girbes, A.R.; de Kam, P.J.; Boomsma, F.; de Zeeuw, D.; Charlesworth, A.; Hampton, J.R.; van Veldhuisen, D.J. Renal func-tion, neurohormonal activation, and survival in patients with chronic heart failure. Circulation 2000, 102, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Schefold, J.C.; Filippatos, G.; Hasenfuss, G.; Anker, S.D.; von Haehling, S. Heart failure and kidney dysfunction: Epidemiolo-gy, mechanisms and management. Nat. Rev. Cardiol. 2016, 12, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Khayyat-Kholghi, M.; Oparil, S.; Davis, B.R.; Tereshchenko, L.G. Worsening kidney function is the major mechanism of heart fail-ure in hypertension. The ALLHAT study. JACC Heart Fail. 2021, 9, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Antoine, S.; Vaidya, G.; Imam, H.; Villarreal, D. Pathophysiologic Mechanisms in Heart Failure: Role of the Sympathetic Nervous System. Am. J. Med. Sci. 2017, 353, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Sharp, T.E., III; Lefer, D.J. Renal denervation to treat heart failure. Annu. Rev. Physiol. 2021, 83, 4.1–4.20. [Google Scholar] [CrossRef]
- Roman, R.J.; Fan, F. 20-HETE. Hypertension and beyond. Hypertension 2018, 72, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Alsaad, A.M.S.; Zordoky, B.; Tse, M.M.Y.; El-Kadi, A.O.S. Role of cytochrome P450–mediated arachidonic acid metabolites in the pathogenesis of cardiac hypertrophy. Drug Metab. Rev. 2013, 45, 173–195. [Google Scholar] [CrossRef] [PubMed]
- Rocic, P.; Schwartzman, M.L. 20-HETE in the regulation of vascular and cardiac function. Pharmacol. Ther. 2018, 192, 74–87. [Google Scholar] [CrossRef]
- El-Sherbeni, A.A.; Aboutabl, M.E.; Zordoky, B.N.M.; Anwa-Mohamed, A.; El-Kadi, A.O.S. Determination of the dominant arachidonic acid cytochrome P450 monooxygenase in rat heart, lung, kidney and liver: Protein expression and metabolic kinetics. AAPS J. 2013, 15, 112–122. [Google Scholar] [CrossRef] [Green Version]
- Kratky, V.; Vanourkova, Z.; Sykora, M.; Bacova, B.S.; Hruskova, Z.; Kikerlova, S.; Huskova, Z.; Kopkan, L. AT1 receptor blocker, but not an ACE inhibitor, prevents kidneys from hypoperfusion during congestive heart failure in normotensive and hypertensive rats. Sci. Rep. 2021, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quanti-tative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 41, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Bas, A.; Forsberg, G.; Hammarstrom, S.; Hammarstrom, M.L. Utility of the housekeeping genes 18S rRNA, beta-actin and glycer-aldehyde-3-phosphate-dehydrogenase for normalization in real-time quantitative reverse transcriptase-polymerase chain re-action analysis of gene expression in human T lymphocytes. Scand. J. Immunol. 2004, 59, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Jíchová, Š.; Doleželová, Š.; Kopkan, L.; Kompanowska-Jezierska, E.; Sadowski, J.; Červenka, L. Fenofibrate Attenuates Malignant Hypertension by Suppression of the Renin-angiotensin System: A Study in Cyp1a1-Ren-2 Transgenic Rats. Am. J. Med. Sci. 2016, 352, 618–630. [Google Scholar] [CrossRef] [PubMed]
- Husková, Z.; Kramer, H.J.; Thumová, M.; Vaňourková, Z.; Bürgelová, M.; Teplan, V.; Malý, J.; Červenka, L. Effects of anaesthesia on plasma and kidney ANG II levels in normotensive and ANG II-dependent hypertensive rats. Kidney Blood Res. 2006, 29, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Husková, Z.; Kopkan, L.; Červenková, L.; Doleželová, Š.; Vaňourková, Z.; Škaroupková, P.; Nishiyama, A.; Kompanowska-Jezierska, E.; Sadowski, J.; Kramer, H.J.; et al. Intrarenal alterations of the angiotensin-converting enzyme type 2/angiotensin 1-7 complex of the renin-angiotensin system do not alter the course of malignant hypertension in Cyp1a1-Ren-2 transgenic rats. Clin. Exp. Pharmacol. Physiol. 2016, 43, 438–449. [Google Scholar] [CrossRef]
- Kala, P.; Bartušková, H.; Piťha, J.; Vaňourková, Z.; Kikerlová, S.; Jíchová, Š.; Melenovský, V.; Hošková, L.; Veselka, J.; Kom-panowska-Jezierska, E.; et al. Deleterious effects of hyperactivity of the ren-in-angiotensin system and hypertension on the course of chemotherapy-induced heart failure after doxorubicin administra-tion: A study in Ren-2 transgenic rats. Int. J. Mol. Sci. 2020, 2, 9337. [Google Scholar] [CrossRef]
- Cohen, J. (Ed.) Some issue in power analysis. In Statistical Power Analysis for Bevavioral Sciences, 2nd ed.; Routledge: Oxford, UK, 2013; pp. 531–542. [Google Scholar]
- Červenka, L.; Melenovský, V.; Husková, Z.; Sporková, A.; Burgelová, M.; Škaroupková, P.; Hwang, S.H.; Hammock, B.D.; Imig, J.D.; Sadowski, J. Inhibition of soluble epoxide hydrolase does not improve the course of congestive heart failure and the develop-ment of renal dysfunction in rats with volume overload induced by aorto-caval fistula. Physiol. Res. 2015, 64, 857–873. [Google Scholar] [CrossRef]
- Kratky, V.; Kopkan, L.; Kikerlova, S.; Huskova, Z.; Taborsky, M.; Sadowski, J.; Kolar, F.; Cervenka, L. The role of renal vascular reac-tivity in the development of renal dysfunction in compensated and decompensated congestive heart failure. Kidney Blood Press. Res. 2018, 43, 1730–1741. [Google Scholar] [CrossRef]
- Yin, F.C.P.; Spurgeon, H.A.; Rakusan, K.; Weisfeldt, M.L.; Lakatta, E.G. Use of tibia length to quantify cardiac hypertrophy: Application in the aging rat. Am. J. Physiol. 1982, 243, H941–H947. [Google Scholar]
- Vaňourková, Z.; Kramer, H.J.; Husková, Z.; Vaněčková, I.; Opočenský, M.; Čertíková Chábová, V.; Tesař, V.; Škaroupková, P.; Thu-mová, M.; Dohnalová, M.; et al. AT1 receptor blockade is superiod to convetional triple therapy in protecting against end-organ damage in Cyp1a1-Ren-2 transgenic rats with inducible hypertension. J. Hypertens. 2006, 24, 2465–2472. [Google Scholar] [CrossRef]
- Hartupee, J.; Mann, D.L. Neurohormonal activation in heart failure with reduced ejection fraction. Nat. Rev. Cardiol. 2017, 14, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; McMurray, J.J. Importance of endogenous compensatory vasoactive peptides in broadening the effects of inhibi-tors of the renin-angiotensin system for the treatment of heart failure. Lancet 2017, 389, 1831–1840. [Google Scholar] [CrossRef]
- Díaz, H.S.; Toledo, C.; Andrade, D.C.; Marcus, N.J.; Del Rio, R. Neuroinflammation in heart failure: New insights for an old disease. J. Physiol. 2019, 598, 33–59. [Google Scholar] [CrossRef]
- Wang, K.; Basu, R.; Poglitsch, M.; Bakal, J.A.; Stat, P.; Oudit, G.Y. Elevated angiotensin 1-7/angiotensin II ratio predicts fa-vorable outcomes in patients with heart failure. Circ. Heart Fail. 2020, 13, e006939. [Google Scholar] [CrossRef] [PubMed]
- Vacková, Š.; Kikerlová, S.; Melenovsky, V.; Kolar, F.; Imig, J.; Kompanowska-Jezierska, E.; Sadowski, J.; Červenka, L. Altered Renal Vascular Responsiveness to Vasoactive Agents in Rats with Angiotensin II-Dependent Hypertension and Congestive Heart Failure. Kidney Blood Press. Res. 2019, 44, 792–809. [Google Scholar] [CrossRef]
- Melenovsky, V.; Skaroupkova, P.; Benes, J.; Torresova, V.; Kopkan, L.; Cervenka, L. The Course of Heart Failure Development and Mortality in Rats with Volume Overload due to Aorto-Caval Fistula. Kidney Blood Press. Res. 2012, 35, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Oka, T.; Nishimura, H.; Ueyama, M.; Kubota, J.; Kawamura, K. Haemodynamic and neurohormonal changes in spontane-ously hypertensive rats with aorto-caval fistula. Clin. Sci. 1993, 84, 531–535. [Google Scholar] [CrossRef]
- Lee, M.A.; Bohm, M.; Paul, M.; Bader, M.; Ganten, U.; Ganten, D. Physiological characterization of the hypertensive trans-genic rat TGR(mREN2)27. Am. J. Physiol. 1996, 270, E919–E929. [Google Scholar]
- Langheinrich, M.; Lee, M.A.; Bohm, M.; Pinto, Y.M.; Ganten, D.; Paul, M. Hypertensive Ren-2 transgenic rat TGR(mREN2)27 in hypertension research. Characteristic and functional aspects. Am. J. Hypertens. 1996, 9, 506–512. [Google Scholar] [CrossRef] [Green Version]
- Lush, D.J.; King, J.A.; Fray, J.C. Pathophysiology of low renin syndromes: Sites of renal renin secretory impairment and prorenin overexpression. Kidney Int. 1993, 43, 983–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.; Chen, C. The Role of Epoxyeicosatrienoic Acids in Cardiac Remodeling. Front. Physiol. 2021, 12, 642470. [Google Scholar] [CrossRef]
- Kim, G.; Uriel, N.; Burkhoff, D. Reverse remodelling and myocardial recovery in heart failure. Nat. Rev. Cardiol. 2018, 15, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Sporková, A.; Husková, Z.; Škaroupková, P.; Reddy, R.N.; Falck, J.R.; Sadowski, J.; Červenka, L. Vasodilatory responses of renal interlobular arteries to epoxyeicosatrienoic acids analog are not enhanced in Ren-2 transgenic hypertensive rats: Evi-dence against a role of direct vascular effects of epoxyeicosatrienoic acids in the progression of experimental heart failure. Physiol. Res. 2017, 66, 29–39. [Google Scholar] [PubMed]
- Ruzicka, M.; Yuan, B.; Harmsen, E.; Leenen, F.H. The renin-angiotensin system and volume overload-induced cardiac hypertrophy in rats. Effects of angiotensin converting enzyme inhibitor versus angiotensin II receptor blocker. Circulation 1993, 87, 921–930. [Google Scholar] [CrossRef] [Green Version]
- Ruzicka, M.; Yuan, B.; Leenen, F.H.H. Effects of enalapril versus losartan on regression of volume overload-induced cardiac hypertrophy in rats. Circulation 1994, 90, 484–491. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID Assay Number | Gene Name | Abbreviation |
|---|---|---|
| Rn00561847_m1 | renin | Ren |
| Rn00561094_m1 | angiotensin I converting enzyme | Ace |
| Rn01416293_m1 | angiotensin I converting enzyme 2 | Ace2 |
| Rn00593114_m1 | angiotensinogen (serpin peptidase inhibitor, clade A, member 8) | Agt |
| Rn02758772_s1 | angiotensin II receptor, type 1a | Agtr1a |
| Rn00562673_s1 | MAS1 proto-oncogene, G protein-coupled receptor | Mas1 |
| Hs99999901_s1 | 18S rRNA ribosomal subunit | 18s rRNA |
| Rn00598510_m1 | cytochrome P450, family 4, subfamily a, polypeptide 1 | Cyp4a1 |
| Rn01413752_m1 | cytochrome P450, family 2, subfamily c, polypeptide 23 | Cyp2c23 |
| Rn00567876_m1 | adrenoceptor alpha 1A | Adra1a |
| Rn01471343_m1 | adrenoceptor alpha 1B | Adra1b |
| Rn00562488_s1 | adrenoceptor alpha 2A | Adra2a |
| Rn00593312_s1 | adrenoceptor alpha 2B | Adra2b |
| Rn00593341_s1 | adrenoceptor alpha 2C | Adra2c |
| Rn00824536_s1 | adrenoceptor beta 1 | Adrb1 |
| Rn00560650_s1 | adrenoceptor beta 2, surface | Adrb2 |
| Rn00560677_s1 | angiotensin II receptor, type 2 | Agtr2 |
| Group | ||||||
|---|---|---|---|---|---|---|
| HanSD | TGR | ACF TGR | ACF TGR | ACF TGR | ACF TGR | |
| +water | +water | +water | +ACEi | +EET-A | +EET-A + ACEi | |
| Body Weight (g) | 465 ± 7 | 487 ± 9 | 415 ± 9 # | 460 ± 16 | 453 ± 8 | 449 ± 7 |
| Tibia length (mm) | 38.2 ± 0.3 | 37.7 ± 0.2 | 37.5 ± 0.2 | 37.8 ± 0.2 | 37.3 ± 0.3 | 37.4 ± 0.2 |
| Whole heart weight (mg)/tibia length (mm) | 37.69 ± 0.74 | 48.01 ± 0.98 * | 68.27 ± 1.07 # | 54.49 ± 1.06 @ | 64.07 ± 1.19 | 56.69 ± 1.04 @ |
| LV weight (mg)/tibia length (mm) | 24.56 ± 0.21 | 33.69 ± 0.91 * | 40.79 ± 0.89 # | 33.86 ± 0.24 @ | 38.07 ± 0.81 | 35.76 ± 0.26 @ |
| RV weight (mg)/tibia length (mm) | 7.28 ± 0.19 | 7.56 ± 0.21 | 14.69 ± 0.39 # | 11.95 ± 0.18 @ | 15.26 ± 0.43 | 11.69 ± 0.21 @ |
| RV weight (mg)/LV weight (mg) | 0.296 ± 0.02 | 0.224 ± 0.01 | 0.361 ± 0.03 # | 0.353 ± 0.02 | 0.401 ± 0.09 | 0.327 ± 0.02 @ |
| Lung weight (mg)/tibia length (mg) | 50.48 ± 1.06 | 48.52 ± 1.29 | 74.89 ± 1.43 # | 61.69 ± 1.17 @ | 68.48 ± 2.39 | 56.64 ± 1.23 @ |
| Kidney weight (mg)/tibia length (mg) | 39.27 ± 0.51 | 42.19 ± 1.29 | 40.35 ± 1.13 | 36.94 ± 1.44 | 39.04 ± 1.14 | 37.89 ± 0.71 |
| Liver weight (mg)/tibia length (mg) | 455 ± 16 | 459 ± 17 | 435 ± 21 | 449 ± 24 | 464 ± 26 | 432 ± 29 |
| Group | ||||||
|---|---|---|---|---|---|---|
| HanSD | TGR | ACF TGR | ACF TGR | ACF TGR | ACF TGR | |
| +water | +water | +water | +ACEi | +EET-A | +EET-A + ACEi | |
| Heart rate (min−1) | 371 ± 11 | 376 ± 10 | 356 ± 9 | 368 ± 8 | 364 ± 8 | 354 ± 11 |
| LV diastolic diameter (mm) | 6.64 ± 0.13 | 6.14 ± 0.16 | 9.99 ± 0.24 # | 8.95 ± 0.21 | 9.83 ± 0.23 | 10.27 ± 0.25 |
| LV systolic diameter (mm) | 3.39 ± 0.16 | 2.99 ± 0.11 | 6.06 ± 0.27 # | 5.36 ± 0.21 | 6.01 ± 0.19 | 6.37 ± 0.21 |
| LV anterior wall thickness in diastole (mm) | 2.06 ± 0.06 | 2.76 ± 0.04 * | 2.18 ± 0.05 # | 2.08 ± 0.04 | 2.06 ± 0.05 | 1.68 ± 0.02 @ |
| LV posterior wall thickness in diastole (mm) | 2.22 ± 0.06 | 3.11 ± 0.08 * | 2.47 ± 0.08 # | 2.39 ± 0.06 | 2.36 ± 0.06 | 1.87 ± 0.02 @ |
| LV relative wall thickness | 0.67 ± 0.02 | 1.02 ± 0.06 * | 0.48 ± 0.02 # | 0.54 ± 0.03 | 0.48 ± 0.02 | 0.37 ± 0.02 @ |
| LV ejection fraction (%) | 78.2 ± 1.7 | 81.6 ± 0.9 | 67.2 ± 1.1 # | 66.8 ± 1.3 | 68.4 ± 1.4 | 65.2 ± 1.2 |
| LV fractional shortening (%) | 48.5 ± 1.7 | 51.3 ± 0.8 | 39.6 ± 1.1 # | 40.3 ± 1.1 | 38.9 ± 1.1 | 37.6 ± 0.9 |
| LV stroke volume (µL) | 179 ± 6.4 | 156 ± 9.9 | 379 ± 19.3 # | 303 ± 11 | 364 ± 18.4 | 376 ± 18.2 |
| Cardiac output (mL/min) | 60.9 ± 1.7 | 58.5 ± 3.6 | 133.6 ± 5.5 # | 111.5 ± 4.6 | 132.8 ± 6.8 | 139.5 ± 6.1 |
| RV basal diameter in diastole (mm) | 3.23 ± 0.08 | 3.19 ± 0.11 | 5.61 ± 0.36 # | 4.26 ± 0.26 | 4.79 ± 0.25 | 5.62 ± 0.18 |
| RV midcavity diameter in diastole (mm) | 3.07 ± 0.09 | 2.67 ± 0.14 | 5.01 ± 0.43 # | 3.88 ± 0.24 | 4.05 ± 0.20 | 5.28 ± 0.16 |
| RV fractional area change (%) | 54.7 ± 1.9 | 55.7 ± 2.8 | 50.3 ± 2.9 | 49.4 ± 2.1 | 51.5 ± 3.2 | 44.1 ± 2.9 |
| Group | |||||
|---|---|---|---|---|---|
| HanSD | TGR | ACF TGR | ACF TGR | ACF TGR | |
| +water | +water | +ACEi | +EET-A | +EET-A + ACEi | |
| Body Weight (g) | 630 ± 10 | 633 ± 9 | 689 ± 8 # | 701 ± 19 | 608 ± 18 @ |
| Tibia length (mm) | 43.8 ± 0.2 | 43.7 ± 0.3 | 44.1 ± 0.4 | 44.2 ± 0.4 | 44.1 ± 0.4 |
| Whole heart weight (mg)/tibia length (mm) | 33.67 ± 0.58 | 46.69 ± 0.79 * | 65.09 ± 1.12 # | 66.12 ± 1.22 # | 55.01 ± 1.09 @ |
| LV weight (mg)/tibia length (mm) | 26.94 ± 0.23 | 34.55 ± 0.89 * | 39.22 ± 0.27 # | 40.27 ± 0.29 # | 33.33 ± 0.21 @ |
| RV weight (mg)/tibia length (mm) | 7.47 ± 0.21 | 7.57 ± 0.18 | 15.87 ± 0.35 # | 15.77 ± 0.33 # | 11.36 ± 0.22 @ |
| RV weight (mg)/LV weight (mg) | 0.277 ± 0.03 | 0.219 ± 0.03 | 0.405 ± 0.04 # | 0.392 ± 0.03 # | 0.341 ± 0.03 @ |
| Lung weight (mg)/tibia length (mg) | 49.77 ± 1.18 | 48.06 ±1.23 | 61.91 ± 1.51 # | 66.97 ± 1.78 # | 51.29 ± 0.98 @ |
| Kidney weight (mg)/tibia length (mg) | 42.69 ± 0.99 | 42.56 ± 1.17 | 39.01 ± 1.23 | 40.27 ± 1.16 | 39.23 ± 1.25 |
| Liver weight (mg)/tibia length (mg) | 458 ± 19 | 440 ± 23 | 444 ± 27 | 437 ± 25 | 447 ± 28 |
| Group | |||||
|---|---|---|---|---|---|
| HanSD | TGR | ACF TGR | ACF TGR | ACF TGR | |
| +water | +water | +ACEi | +EET-A | +EET-A + ACEi | |
| Heart rate (min−1) | 372 ± 9 | 365 ± 18 | 363 ± 9 | 365 ± 11 | 368 ± 19 |
| LV diastolic diameter (mm) | 6.96 ± 0.22 | 7.09 ± 0.27 | 11.29 ± 0.31 # | 11.12 ± 0.51 # | 11.51 ± 0.29 # |
| LV systolic diameter (mm) | 3.78 ± 0.22 | 4.35 ± 0.39 | 7.55 ± 0.26 # | 7.63 ± 0.44 # | 7.69 ± 0.37 # |
| LV anterior wall thickness in diastole (mm) | 2.32 ± 0.06 | 3.05 ± 0.06 * | 2.06 ± 0.05 # | 2.25 ± 0.06 # | 1.87 ± 0.05 # |
| LV posterior wall thickness in diastole (mm) | 2.55 ± 0.06 | 3.07 ± 0.11 * | 2.08 ± 0.05 # | 2.12 ± 0.07 # | 2.02 ± 0.05 # |
| LV relative wall thickness | 0.738 ± 0.04 | 0.913 ± 0.04 * | 0.368 ± 0.02 # | 0.393 ± 0.02 # | 0.369 ± 0.03 # |
| LV ejection fraction (%) | 75.8 ± 1.9 | 71.6 ± 2.6 | 55.8 ± 1.6 # | 53.9 ± 1.4 # | 57.3 ± 1.5 # |
| LV fractional shortening (%) | 46.1 ± 1.7 | 44.6 ± 1.6 | 33.3 ± 0.7 # | 32.5 ± 1.1 # | 32.4 ± 0.8 # |
| LV stroke volume (µL) | 191 ± 11 | 174 ± 8 | 437 ± 22 # | 408 ± 29 # | 414 ± 31 # |
| Cardiac output (mL/min) | 69.9 ± 1.5 | 63.6 ± 4.2 | 158 ± 6.2 # | 152 ± 10.1 # | 155 ± 8.7 # |
| RV basal diameter in diastole (mm) | 3.06 ± 0.13 | 3.08 ± 0.11 | 6.65 ± 0.19 # | 5.81 ± 0.36 # | 5.41 ± 0.13 @ |
| RV midcavity diameter in diastole (mm) | 2.45 ± 0.11 | 2.49 ± 0.12 | 6.03 ± 0.16 # | 5.28 ± 0.21 # | 5.02 ± 0.12 @ |
| RV fractional area change (%) | 61.9 ± 5.8 | 65.1 ± 5.2 | 35.9 ± 1.1 # | 39.5 ± 1.6 # | 33.7 ± 1.4 # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kala, P.; Miklovič, M.; Jíchová, Š.; Škaroupková, P.; Vaňourková, Z.; Maxová, H.; Gawrys, O.; Kompanowska-Jezierska, E.; Sadowski, J.; Imig, J.D.; et al. Effects of Epoxyeicosatrienoic Acid-Enhancing Therapy on the Course of Congestive Heart Failure in Angiotensin II-Dependent Rat Hypertension: From mRNA Analysis towards Functional In Vivo Evaluation. Biomedicines 2021, 9, 1053. https://doi.org/10.3390/biomedicines9081053
Kala P, Miklovič M, Jíchová Š, Škaroupková P, Vaňourková Z, Maxová H, Gawrys O, Kompanowska-Jezierska E, Sadowski J, Imig JD, et al. Effects of Epoxyeicosatrienoic Acid-Enhancing Therapy on the Course of Congestive Heart Failure in Angiotensin II-Dependent Rat Hypertension: From mRNA Analysis towards Functional In Vivo Evaluation. Biomedicines. 2021; 9(8):1053. https://doi.org/10.3390/biomedicines9081053
Chicago/Turabian StyleKala, Petr, Matúš Miklovič, Šárka Jíchová, Petra Škaroupková, Zdeňka Vaňourková, Hana Maxová, Olga Gawrys, Elzbieta Kompanowska-Jezierska, Janusz Sadowski, John D. Imig, and et al. 2021. "Effects of Epoxyeicosatrienoic Acid-Enhancing Therapy on the Course of Congestive Heart Failure in Angiotensin II-Dependent Rat Hypertension: From mRNA Analysis towards Functional In Vivo Evaluation" Biomedicines 9, no. 8: 1053. https://doi.org/10.3390/biomedicines9081053
APA StyleKala, P., Miklovič, M., Jíchová, Š., Škaroupková, P., Vaňourková, Z., Maxová, H., Gawrys, O., Kompanowska-Jezierska, E., Sadowski, J., Imig, J. D., Falck, J. R., Veselka, J., Červenka, L., Aiglová, R., Vícha, M., Gloger, V., & Táborský, M. (2021). Effects of Epoxyeicosatrienoic Acid-Enhancing Therapy on the Course of Congestive Heart Failure in Angiotensin II-Dependent Rat Hypertension: From mRNA Analysis towards Functional In Vivo Evaluation. Biomedicines, 9(8), 1053. https://doi.org/10.3390/biomedicines9081053