
The Effects of Obesity on Lymphatic Pain and Swelling in Breast Cancer Patients

 , ,
, , 
Abstract: Background
1. Introduction
2. Materials and Methods
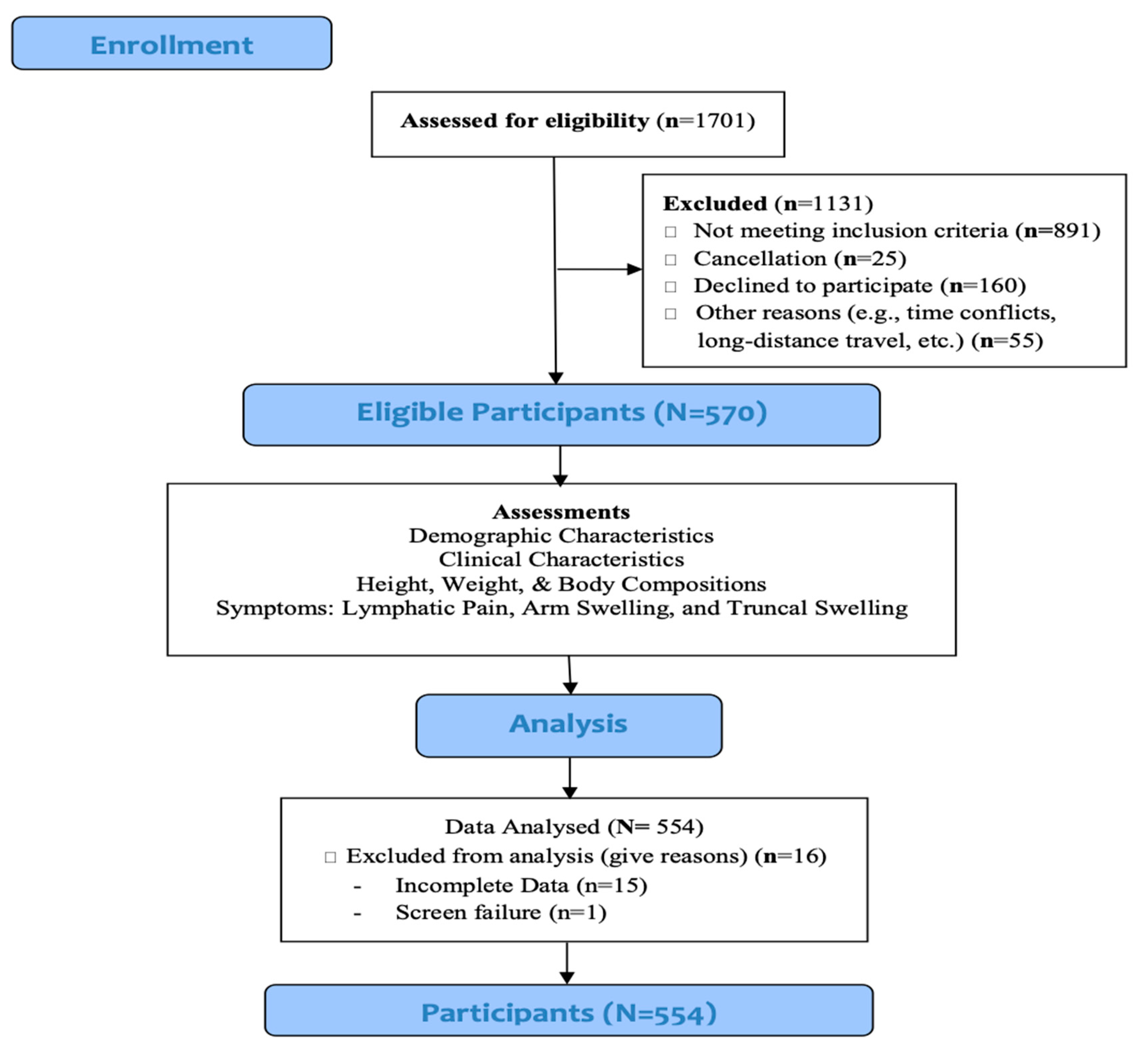
2.1. Study Design
2.2. Ethical Considerations
2.3. Setting
2.4. Study Population
2.5. Variables and Measures
2.5.1. Obesity
2.5.2. Lymphatic Pain, Arm Swelling, and Truncal Swelling
2.5.3. Demographic and Clinical Data
2.6. Study Procedures and Data Collection
2.7. Data Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Participants
3.2. Obesity, Body Fat Percentage and Body Fat Mass
3.3. The Effect of Obesity on Lymphatic Pain
3.4. The Effect of Obesity on Arm Swelling
3.5. The Effect of Obesity on Truncal Swelling
4. Discussion
Limitations and Strengths of the study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 9 May 2021).
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Briefs 2020, 360, 1–8. [Google Scholar]
- Snitker, S. Use of body fatness cutoff points. Mayo Clin. Proc. 2010, 85, 1057–1058. [Google Scholar] [CrossRef] [Green Version]
- Imayama, I.; Alfano, C.M.; Neuhouser, M.L.; George, S.M.; Wilder Smith, A.; Baumgartner, R.N.; Baumgartner, K.B.; Bernstein, L.; Wang, C.Y.; Duggan, C.; et al. Weight, inflammation, cancer-related symptoms and health related quality of life among breast cancer survivors. Breast Cancer Res. Treat. 2013, 140, 159–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agurs-Collins, T.; Ross, S.A.; Dunn, B.K. The many faces of obesity and its influence on breast cancer risk. Front. Oncol. 2019, 9, 765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argolo, D.F.; Hudis, C.A.; Iyengar, N.M. The impact of obesity on breast cancer. Curr. Oncol. Rep. 2018, 20, 47. [Google Scholar] [CrossRef]
- Chan, D.; Vieira, A.R.; Aune, D.; Bandera, E.V.; Greenwood, D.C.; McTiernan, A.; Navarro Rosenblatt, D.; Thune, I.; Vieira, R.; Norat, T. Body mass index and survival in women with breast cancer-systematic literature review and meta-analysis of 82 follow-up studies. Ann. Oncol. 2014, 25, 1901–1914. [Google Scholar] [CrossRef]
- Brorson, H.; Ohlin, K.; Olsson, G.; Nilsson, M. Adipose tissue dominates chronic arm lymphedema following breast cancer: An analysis using volume rendered CT images. Lymphat. Res. Biol. 2006, 4, 199–210. [Google Scholar] [CrossRef]
- Ding, Y.Y.; Yao, P.; Wu, L.; Han, Z.K.; Hong, T.; Zhu, Y.Q.; Li, H.X. Body mass index and persistent pain after breast cancer surgery: Findings from the women’s healthy eating and living study and a meta-analysis. Oncotarget 2017, 8, 43332–43343. [Google Scholar] [CrossRef]
- Degnim, A.C.; Miller, J.; Hoskin, T.L.; Boughey, J.C.; Loprinzi, M.; Thomsen, K.; Maloney, S.; Baddour, L.M.; Cheville, A.L. A prospective study of breast lymphedema: Frequency, symptoms, and quality of life. Breast Cancer Res. Treat. 2012, 134, 915–922. [Google Scholar] [CrossRef] [Green Version]
- Eaton, L.H.; Narkthong, N.; Hulett, J.M. Psychosocial Issues Associated with Breast Cancer-Related Lymphedema: A Literature Review. Curr. Breast Cancer Rep. 2020, 1–9. [Google Scholar] [CrossRef]
- World Health Organization. Breast Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 9 May 2021).
- American Cancer Society. Breast Cancer Facts & Figures 2019–2020. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2019-2020.pdf (accessed on 5 May 2021).
- Washington, A.E.; Lipstein, S.H. The patient-centered outcomes research institute--promoting better information, decisions, and health. N. Engl. J. Med. 2011, 365, e31. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.R.; McTernan, M.L.; Qiu, J.M. The Effects of Kinect-Enhanced Lymphatic Exercise Intervention on Lymphatic Pain, Swelling, and Lymph Fluid Level. Integr. Cancer Ther. 2021, 1–14. [Google Scholar] [CrossRef]
- Armer, J.A.; Ostby, P.; Ginex, P.; Beck, M.; Deng, J.; Fu, M.R.; Lasinski, B.B.; Lockwood, S.; Poage, E.; White, J.; et al. ONS Guidelines for Cancer treatment-related lymphedema. Oncol. Nurs. Forum 2020, 47, 518–538. [Google Scholar] [CrossRef]
- Fu, M.R.; Aouizerat, B.E.; Yu, G.; Conley, Y.; Axelrod, D.; Guth, A.A.; Gagner, J.-P.; Qiu, J.M.; Zagzag, D. Model-based patterns of lymphedema symptomology: Phenotypic and biomarker characterization. Curr. Breast Cancer Rep. 2020. [Google Scholar] [CrossRef]
- Fu, M.R.; Conley, Y.P.; Axelrod, D.; Guth, A.; Yu, G.; Fletcher, J.; Zagzag, D. Precision assessment of heterogeneity of lymphedema phenotype, genotypes and risk prediction. Breast 2016, 29, 231–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, M.R.; Axelrod, D.; Cleland, C.M.; Qiu, Z.; Guth, A.A.; Kleinman, R.; Scagliola, J.; Haber, J. Symptom reporting in detecting breast cancer-related lymphedema. Breast Cancer 2015, 7, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helyer, L.K.; Varnic, M.; Le, L.W.; Leong, W.; McCready, D. Obesity is a risk factor for developing postoperative lymphedema in breast cancer patients. Breast J. 2010, 16, 48–54. [Google Scholar] [CrossRef]
- Greene, A.K.; Zurakowski, D.; Goss, J.A. Body mass index and lymphedema morbidity: Comparison of obese versus normal-weight patients. Plast. Reconstr. Surg. 2020, 146, 402–407. [Google Scholar] [CrossRef]
- Wu, R.; Huang, X.; Dong, X.; Zhang, H.; Zhuang, L. Obese patients have higher risk of breast cancer-related lymphedema than overweight patients after breast cancer: A meta-analysis. Ann. Transl. Med. 2019, 7, 172. [Google Scholar] [CrossRef]
- Forsythe, L.P.; Alfano, C.M.; George, S.M.; McTiernan, A.; Baumgartner, K.B.; Bernstein, L.; Ballard-Barbash, R. Pain in long-term breast cancer survivors: The role of body mass index, physical activity, and sedentary behavior. Breast Cancer Res. Treat. 2013, 137, 617–630. [Google Scholar] [CrossRef] [Green Version]
- Leysen, L.; Beckwée, D.; Nijs, J.; Pas, R.; Bilterys, T.; Vermeir, S.; Adriaenssens, N. Risk factors of pain in breast cancer survivors: A systematic review and meta-analysis. Support Care Cancer 2017, 25, 3607–3643. [Google Scholar] [CrossRef]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Rampertaap, K.; El-Shammaa, N.; Hiotis, K.; Scagliola, J.; Yu, G.; Wang, Y. mHealth self-care interventions: Managing symptoms following breast cancer treatment. mHealth 2016, 2, 28. [Google Scholar] [CrossRef]
- Shi, S.; Lu, Q.; Fu, M.R.; Ouyang, Q.; Liu, C.; Lv, J.; Wang, Y. Psychometric properties of the breast cancer and lymphedema symptom experience index: The Chinese version. Eur. J. Oncol. Nurs. 2016, 20, 10–16. [Google Scholar] [CrossRef]
- Norton, E.C.; Dowd, B.E.; Maciejewski, M.L. Odds Ratios-Current Best Practice and Use. JAMA 2018, 320, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Fletcher, J.; Qiu, J.M.; Scagliola, J.; Kleinman, R.; Ryan CEChan, N.; Haber, J. Patterns of obesity and lymph fluid level during the first year of breast cancer treatment: A prospective study. J. Pers. Med. 2015, 5, 326–340. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A. Racism and Health: Evidence and Needed Research. Annu. Rev. Public Health 2019, 40, 105–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naito, R.; Leong, D.P.; Bankdiwala, S.I.; Mckee, M.; Subramanian, S.V.; McKee, M.; Subramanian, S.V.; Rangarajan, S.; Islam, S.; Avezum, A.; et al. Impact if social on mortality and morbidity in 20 high-income, middle-income and low-income countries in five continents. BMJ Glob. Health 2021, 6, e004124. [Google Scholar] [CrossRef]


{kind=link}
| All Sample N = 554 | Obesity BMI ≥ 30 kg/m2 n = 135 | Non-Obesity BMI < 30 kg/m2 n = 419 | Test Statistics | ||||
|---|---|---|---|---|---|---|---|
| Continuous Variables | 1 (Range) | (Range) | (Range) | t | df 1 | p (t-Test) | Effect Size 2 |
| Age (in years) | 11.31 (26–85) | 11.31 (32–82) | 58.1111.32 (26–85) | 0.54 | 552 | 0.5916 | 0.05 |
| Body fat percentage | 8.96 (7.8–55.2) | 4.90 (29.2–55.2) | 7.20 (7.8–51.1) | −20.82 | 552 | <0.001 | −2.06 |
| Body fat mass | 25.93 (7.5–182.3) | 20.44 (54.4–182.3) | 14.69 (7.5–83.7) | −29.18 | 552 | <0.001 | −2.89 |
| Categorical Variables | n (%) | n (%) | n (%) | Pearson χ2 | df | p (χ2) | Effect Size |
| Ethnicity | 12.92 | 1 | <0.001 | −0.15 | |||
| Non-white | 162 (29.24) | 56 (41.48) | 106 (25.30) | ||||
| White | 392 (70.76) | 79 (58.52) | 313 (74.70) | ||||
| Marital status | 0.03 | 1 | 0.852 | −0.01 | |||
| Married/partnered | 328 (59.21) | 79 (58.52) | 249 (59.43) | ||||
| Not married | 226 (40.79) | 56 (41.48) | 170 (40.57) | ||||
| Education | 2.73 | 2 | 0.255 | 0.07 | |||
| Associate Degree or less | 146 (26.35) | 41 (30.37) | 105 (25.06) | ||||
| Bachelor’s Degree | 209 (37.73) | 53 (39.26) | 156 (37.23) | ||||
| Graduate Degree | 199 (35.92) | 41 (30.37) | 158 (37.71) | ||||
| Financial status | 16.52 | 2 | <0.001 | 0.17 | |||
| Comfortable Finance: Have more than enough to make ends meet | 343 (61.91) | 68 (50.37) | 275 (65.63) | ||||
| Adequate Finance: Have enough to make ends meet | 176 (31.77) | 50 (37.04) | 126 (30.07) | ||||
| Financial Hardship: Do not have enough to make ends meet | 35 (6.32) | 17 (12.59) | 18 (4.30) | ||||
| Employment status | 0.01 | 1 | 0.920 | −0.004 | |||
| Employed | 359 (64.80) | 87 (64.44) | 272 (64.92) | ||||
| Unemployed | 195 (35.20) | 48 (35.56) | 147 (35.08) | ||||
| All Sample N = 554 | Obesity BMI ≥30 kg/m2 n = 135 | Non-Obesity BMI < 30 kg/m2 n = 419 | Test Statistics | ||||
|---|---|---|---|---|---|---|---|
| Continuous Variables | 1 (Range) | (Range) | (Range) | t | df 1 | p (t-Test) | Effect Size 2 |
| Years elapsed since the breast cancer treatment | 5.59 (0–43) | 5.10 (0–27) | 5.72 (0–43) | 0.89 | 552 | 0.3743 | 0.09 |
| Number of lymph nodes removed | 8.41 (1–35) | 7.44 (1–35) | 8.71 (1–35) | 0.32 | 552 | 0.7508 | 0.03 |
| Categorical Variables | n (%) | n (%) | n (%) | Pearson χ2 | df | p (χ2) | Effect Size |
| Lymphedema diagnosis | 7.25 | 1 | 0.007 | 0.11 | |||
| Yes | 122 (22.02) | 41 (30.37) | 81 (19.33) | ||||
| No | 432 (77.98) | 94 (69.63) | 338 (80.67) | ||||
| Diabetes | 11.32 | 1 | 0.001 | 0.14 | |||
| Yes | 22 (3.97) | 12 (8.89) | 10 (2.39) | ||||
| No | 532 (96.03) | 123 (91.11) | 409 (97.61) | ||||
| Lymph node procedures | 1.50 | 1 | 0.221 | 0.05 | |||
| Axillary lymph node dissection | 328 (59.21) | 86 (63.70) | 242 (57.76) | ||||
| Sentinel lymph node biopsy | 226 (40.79) | 49 (36.30) | 177 (42.24) | ||||
| Radiotherapy | 1.49 | 1 | 0.222 | 0.05 | |||
| Yes | 400 (72.20) | 103 (76.30) | 297 (70.88) | ||||
| No | 154 (27.80) | 32 (23.70) | 122 (29.12) | ||||
| Chemotherapy | 0.52 | 1 | 0.471 | 0.03 | |||
| Yes | 355 (64.08) | 90 (66.67) | 265 (63.25) | ||||
| No | 199 (35.92) | 45 (33.33) | 154 (36.75) | ||||
| Hormonal Therapy | 0.10 | 1 | 0.754 | 0.01 | |||
| Yes | 463 (83.57) | 114 (84.44) | 349 (83.29) | ||||
| No | 91 (16.43) | 21 (15.56) | 70 (16.71) | ||||
| All Sample N = 554 | Obesity BMI ≥30 kg/m2 n = 135 | Non-Obesity BMI < 30 kg/m2 n = 419 | Test Statistics | |||
|---|---|---|---|---|---|---|
| Outcome Variables | n (%) | n (%) | n (%) | Pearson χ2 | df 1 | p(χ2) |
| Lymphatic Pain | 29.21 | 1 | <0.001 | |||
| Yes | 182 (32.85) | 70 (51.85) | 112 (26.73) | |||
| No | 372 (67.15) | 65 (48.15) | 307 (73.27) | |||
| Arm Swelling | 23.92 | 1 | <0.001 | |||
| Yes | 217 (39.17) | 77 (57.04) | 140 (33.41) | |||
| No | 337 (60.83) | 58 (42.96) | 279 (66.59) | |||
| Truncal Swelling | 14.08 | 1 | <0.001 | |||
| Yes | 145 (26.17) | 52 (38.52) | 93 (22.20) | |||
| No | 409 (73.83) | 83 (61.48) | 326 (77.80) | |||
| Multivariable Logistic Regression | ||||||
|---|---|---|---|---|---|---|
| B 1 | SE | z-Value | Odds Ratio | OR 95% CI | p Value | |
| Obesity | ||||||
| Yes | 1.25 | 0.32 | 3.94 | 3.49 | (1.87, 6.50) | <0.001 |
| No | -- | -- | -- | -- | -- | |
| Diabetes | ||||||
| Yes | 0.27 | 0.49 | 0.55 | 1.31 | (0.50, 3.43) | 0.583 |
| No | -- | -- | -- | -- | -- | |
| Ethnicity | ||||||
| Non-white | −0.20 | 0.23 | −0.89 | 0.82 | (0.53, 1.27) | 0.374 |
| White | -- | -- | -- | -- | -- | |
| Marital status | ||||||
| Married/partnered | −0.15 | 0.21 | −0.70 | 0.86 | (0.57, 1.31) | 0.483 |
| Not married | -- | -- | -- | -- | -- | |
| Education | ||||||
| Associate Degree or less | 0.42 | 0.26 | 1.60 | 1.52 | (0.91, 2.54) | 0.110 |
| Bachelor’s degree | -- | -- | -- | -- | -- | |
| ≥Master’s Degree | −0.13 | 0.24 | −0.54 | 0.88 | (0.55, 1.41) | 0.592 |
| Financial status | ||||||
| Comfortable finance | 0.16 | 0.22 | 0.71 | 1.17 | (0.76, 1.81) | 0.477 |
| Financial hardship | 1.16 | 0.42 | 2.74 | 3.19 | (1.39, 7.31) | 0.006 |
| Adequate finance | -- | -- | -- | -- | -- | |
| Employment status | ||||||
| Employed | 0.12 | 0.23 | 0.52 | 1.13 | (0.72, 1.79) | 0.600 |
| Unemployed | -- | -- | -- | -- | -- | |
| Types of surgery | ||||||
| Mastectomy | 0.40 | 0.25 | 1.60 | 1.50 | (0.91, 2.45) | 0.109 |
| Lumpectomy | -- | -- | -- | -- | -- | |
| Lymph node procedures | ||||||
| Axillary lymph node dissection | 0.42 | 0.27 | 1.57 | 1.52 | (0.90, 2.56) | 0.117 |
| Sentinel lymph node biopsy | -- | -- | -- | -- | -- | |
| Radiotherapy | ||||||
| Yes | 0.58 | 0.27 | 2.13 | 1.78 | (1.05, 3.03) | 0.033 |
| No | -- | -- | -- | -- | -- | |
| Chemotherapy | ||||||
| Yes | 0.33 | 0.24 | 1.36 | 1.39 | (0.87, 2.24) | 0.173 |
| No | -- | -- | -- | -- | -- | |
| Hormonal therapy | ||||||
| Yes | 0.52 | 0.30 | 1.74 | 1.69 | (0.94, 3.04) | 0.082 |
| No | -- | -- | -- | -- | -- | |
| Age (in years) | −0.02 | 0.01 | −1.47 | 0.98 | (0.96, 1.01) | 0.142 |
| Years elapsed since the breast cancer treatment | −0.02 | 0.02 | −0.99 | 0.98 | (0.94, 1.02) | 0.323 |
| Numbers of lymph nodes removed | 0.03 | 0.02 | 2.05 | 1.03 | (1.00, 1.06) | 0.041 |
| Body fat percentage | −0.01 | 0.02 | −0.94 | 0.99 | (0.96, 1.02) | 0.348 |
| Intercept | −2.29 | 0.67 | −3.40 | 0.10 | (0.03, 0.38) | 0.001 |
| McFadden’s Pseudo R2 | 0.137 | |||||
| LR χ2 (18) | 95.77 | |||||
| Prob > χ2 | <0.001 | |||||
| Multivariable Logistic Regression | ||||||
|---|---|---|---|---|---|---|
| B 1 | SE | z-Value | Odds Ratio | OR 95% CI | p Value | |
| Obesity | ||||||
| Yes | 1.38 | 0.31 | 4.40 | 3.98 | (1.82, 4.43) | <0.001 |
| No | -- | -- | -- | -- | -- | |
| Diabetes | ||||||
| Yes | 0.20 | 0.50 | 0.39 | 1.22 | (0.46, 3.22) | 0.695 |
| No | -- | -- | -- | -- | -- | |
| Ethnicity | ||||||
| Non-white | −0.09 | 0.22 | −0.39 | 0.92 | (0.60, 1.41) | 0.696 |
| White | -- | -- | -- | -- | -- | |
| Marital status | ||||||
| Married/partnered | −0.20 | 0.20 | −0.97 | 0.82 | (0.55, 1.22) | 0.330 |
| Not married | -- | -- | -- | -- | -- | |
| Education | ||||||
| Associate Degree or less | 0.35 | 0.26 | 1.34 | 1.41 | (0.85, 2.34) | 0.179 |
| Bachelor’s degree | -- | -- | -- | -- | -- | |
| ≥Master’s Degree | −0.12 | 0.23 | −0.51 | 0.89 | (0.56, 1.40) | 0.612 |
| Financial Status | ||||||
| Comfortable finance | −0.04 | 0.22 | −0.19 | 0.96 | (0.63, 1.47) | 0.848 |
| Financial hardship | 0.89 | 0.44 | 2.03 | 2.43 | (1.03, 5.74) | 0.043 |
| Adequate finance | -- | -- | -- | -- | -- | |
| Employment status | ||||||
| Employed | 0.002 | 0.22 | 0.01 | 1.00 | (0.65, 1.56) | 0.992 |
| Unemployed | -- | -- | -- | -- | -- | |
| Types of surgery | ||||||
| Mastectomy | 0.78 | 0.25 | 3.13 | 2.17 | (1.4, 3.53) | 0.002 |
| Lumpectomy | -- | -- | -- | -- | -- | |
| Lymph node procedures | ||||||
| Axillary lymph node dissection | 0.53 | 0.26 | 2.06 | 1.69 | (1.03, 2.80) | 0.040 |
| Sentinel lymph node biopsy | -- | -- | -- | -- | -- | |
| Radiotherapy | ||||||
| Yes | 0.80 | 0.26 | 3.03 | 2.23 | (1.33, 3.75) | 0.002 |
| No | -- | -- | -- | -- | -- | |
| Chemotherapy | ||||||
| Yes | 0.17 | 0.23 | 0.76 | 1.19 | (0.76, 1.87) | 0.448 |
| No | -- | -- | -- | -- | -- | |
| Hormonal therapy | ||||||
| Yes | −0.02 | 0.27 | −0.06 | 0.98 | (0.58, 1.67) | 0.948 |
| No | -- | -- | -- | -- | -- | |
| Age (in years) | −0.01 | 0.01 | −0.50 | 0.99 | (0.97, 1.02) | 0.620 |
| Years elapsed since the breast cancer treatment | −0.003 | 0.02 | −0.19 | 1.00 | (0.96, 1.03) | 0.852 |
| Number of lymph nodes removed | 0.03 | 0.02 | 2.05 | 1.03 | (1.00, 1.06) | 0.040 |
| Body fat percentage | −0.03 | 0.02 | −1.93 | 0.97 | (0.94, 1.00) | 0.053 |
| Intercept | −1.20 | 0.62 | −1.94 | 0.30 | (0.09, 1.01) | 0.052 |
| McFadden’s Pseudo R2 | 0.142 | |||||
| LR χ2 (18) | 105.47 | |||||
| Prob > χ2 | <0.001 | |||||
| Multivariable Logistic Regression | ||||||
|---|---|---|---|---|---|---|
| B 1 | SE | z-Value | Odds Ratio | OR 95% CI | p Value | |
| Obesity | ||||||
| Yes | 0.61 | 0.31 | 1.95 | 1.85 | (1.00, 3.42) | 0.051 |
| No | -- | -- | -- | -- | -- | |
| Diabetes | ||||||
| Yes | 0.001 | 0.51 | 0.00 | 1.00 | (0.37, 2.70) | 0.997 |
| No | -- | -- | -- | -- | -- | |
| Ethnicity | ||||||
| Non-white | −0.06 | 0.23 | −0.25 | 0.94 | (0.60, 1.48) | 0.805 |
| White | -- | -- | -- | -- | -- | |
| Marital status | ||||||
| Married/partnered | −0.14 | 0.21 | −0.65 | 0.87 | (0.57, 1.32) | 0.514 |
| Not married | -- | -- | -- | -- | -- | |
| Education | ||||||
| Associate Degree or less | 0.38 | 0.27 | 1.43 | 1.47 | (0.87, 2.48) | 0.152 |
| Bachelor’s degree | -- | -- | -- | -- | -- | |
| ≥Master’s Degree | 0.26 | 0.24 | 1.07 | 1.30 | (0.80, 2.09) | 0.286 |
| Financial status | ||||||
| Comfortable finance | 0.30 | 0.22 | 1.35 | 1.35 | (0.87, 2.09) | 0.176 |
| Financial hardship | 0.22 | 0.42 | 0.52 | 1.24 | (0.55, 2.81) | 0.602 |
| Adequate finance | -- | -- | -- | -- | -- | -- |
| Employment status | ||||||
| Employed | −0.04 | 0.23 | −0.16 | 0.96 | (0.61, 1.52) | 0.869 |
| Unemployed | -- | -- | -- | -- | -- | |
| Types of surgery | ||||||
| Mastectomy | −0.64 | 0.26 | −2.45 | 0.53 | (0.32, 0.88) | 0.014 |
| Lumpectomy | -- | -- | -- | -- | -- | |
| Lymph node procedures | ||||||
| Axillary lymph node dissection | 0.25 | 0.26 | 0.96 | 1.29 | (0.77, 2.17) | 0.337 |
| Sentinel lymph node biopsy | -- | -- | -- | -- | -- | |
| Radiotherapy | ||||||
| Yes | 0.10 | 0.28 | 0.36 | 1.11 | (0.64, 1.92) | 0.722 |
| No | -- | -- | -- | -- | -- | |
| Chemotherapy | ||||||
| Yes | 0.13 | 0.24 | 0.54 | 1.13 | (0.71, 1.80) | 0.591 |
| No | -- | -- | -- | -- | -- | |
| Hormonal therapy | ||||||
| Yes | −0.01 | 0.28 | −0.05 | 0.99 | (0.57, 1.71) | 0.959 |
| No | -- | -- | -- | -- | -- | |
| Age (in years) | −0.02 | 0.01 | −2.10 | 0.98 | (0.96, 1.00) | 0.036 |
| Years elapsed since the breast cancer treatment | −0.04 | 0.02 | −1.85 | 0.96 | (0.91, 1.00) | 0.064 |
| Numbers of lymph nodes removed | 0.004 | 0.02 | 0.26 | 1.00 | (0.97, 1.04) | 0.793 |
| Body fat percentage | 0.01 | 0.02 | 0.57 | 1.01 | (0.98, 1.04) | 0.570 |
| Intercept | −1.73 | 0.67 | −2.59 | 0.18 | (0.09, 0.60) | 0.010 |
| McFadden’s Pseudo R2: | 0.060 | |||||
| LR χ2 (18) | 38.35 | |||||
| Prob > χ2 | 0.004 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, M.R.; Axelrod, D.; Guth, A.; McTernan, M.L.; Qiu, J.M.; Zhou, Z.; Ko, E.; Magny-Normilus, C.; Scagliola, J.; Wang, Y. The Effects of Obesity on Lymphatic Pain and Swelling in Breast Cancer Patients. Biomedicines 2021, 9, 818. https://doi.org/10.3390/biomedicines9070818
Fu MR, Axelrod D, Guth A, McTernan ML, Qiu JM, Zhou Z, Ko E, Magny-Normilus C, Scagliola J, Wang Y. The Effects of Obesity on Lymphatic Pain and Swelling in Breast Cancer Patients. Biomedicines. 2021; 9(7):818. https://doi.org/10.3390/biomedicines9070818
Chicago/Turabian StyleFu, Mei Rosemary, Deborah Axelrod, Amber Guth, Melissa L. McTernan, Jeanna M. Qiu, Zhuzhu Zhou, Eunjung Ko, Cherlie Magny-Normilus, Joan Scagliola, and Yao Wang. 2021. "The Effects of Obesity on Lymphatic Pain and Swelling in Breast Cancer Patients" Biomedicines 9, no. 7: 818. https://doi.org/10.3390/biomedicines9070818
APA StyleFu, M. R., Axelrod, D., Guth, A., McTernan, M. L., Qiu, J. M., Zhou, Z., Ko, E., Magny-Normilus, C., Scagliola, J., & Wang, Y. (2021). The Effects of Obesity on Lymphatic Pain and Swelling in Breast Cancer Patients. Biomedicines, 9(7), 818. https://doi.org/10.3390/biomedicines9070818