
Potential of an Enzyme Mixture of Glucose Oxidase, Glucosyl Transferase, and Fructosyl Transferase as an Antidiabetic Medicine

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Reagents
2.2. Animals and Experimental Design
2.3. Biochemical and Histopathological Examinations
2.4. Gut Microbiota Analysis
2.5. Statistical Analysis
3. Results
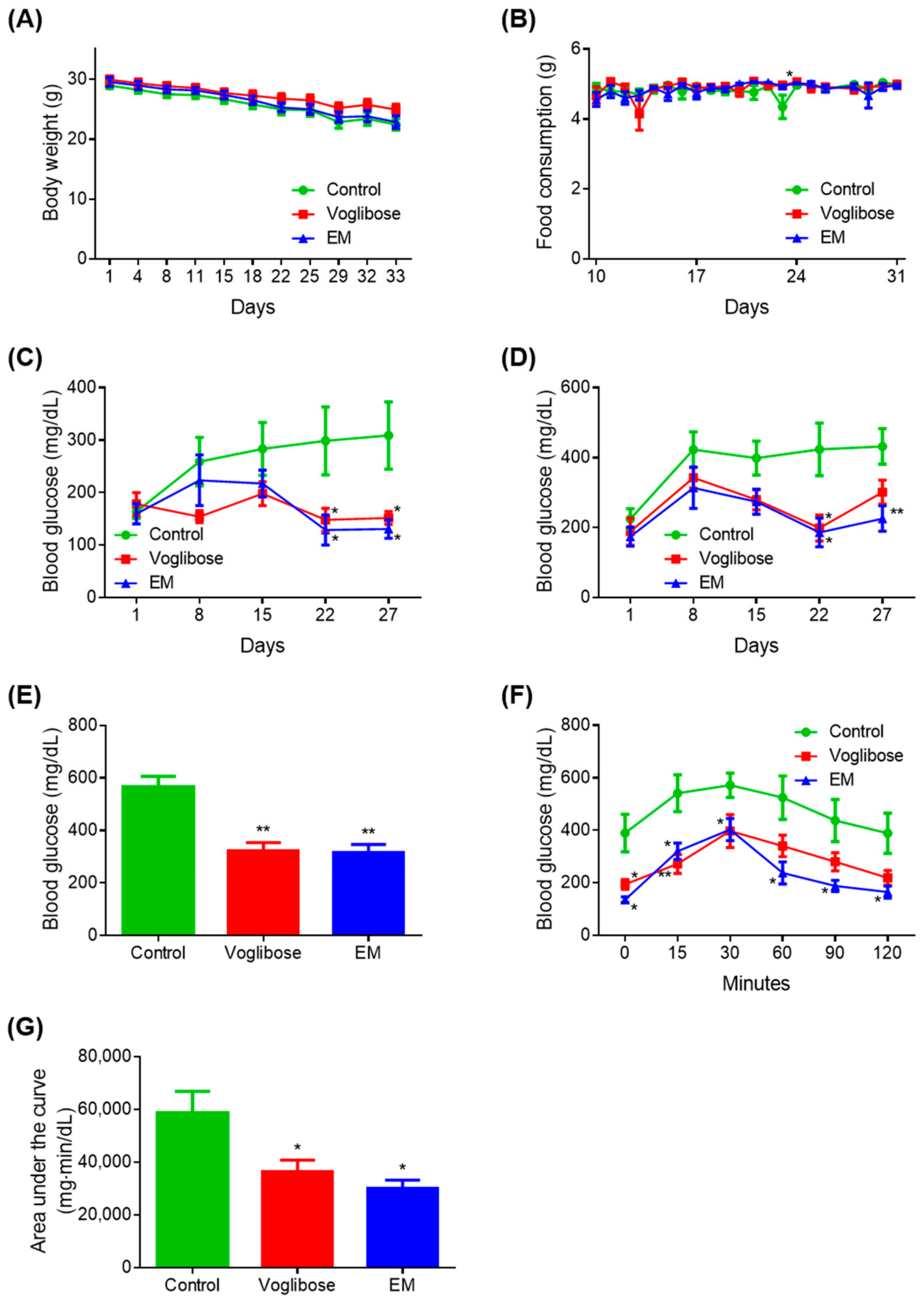
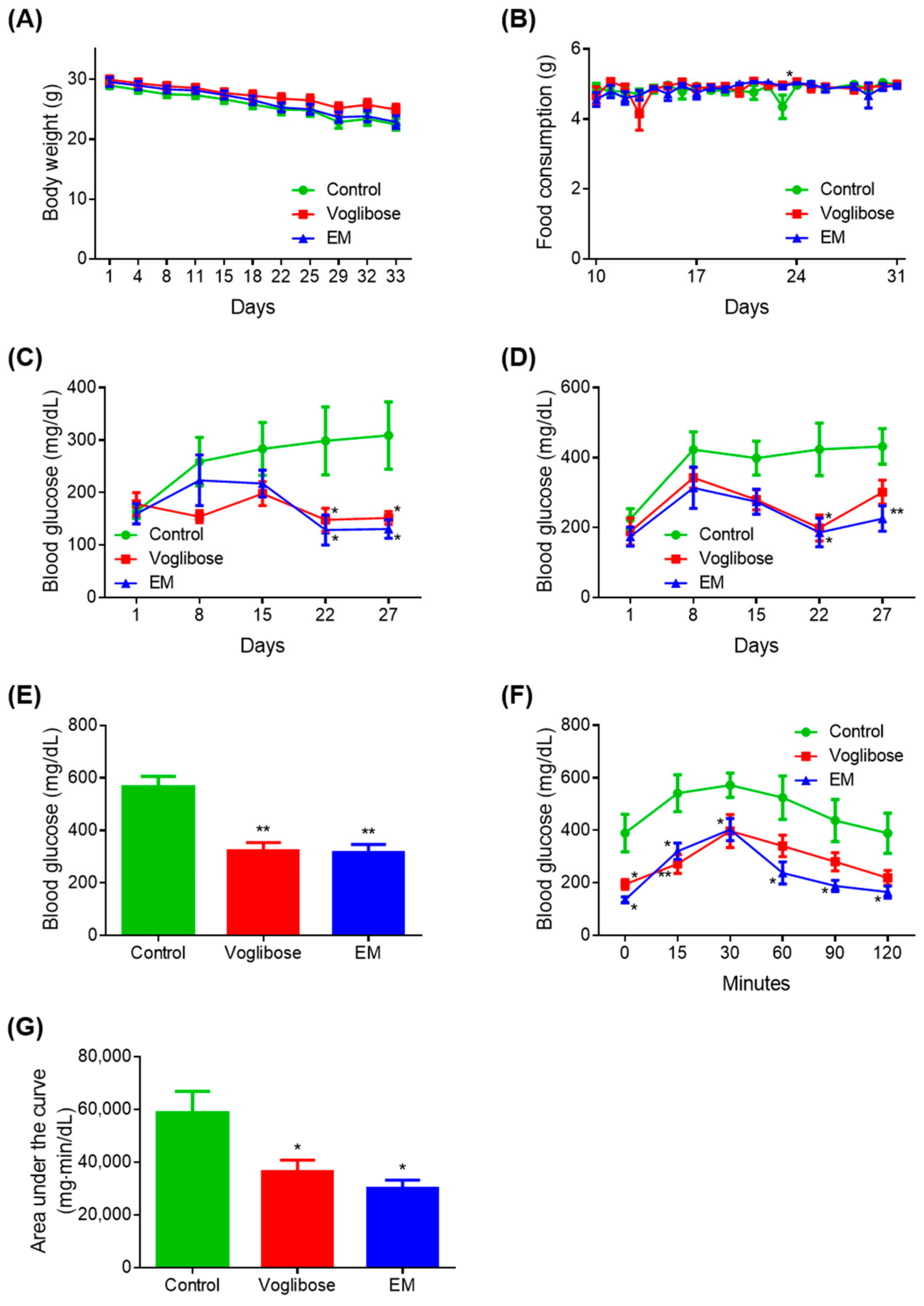
3.1. Antidiabetic Effects of EM Administration
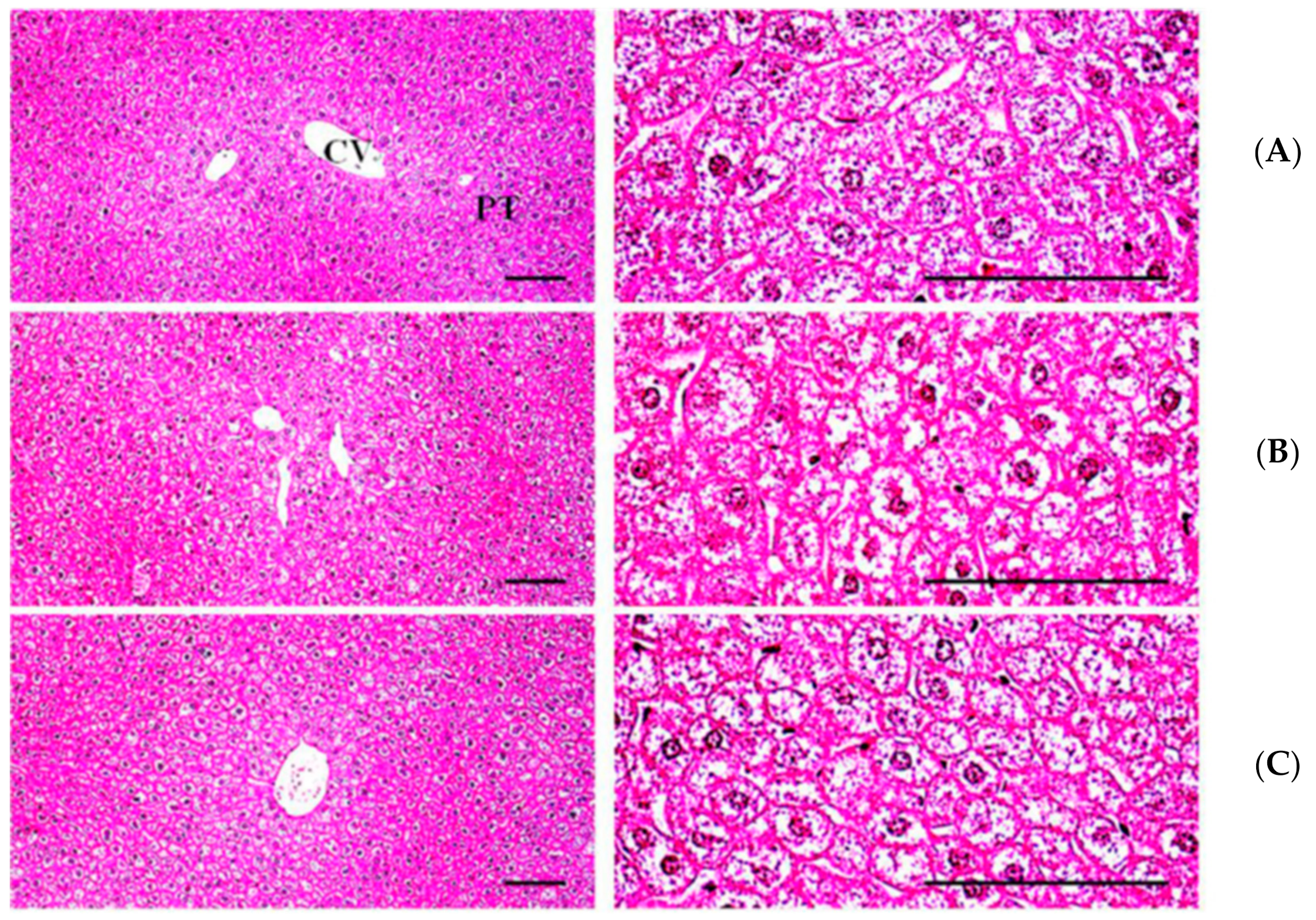
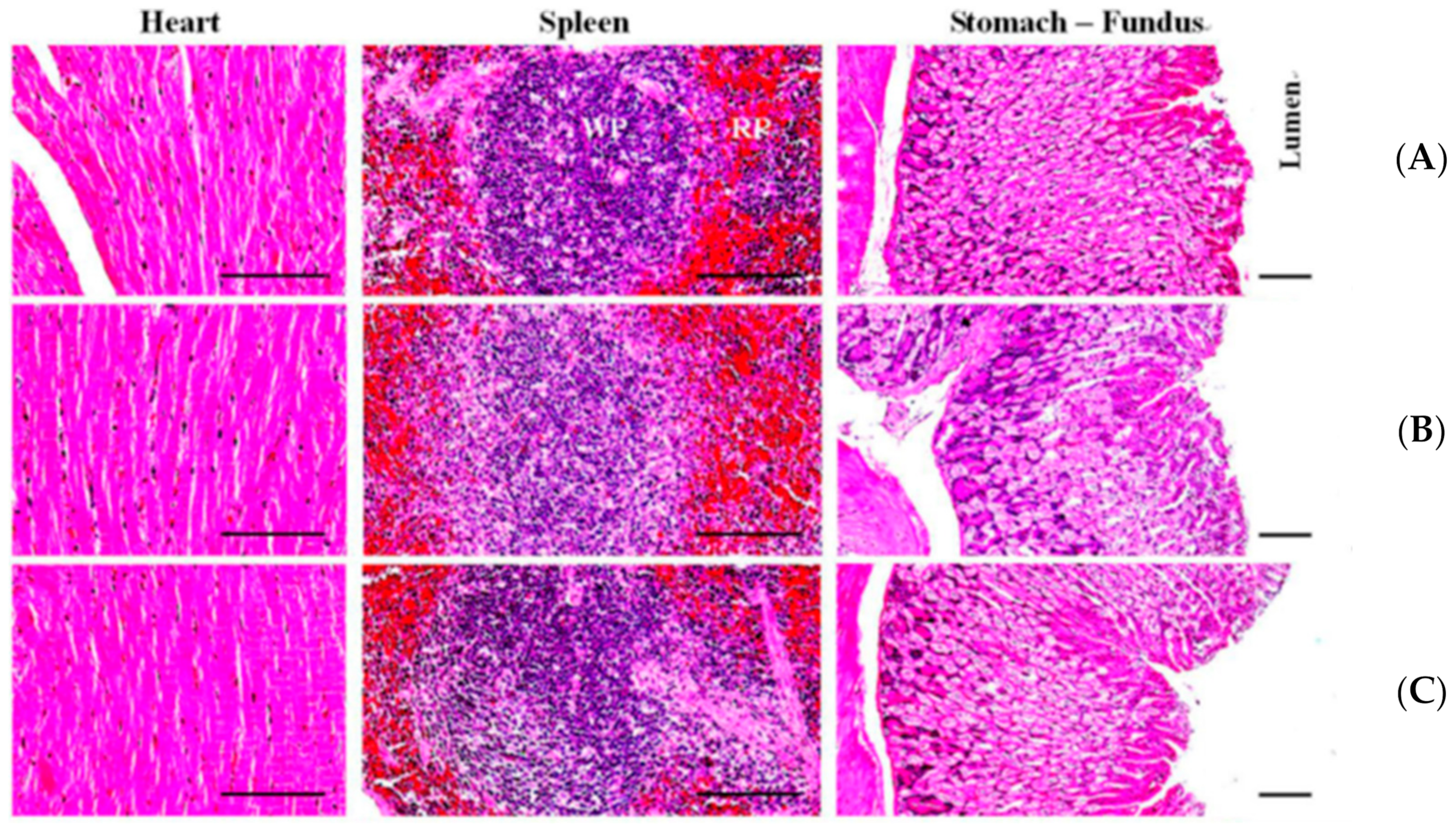
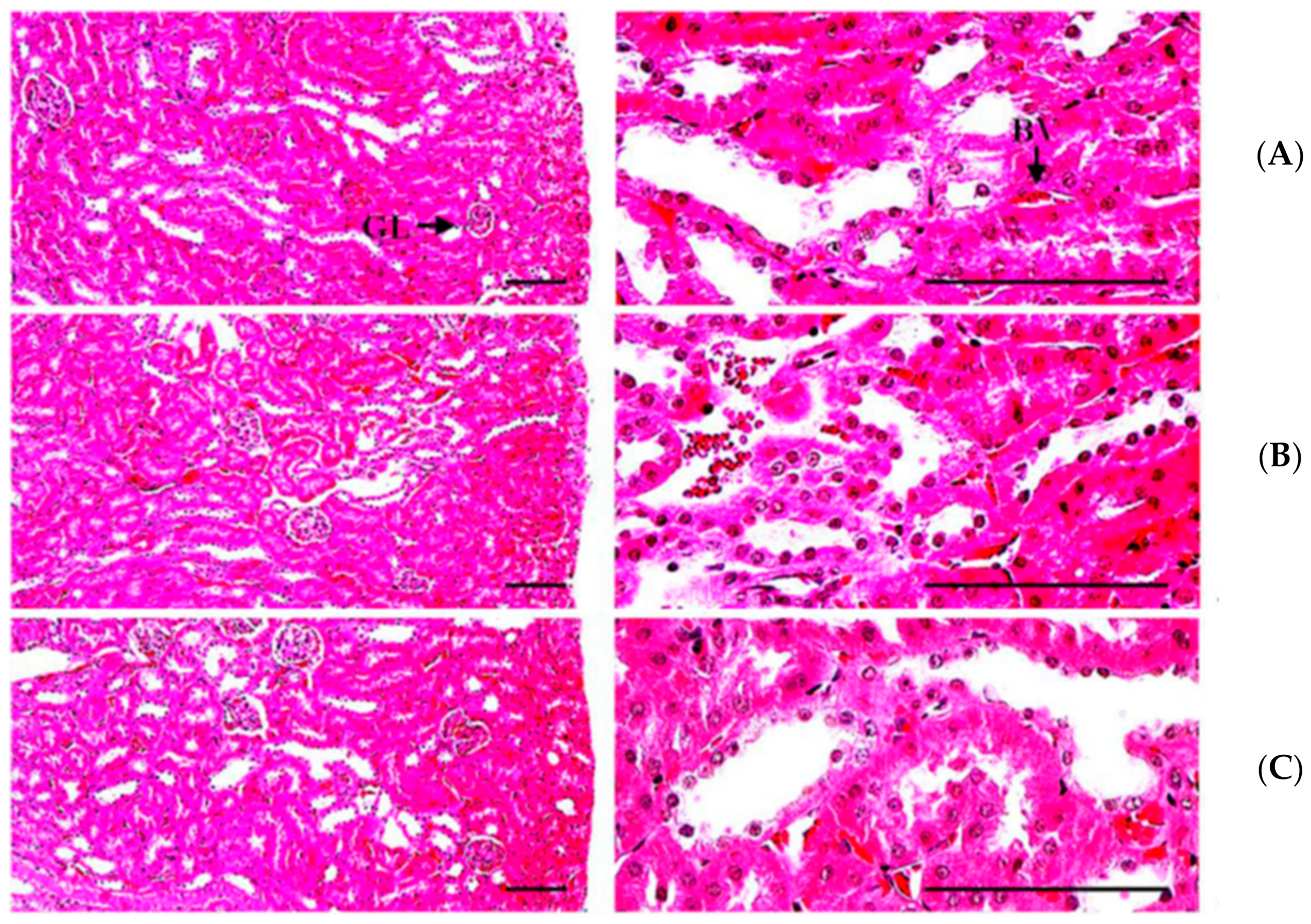
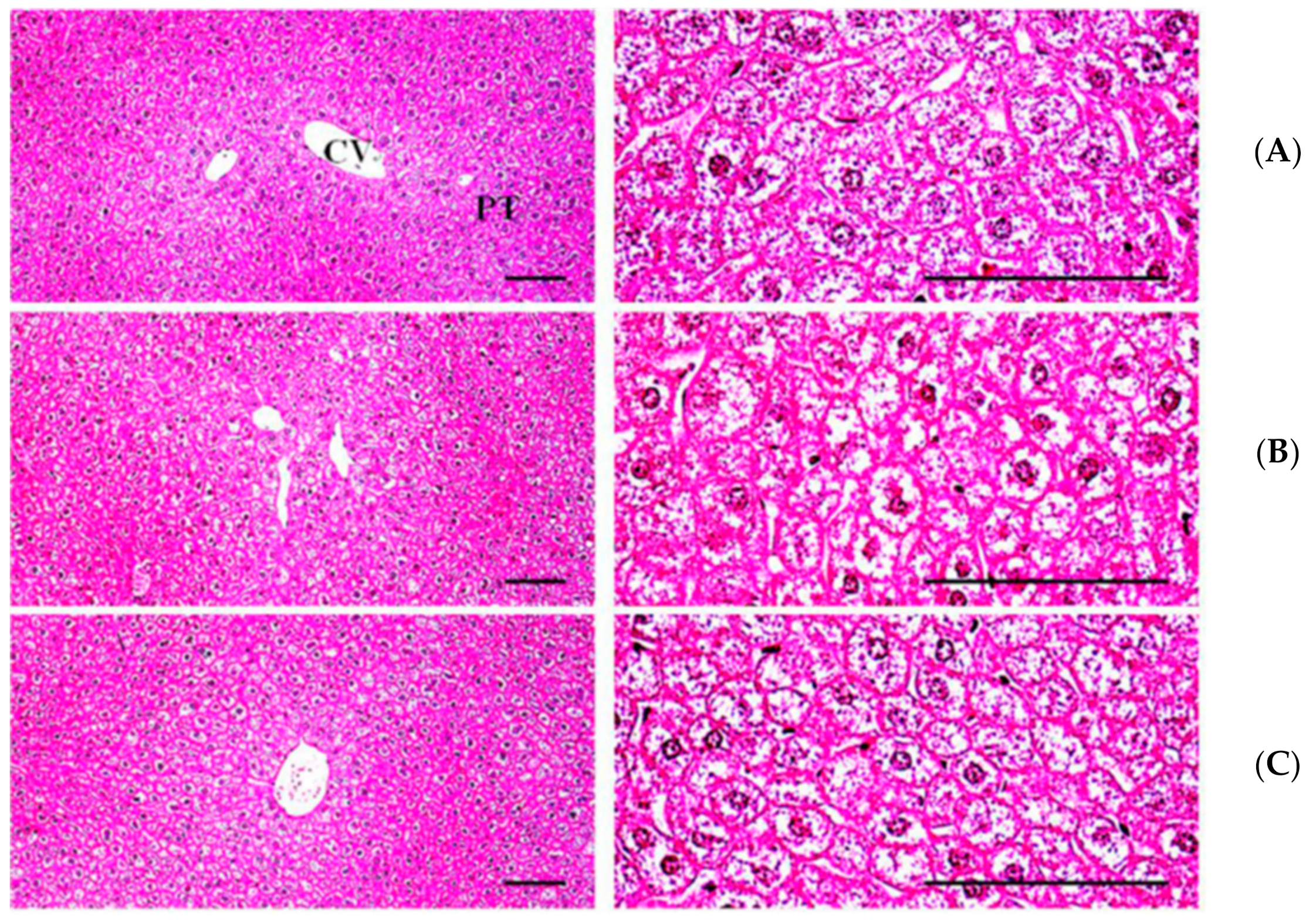
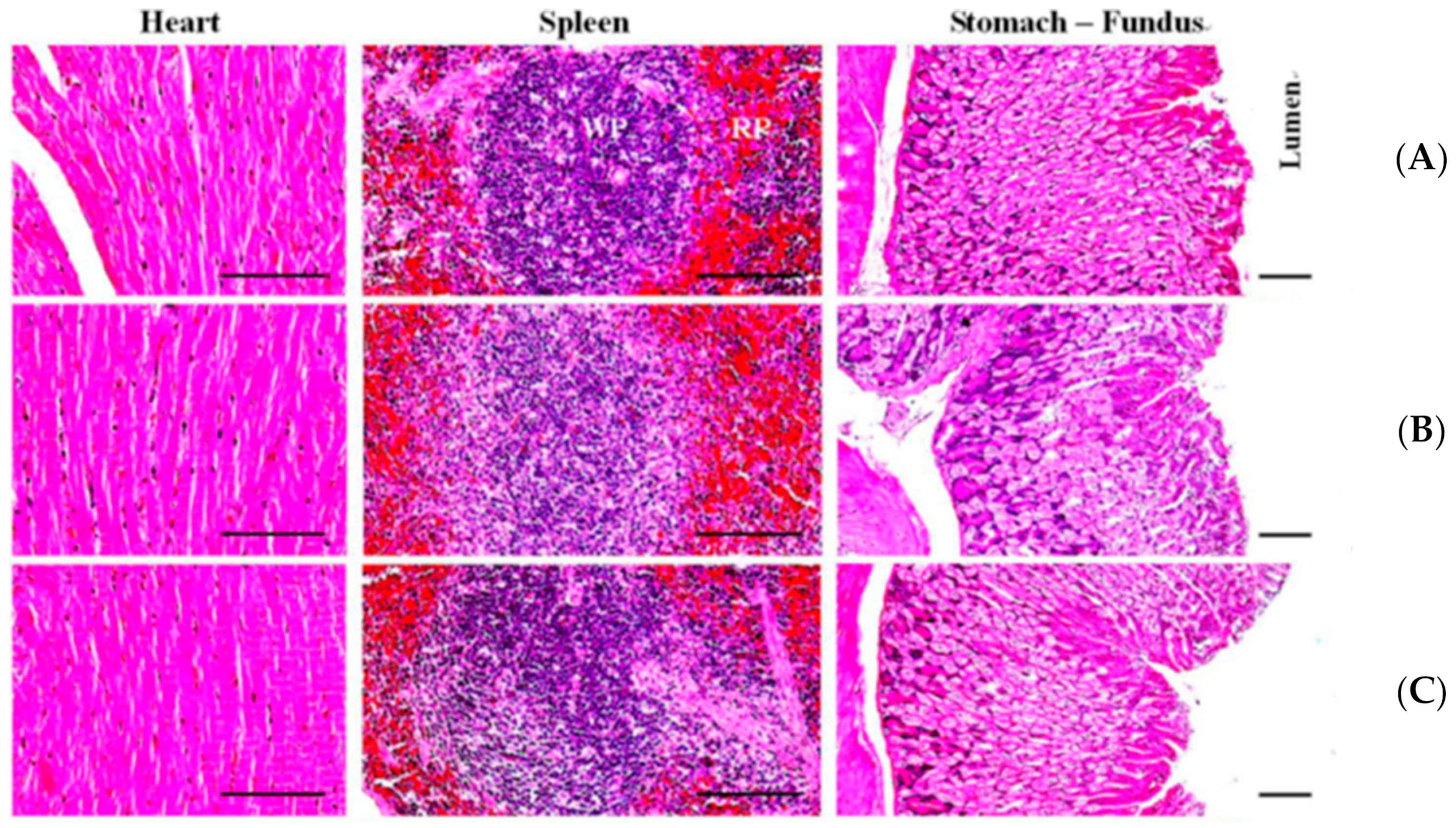
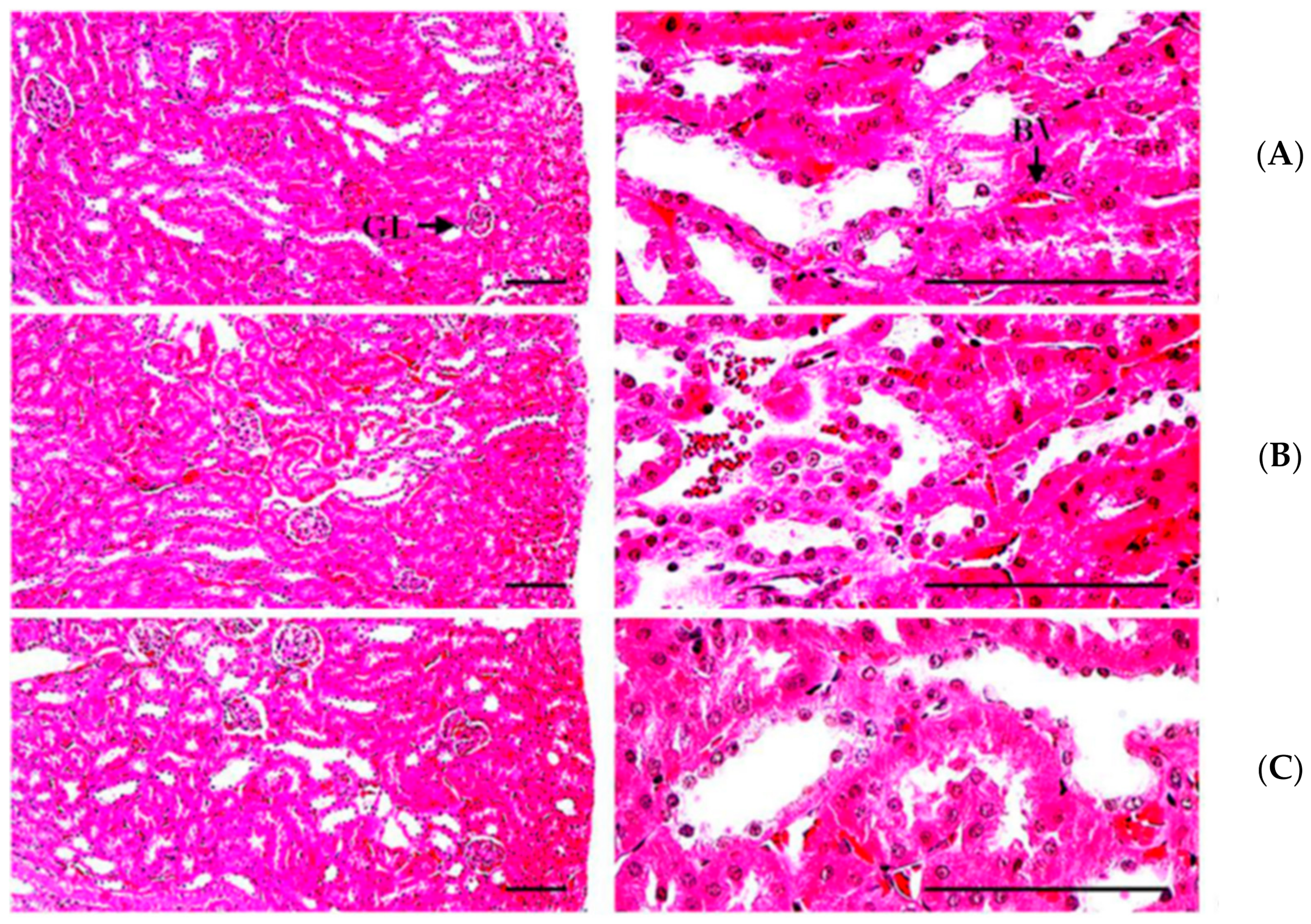
3.2. Biochemical and Histopathological Examination after EM Administration
3.3. Gut Microbiota Analysis before and after EM Administration
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Al-Lawati, J.A. Diabetes Mellitus: A Local and Global Public Health Emergency! Oman Med. J. 2017, 32, 177–179. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Dietz, W.H.; Colditz, G. Guidelines for Healthy Weight. N. Engl. J. Med. 1999, 341, 427–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 8. Obesity Management for the Treatment of Type 2 Diabetes:Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S100–S110. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Hjorth, M.F.; Astrup, A. Diet and exercise in the prevention and treatment of type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2020, 16, 545–555. [Google Scholar] [CrossRef]
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S111–S124. [Google Scholar] [CrossRef]
- Zheng, Y.; Gou, X.; Zhang, L.; Gao, H.; Wei, Y.; Yu, X.; Pang, B.; Tian, J.; Tong, X.; Li, M. Interactions Between Gut Microbiota, Host, and Herbal Medicines: A Review of New Insights into the Pathogenesis and Treatment of Type 2 Diabetes. Front. Cell Infect. Microbiol. 2020, 10, 360. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 3. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S34–S39. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- The Diabetes Prevention Program Research Group. Long-Term Safety, Tolerability, and Weight Loss Associated with Metformin in the Diabetes Prevention Program Outcomes Study. Diabetes Care 2012, 35, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Aroda, V.R.; Edelstein, S.L.; Goldberg, R.B.; Knowler, W.C.; Marcovina, S.M.; Orchard, T.; Bray, G.A.; Schade, D.S.; Temprosa, M.G.; White, N.H.; et al. Long-term Metformin Use and Vitamin B12 Deficiency in the Diabetes Prevention Program Outcomes Study. J. Clin. Endocrinol. Metab. 2016, 101, 1754–1761. [Google Scholar] [CrossRef]
- Sasaki, M.; Ogasawara, N.; Funaki, Y.; Mizuno, M.; Iida, A.; Goto, C.; Koikeda, S.; Kasugai, K.; Joh, T. Transglucosidase improves the gut microbiota profile of type 2 diabetes mellitus patients: A randomized double-blind, placebo-controlled study. BMC Gastroenterol. 2013, 13, 81. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Joh, T.; Koikeda, S.; Kataoka, H.; Tanida, S.; Oshima, T.; Ogasawara, N.; Ohara, H.; Nakao, H.; Kamiya, T. A Novel Strategy in Production of Oligosaccharides in Digestive Tract: Prevention of Postprandial Hyperglycemia and Hyperinsulinemia. J. Clin. Biochem. Nutr. 2007, 41, 191–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, M.; Imaeda, K.; Okayama, N.; Mizuno, T.; Kataoka, H.; Kamiya, T.; Kubota, E.; Ogasawara, N.; Funaki, Y.; Mizuno, M.; et al. Effects of transglucosidase on diabetes, cardiovascular risk factors and hepatic biomarkers in patients with type 2 diabetes: A 12-week, randomized, double-blind, placebo-controlled trial. Diabetes Obes. Metab. 2011, 14, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Daliri, E.B.-M.; Lee, B.H. Current Trends and Future Perspectives on Functional Foods and Nutraceuticals. In Beneficial Microorganisms in Food and Nutraceuticals; Springer: Berlin/Heidelberg, Germany, 2015; pp. 221–244. [Google Scholar]
- Rehrig, A.; DeMagistris, M.; Callan, C. Refinements in laboratory cat management: While the humans are away, the cats will play! Lab. Anim. Sci. Prof. 2013, 1, 32–35. [Google Scholar]
- Czech, M.P. Insulin action and resistance in obesity and type 2 diabetes. Nat. Med. 2017, 23, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Hyde, P.N.; Sapper, T.N.; Crabtree, C.D.; LaFountain, R.A.; Bowling, M.L.; Buga, A.; Fell, B.; McSwiney, F.; Dickerson, R.M.; Miller, V.J.; et al. Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI Insight 2019, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hummel, K.P.; Dickie, M.M.; Coleman, D.L. Diabetes, a New Mutafton in the Mouse. Science 1966, 153, 1127–1128. [Google Scholar] [CrossRef]
- Parks, E.J. Effect of Dietary Carbohydrate on Triglyceride Metabolism in Humans. J. Nutr. 2001, 131, 2772S–2774S. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O’Keefe, J.H.; Lucan, S.C. Added Fructose. Mayo Clin. Proc. 2015, 90, 372–381. [Google Scholar] [CrossRef] [Green Version]
- Bankar, S.B.; Bule, M.V.; Singhal, R.; Ananthanarayan, L. Glucose oxidase—An overview. Biotechnol. Adv. 2009, 27, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Kapat, A.; Jung, J.-K.; Park, Y.-H. Improvement of extracellular recombinant glucose oxidase production in fed-batch culture of Saccharomyces cerevisiae: Effect of different feeding strategies. Biotechnol. Lett. 1998, 20, 319–323. [Google Scholar] [CrossRef]
- Wu, S.; Li, T.; Niu, H.; Zhu, Y.; Liu, Y.; Duan, Y.; Sun, Q.; Yang, X. Effects of glucose oxidase on growth performance, gut function, and cecal microbiota of broiler chickens. Poult. Sci. 2019, 98, 828–841. [Google Scholar] [CrossRef]
- Knaus, U.G.; Hertzberger, R.; Pircalabioru, G.G.; Yousefi, S.P.M.; Dos Santos, F.B. Pathogen control at the intestinal mucosa—H2O2 to the rescue. Gut Microbes 2016, 8, 67–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botteaux, A.; Hoste, C.; Dumont, J.; Van Sande, J.; Allaoui, A. Potential role of Noxes in the protection of mucosae: H2O2 as abacterial repellent. Microbes Infect. 2009, 11, 537–544. [Google Scholar] [CrossRef]
- Corcionivoschi, N.; Alvarez, L.A.; Sharp, T.; Strengert, M.; Alemka, A.; Mantell, J.; Verkade, P.; Knaus, U.G.; Bourke, B. Mucosal Reactive Oxygen Species Decrease Virulence by Disrupting Campylobacter jejuni Phosphotyrosine Signaling. Cell Host Microbe 2012, 12, 47–59. [Google Scholar] [CrossRef] [Green Version]
- van Baarlen, P.; Wells, J.M.; Kleerebezem, M. Regulation of intestinal homeostasis and immunity with probiotic lactobacilli. Trends Immunol. 2013, 34, 208–215. [Google Scholar] [CrossRef]
- Saez-Lara, M.J.; Gomez-Llorente, C.; Plaza-Diaz, J.; Gil, A. The Role of Probiotic Lactic Acid Bacteria and Bifidobacteria in the Prevention and Treatment of Inflammatory Bowel Disease and Other Related Diseases: A Systematic Review of Randomized Human Clinical Trials. BioMed Res. Int. 2015, 2015, 1–15. [Google Scholar] [CrossRef]
- Wasilewski, A.; Zielińska, M.; Storr, M.; Fichna, J. Beneficial Effects of Probiotics, Prebiotics, Synbiotics, and Psychobiotics in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2015, 21, 1674–1682. [Google Scholar] [CrossRef]
- Sako, T.; Mori, A.; Lee, P.; Goto, H.; Fukuta, H.; Oda, H.; Saeki, K.; Miki, Y.; Makino, Y.; Ishioka, K.; et al. Supplementing transglucosidase with a high-fiber diet for prevention of postprandial hyperglycemia in streptozotocin-induced diabetic dogs. Vet. Res. Commun. 2010, 34, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.R. Dietary Modulation of the Human Gut Microflora Using the Prebiotics Oligofructose and Inulin. J. Nutr. 1999, 129, 1438S–1441S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langlands, S.J.; Hopkins, M.J.; Coleman, N.; Cummings, J.H. Prebiotic carbohydrates modify the mucosa associated microflora of the human large bowel. Gut 2004, 53, 1610–1616. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E.; Bäckhed, F.; Turnbaugh, P.; Lozupone, C.A.; Knight, R.D.; Gordon, J.I. Obesity alters gut microbial ecology. Proc. Natl. Acad. Sci. USA 2005, 102, 11070–11075. [Google Scholar] [CrossRef] [Green Version]
- Turnbaugh, P.J.; Bäckhed, F.; Fulton, L.; Gordon, J.I. Diet-Induced Obesity Is Linked to Marked but Reversible Alterations in the Mouse Distal Gut Microbiome. Cell Host Microbe 2008, 3, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ley, R.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Human gut microbes associated with obesity. Nat. Cell Biol. 2006, 444, 1022–1023. [Google Scholar] [CrossRef]
- Laigaard, A.; Krych, L.; Zachariassen, L.F.; Ellegaard-Jensen, L.; Nielsen, D.S.; Hansen, A.K.; Hansen, C.H.F. Dietary prebiotics promote intestinal Prevotella in association with a low-responding phenotype in a murine oxazolone-induced model of atopic dermatitis. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Zhang, X.; Fang, Z.; Zhang, C.; Xia, H.; Jie, Z.; Han, X.; Chen, Y.; Ji, L. Effects of Acarbose on the Gut Microbiota of Prediabetic Patients: A Randomized, Double-blind, Controlled Crossover Trial. Diabetes Ther. 2017, 8, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Van De Laar, F.A.; Lucassen, P.L.; Akkermans, R.P.; Van De Lisdonk, E.H.; Rutten, G.E.; Van Weel, C. Glucosidase Inhibitors for Patients with Type 2 Diabetes: Results from a Cochrane systematic review and meta-analysis. Diabetes Care 2004, 28, 154–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
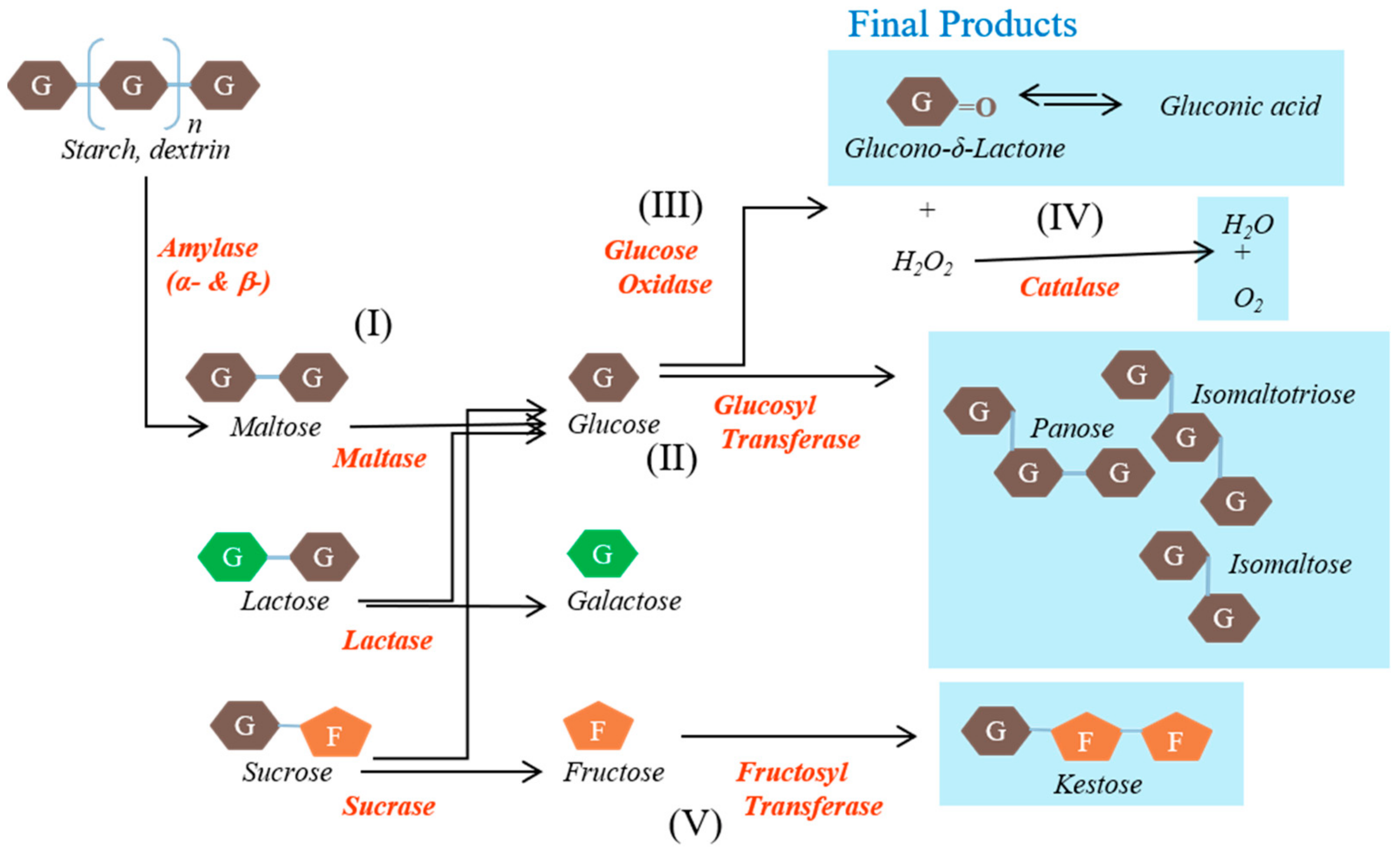
| Enzyme | Reaction Step(s) | Origin | Activity (U/mg) |
|---|---|---|---|
| Glucose oxidase | (III) | Aspergillus niger | 25 |
| Glucosyl transferase | (I) and (II) | Aspergillus niger | 7.5 |
| Fructosyl transferase | (I) and (V) | Aspergillus niger | 0.25 |
| Catalase | (IV) | Aspergillus niger | 125 |
| Amylase | (I) | Aspergillus oryzae | 1.25 |
| Lactase | (I) | Aspergillus niger | 1 |
| Biochemical Analyte | Control | Voglibose | EM |
|---|---|---|---|
| Total cholesterol (mg/dL) | 83.00 ± 8.21 | 58.29 ± 3.06 * | 75.29 ± 9.91 |
| High-density lipoprotein (mg/dL) | 52.63 ± 5.38 | 43.46 ± 2.63 | 54.24 ± 7.62 |
| Low-density lipoprotein (mg/dL) | 19.50 ± 3.61 | 12.43 ± 0.78 | 13.14 ± 1.20 |
| Triglycerides (mg/dL) | 124.50 ± 13.76 | 88.29 ± 6.64 * | 91.14 ± 6.34 * |
| Aspartate aminotransferase (U/L) | 80.80 ± 6.83 | 82.41 ± 7.81 | 89.70 ± 9.75 |
| Alanine aminotransferase (U/L) | 49.97 ± 4.57 | 57.56 ± 4.19 | 61.10 ± 7.22 |
| Creatinine (mg/dL) | 0.29 ± 0.01 | 0.25 ± 0.03 | 0.28 ± 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Yu, J.; Wang, E.K.; Lee, S.; Kim, J.S.; Hwang, J.; Ku, C.R.; Cho, Y.H.; Lee, E.J. Potential of an Enzyme Mixture of Glucose Oxidase, Glucosyl Transferase, and Fructosyl Transferase as an Antidiabetic Medicine. Biomedicines 2021, 9, 745. https://doi.org/10.3390/biomedicines9070745
Kim D, Yu J, Wang EK, Lee S, Kim JS, Hwang J, Ku CR, Cho YH, Lee EJ. Potential of an Enzyme Mixture of Glucose Oxidase, Glucosyl Transferase, and Fructosyl Transferase as an Antidiabetic Medicine. Biomedicines. 2021; 9(7):745. https://doi.org/10.3390/biomedicines9070745
Chicago/Turabian StyleKim, Daham, Juyeon Yu, Eun Kyung Wang, Soohyun Lee, Jung Seung Kim, Jihwan Hwang, Cheol Ryong Ku, Yoon Hee Cho, and Eun Jig Lee. 2021. "Potential of an Enzyme Mixture of Glucose Oxidase, Glucosyl Transferase, and Fructosyl Transferase as an Antidiabetic Medicine" Biomedicines 9, no. 7: 745. https://doi.org/10.3390/biomedicines9070745
APA StyleKim, D., Yu, J., Wang, E. K., Lee, S., Kim, J. S., Hwang, J., Ku, C. R., Cho, Y. H., & Lee, E. J. (2021). Potential of an Enzyme Mixture of Glucose Oxidase, Glucosyl Transferase, and Fructosyl Transferase as an Antidiabetic Medicine. Biomedicines, 9(7), 745. https://doi.org/10.3390/biomedicines9070745