
Multi-Aspect Optoacoustic Imaging of Breast Tumors under Chemotherapy with Exogenous and Endogenous Contrasts: Focus on Apoptosis and Hypoxia

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
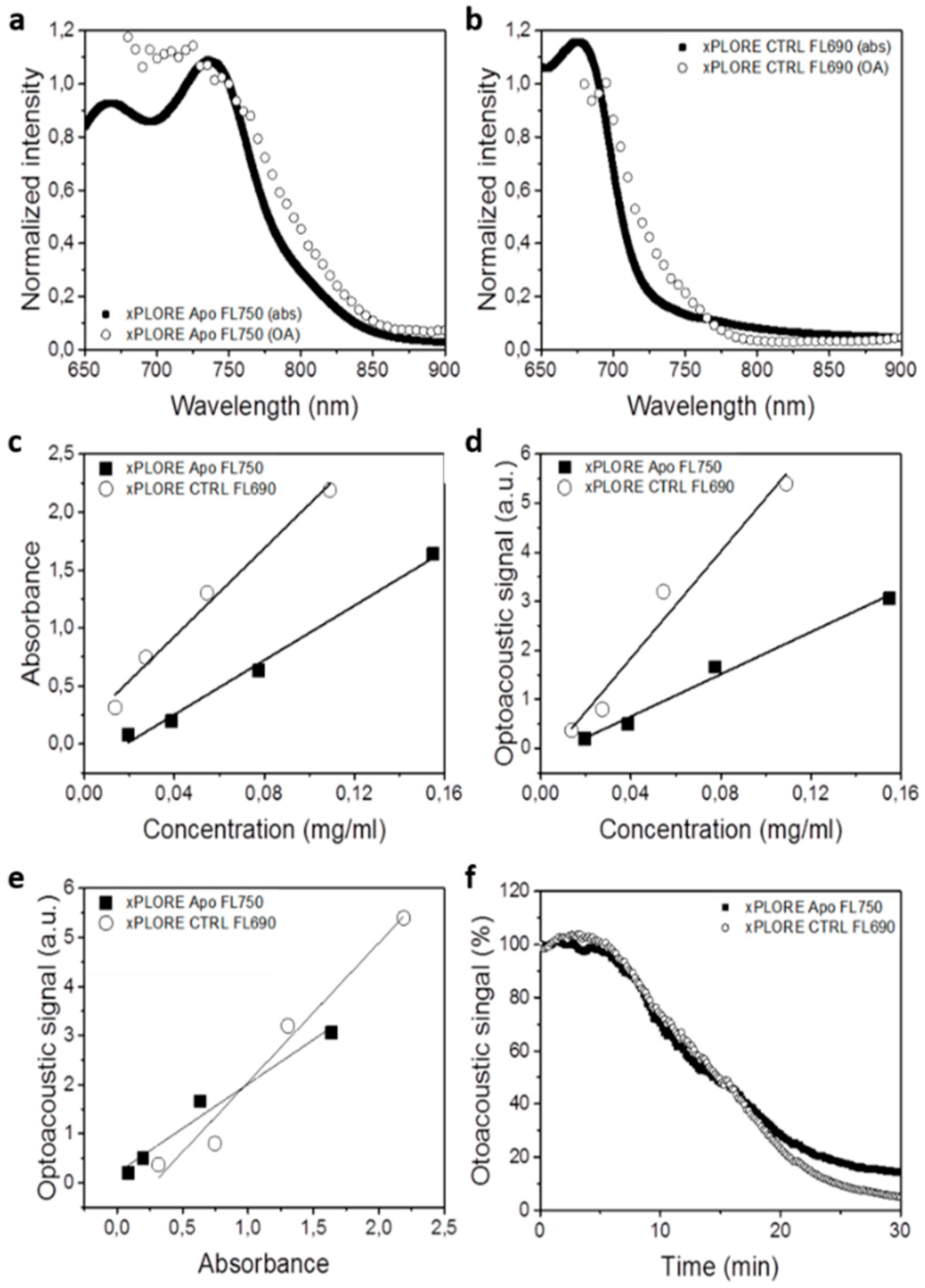
2.1. In Vitro Characterization of Exogenous Contrast Agents
2.2. Animal Handling
2.3. MSOT Setup, In Vivo Measurements and Data Analysis
2.4. Ex Vivo Fluorescence Cryoimaging
3. Results
3.1. xPLORE-Apo-FL750© as Optoacoustic Contrast Agent to Monitor Apoptosis
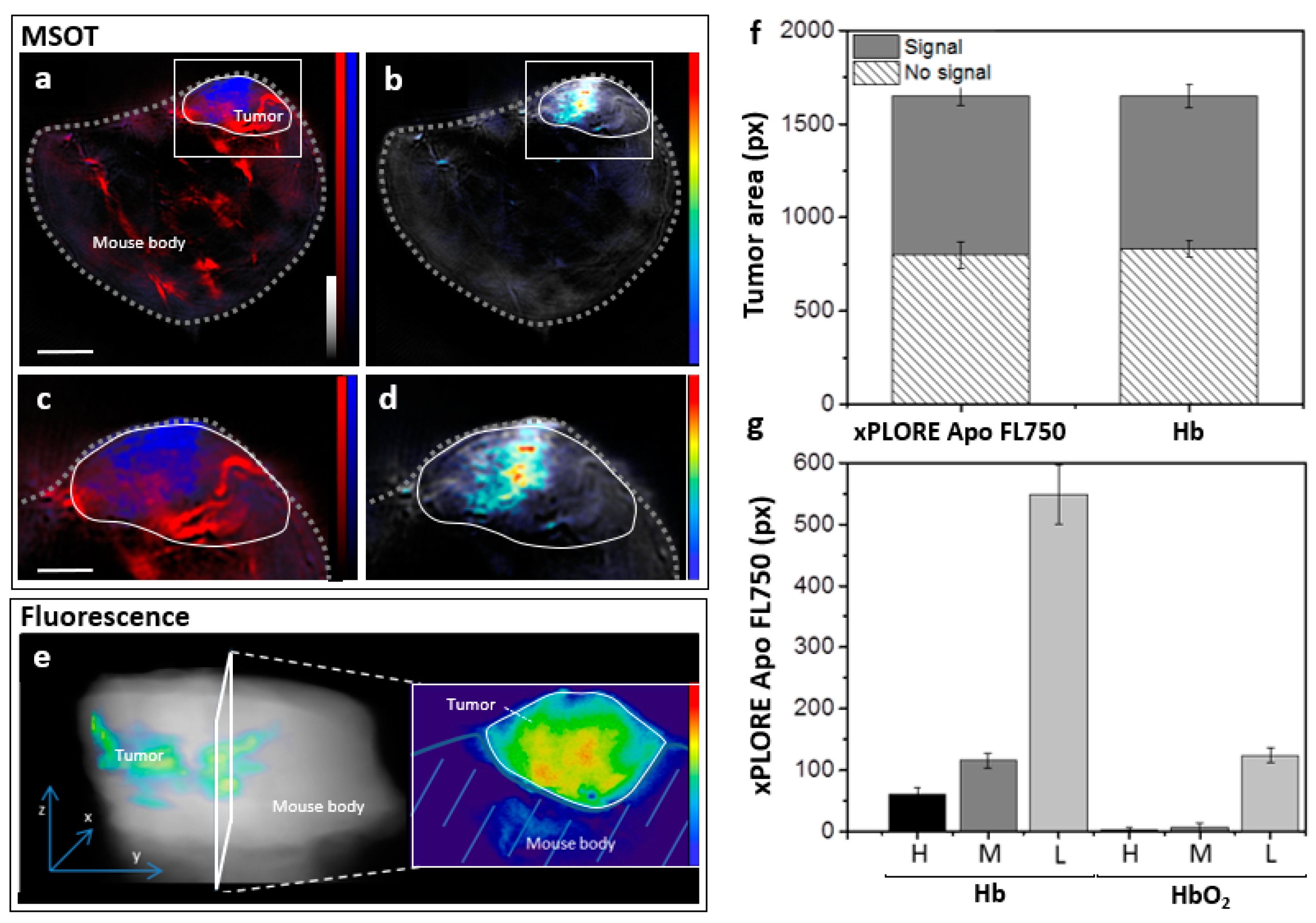
3.2. MSOT Imaging of Intratumoral Apoptosis and Hypoxia In Vivo
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elmi, A.; McDonald, E.S.; Mankoff, D. Imaging Tumor Proliferation in Breast Cancer: Current Update on Predictive Imaging Biomarkers. PET Clin. 2018, 13, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Filho, A.L.; Lopes, J.M.; Schmitt, F.C. Angiogenesis and breast cancer. J. Oncol. 2010, 2010, 576384. [Google Scholar] [CrossRef]
- DeNardo, D.G.; Coussens, L.M. Inflammation and breast cancer. Balancing immune response: Crosstalk between adaptive and innate immune cells during breast cancer progression. Breast Cancer Res. 2007, 9, 212. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. The hypoxic tumor microenvironment: A driving force for breast cancer progression. Biochim. Biophys. Acta (BBA)—Mol. Cell Res. 2016, 1863, 382–391. [Google Scholar] [CrossRef]
- Parton, M.; Dowsett, M.; Smith, I. Studies of apoptosis in breast cancer. BMJ 2001, 322, 1528–1532. [Google Scholar] [CrossRef]
- Desmedt, C.; Haibe-Kains, B.; Wirapati, P.; Buyse, M.; Larsimont, D.; Bontempi, G.; Delorenzi, M.; Piccart-Gebhart, M.; Sotiriou, C. Biological Processes Associated with Breast Cancer Clinical Outcome Depend on the Molecular Subtypes. Clin. Cancer Res. 2008, 14, 5158–5165. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Cochet, A.; Humbert, O.; Alberini, J.-L.; Hindié, E.; Mankoff, D. 18F-FDG PET/CT for Staging and Restaging of Breast Cancer. J. Nucl. Med. 2016, 57, 17S–26S. [Google Scholar] [CrossRef] [PubMed]
- Goorts, B.; Vöö, S.; Van Nijnatten, T.J.A.; Kooreman, L.F.S.; De Boer, M.; Keymeulen, K.B.M.I.; Aarnoutse, R.; Wildberger, J.E.; Mottaghy, F.M.; Lobbes, M.B.I.; et al. Hybrid 18F–FDG PET/MRI might improve locoregional staging of breast cancer patients prior to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1796–1805. [Google Scholar] [CrossRef]
- Xu, G.; Lin, Q.; Lian, L.; Qian, Y.; Lu, L.; Zhang, Z. CT/FMT dual-model imaging of breast cancer based on peptide-lipid nanoparticles. Biophotonics Immune Responses XI 2016, 9709, 97090. [Google Scholar]
- Park, E.K.; Lee, K.-S.; Seo, B.K.; Cho, K.R.; Woo, O.H.; Son, G.S.; Lee, H.Y.; Chang, Y.W. Machine Learning Approaches to Radiogenomics of Breast Cancer using Low-Dose Perfusion Computed Tomography: Predicting Prognostic Biomarkers and Molecular Subtypes. Sci. Rep. 2019, 9, 17847. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Chen, C.; Axel, L. Fast multi-contrast MRI reconstruction. Magn. Reson. Imaging 2014, 32, 1344–1352. [Google Scholar] [CrossRef]
- Mawlawi, O.; Erasmus, J.J.; Munden, R.F.; Pan, T.; Knight, A.E.; Macapinlac, H.A.; Podoloff, N.A.; Chasen, M. Quantifying the Effect of IV Contrast Media on Integrated PET/CT: Clinical Evaluation. Am. J. Roentgenol. 2006, 186, 308–319. [Google Scholar] [CrossRef]
- Lois, C.; Bezrukov, I.; Schmidt, H.; Schwenzer, N.; Werner, M.K.; Kupferschläger, J.; Beyer, T. Effect of MR contrast agents on quantitative accuracy of PET in combined whole-body PET/MR imaging. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1756–1766. [Google Scholar] [CrossRef]
- Manohar, S.; Dantuma, M. Current and future trends in photoacoustic breast imaging. Photoacoustics 2019, 16, 100134. [Google Scholar] [CrossRef]
- Crane, L.M.A.; Themelis, G.; Pleijhuis, R.G.; Harlaar, N.J.; Sarantopoulos, A.; Arts, H.J.G.; van der Zee, A.G.J.; Ntziachristos, V.; van Dam, G.M. Intraoperative multispectral fluorescence imaging for the detection of the sentinel lymph node in cervical cancer: A novel concept. Mol. Imaging Biol. 2011, 13, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Aboughaleb, I.H.; Aref, M.H.; El-Sharkawy, Y.H. Hyperspectral imaging for diagnosis and detection of ex-vivo breast cancer. Photodiagn. Photodyn. Ther. 2020, 31, 101922. [Google Scholar] [CrossRef] [PubMed]
- Karlas, A.; Fasoula, N.-A.; Paul-Yuan, K.; Reber, J.; Kallmayer, M.; Bozhko, D.; Seeger, M.; Eckstein, H.-H.; Wildgruber, M.; Ntziachristos, V. Cardiovascular optoacoustics: From mice to men–A review. Photoacoustics 2019, 14, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Karlas, A.; Pleitez, M.A.; Aguirre, J.; Ntziachristos, V. Optoacoustic imaging in endocrinology and metabolism. Nat. Rev. Endocrinol. 2021, 17, 323–335. [Google Scholar] [CrossRef]
- Weber, J.; Beard, P.C.; Bohndiek, S. Contrast agents for molecular photoacoustic imaging. Nat. Methods 2016, 13, 639–650. [Google Scholar] [CrossRef]
- Liapis, E.; Klemm, U.; Karlas, A.; Reber, J.; Ntziachristos, V. Resolution of spatial and temporal heterogeneity in bevacizumab-treated breast tumors by eigenspectra multispectral optoacoustic tomography. Cancer Res. 2020, 80, 5291–5304. [Google Scholar] [CrossRef]
- Knieling, F.; Neufert, C.; Hartmann, A.; Claussen, J.; Urich, A.; Egger, C.; Vetter, M.; Fischer, S.; Pfeifer, L.; Hagel, A.; et al. Multispectral Optoacoustic Tomography for Assessment of Crohn’s Disease Activity. N. Engl. J. Med. 2017, 376, 1292–1294. [Google Scholar] [CrossRef]
- Masthoff, M.; Helfen, A.; Claussen, J.; Karlas, A.; Markwardt, N.A.; Ntziachristos, V.; Eisenblätter, M.; Wildgruber, M. Use of Multispectral Optoacoustic Tomography to Diagnose Vascular Malformations. JAMA Dermatol. 2018, 154, 1457–1462. [Google Scholar] [CrossRef] [PubMed]
- Roll, W.; Markwardt, N.A.; Masthoff, M.; Helfen, A.; Claussen, J.; Eisenblätter, M.; Hasenbach, A.; Hermann, S.; Karlas, A.; Wildgruber, M.; et al. Multispectral Optoacoustic Tomography of Benign and Malignant Thyroid Disorders: A Pilot Study. J. Nucl. Med. 2019, 60, 1461–1466. [Google Scholar] [CrossRef]
- Regensburger, A.P.; Fonteyne, L.M.; Jüngert, J.; Wagner, A.L.; Gerhalter, T.; Nagel, A.M.; Heiss, R.; Flenkenthaler, F.; Qurashi, M.; Neurath, M.F.; et al. Detection of collagens by multispectral optoacoustic tomography as an imaging biomarker for Duchenne muscular dystrophy. Nat. Med. 2019, 25, 1905–1915. [Google Scholar] [CrossRef]
- Karlas, A.; Kallmayer, M.; Fasoula, N.; Liapis, E.; Bariotakis, M.; Krönke, M.; Ms, M.A.; Reber, J.; Eckstein, H.; Ntziachristos, V. Multispectral optoacoustic tomography of muscle perfusion and oxygenation under arterial and venous occlusion: A human pilot study. J. Biophotonics 2020, 13, e201960169. [Google Scholar] [CrossRef]
- Li, Y.; Schnabl, K.; Gabler, S.-M.; Willershäuser, M.; Reber, J.; Karlas, A.; Laurila, S.; Lahesmaa, M.; U-Din, M.; Bast-Habersbrunner, A.; et al. Secretin-Activated Brown Fat Mediates Prandial Thermogenesis to Induce Satiation. Cell 2018, 175, 1561–1574.e12. [Google Scholar] [CrossRef] [PubMed]
- Reber, J.; Willershäuser, M.; Karlas, A.; Paul-Yuan, K.; Diot, G.; Franz, D.; Fromme, T.; Ovsepian, S.V.; Beziere, N.; Dubikovskaya, E.; et al. Non-invasive Measurement of Brown Fat Metabolism Based on Optoacoustic Imaging of Hemoglobin Gradients. Cell Metab. 2018, 27, 689–701.e4. [Google Scholar] [CrossRef] [PubMed]
- Karlas, A.; Masthoff, M.; Kallmayer, M.; Helfen, A.; Bariotakis, M.; Fasoula, N.A.; Schäfers, M.; Seidensticker, M.; Eckstein, H.-H.; Ntziachristos, V.; et al. Multispectral optoacoustic tomography of peripheral arterial disease based on muscle hemoglobin gradients—a pilot clinical study. Ann. Transl. Med. 2021, 9, 36. [Google Scholar] [CrossRef]
- Fasoula, N.-A.; Karlas, A.; Kallmayer, M.; Milik, A.B.; Pelisek, J.; Eckstein, H.-H.; Klingenspor, M.; Ntziachristos, V. Multicompartmental Non-invasive Sensing of Postprandial Lipemia in Humans with Multispectral Optoacoustic Tomography. Mol. Metab. 2021, 47, 101184. [Google Scholar] [CrossRef]
- Karlas, A.; Kallmayer, M.; Bariotakis, M.; Fasoula, N.A.; Liapis, E.; Hyafil, F.; Pelisek, J.; Wildgruber, M.; Eckstein, H.H.; Ntziachristos, V. Multispectral optoacoustic tomography of lipid and hemoglobin contrast in human carotid atherosclerosis. Photoacoustics 2021, 23, 100283. [Google Scholar] [CrossRef]
- CLiu, C.; Gong, X.; Lin, R.; Liu, F.; Chen, J.; Wang, Z.; Song, L.; Chu, J. Advances in Imaging Techniques and Genetically Encoded Probes for Photoacoustic Imaging. Theranostics 2016, 6, 2414–2430. [Google Scholar]
- Laramie, M.D.; Smith, M.K.; Marmarchi, F.; McNally, L.R.; Henary, M. Small Molecule Optoacoustic Contrast Agents: An Unexplored Avenue for Enhancing In Vivo Imaging. Molecules 2018, 23, 2766. [Google Scholar] [CrossRef] [PubMed]
- Mishra, K.; Stankevych, M.; Fuenzalida-Werner, J.P.; Grassmann, S.; Gujrati, V.; Huang, Y.; Klemm, U.; Buchholz, V.R.; Ntziachristos, V.; Stiel, A.C. Multiplexed whole-animal imaging with reversibly switchable optoacoustic proteins. Sci. Adv. 2020, 6, eaaz6293. [Google Scholar] [CrossRef] [PubMed]
- Edgington-Mitchell, L.; Berger, A.B.; Blum, G.; Albrow, V.E.; Paulick, M.G.; Lineberry, N.; Bogyo, M. Noninvasive optical imaging of apoptosis by caspase-targeted activity-based probes. Nat. Med. 2009, 15, 967–973. [Google Scholar] [CrossRef]
- Tzoumas, S.; Zaremba, A.; Klemm, U.; Nunes, A.; Schaefer, K.; Ntziachristos, V. Immune cell imaging using multi-spectral optoacoustic tomography. Opt. Lett. 2014, 39, 3523–3526. [Google Scholar] [CrossRef]
- Tzoumas, S.; Nunes, A.; Olefir, I.; Stangl, S.; Symvoulidis, P.; Glasl, S.; Bayer, C.; Multhoff, G.; Ntziachristos, V. Eigenspectra optoacoustic tomography achieves quantitative blood oxygenation imaging deep in tissues. Nat. Commun. 2016, 7, 12121. [Google Scholar] [CrossRef]
- Razansky, D.; Bühler, A.; Ntziachristos, V. Volumetric real-time multispectral optoacoustic tomography of biomarkers. Nat. Protoc. 2011, 6, 1121–1129. [Google Scholar] [CrossRef]
- Wang, H.; Willershäuser, M.; Karlas, A.; Gorpas, D.; Reber, J.; Ntziachristos, V.; Maurer, S.; Fromme, T.; Li, Y.; Klingenspor, M. A dual Ucp1 reporter mouse model for imaging and quantitation of brown and brite fat recruitment. Mol. Metab. 2019, 20, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C.; Ozols, R.F.; Myers, C.E. The Anthracycline Antineoplastic Drugs. N. Engl. J. Med. 1981, 305, 139–153. [Google Scholar] [CrossRef]
- Call, J.A.; Eckhardt, S.G.; Camidge, D.R. Targeted manipulation of apoptosis in cancer treatment. Lancet Oncol. 2008, 9, 1002–1011. [Google Scholar] [CrossRef]
- Lopez-Neblina, F.; Toledo, A.H.; Toledo-Pereyra, L.H. Molecular Biology of Apoptosis in Ischemia and Reperfusion. J. Investig. Surg. 2005, 18, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Pope, R.M. The role of apoptosis in rheumatoid arthritis. Curr. Opin. Pharmacol. 2003, 3, 317–322. [Google Scholar] [CrossRef]
- Yang, Q.; Cui, H.; Cai, S.; Yang, X.; Forrest, M.L. In vivo photoacoustic imaging of chemotherapy-induced apoptosis in squamous cell carcinoma using a near-infrared caspase-9 probe. J. Biomed. Opt. 2011, 16, 116026–1160264. [Google Scholar] [CrossRef] [PubMed]
- Kannadorai, R.K.; Udumala, S.K.; Sidney, Y.W.K. Noninvasive in vivo multispectral optoacoustic imaging of apoptosis in triple negative breast cancer using indocyanine green conjugated phosphatidylserine monoclonal antibody. J. Biomed. Opt. 2016, 21, 126002. [Google Scholar] [CrossRef]
- Xie, B.; Tomaszewski, M.; Neves, A.; Ros, S.; Hu, D.; McGuire, S.; Mullins, S.; Tice, D.; Sainson, R.; Bohndiek, S.; et al. Optoacoustic detection of early therapy-induced tumor cell death using a targeted imaging agent. Clin. Cancer Res. 2017, 23, 6893–6903. [Google Scholar] [CrossRef]
- Buehler, A.; Herzog, E.; Ale, A.; Smith, B.D.; Ntziachristos, V.; Razansky, D. High resolution tumor targeting in living mice by means of multispectral optoacoustic tomography. EJNMMI Res. 2012, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, X.; Weng, J.; Li, J.; Fan, Q.; Zhang, Y.; Ye, D. A Photoacoustic Probe for the Imaging of Tumor Apoptosis by Caspase-Mediated Macrocyclization and Self-Assembly. Angew. Chem. Int. Ed. 2019, 58, 4886–4890. [Google Scholar] [CrossRef]
- Fesik, S.W. Promoting apoptosis as a strategy for cancer drug discovery. Nat. Rev. Cancer 2005, 5, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Igney, F.H.; Krammer, P.H. Death and anti-death: Tumour resistance to apoptosis. Nat. Rev. Cancer 2002, 2, 277–288. [Google Scholar] [CrossRef]
- Guo, K.; Searfoss, G.; Krolikowski, D.; Pagnoni, M.; Franks, C.; Clark, K.; Yu, K.T.; Jaye, M.; Ivashchenko, Y. Hypoxia induces the expression of the pro-apoptotic gene BNIP3. Cell Death Differ. 2001, 8, 367–376. [Google Scholar] [CrossRef]
- Greijer, A.E.; van der Wall, E. The role of hypoxia inducible factor 1 (HIF-1) in hypoxia induced apoptosis. J. Clin. Pathol. 2004, 57, 1009–1014. [Google Scholar] [CrossRef]
- Shimizu, S.; Eguchi, Y.; Kamiike, W.; Itoh, Y.; Hasegawa, J.; Yamabe, K.; Otsuki, Y.; Matsuda, H.; Tsujimoto, Y. Induction of apoptosis as well as necrosis by hypoxia and predominant prevention of apoptosis by Bcl-2 and Bcl-XL. Cancer Res. 1996, 56, 2161–2166. [Google Scholar]
- Marusyk, A.; Almendro, V.; Polyak, K. Intra-tumour heterogeneity: A looking glass for cancer? Nat. Rev. Cancer 2012, 12, 323–334. [Google Scholar] [CrossRef]
- Gerl, R.; Vaux, D.L. Apoptosis in the development and treatment of cancer. Carcinogenesis 2005, 26, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Ehemann, V.; Sykora, J.; Vera-Delgado, J.; Lange, A.; Otto, H.F. Flow cytometric detection of spontaneous apoptosis in human breast cancer using the TUNEL-technique. Cancer Lett. 2003, 194, 125–131. [Google Scholar] [CrossRef]
- Tewey, K.M.; Rowe, T.C.; Yang, L.; Halligan, B.D.; Liu, L.F. Adriamycin-Induced DNA Damage Mediated by Mammalian DNA Topoisomerase II. Science 1984, 226, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Keizer, H.G.; Pinedo, H.M.; Schuurhuis, G.J.; Joenje, H. Doxorubicin (adriamycin): A critical review of free radical-dependent mechanisms of cytotoxicity. Pharmacol. Ther. 1990, 47, 219–231. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlas, A.; Nunes, A.; Driessen, W.; Liapis, E.; Reber, J. Multi-Aspect Optoacoustic Imaging of Breast Tumors under Chemotherapy with Exogenous and Endogenous Contrasts: Focus on Apoptosis and Hypoxia. Biomedicines 2021, 9, 1696. https://doi.org/10.3390/biomedicines9111696
Karlas A, Nunes A, Driessen W, Liapis E, Reber J. Multi-Aspect Optoacoustic Imaging of Breast Tumors under Chemotherapy with Exogenous and Endogenous Contrasts: Focus on Apoptosis and Hypoxia. Biomedicines. 2021; 9(11):1696. https://doi.org/10.3390/biomedicines9111696
Chicago/Turabian StyleKarlas, Angelos, Antonio Nunes, Wouter Driessen, Evangelos Liapis, and Josefine Reber. 2021. "Multi-Aspect Optoacoustic Imaging of Breast Tumors under Chemotherapy with Exogenous and Endogenous Contrasts: Focus on Apoptosis and Hypoxia" Biomedicines 9, no. 11: 1696. https://doi.org/10.3390/biomedicines9111696
APA StyleKarlas, A., Nunes, A., Driessen, W., Liapis, E., & Reber, J. (2021). Multi-Aspect Optoacoustic Imaging of Breast Tumors under Chemotherapy with Exogenous and Endogenous Contrasts: Focus on Apoptosis and Hypoxia. Biomedicines, 9(11), 1696. https://doi.org/10.3390/biomedicines9111696