
Efficacy of Penile Low-Intensity Shockwave Therapy and Determinants of Treatment Response in Taiwanese Patients with Erectile Dysfunction

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Inclusion and Exclusion Criteria
2.3. Li-ESWT Protocol
2.4. Assessment of Li-ESWT Efficacy Using Erectile Function (EF) Indices
2.5. Li-ESWT Outcome Measurement
2.6. Statistical Analysis
3. Results
3.1. Taiwanese Patients with ED Are Mostly Older Than 45 Years and Present with Advanced Disease Severity
3.2. Li-ESWT Significantly Improves the Erectile Function of Taiwanese Patients Compared with Baseline
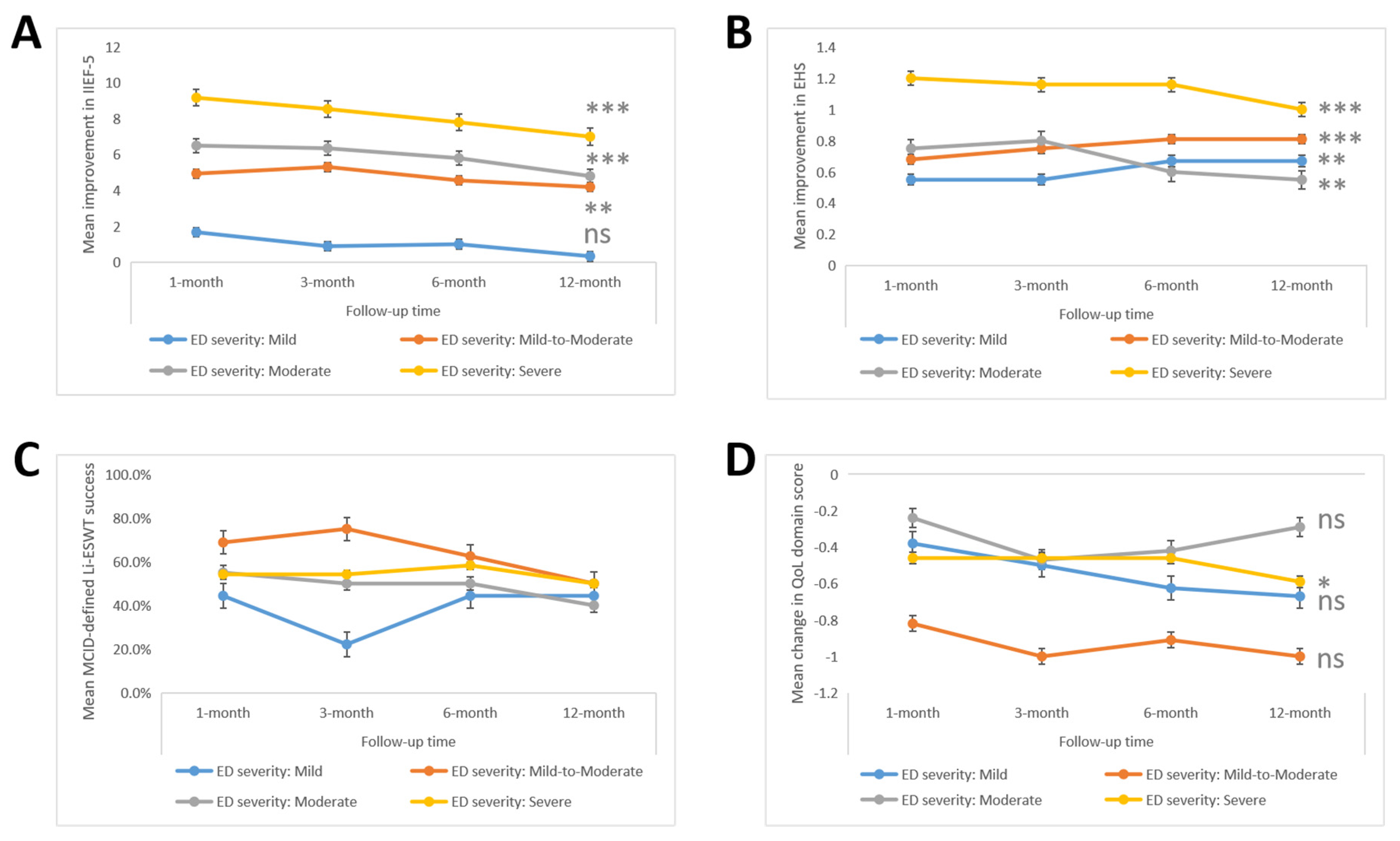
3.3. Taiwanese Patients with Advanced ED Severity Benefit More from the Therapeutic Effect of Li-ESWT, Compared with the Less Severe Cases
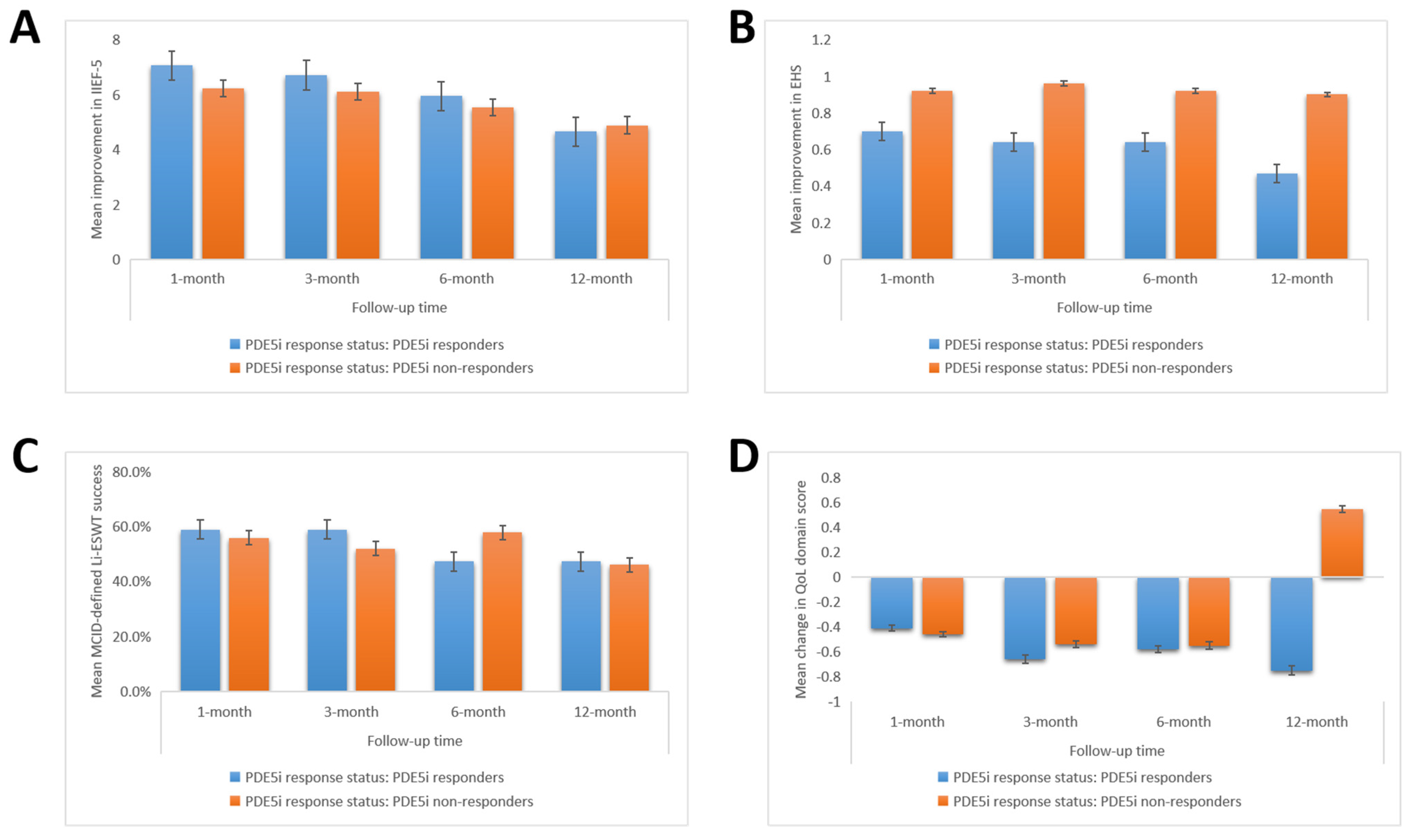
3.4. Li-ESWT Is Therapeutically Efficacious in Taiwanese Patients Regardless of Their PDE5i Response Status, Albeit Slightly More So among PDE5i Responders
3.5. Age > 45 Years and Uncontrolled Hyperlipidemia Are Independent Negative Predictors of Li-ESWT Response or Success in Taiwanese Patients with ED
4. Discussion
4.1. Limitations
4.2. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- Shamloul, R.; Ghanem, H. Erectile dysfunction. Lancet 2013, 381, 153–165. [Google Scholar] [CrossRef]
- Najari, B.B.; Kashanian, J.A. Erectile Dysfunction. JAMA 2016, 316, 1838. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.A.; Lie, J.D. Phosphodiesterase-5 (PDE5) Inhibitors in the Management of Erectile Dysfunction. Pharm. Ther. 2013, 38, 407–419. [Google Scholar]
- Moon, D.G. Evolution of Phosphodiesterase-5 Inhibitors. World J. Mens Health 2015, 33, 123–124. [Google Scholar] [CrossRef][Green Version]
- Matic, H.; McCabe, M.P. Duration of erectile dysfunction and its relationship to treatment seeking and satisfaction with treatment using PDE5 inhibitors. Int. J. Urol. 2008, 15, 346–349. [Google Scholar] [CrossRef]
- Porst, H. Review of the Current Status of Low Intensity Extracorporeal Shockwave Therapy (Li-ESWT) in Erectile Dysfunction (ED), Peyronie’s Disease (PD), and Sexual Rehabilitation After Radical Prostatectomy With Special Focus on Technical Aspects of the Different Marketed ESWT Devices Including Personal Experiences in 350 Patients. Sex. Med. Rev. 2021, 9, 93–122. [Google Scholar] [CrossRef]
- Vardi, Y.; Appel, B.; Jacob, G.; Massarwi, O.; Gruenwald, I. Can Low-Intensity Extracorporeal Shockwave Therapy Improve Erectile Function? A 6-Month Follow-up Pilot Study in Patients with Organic Erectile Dysfunction. Eur. Urol. 2010, 58, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Gruenwald, I.; Appel, B.; Vardi, Y. Low-Intensity Extracorporeal Shock Wave Therapy—A Novel Effective Treatment for Erectile Dysfunction in Severe ED Patients Who Respond Poorly to PDE5 Inhibitor Therapy. J. Sex. Med. 2012, 9, 259–264. [Google Scholar] [CrossRef]
- Tsai, C.-C.; Wang, C.-J.; Lee, Y.-C.; Kuo, Y.-T.; Lin, H.-H.; Li, C.-C.; Wu, W.J.; Liu, C.-C. Low-Intensity Extracorporeal Shockwave Therapy Can Improve Erectile Function in Patients Who Failed to Respond to Phosphodiesterase Type 5 Inhibitors. Am. J. Mens Health 2017, 11, 1781–1790. [Google Scholar] [CrossRef]
- Wu, S.S.; Ericson, K.J.; Shoskes, D.A. Retrospective comparison of focused shockwave therapy and radial wave therapy for men with erectile dysfunction. Transl. Androl. Urol. 2020, 9, 2122–2128. [Google Scholar] [CrossRef]
- Sokolakis, I.; Dimitriadis, F.; Psalla, D.; Karakiulakis, G.; Kalyvianakis, D.; Hatzichristou, D. Effects of low-intensity shock wave therapy (LiST) on the erectile tissue of naturally aged rats. Int. J. Impot. Res. 2019, 31, 162–169. [Google Scholar] [CrossRef]
- Drury, R.; Natale, C.; Hellstrom, W.J.G. Reviewing the evidence for shockwave- and cell-based regenerative therapies in the treatment of erectile dysfunction. Ther. Adv. Urol. 2021, 13, 17562872211002059. [Google Scholar] [CrossRef]
- Capogrosso, P.; Frey, A.; Jensen, C.F.S.; Rastrelli, G.; Russo, G.I.; Torremade, J.; Albersen, M.; Gruenwald, I.; Reisman, Y.; Corona, G. Low-Intensity Shock Wave Therapy in Sexual Medicine—Clinical Recommendations from the European Society of Sexual Medicine (ESSM). J. Sex. Med. 2019, 16, 1490–1505. [Google Scholar] [CrossRef] [PubMed]
- Schoofs, E.; Fode, M.; Capogrosso, P.; Albersen, M. for the European Association of Urology Young Academic Urologists (EAU-YAU) Men’s Health Group. Current guideline recommendations and analysis of evidence quality on low-intensity shockwave therapy for erectile dysfunction. Int. J. Impot. Res. 2019, 31, 209–217. [Google Scholar] [CrossRef]
- Neijenhuijs, K.I.; Holtmaat, K.; Aaronson, N.K.; Holzner, B.; Terwee, C.B.; Cuijpers, P.; Leeuw, I.M.V.-D. The International Index of Erectile Function (IIEF)—A Systematic Review of Measurement Properties. J. Sex. Med. 2019, 16, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Parisot, J.; Yiou, R.; Salomon, L.; de la Taille, A.; Lingombet, O.; Audureau, E. Erection Hardness Score for the Evaluation of Erectile Dysfunction: Further Psychometric Assessment in Patients Treated by Intracavernous Prostaglandins Injections after Radical Prostatectomy. J. Sex. Med. 2014, 11, 2109–2118. [Google Scholar] [CrossRef]
- Maltenfort, M.G. The Minimally Important Clinical Difference. Clin. Spine Surg. 2016, 29, 383. [Google Scholar] [CrossRef]
- Rosen, R.C.; Allen, K.R.; Ni, X.; Araujo, A.B. Minimal Clinically Important Differences in the Erectile Function Domain of the International Index of Erectile Function Scale. Eur. Urol. 2011, 60, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and Its Medical and Psychosocial Correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef]
- Hall, S.A.; Kupelian, V.; Rosen, R.C.; Travison, T.G.; Link, C.L.; Miner, M.M.; Ganz, P.; McKinlay, J.B. Is Hyperlipidemia or Its Treatment Associated with Erectile Dysfunction?: Results from the Boston Area Community Health (BACH) Survey. J. Sex. Med. 2009, 6, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Hisasue, S.-I.; China, T.; Horiuchi, A.; Kimura, M.; Saito, K.; Isotani, S.; Ide, H.; Muto, S.; Yamaguchi, R.; Horie, S. Impact of aging and comorbidity on the efficacy of low-intensity shock wave therapy for erectile dysfunction. Int. J. Urol. 2015, 23, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; McBain, H.; Amirova, A.; Newman, S.; Mulligan, K. Men’s beliefs about treatment for erectile dysfunction—what influences treatment use? A systematic review. Int. J. Impot. Res. 2020, 33, 1–27. [Google Scholar] [CrossRef]
- Mobley, D.F.; Khera, M.; Baum, N. Recent advances in the treatment of erectile dysfunction. Postgrad. Med. J. 2017, 93, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Rizk, P.J.; Krieger, J.R.; Kohn, T.P.; Pastuszak, A.W. Low-Intensity Shockwave Therapy for Erectile Dysfunction. Sex. Med. Rev. 2018, 6, 624–630. [Google Scholar] [CrossRef]
- Spivak, L.; Shultz, T.; Appel, B.; Verze, P.; Yagudaev, D.; Vinarov, A. Low-Intensity Extracorporeal Shockwave Therapy for Erectile Dysfunction in Diabetic Patients. Sex. Med. Rev. 2021, 9, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Srini, V.S.; Reddy, R.K.; Shultz, T.; Denes, B. Low intensity extracorporeal shockwave therapy for erectile dysfunction: A study in an Indian population. Can. J. Urol. 2015, 22, 7614–7622. [Google Scholar]
- Lee, R.K.; Chughtai, B.; Te, A.E.; Kaplan, S.A. Sexual Function in Men with Metabolic Syndrome. Urol. Clin. N. Am. 2012, 39, 53–62. [Google Scholar] [CrossRef]
- Cohen, S.D. The Challenge of Erectile Dysfunction Management in the Young Man. Curr. Urol. Rep. 2015, 16, 1–9. [Google Scholar] [CrossRef]
- Vita, R.; Benvenga, S.; Giammusso, B.; La Vignera, S. Determinants of Early Response to Low-Intensity Extracorporeal Shockwaves for the Treatment of Vasculogenic Erectile Dysfunction: An Open-Label, Prospective Study. J. Clin. Med. 2019, 8, 1017. [Google Scholar] [CrossRef] [PubMed]
- Mata, D.A.; Katchi, F.M.; Ramasamy, R. Precision Medicine and Men’s Health. Am. J. Men’s Health 2017, 11, 1124–1129. [Google Scholar] [CrossRef]
- Bivalacqua, T.J.; Usta, M.F.; Champion, H.C.; Kadowitz, P.J.; Hellstrom, W.J.G. Endothelial Dysfunction in Erectile Dysfunction: Role of the Endothelium in Erectile Physiology and Disease. J. Androl. 2003, 24, S17–S37. [Google Scholar] [CrossRef]
- Ferrini, M.G.; Gonzalez-Cadavid, N.F.; Rajfer, J. Aging related erectile dysfunction—potential mechanism to halt or delay its onset. Transl. Androl. Urol. 2017, 6, 20–27. [Google Scholar] [CrossRef]
- Blick, C.; Ritchie, R.; Sullivan, M. Is Erectile Dysfunction an Example of Abnormal Endothelial Function? Curr. Vasc. Pharmacol. 2016, 14, 163–167. [Google Scholar] [CrossRef]
- Konstantinovsky, A.; Tamir, S.; Katz, G.; Tzischinsky, O.; Kuchersky, N.; Blum, N.; Blum, A. Erec-tile Dysfunction, Sleep Disorders, and Endothelial Function. Isr. Med. Assoc. J. 2019, 21, 408–411. [Google Scholar] [PubMed]
- Vilahur, G.; Badimon, L. Dyslipidemias and Microcirculation. Curr. Pharm. Des. 2018, 24, 2921–2926. [Google Scholar] [CrossRef]
- Mitidieri, E.; Cirino, G.; Bianca, R.D.D.V.; Sorrentino, R. Pharmacology and perspectives in erectile dysfunction in man. Pharmacol. Ther. 2020, 208, 107493. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.-J.; Cai, X.; Tian, Y.; Wu, T.; Cao, C.-X.; Bu, S.-Y. The role of statins in erectile dysfunction: A systematic review and meta-analysis. Asian J. Androl. 2014, 16, 461–466. [Google Scholar] [CrossRef]
- Chung, E.; Cartmill, R. Evaluation of clinical efficacy, safety and patient satisfaction rate after low-intensity extracorporeal shockwave therapy for the treatment of male erectile dysfunction: An Australian first open-label single-arm prospective clinical trial. BJU Int. 2015, 115, 46–49. [Google Scholar] [CrossRef]
- Fojecki, G.L.; Tiessen, S.; Osther, P.J. Effect of Low-Energy Linear Shockwave Therapy on Erectile Dysfunction—A Double-Blinded, Sham-Controlled, Randomized Clinical Trial. J. Sex. Med. 2017, 14, 106–112. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age (years, median (Q1–Q3)) | 55 (45–66) |
| Body mass index (kg/m2, median (SD)) | 24.6 (3.89) |
| Baseline erectile function, median (SD) | |
| EHS | 2.0 (0.80) |
| IIEF-5 | 10 (5.54) |
| ED Severity, n (%) | |
| Mild (IIEF-5 score: 17–21) | 6 (8.6%) |
| Mild-to-Moderate (IIEF-5 score: 12–16) | 16 (23.2%) |
| Moderate (IIEF-5 score: 8–11) | 20 (29%) |
| Severe (IIEF-5 score: 5–7) | 24 (34.8%) |
| Duration of ED (months, median (Q1–Q3)) | 12 (6–36) |
| PDE5i non-responders, n (%) | 52 (75.4%) |
| Testosterone level (ng/dL, mean (SD)) | 3.92 (1.45) |
| Co-morbidity, n (%) | |
| Diabetes mellitus | 29 (42%) |
| Hypertension | 16 (23.2%) |
| Hyperlipidemia | 33 (47.8%) |
| Chronic kidney disease | 9 (13%) |
| Hypogonadism | 21 (30.4%) |
| Tobacco smoking, n (%) | 7 (10.1%) |
| Erectile Function Index | Change from Baseline | |
|---|---|---|
| Mean (95% CI) | p-Value | |
| 1 month follow-up | ||
| IIEF-5 | 6.65 (5.30–7.99) | <0.001 |
| EHS | 0.88 (0.67–1.09) | <0.001 |
| QoL | −0.45 (−0.74–−0.16) | 0.003 |
| Success * n (%) | 39 (56.5%) | |
| 3 months follow-up | ||
| IIEF-5 | 6.37 (5.08–7.67) | <0.001 |
| EHS | 0.89 (0.69–1.10) | <0.001 |
| QoL | −0.57 (−0.83–−0.30) | <0.001 |
| Success * n (%) | 37 (53.6%) | |
| 6 months follow-up | ||
| IIEF-5 | 5.79 (4.46–7.12) | <0.001 |
| EHS | 0.86 (0.64–1.09) | <0.001 |
| QoL | −0.56(−0.83–−0.29) | <0.001 |
| Success * n (%) | 38 (55.1%) | |
| 12 months follow-up | ||
| IIEF-5 | 5.10 (3.65–6.55) | <0.001 |
| EHS | 0.80 (0.58–1.03) | <0.001 |
| QoL | −0.59 (−0.86–−0.32) | <0.001 |
| Success * n (%) | 32 (46.4%) | |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Odds Ratio | p-Value | Odds Ratio | p-Value | |
| Age (>45 years) | 0.27 | 0.04 * | 0.24 | 0.04 * |
| BMI (kg/m2) | 0.90 | 0.25 | ||
| Tobacco smoking | 1.30 | 0.28 | ||
| Hypogonadism | 0.63 | 0.40 | ||
| Hypertension | 0.71 | 0.54 | ||
| Diabetes mellitus | 0.43 | 0.09 | ||
| Diabetes mellitus (uncontrolled) | 0.17 | 0.04 * | 0.21 | 0.08 |
| Hyperlipidemia | 0.53 | 0.19 | ||
| Hyperlipidemia (uncontrolled) | 0.25 | 0.01 ** | 0.27 | 0.03 * |
| Severe and moderate ED | 0.56 | 0.27 | ||
| Duration of ED (>2 year) | 0.54 | 0.38 | ||
| EHS < 3 | 0.62 | 0.37 | ||
| PDE5i non-responders | 0.88 | 0.83 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzou, K.-Y.; Hu, S.-W.; Bamodu, O.A.; Wang, Y.-H.; Wu, W.-L.; Wu, C.-C. Efficacy of Penile Low-Intensity Shockwave Therapy and Determinants of Treatment Response in Taiwanese Patients with Erectile Dysfunction. Biomedicines 2021, 9, 1670. https://doi.org/10.3390/biomedicines9111670
Tzou K-Y, Hu S-W, Bamodu OA, Wang Y-H, Wu W-L, Wu C-C. Efficacy of Penile Low-Intensity Shockwave Therapy and Determinants of Treatment Response in Taiwanese Patients with Erectile Dysfunction. Biomedicines. 2021; 9(11):1670. https://doi.org/10.3390/biomedicines9111670
Chicago/Turabian StyleTzou, Kai-Yi, Su-Wei Hu, Oluwaseun Adebayo Bamodu, Yuan-Hung Wang, Wen-Ling Wu, and Chia-Chang Wu. 2021. "Efficacy of Penile Low-Intensity Shockwave Therapy and Determinants of Treatment Response in Taiwanese Patients with Erectile Dysfunction" Biomedicines 9, no. 11: 1670. https://doi.org/10.3390/biomedicines9111670
APA StyleTzou, K.-Y., Hu, S.-W., Bamodu, O. A., Wang, Y.-H., Wu, W.-L., & Wu, C.-C. (2021). Efficacy of Penile Low-Intensity Shockwave Therapy and Determinants of Treatment Response in Taiwanese Patients with Erectile Dysfunction. Biomedicines, 9(11), 1670. https://doi.org/10.3390/biomedicines9111670