
Oral Mucositis in Cancer and Potential Use of Omega-3 Free Fatty Acids in Its Management: A Review



Abstract
1. Introduction
2. Incidence and Risk Assessment
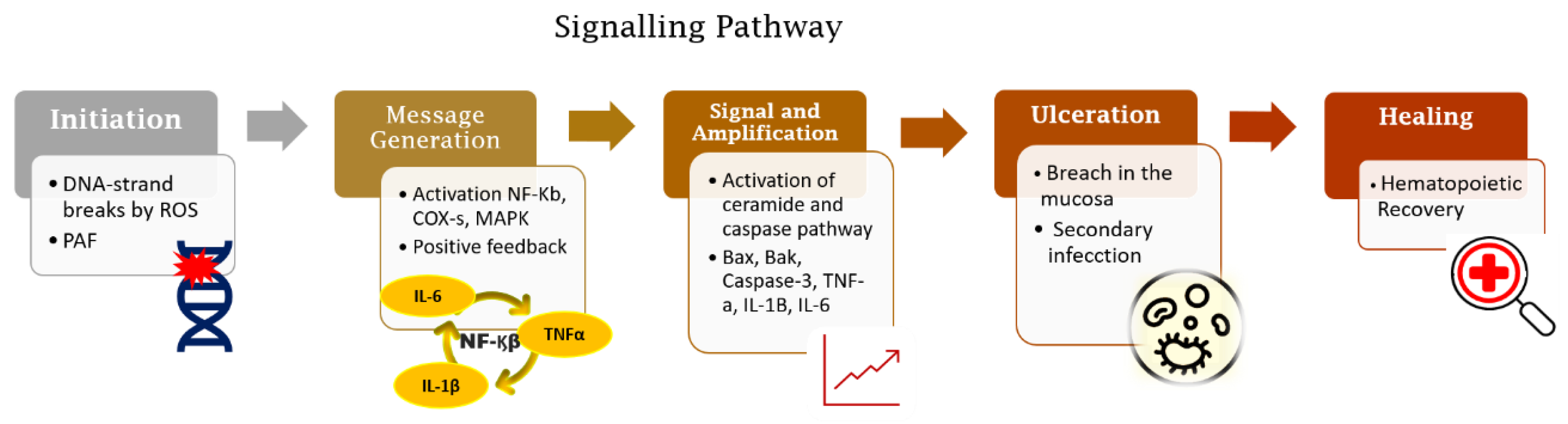
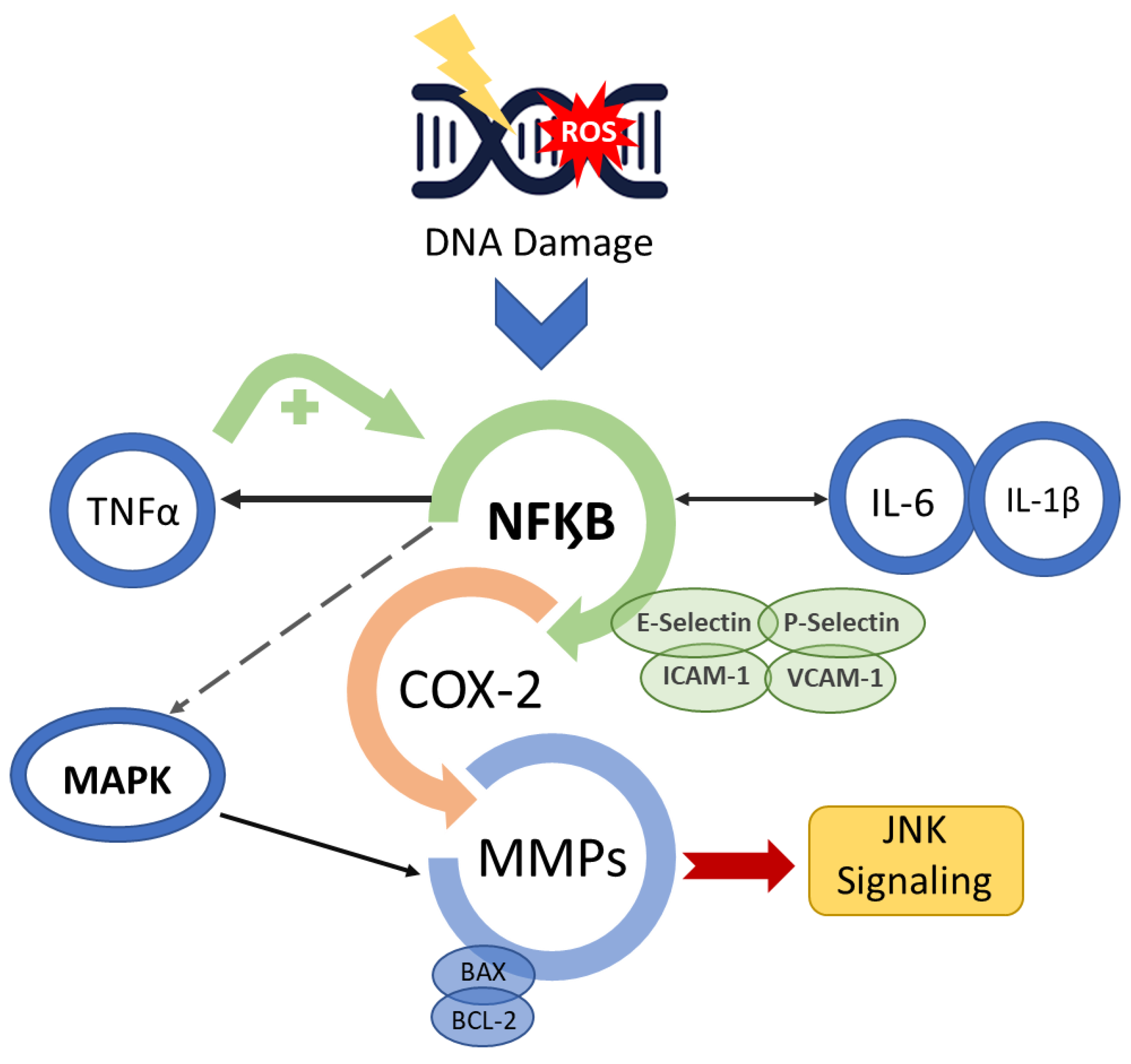
3. Biomolecular Mechanisms of OM
4. Prevention and Management Strategies
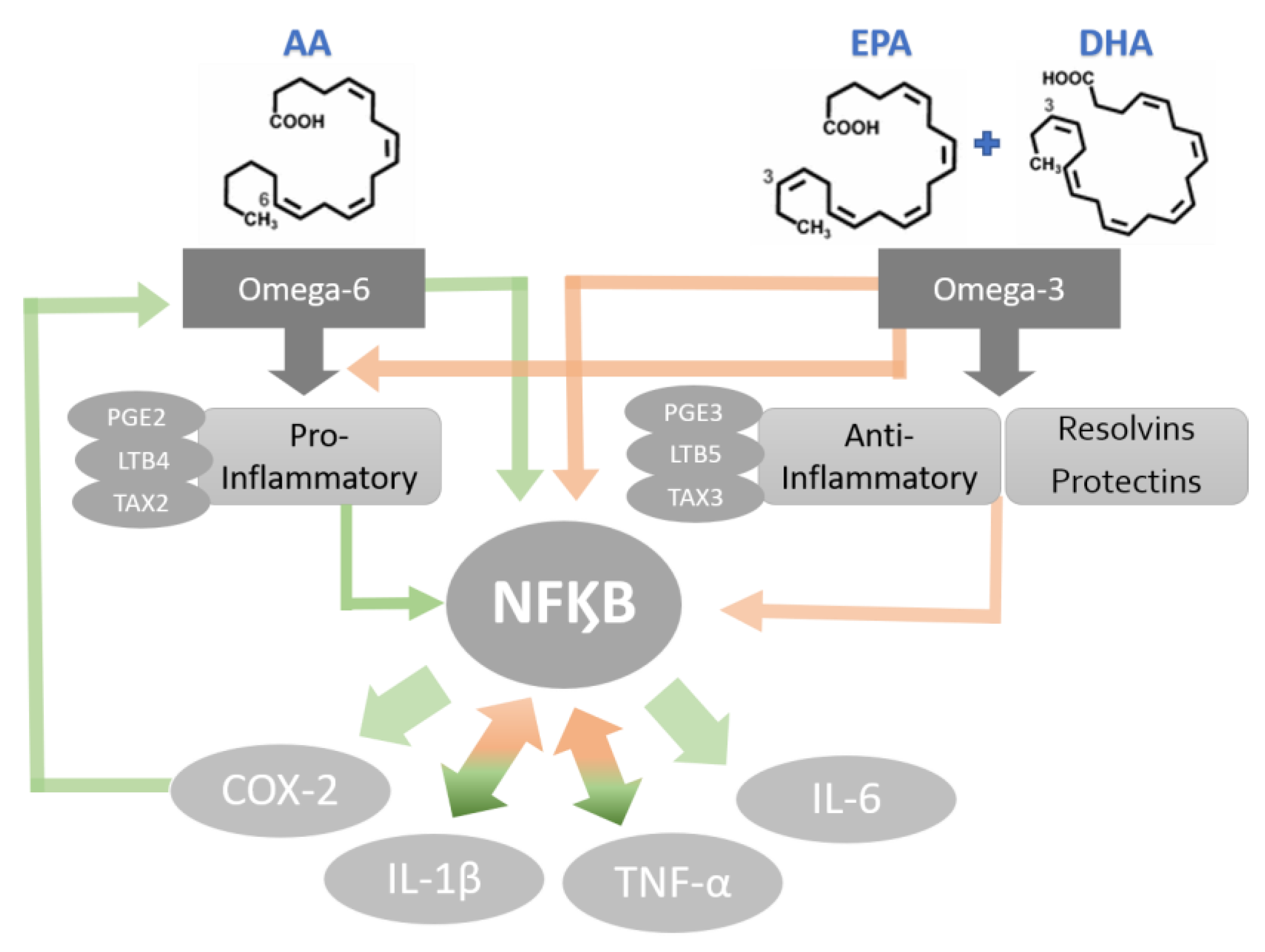
5. Omega-3: Inflammation Reduction and Tissue Homeostasis Recovery
6. Evidence of Omega-3 as Therapeutic Strategy
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | Arachidonic acid |
| AHA | American Heart Association |
| ALA | Alpha-linolenic acid |
| AP1 | Activator protein 1. |
| BAX | BCL-2-like protein 4 |
| BCL2 | B-cell lymphoma 2 gene |
| COX-2 | Cyclooxygenase-2 |
| DHA | Docosahexaenoic acid |
| DNA | Deoxyribonucleic acid |
| EPA | Eicosapentaenoic acid |
| FFA | Free fatty acids |
| GPx | Glutathione peroxidase |
| HO-1 | Heme oxygenase 1 |
| HSCT | Hematopoietic stem cell transplantation |
| ICAM-1 | Endothelial- and leukocyte-associated transmembrane |
| ICU | Intensive care unit |
| IL-1β | Interleukin 1 beta |
| IL-6 | Interleukin 6 |
| JNK | c- Jun N-terminal kinase |
| LLLT | Low-level laser therapy |
| MAPK | Mitogenated protein kinase |
| MASCC/ISOO | The Mucositis Study Group of the Multinational Association for Supportive Care in Cancer and the International Society of Oral Oncology |
| MMP | Matrix metalloproteinase |
| MTX | Methotrexate |
| NF-kB | Nuclear factor-kape Beta |
| OM | Oral mucositis |
| ω-3 | Omega-3PAF: Platelet-activating factor |
| PBM | Photobiomodulation |
| PMN | Polymorphonuclear leukocytes |
| PPARg | Peroxisome Proliferator Activated Receptor Gamma |
| PUFA | Polyunsaturated fatty acids |
| ROS | Reactive oxygen species |
| TNF-α | Tumour necrosis factor alpha |
| TPN | Total parenteral nutrition |
| U.S. FDA | United States Food and Drug Administration |
| VCAM-1 | Vascular adhesion molecule 1 |
References
- Lalla, R.V.; Sonis, S.T.; Peterson, D.E. Management of oral mucositis in patients who have cancer. Dent. Clin. N. Am. 2008, 52, 61–77. [Google Scholar] [CrossRef] [PubMed]
- Nonzee, N.J.; Dandade, N.A.; Patel, U.; Markossian, T.; Agulnik, M.; Argiris, A.; Patel, J.D.; Kern, R.C.; Munshi, H.G.; Calhoun, E.A.; et al. Evaluating the supportive care costs of severe radiochemotherapy-induced mucositis and pharyngitis: Results from a Northwestern University Costs of Cancer Program pilot study with head and neck and nonsmall cell lung cancer patients who received care at a county hospital, a Veterans Administration hospital, or a comprehensive cancer care center. Cancer 2008, 113, 1446–14452. [Google Scholar] [CrossRef] [PubMed]
- Alvariño-Martín, C.; Sarrión-Pérez, M.G. Prevention and treatment of oral mucositis in patients receiving chemotherapy. J. Clin. Exp. Dent. 2014, 6, e74–e80. [Google Scholar] [CrossRef] [PubMed]
- De Barros, P.A.V.; Rabelo Andrade, M.E.; de Vasconcelos Generoso, S.; Mendes Miranda, S.E.; Dos Reis, D.C.; Lacerda Leocádio, P.C.; de Sales E Souza, É.L.; Dos Santos Martins, F.; da Gama, M.A.S.; Cassali, G.D.; et al. Conjugated linoleic acid prevents damage caused by intestinal mucositis induced by 5-fluorouracil in an experimental model. Biomed. Pharmacother. 2018, 103, 1567–1576. [Google Scholar] [CrossRef]
- Villa, A.; Sonis, S.T. Mucositis: Pathobiology and management. Curr. Opin. Oncol. 2015, 27, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T. The pathobiology of mucositis. Nat. Rev. Cancer 2004, 4, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T.; Elting, L.S.; Keefe, D.; Peterson, D.E.; Schubert, M.; Hauer-Jensen, M.; Bekele, B.N.; Raber-Durlacher, J.; Donnelly, J.P.; Rubenstein, E.B. Mucositis Study Section of the Multinational Association for Supportive Care in Cancer; International Society for Oral Oncology. Perspectives on cancer therapy-induced mucosal injury: Pathogenesis, measurement, epidemiology, and consequences for patients. Cancer 2004, 100, 1995–2025. [Google Scholar] [CrossRef]
- Liu, S.; Zhao, Q.; Zheng, Z.; Liu, Z.; Meng, L.; Dong, L.; Jiang, X. Status of treatment and prophylaxis for radiation-induced oral mucositis in patients with head and neck cancer. Front. Oncol. 2021, 11, 642575. [Google Scholar] [CrossRef] [PubMed]
- Pulito, C.; Cristaudo, A.; Porta, C.; Zapperi, S.; Blandino, G.; Morrone, A.; Strano, S. Oral mucositis: The hidden side of cancer therapy. J. Exp. Clin. Cancer Res. 2020, 39, 210. [Google Scholar] [CrossRef]
- Naidu, M.U.; Ramana, G.V.; Rani, P.U.; Mohan, I.K.; Suman, A.; Roy, P. Chemotherapy-induced and/or radiation therapy-induced oral mucositis--complicating the treatment of cancer. Neoplasia 2004, 6, 423–431. [Google Scholar] [CrossRef]
- Silva, A.P.; Caruso, P.; Jaguar, G.C.; Carvalho, P.A.; Alves, F.A. Oral evaluation and procedures performed by dentists in patients admitted to the intensive care unit of a cancer center. Supportive Care Cancer 2014, 22, 2645–2650. [Google Scholar] [CrossRef] [PubMed]
- Campos, M.I.; Campos, C.N.; Aarestrup, F.M.; Aarestrup, B.J. Oral mucositis in cancer treatment: Natural history, prevention and treatment. Mol. Clin. Oncol. 2014, 2, 337–340. [Google Scholar] [CrossRef]
- Treister, N.; Sonis, S. Mucositis: Biology and management. Curr. Opin. Otolaryngol. Head Neck Surg. 2007, 15, 123–129. [Google Scholar] [CrossRef]
- Sonis, S.T. A biological approach to mucositis. J. Supp. Oncol. 2004, 2, 21–32. [Google Scholar]
- Shankar, A.; Roy, S.; Bhandari, M.; Rath, G.K.; Biswas, A.S.; Kanodia, R.; Adhikari, N.; Sachan, R. Current Trends in Management of Oral Mucositis in Cancer Treatment. Asian Pac. J. Cancer Prev. 2017, 18, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Blijlevens, N.; Sonis, S. Palifermin (recombinant keratinocyte growth factor-1): A pleiotropic growth factor with multiple biological activities in preventing chemotherapy- and radiotherapy-induced mucositis. Ann. Oncol. 2007, 18, 817–826. [Google Scholar] [CrossRef]
- Razmara, F.; Khayamzadeh, M. An Investigation into the Prevalence and Treatment of Oral Mucositis After Cancer Treatment. Int. J. Cancer Manag. 2019, 12, e88405. [Google Scholar] [CrossRef]
- Logan, R.M.; Gibson, R.J.; Sonis, S.T.; Keefe, D.M.K. Nuclear factor-κB (NF-κB) and cyclooxygenase-2 (COX-2) expression in the oral mucosa following cancer chemotherapy. Oral Oncol. 2007, 43, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Lionel, D.; Christophe, L.; Marc, A.; Jean-Luc, C. Oral mucositis induced by anticancer treatments: Physiopathology and treatments. Ther. Clin. Risk. Manag. 2006, 2, 159–168. [Google Scholar] [CrossRef]
- Mafra, C.A.D.C.C.; Vasconcelos, R.C.; de Medeiros, C.A.C.X.; Leitão, R.F.C.; Brito, G.A.C.; Costa, D.V.D.S.; Guerra, G.C.B.; de Araújo, R.F., Jr.; Medeiros, A.C.; de Araújo, A.A. Gliclazide Prevents 5-FU-Induced Oral Mucositis by Reducing Oxidative Stress, Inflammation, and P-Selectin Adhesion Molecules. Front. Physiol. 2019, 10, 327. [Google Scholar] [CrossRef]
- Sonis, S.T. The biologic role for nuclear factor-kappaB in disease and its potential involvement in mucosal injury associated with anti-neoplastic therapy. Crit. Rev. Oral Biol. Med. 2002, 13, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Al-Dasooqi, N.; Gibson, R.J.; Bowen, J.M.; Logan, R.M.; Stringer, A.M.; Keefe, D.M. Matrix metalloproteinases are possible mediators for the development of alimentary tract mucositis in the dark agouti rat. Exp. Biol. Med. 2010, 235, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- Al-Dasooqi, N.; Sonis, S.T.; Bowen, J.M.; Bateman, E.; Blijlevens, N.; Gibson, R.J.; Logan, R.M.; Nair, R.G.; Stringer, A.M.; Yazbeck, R.; et al. Mucositis Study Group of Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO). Emerging evidence on the pathobiology of mucositis. Supportive Care Cancer 2013, 21, 2075–2083. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T. Pathobiology of oral mucositis: Novel insights and opportunities. J. Support Oncol. 2007, 5, 3–11. [Google Scholar] [PubMed]
- Vesty, A.; Gear, K.; Biswas, K.; Mackenzie, B.W.; Taylor, M.W.; Douglas, R.G. Oral microbial influences on oral mucositis during radiotherapy treatment of head and neck cancer. Supportive Care Cancer 2020, 28, 2683–2691. [Google Scholar] [CrossRef]
- Haverman, T.M.; Laheij, A.M.G.A.; Nie, M.; Deng, D.M.; Raber-Durlacher, J.E.; de Soet, J.J.; Rozema, F.R. Exploring the role of oral microorganisms in the pathogenesis of mucositis by assessing their impact on metabolic activity and reproductive capacity of epithelial cells in vitro. Supportive Care Cancer 2020, 28, 4729–4735. [Google Scholar] [CrossRef]
- Laheij, A.M.; de Soet, J.J. Can the oral microflora affect oral ulcerative mucositis? Curr. Opin. Supportive Palliat. Care 2014, 8, 180–187. [Google Scholar] [CrossRef]
- Van Saene, H.K.; Martin, M.V. Do microorganisms play a role in irradiation mucositis? Eur. J. Clin. Microbiol. Infect. Dis. 1990, 9, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Napeñas, J.J.; Brennan, M.T.; Bahrani-Mougeot, F.K.; Fox, P.C.; Lockhart, P.B. Relationship between mucositis and changes in oral microflora during cancer chemotherapy. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2007, 103, 48–59. [Google Scholar] [CrossRef]
- Hensley, M.L.; Hagerty, K.L.; Kewalramani, T.; Green, D.M.; Meropol, N.J.; Wasserman, T.H.; Cohen, G.I.; Emami, B.; Gradishar, W.J.; Mitchell, R.B.; et al. Clinical practice guideline update: Use of chemotherapy and radiation therapy protectants. J. Clin. Oncol. 2009, 27, 127–145. [Google Scholar] [CrossRef]
- Al-Ansari, S.; Zecha, J.A.; Barasch, A.; de Lange, J.; Rozema, F.R.; Raber-Durlacher, J.E. Oral mucositis induced by anticancer therapies. Curr. Oral. Health Rep. 2015, 2, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.B.; Jarvis, V.; Zadik, Y.; Barasch, A.; Ariyawardana, A.; Hovan, A.; Yarom, N.; Lalla, R.V.; Bowen, J.; Elad, S. Mucositis Study Group of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO). Systematic review of miscellaneous agents for the management of oral mucositis in cancer patients. Supportive Care Cancer 2013, 21, 3223–3232. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cinausero, M.; Aprile, G.; Ermacora, P.; Basile, D.; Vitale, M.G.; Fanotto, V.; Parisi, G.; Calvetti, L.; Sonis, S.T. New Frontiers in the Pathobiology and Treatment of Cancer Regimen-Related Mucosal Injury. Front. Pharmacol. 2017, 8, 354. [Google Scholar] [CrossRef] [PubMed]
- Lalla, R.V.; Bowen, J.; Barasch, A.; Elting, L.; Epstein, J.; Keefe, D.M.; McGuire, D.B.; Migliorati, C.; Nicolatou-Galitis, O.; Peterson, D.E.; et al. Mucositis Guidelines Leadership Group of the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology (MASCC/ISOO). MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2014, 120, 1453–1461. [Google Scholar] [CrossRef]
- Elad, S.; Cheng, K.K.F.; Lalla, R.V.; Yarom, N.; Hong, C.; Logan, R.M.; Bowen, J.; Gibson, R.; Saunders, D.P.; Zadik, Y.; et al. Mucositis Guidelines Leadership Group of the Multinational Association of Supportive Care in Cancer and International Society of Oral Oncology (MASCC/ISOO). MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2020, 126, 4423–4431. [Google Scholar] [CrossRef]
- Chaveli-López, B.; Bagán-Sebastián, J.V. Treatment of oral mucositis due to chemotherapy. J. Clin. Exp. Dent. 2016, 8, e201–e209. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, P.A.G.; Lessa, R.C.; Carraro, D.M.; Assis Pellizzon, A.C.; Jaguar, G.C.; Alves, F.A. Three photobiomodulation protocols in the prevention/treatment of radiotherapy-induced oral mucositis. Photodiagnosis Photodyn. Ther. 2020, 31, 101906. [Google Scholar] [CrossRef]
- Bensadoun, R.J.; Franquin, J.C.; Ciais, G.; Darcourt, V.; Schubert, M.M.; Viot, M.; Dejou, J.; Tardieu, C.; Benezery, K.; Nguyen, T.D.; et al. Low-energy He/Ne laser in the prevention of radiation-induced mucositis. A multicenter phase III randomized study in patients with head and neck cancer. Supportive Care Cancer 1999, 7, 244–252. [Google Scholar] [CrossRef]
- Arora, H.; Pai, K.M.; Maiya, A.; Vidyasagar, M.S.; Rajeev, A. Efficacy of He-Ne Laser in the prevention and treatment of radiotherapy-induced oral mucositis in oral cancer patients. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2008, 105, 180–186.e1. [Google Scholar] [CrossRef]
- Zanin, T.; Zanin, F.; Carvalhosa, A.A.; Castro, P.H.; Pacheco, M.T.; Zanin, I.C.; Brugnera, A., Jr. Use of 660-nm diode laser in the prevention and treatment of human oral mucositis induced by radiotherapy and chemotherapy. Photomed. Laser Surg. 2010, 28, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Simões, A.; de Campos, L.; de Souza, D.N.; de Matos, J.A.; Freitas, P.M.; Nicolau, J. Laser phototherapy as topical prophylaxis against radiation-induced xerostomia. Photomed. Laser Surg. 2010, 28, 357–363. [Google Scholar] [CrossRef]
- Gouvêa de Lima, A.; Villar, R.C.; de Castro, G., Jr.; Antequera, R.; Gil, E.; Rosalmeida, M.C.; Federico, M.H.; Snitcovsky, I.M. Oral mucositis prevention by low-level laser therapy in head-and-neck cancer patients undergoing concurrent chemoradiotherapy: A phase III randomised study. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 270–275. [Google Scholar] [CrossRef]
- Carvalho, P.A.; Jaguar, G.C.; Pellizzon, A.C.; Prado, J.D.; Lopes, R.N.; Alves, F.A. Evaluation of low-level laser therapy in the prevention and treatment of radiation-induced mucositis: A double-blind randomized study in head and neck cancer patients. Oral Oncol. 2011, 47, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Lopes Martins, A.F.; Nogueira, T.E.; Morais, M.O.; de Sousa-Neto, S.S.; Oton-Leite, A.F.; Valadares, M.C.; Aires Freitas, N.M.; Leles, C.R.; Mendonça, E.F. Cost-effectiveness randomized clinical trial on the effect of photobiomodulation therapy for prevention of radiotherapy-induced severe oral mucositis in a Brazilian cancer hospital setting. Supportive Care Cancer 2021, 29, 1245–1256. [Google Scholar] [CrossRef] [PubMed]
- Pires Marques, E.C.; Piccolo Lopes, F.; Nascimento, I.C.; Morelli, J.; Pereira, M.V.; Machado Meiken, V.M.; Pinheiro, S.L. Photobiomodulation and photodynamic therapy for the treatment of oral mucositis in patients with cancer. Photodiagnosis Photodyn. Ther. 2020, 29, 101621. [Google Scholar] [CrossRef] [PubMed]
- Yarom, N.; Hovan, A.; Bossi, P.; Ariyawardana, A.; Jensen, S.B.; Gobbo, M.; Saca-Hazboun, H.; Kandwal, A.; Majorana, A.; Ottaviani, G.; et al. Mucositis Study Group of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO). Systematic review of natural and miscellaneous agents, for the management of oral mucositis in cancer patients and clinical practice guidelines—Part 2: Honey, herbal compounds, saliva stimulants, probiotics, and miscellaneous agents. Supportive Care Cancer 2020, 28, 2457–2472. [Google Scholar] [CrossRef]
- Migliorati, C.A.; Oberle-Edwards, L.; Schubert, M. The role of alternative and natural agents, cryotherapy, and/or laser for management of alimentary mucositis. Supportive Care Cancer 2006, 14, 533–540. [Google Scholar] [CrossRef]
- Baharvand, M.; Jafari, S.; Mortazavi, H. Herbs in Oral Mucositis. J. Clin. Diagn Res. 2017, 11, ZE05–ZE11. [Google Scholar] [CrossRef] [PubMed]
- Aghamohamamdi, A.; Hosseinimehr, S.J. Natural Products for Management of Oral Mucositis Induced by Radiotherapy and Chemotherapy. Integr. Cancer Ther. 2016, 15, 60–68. [Google Scholar] [CrossRef]
- Kaur, M.; Sable, D.M.; Chowdhery, A.; Chavan, M. A Review of Omega 3 and it “s Role in Oral Diseases. Int. J. Curr. Adv. Res. 2016, 4, 921–925. [Google Scholar] [CrossRef]
- Cholewski, M.; Tomczykowa, M.; Tomczyk, M. A Comprehensive Review of Chemistry, Sources and Bioavailability of Omega-3 Fatty Acids. Nutrients 2018, 10, 1662. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am. J. Clin. Nutr. 2006, 83, 1505S–1519S. [Google Scholar] [CrossRef] [PubMed]
- Surette, M.E. The science behind dietary omega-3 fatty acids. CMAJ 2008, 178, 177–180. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 polyunsaturated fatty acids and inflammatory processes: Nutrition or pharmacology? Br. J. Clin. Pharmacol. 2013, 75, 645–662. [Google Scholar] [CrossRef]
- Gutiérrez, S.; Svahn, S.L.; Johansson, M.E. Effects of Omega-3 Fatty Acids on Immune Cells. Int. J. Mol. Sci. 2019, 20, 5028. [Google Scholar] [CrossRef]
- McDaniel, J.C.; Belury, M.; Ahijevych, K.; Blakely, W. Omega-3 fatty acids effect on wound healing. Wound Repair Regen. 2008, 16, 337–345. [Google Scholar] [CrossRef]
- Smith, P.C.; Martínez, C. Wound Healing in the Oral Mucosa. In Oral Mucosa in Health and Disease; Bergmeier, L., Ed.; Springer: Cham, Switzerland, 2018; pp. 77–90. [Google Scholar] [CrossRef]
- Kang, J.X.; Weylandt, K.H. Modulation of Inflammatory Cytokines by Omega-3 Fatty Acids. In Lipids in Health and Disease; Quinn, P.J., Wang, X., Eds.; Springer: Dordrecht, The Netherlands, 2008; pp. 133–143. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes: From molecules to man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef]
- Sommakia, S.; Baker, O.J. Regulation of inflammation by lipid mediators in oral diseases. Oral Dis. 2017, 23, 576–597. [Google Scholar] [CrossRef] [PubMed]
- Al-Taie, A.; Al-Shohani, A.D.; Albasry, Z.; Altaee, A. Current topical trends and novel therapeutic approaches and delivery systems for oral mucositis management. J. Pharm Bioall Sci. 2020, 12, 94–101. [Google Scholar] [CrossRef]
- Lee, J.Y.; Sohn, K.H.; Rhee, S.H.; Hwang, D. Saturated fatty acids, but not unsaturated fatty acids, induce the expression of cyclooxygenase-2 mediated through Toll- like receptor 4. J. Biol. Chem. 2001, 18, 16683–16689. [Google Scholar] [CrossRef]
- Calder, P.C. Immunonutrition. BMJ 2003, 327, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Vanden Berghe, W.; Vermeulen, L.; Delerive, P.; de Bosscher, K.; Staels, B.; Haegeman, G. A paradigm for gene regulation: Inflammation, NF-kappaB and PPAR. Adv. Exp. Med. Biol. 2003, 544, 181–196. [Google Scholar] [CrossRef]
- Alvarado, Y.; Bellm, L.A.; Giles, F.J. Oral Mucositis: Time for More Studies. Hematology 2020, 7, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Nagi, R.; Patil, D.J.; Rakesh, N.; Jain, S.; Sahu, S. Natural agents in the management of oral mucositis in cancer patients-systematic review. J. Oral Biol Craniofac Res. 2018, 8, 245–254. [Google Scholar] [CrossRef]
- Chow, O.; Barbul, A. Immunonutrition: Role in Wound Healing and Tissue Regeneration. Adv. Wound Care 2014, 3, 46–53. [Google Scholar] [CrossRef]
- McDaniel, J.C.; Massey, K.; Nicolaou, A. Fish oil supplementation alters levels of lipid mediators of inflammation in microenvironment of acute human wounds. Wound Repair Regen. 2011, 19, 189–200. [Google Scholar] [CrossRef]
- Freitas, R.D.S.; Campos, M.M. Protective Effects of Omega-3 Fatty Acids in Cancer- Related Complications. Nutrients 2019, 11, 945. [Google Scholar] [CrossRef] [PubMed]
- Abdelsalam, N.N.; Aboubakr, S.H. Impact of Omega-3 on Healing of Buccal Traumatic Ulcer of Albino Rats (Histological and Immunohistological Study). Egypt. Dent. J. 2017, 63, 3193–3201. [Google Scholar] [CrossRef][Green Version]
- Hashemipour, M.A.; Ghasemi, A.R.; Dogaheh, M.A.; Torabi, M. Effects of Locally and Systemically Applied n-3 Fatty Acid on Oral Ulcer Recovery Process in Rats. Wounds 2012, 24, 258–266. [Google Scholar]
- El Khouli, A.M.; El-Gendy, E.A. Efficacy of omega-3 in treatment of recurrent aphthous stomatitis and improvement of quality of life: A randomizedrandomised, double-blind, placebo-controlled study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 117, 191–196. [Google Scholar] [CrossRef]
- Nosratzehi, T.; Akar, A. Efficacy of Omega-3 in Treatment of Recurrent Aphthous Stomatitis: A Randomised, Double-blind, Placebo-controlled Study. Chin. J. Dent. Res. 2016, 19, 159–164. [Google Scholar] [CrossRef]
- Hashemipour, M.A.; Barzegari, S.; Kakoie, S.; Aghahi, R.H. Effects of Omega-3 Fatty Acids Against Chemotherapy-induced Mucositis: A Double-blind Randomized Clinical Trial. Wounds 2017, 29, 360–366. [Google Scholar] [PubMed]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. AHA Nutrition Committee. American Heart Association. Omega-3 fatty acids and cardiovascular disease: New recommendations from the American Heart Association. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 151–152. [Google Scholar] [CrossRef]
- Serhan, C.N. Novel lipid mediators and resolution mechanisms in acute inflammation: To resolve or not? Am. J. Pathol. 2010, 177, 1576–1591. [Google Scholar] [CrossRef] [PubMed]
- Yates, C.M.; Calder, P.C.; Ed Rainger, G. Pharmacology and therapeutics of omega-3 polyunsaturated fatty acids in chronic inflammatory disease. Pharmacol. Ther. 2014, 141, 272–282. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| References | Study Description | Omega-3 Dose | Key Finding | |
|---|---|---|---|---|
| McDaniel et al. 2008 [56] | Clinical Trial, Randomized and Double-blind Control Study. | Evaluation of plasma fatty acid levels in healthy individuals (n = 30) at baseline and after 4 weeks in a blister wound model. | ω-3 group: total daily intake of 1.6 g of EPA and 1.1 g DHA capsules daily/4 weeks. | PUFA may increase proinflammatory cytokine production at wound sites at 24 h and non significantly slower wound healing. |
| McDaniel et al. 2011 [68] | Clinical Trial, Randomized and Double-blind Control Study. | Evaluation of lipid mediator levels in acute wound and the reduction of PMN levels in healthy individuals (n = 18) by a blister wound model. | Active group: 1.6 g of EPA and 1.2 g of DHA per day/28 days. | ω-3 group presented lower mean levels of myeloperoxidase at 12 h and more reepithelialisation on Day 5 post wounding. |
| Abdelsalam et al. 2017 [70] | Murine model, Group-control Study | 2 groups (n = 15 per group). Histological samples harvested on post-injury days 3, 7 and 14. | Systemic: 93 mg/kg body weight | The study group had high reepithelialisation and connective tissue healing score on day 7 and 14. |
| Hashemipour et al. 2012 [71] | Murine model, Group-control Study | 5 groups (n = 16 per group). On post-injury days 2, 4, 6, and 8, tissues harvested for histological evaluation. | Local: 100 mg/kg (0.2% total weight) and Systemic: 200 mg/kg (0.4% total weight) | The control group had highest inflammation, and the lowest reepithelialisation. The thickest epithelium was observed in the local and systemic groups on days 6 and 8. |
| El Khouli & El-Gendy 2014 [72] | Clinical Trial, Randomized and Double-blind Control Study. | Patients diagnosis with recurrent aphthous ulcer (n = 50). Evaluation by number of new ulcers, duration of ulcer episodes, and pain level through questionnaires. | Experimental group: ω-3 (1 g-200 mg of DHA and 300 mg of EPA), 3x daily/6 months. | Daily ω-3 treatment achieved a significant reduction in number of ulcers, duration of ulcers, and level of pain by 3 months that persist for 6 months. |
| Nosratzehi & Akar 2016 [73] | Clinical Trial, Randomized and Double-blind Control Study. | Patients diagnosis with recurrent aphthous ulcer (n = 50). Size and rate of ulcers was measured weekly. | ω-3 group: 1 g of DHA and EPA, 3 times daily for 6 months. | The ω-3 group present less pain and irritation. The ulcer size decrease from 2.3 to 1.48 mm (p = 0.062). The number of ulcers indicates a reduction in comparison with the control group. |
| Hashemipour et al. 2017 [74] | Clinical Trial, Randomized and Double-blind Control Study. | Patients with leukaemia or breast cancer diagnosis undergoing chemotherapy treatment that developed oral mucositis (n = 60). Oral examinations were repeated on days 1, 7, 14, and 21. | ω-3 group: 1 g pearl (360 mg of EPA, and 240 mg of DHA), 2 capsules daily. | Differences in the severity of mucositis and pain score between the ω-3 and placebo groups in the first, second, and third weeks of treatment were noted. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lessa, R.C.; Alves, F.d.A.; Fortunati, E.; Lu, J. Oral Mucositis in Cancer and Potential Use of Omega-3 Free Fatty Acids in Its Management: A Review. Biomedicines 2021, 9, 1531. https://doi.org/10.3390/biomedicines9111531
Lessa RC, Alves FdA, Fortunati E, Lu J. Oral Mucositis in Cancer and Potential Use of Omega-3 Free Fatty Acids in Its Management: A Review. Biomedicines. 2021; 9(11):1531. https://doi.org/10.3390/biomedicines9111531
Chicago/Turabian StyleLessa, Roberta Cardim, Fabio de Abreu Alves, Erika Fortunati, and Jun Lu. 2021. "Oral Mucositis in Cancer and Potential Use of Omega-3 Free Fatty Acids in Its Management: A Review" Biomedicines 9, no. 11: 1531. https://doi.org/10.3390/biomedicines9111531
APA StyleLessa, R. C., Alves, F. d. A., Fortunati, E., & Lu, J. (2021). Oral Mucositis in Cancer and Potential Use of Omega-3 Free Fatty Acids in Its Management: A Review. Biomedicines, 9(11), 1531. https://doi.org/10.3390/biomedicines9111531