Effects of Pitavastatin, Atorvastatin, and Rosuvastatin on the Risk of New-Onset Diabetes Mellitus: A Single-Center Cohort Study

 ,
,  , ,
, ,  and
and
Abstract

1. Introduction
2. Material and Methods
2.1. Population
2.2. Observational Variables
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; Simes, J.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef] [PubMed]
- Adhyaru, B.B.; Jacobson, T.A. Safety and efficacy of statin therapy. Nat. Rev. Cardiol. 2018, 15, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M., Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.; Blauw, G.J.; Murphy, M.B.; Bollen, E.L.; Buckley, B.M.; Cobbe, S.M.; Ford, I.; Gaw, A.; Hyland, M.; Jukema, J.W.; et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): A randomised controlled trial. Lancet 2002, 360, 1623–1630. [Google Scholar] [CrossRef]
- Carter, A.A.; Gomes, T.; Camacho, X.; Juurlink, D.N.; Shah, B.R.; Mamdani, M.M. Risk of incident diabetes among patients treated with statins: Population based study. BMJ 2013, 346, f2610. [Google Scholar] [CrossRef]
- Cho, Y.; Choe, E.; Lee, Y.H.; Seo, J.W.; Choi, Y.; Yun, Y.; Wang, H.J.; Ahn, C.W.; Cha, B.S.; Lee, H.C.; et al. Risk of diabetes in patients treated with HMG-CoA reductase inhibitors. Metabolism 2015, 64, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, H.S.; Lee, K.Y. Effect of statins on fasting glucose in non-diabetic individuals: Nationwide population-based health examination in Korea. Cardiovasc. Diabetol. 2018, 17, 155. [Google Scholar] [CrossRef]
- Cederberg, H.; Stancakova, A.; Yaluri, N.; Modi, S.; Kuusisto, J.; Laakso, M. Increased risk of diabetes with statin treatment is associated with impaired insulin sensitivity and insulin secretion: A 6 year follow-up study of the METSIM cohort. Diabetologia 2015, 58, 1109–1117. [Google Scholar] [CrossRef]
- Yamazaki, T.; Kishimoto, J.; Ito, C.; Noda, M.; Odawara, M.; Terauchi, Y.; Shiba, T.; Kitazato, H.; Iwamoto, Y.; Akanuma, Y.; et al. Effect of pitavastatin on the incidence of diabetes in Japanese individuals with impaired glucose tolerance. Diabetologia 2013, 56 (Suppl. S1), S299. [Google Scholar] [CrossRef]
- Thakker, D.; Nair, S.; Pagada, A.; Jamdade, V.; Malik, A. Statin use and the risk of developing diabetes: A network meta-analysis. Pharmacoepidemiol. Drug Saf. 2016, 25, 1131–1149. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.; Sheen, S.S.; Lee, S.; Choi, Y.J.; Park, R.W.; Lim, H.S. Statins and risk for new-onset diabetes mellitus: A real-world cohort study using a clinical research database. Medicine (Baltimore) 2016, 95, e5429. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Sung, J.M.; Cho, I.J.; Kim, H.C.; Chang, H.J. Risk of new-onset diabetes among patients treated with statins according to hypertension and gender: Results from a nationwide health-screening cohort. PLoS ONE 2018, 13, e0195459. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Choi, C.U.; Hwang, S.Y.; Choi, B.G.; Jang, W.Y.; Kim, D.Y.; Kim, W.; Park, E.J.; Lee, S.; Na, J.O.; et al. Effect of Pitavastatin Compared with Atorvastatin andRosuvastatin on New-Onset Diabetes Mellitus in PatientsWith Acute Myocardial Infarction. Am. J. Cardiol. 2018, 122, 922–928. [Google Scholar] [CrossRef]
- Carmena, R.; Betteridge, D.J. Diabetogenic Action of Statins: Mechanisms. Curr. Atheroscler. Rep. 2019, 21, 23. [Google Scholar] [CrossRef] [PubMed]
- Salunkhe, V.A.; Elvstam, O.; Eliasson, L.; Wendt, A. Rosuvastatin Treatment Affects Both Basal and Glucose-Induced Insulin Secretion in INS-1 832/13 Cells. PLoS ONE 2016, 11, e0151592. [Google Scholar] [CrossRef]
- Donath, M.Y.; Boni-Schnetzler, M.; Ellingsgaard, H.; Ehses, J.A. Islet inflammation impairs the pancreatic beta-cell in type 2 diabetes. Physiology (Bethesda) 2009, 24, 325–331. [Google Scholar] [CrossRef]
- Supale, S.; Li, N.; Brun, T.; Maechler, P. Mitochondrial dysfunction in pancreatic beta cells. Trends Endocrinol. Metab. 2012, 23, 477–487. [Google Scholar] [CrossRef]
- Mabuchi, H.; Higashikata, T.; Kawashiri, M.; Katsuda, S.; Mizuno, M.; Nohara, A.; Inazu, A.; Koizumi, J.; Kobayashi, J. Reduction of serum ubiquinol-10 and ubiquinone-10 levels by atorvastatin in hypercholesterolemic patients. J. Atheroscler. Thromb. 2005, 12, 111–119. [Google Scholar] [CrossRef]
- Swerdlow, D.I.; Preiss, D.; Kuchenbaecker, K.B.; Holmes, M.V.; Engmann, J.E.; Shah, T.; Sofat, R.; Stender, S.; Johnson, P.C.; Scott, R.A.; et al. HMG-coenzyme A reductase inhibition, type 2 diabetes, and bodyweight: Evidence from genetic analysis and randomised trials. Lancet 2015, 385, 351–361. [Google Scholar] [CrossRef]
- Nakata, M.; Nagasaka, S.; Kusaka, I.; Matsuoka, H.; Ishibashi, S.; Yada, T. Effects of statins on the adipocyte maturation and expression of glucose transporter 4 (SLC2A4): Implications in glycaemic control. Diabetologia 2006, 49, 1881–1892. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Shin, H.J.; Ding, E.L.; van Dam, R.M. Adiponectin levels and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2009, 302, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Tsugawa, Y.; Tseng, C.H.; Kobayashi, Y.; Shapiro, M.F. Different time trends of caloric and fat intake between statin users and nonusers among US adults: Gluttony in the time of statins? JAMA Intern. Med. 2014, 174, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Takaguri, A.; Satoh, K.; Itagaki, M.; Tokumitsu, Y.; Ichihara, K. Effects of atorvastatin and pravastatin on signal transduction related to glucose uptake in 3T3L1 adipocytes. J. Pharmacol. Sci. 2008, 107, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Preiss, D.; Murray, H.M.; Welsh, P.; Buckley, B.M.; de Craen, A.J.; Seshasai, S.R.; McMurray, J.J.; Freeman, D.J.; Jukema, J.W.; et al. Statins and risk of incident diabetes: A collaborative meta-analysis of randomised statin trials. Lancet 2010, 375, 735–742. [Google Scholar] [CrossRef]
- Arnaboldi, L.; Corsini, A. Could changes in adiponectin drive the effect of statins on the risk of new-onset diabetes? The case of pitavastatin. Atheroscler. Suppl. 2015, 16, 1–27. [Google Scholar] [CrossRef]
- Preiss, D.; Seshasai, S.R.; Welsh, P.; Murphy, S.A.; Ho, J.E.; Waters, D.D.; DeMicco, D.A.; Barter, P.; Cannon, C.P.; Sabatine, M.S.; et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: A meta-analysis. JAMA 2011, 305, 2556–2564. [Google Scholar] [CrossRef]
- Nakamura, H.; Arakawa, K.; Itakura, H.; Kitabatake, A.; Goto, Y.; Toyota, T.; Nakaya, N.; Nishimoto, S.; Muranaka, M.; Yamamoto, A.; et al. Primary prevention of cardiovascular disease with pravastatin in Japan (MEGA Study): A prospective randomised controlled trial. Lancet 2006, 368, 1155–1163. [Google Scholar] [CrossRef]
- Kim, T.M.; Kim, H.; Jeong, Y.J.; Baik, S.J.; Yang, S.J.; Lee, S.H.; Cho, J.H.; Lee, H.; Yim, H.W.; Choi, I.Y.; et al. The differences in the incidence of diabetes mellitus and prediabetes according to the type of HMG-CoA reductase inhibitors prescribed in Korean patients. Pharmacoepidemiol. Drug Saf. 2017, 26, 1156–1163. [Google Scholar] [CrossRef]
- Vallejo-Vaz, A.J.; Kondapally Seshasai, S.R.; Kurogi, K.; Michishita, I.; Nozue, T.; Sugiyama, S.; Tsimikas, S.; Yoshida, H.; Ray, K.K. Effect of pitavastatin on glucose, HbA1c and incident diabetes: A meta-analysis of randomized controlled clinical trials in individuals without diabetes. Atherosclerosis 2015, 241, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.; Halim, A. The effects of inflammation, aging and oxidative stress on the pathogenesis of diabetes mellitus (type 2 diabetes). Diabetes Metab. Syndr. 2019, 13, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Bu, D.X.; Tarrio, M.; Grabie, N.; Zhang, Y.; Yamazaki, H.; Stavrakis, G.; Maganto-Garcia, E.; Pepper-Cunningham, Z.; Jarolim, P.; Aikawa, M.; et al. Statin-induced Kruppel-like factor 2 expression in human and mouse T cells reduces inflammatory and pathogenic responses. J. Clin. Investig. 2010, 120, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.W.; Lin, C.S.; Tsai, M.C.; Shih, S.F.; Lim, Z.W.; Chen, S.J.; Tsui, P.F.; Ho, L.J.; Lai, J.H.; Liou, J.T. Pitavastatin Exerts Potent Anti-Inflammatory and Immunomodulatory Effects via the Suppression of AP-1 Signal Transduction in Human T Cells. Int. J. Mol. Sci. 2019, 20, 3534. [Google Scholar] [CrossRef]
- Goldberg, R.B. Cytokine and cytokine-like inflammation markers, endothelial dysfunction, and imbalanced coagulation in development of diabetes and its complications. J. Clin. Endocrinol. Metab. 2009, 94, 3171–3182. [Google Scholar] [CrossRef]
- Nakagomi, A.; Shibui, T.; Kohashi, K.; Kosugi, M.; Kusama, Y.; Atarashi, H.; Shimizu, W. Differential Effects of Atorvastatin and Pitavastatin on Inflammation, Insulin Resistance, and the Carotid Intima-Media Thickness in Patients with Dyslipidemia. J. Atheroscler. Thromb. 2015, 22, 1158–1171. [Google Scholar] [CrossRef]
- Tsai, A.C.; Lee, S.H. Determinants of new-onset diabetes in older adults-Results of a national cohort study. Clin. Nutr. 2015, 34, 937–942. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Coupland, C. Development and validation of QDiabetes-2018 risk prediction algorithm to estimate future risk of type 2 diabetes: Cohort study. BMJ 2017, 359, j5019. [Google Scholar] [CrossRef]
- Lin, C.S.; Liu, C.C.; Yeh, C.C.; Chang, Y.C.; Chung, C.L.; Lane, H.L.; Shih, C.C.; Chen, T.L.; Liao, C.C. Diabetes risks and outcomes in chronic obstructive pulmonary disease patients: Two nationwide population-based retrospective cohort studies. PLoS ONE 2017, 12, e0181815. [Google Scholar] [CrossRef]
- Fathallah, N.; Slim, R.; Larif, S.; Hmouda, H.; Ben Salem, C. Drug-Induced Hyperglycaemia and Diabetes. Drug Saf. 2015, 38, 1153–1168. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variables | Pitavastatin (N = 1312, 15.7%) | Atorvastatin (N = 3034, 36.4%) | Rosuvastatin (N = 3991, 47.9%) | p-Value |
|---|---|---|---|---|
| Follow up (days) | 468.31 ± 446.18 | 558.30 ± 666.85 | 648.30 ± 796.06 | <0.001 |
| NODM | 167 (12.7%) | 555 (18.3%) | 864 (21.6%) | <0.001 |
| Gender (male) | 728 (55.5%) | 1546 (51.0%) | 2236 (56.0%) | <0.001 |
| Age | 60.42 ± 12.44 | 61.53 ± 13.54 | 58.21 ± 13.45 | <0.001 |
| BMI | 25.71 ± 4.18 | 24.75 ± 4.08 | 25.11 ± 4.38 | 0.017 |
| Comorbidities | ||||
| CAD | 551 (42.0%) | 798 (26.3%) | 931 (23.3%) | <0.001 |
| Hypertension | 796 (60.7%) | 1416 (46.7%) | 1864 (46.7%) | <0.001 |
| COPD | 195 (14.9%) | 363 (12.0%) | 419 (10.5%) | <0.001 |
| CKD | 29 (2.2%) | 154 (5.1%) | 90 (2.3%) | <0.001 |
| Cancer | 82 (6.2%) | 313 (10.3%) | 266 (6.7%) | <0.001 |
| Ischemic stroke | 160 (12.2%) | 508 (16.7%) | 736 (18.4%) | <0.001 |
| Hemorrhagic stroke | 24 (1.8%) | 76 (2.5%) | 71 (1.8%) | 0.086 |
| Heart failure | 100 (7.6%) | 213 (7.0%) | 256 (6.4%) | 0.279 |
| Biochemistry | ||||
| LDL (mg/dL) | 131.52 ± 28.51 | 122.94 ± 37.57 | 141.30 ± 45.86 | <0.001 |
| TC (mg/dL) | 202.91 ± 35.03 | 198.53 ± 46.67 | 218.96 ± 54.14 | <0.001 |
| TG (mg/dL) | 138.95 ± 74.01 | 138.80 ± 84.14 | 164.14 ± 133.90 | <0.001 |
| Creatinine (mg/dL) | 0.89 ± 0.27 | 1.03 ± 0.98 | 0.94 ± 0.64 | <0.001 |
| ALT (U/L) | 23.59 ± 16.43 | 23.64 ± 20.52 | 25.78 ± 19.71 | <0.001 |
| Uric Acid (mg/dL) | 6.07 ± 1.56 | 6.05 ± 1.66 | 6.13 ± 1.79 | 0.376 |
| FG (mg/dL) | 99.94 ± 15.74 | 99.27 ± 17.31 | 99.57 ± 17.98 | 0.581 |
| HbA1c (%) | 6.05 ± 0.98 | 6.08 ± 1.17 | 6.09 ± 1.23 | 0.872 |
| Variables | Crude-HR (95% CI) | p-Value | Adj-HR (95% CI) # | p-Value |
|---|---|---|---|---|
| Gender (male) | 1.00 (0.91–1.10) | 0.987 | 1.17 (1.05–1.29) | 0.003 |
| Age | 1.01 (1.01–1.02) | <0.001 | 1.02 (1.01–1.02) | <0.001 |
| Comorbidities | ||||
| CAD | 0.64 (0.57–0.73) | <0.001 | 0.63 (0.55–0.72) | <0.001 |
| Hypertension | 0.81 (0.73–0.89) | <0.001 | 0.78 (0.70–0.87) | <0.001 |
| COPD | 0.73 (0.61–0.88) | 0.001 | 0.71 (0.59–0.86) | <0.001 |
| CKD | 1.58 (1.22–2.04) | 0.001 | 1.56 (1.20–2.02) | 0.001 |
| cancer | 0.93 (0.76–1.12) | 0.433 | 0.83 (0.69–1.01) | 0.067 |
| Ischemic stroke | 1.16 (1.02–1.32) | 0.028 | 1.00 (0.87–1.16) | 0.964 |
| Hemorrhagic stroke | 1.06 (0.73–1.54) | 0.761 | 0.99 (0.68–1.45) | 0.969 |
| Heart failure | 1.16 (0.96–1.40) | 0.113 | 1.17 (0.96–1.42) | 0.121 |
| Biochemistry | ||||
| LDL (per 10 mg/dL) | 0.97 (0.95–0.99) | <0.001 | 0.97 (0.96–0.99) | 0.006 |
| TC (per 10 mg/dL) | 0.97 (0.95–0.98) | <0.001 | 0.97 (0.96–0.99) | 0.001 |
| TG (per 10 mg/dL) | 1.01 (1.01–1.02) | <0.001 | 1.02 (1.01–1.02) | <0.001 |
| Cr (per 1 mg/dL) | 1.18 (1.12–1.25) | <0.001 | 1.14 (1.07–1.23) | <0.001 |
| ALT (per 1 U/L) | 1.01 (1.00–1.01) | <0.001 | 1.01 (1.01–1.01) | <0.001 |
| UA (per 1 mg/dL) | 1.06 (1.02–1.11) | 0.006 | 1.05 (1.00–1.09) | 0.043 |
| FG (per 1 mg/dL) | 1.03 (1.03–1.03) | <0.001 | 1.03 (1.03–1.03) | <0.001 |
| HbA1c (per 1%) | 1.63 (1.55–1.70) | <0.001 | 1.64 (1.57–1.73) | <0.001 |
| Independent Variables | Crude-HR (95% CI) | p-Value | Adj-HR (95% CI) # | p-Value |
|---|---|---|---|---|
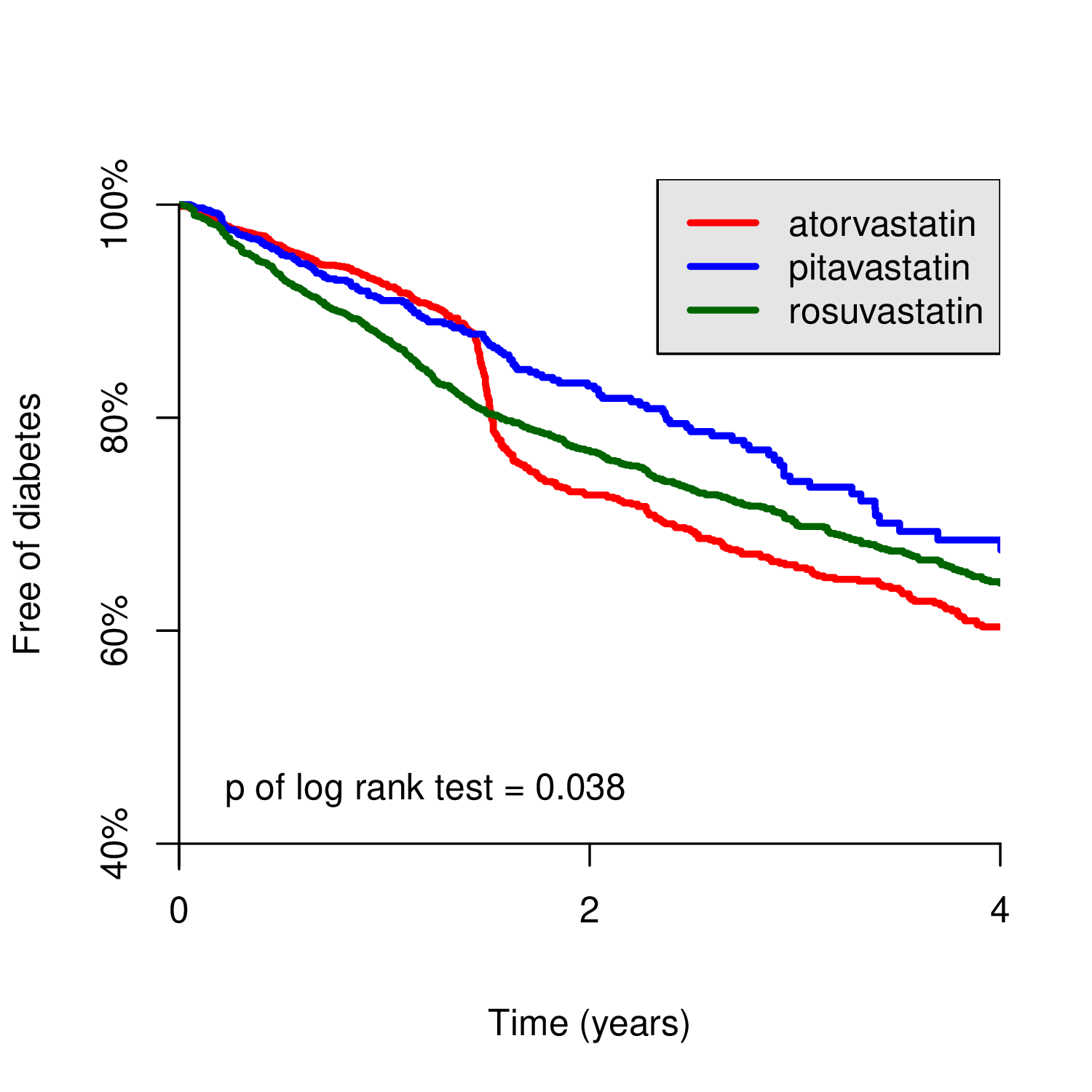
| Comparison 1 | 0.038 | 0.230 | ||
| Pitavastatin | 1.00 | 1.00 | ||
| Atorvastatin | 1.21 (1.02–1.44) | 0.032 | 1.04 (0.87–1.25) | 0.677 |
| Rosuvastatin | 1.24 (1.05–1.47) | 0.011 | 1.13 (0.94–1.35) | 0.196 |
| Comparison 2 | ||||
| Pitavastatin | 1.00 | 1.00 | ||
| Atorvastatin/Rosuvastatin | 1.23 (1.05–1.45) | 0.012 | 1.09 (0.91–1.29) | 0.356 |
| Stratified Variables | Drugs | Crude-HR (95% CI) | p-Value | Adj-HR (95% CI) # | p-Value |
|---|---|---|---|---|---|
| Gender | |||||
| Female | Pitavastatin | 1.00 | 1.00 | ||
| (N = 3827) | Atorvastatin | 1.25 (0.96–1.64) | 0.103 | 1.07 (0.81–1.43) | 0.627 |
| Rosuvastatin | 1.43 (1.10–1.86) | 0.007 | 1.31 (0.99–1.73) | 0.063 | |
| Male | Pitavastatin | 1.00 | 1.00 | ||
| (N = 4510) | Atorvastatin | 1.19 (0.95–1.50) | 0.131 | 1.03 (0.81–1.31) | 0.792 |
| Rosuvastatin | 1.12 (0.90–1.39) | 0.317 | 1.02 (0.80–1.29) | 0.899 | |
| Comorbidities | |||||
| No CAD | Pitavastatin | 1.00 | 1.00 | ||
| (N = 6057) | Atorvastatin | 1.09 (0.88–1.34) | 0.431 | 0.93 (0.75–1.16) | 0.535 |
| Rosuvastatin | 1.12 (0.91–1.37) | 0.279 | 1.01 (0.81–1.25) | 0.926 | |
| CAD | Pitavastatin | 1.00 | 1.00 | ||
| (N = 2280) | Atorvastatin | 1.17 (0.84–1.62) | 0.365 | 1.25 (0.89–1.74) | 0.202 |
| Rosuvastatin | 1.16 (0.85–1.59) | 0.357 | 1.47 (1.05–2.05) | 0.025 | |
| No HTN | Pitavastatin | 1.00 | 1.00 | ||
| (N = 4261) | Atorvastatin | 1.37 (1.03–1.82) | 0.031 | 0.87 (0.64–1.19) | 0.379 |
| Rosuvastatin | 1.44 (1.09–1.90) | 0.011 | 0.99 (0.73–1.34) | 0.934 | |
| HTN | Pitavastatin | 1.00 | 1.00 | ||
| (N = 4076) | Atorvastatin | 1.03 (0.82–1.30) | 0.778 | 1.13 (0.90–1.43) | 0.295 |
| Rosuvastatin | 1.05 (0.84–1.30) | 0.688 | 1.26 (1.00–1.59) | 0.047 | |
| No COPD | Pitavastatin | 1.00 | 1.00 | ||
| (N = 7360) | Atorvastatin | 1.23 (1.02–1.48) | 0.028 | 1.04 (0.86–1.27) | 0.691 |
| Rosuvastatin | 1.22 (1.02–1.46) | 0.026 | 1.09 (0.90–1.32) | 0.381 | |
| COPD | Pitavastatin | 1.00 | 1.00 | ||
| (N = 977) | Atorvastatin | 0.90 (0.52–1.55) | 0.698 | 0.99 (0.57–1.72) | 0.965 |
| Rosuvastatin | 1.31 (0.79–2.16) | 0.292 | 1.74 (1.02–2.94) | 0.040 | |
| No CKD | Pitavastatin | 1.00 | 1.00 | ||
| (N = 8064) | Atorvastatin | 1.17 (0.98–1.40) | 0.077 | 1.00 (0.83–1.21) | 0.999 |
| Rosuvastatin | 1.22 (1.03–1.44) | 0.024 | 1.08 (0.90–1.30) | 0.385 | |
| CKD | Pitavastatin | 1.00 | 1.00 | ||
| (N = 273) | Atorvastatin | 2.54 (0.78–8.32) | 0.123 | 2.67 (0.79–8.99) | 0.114 |
| Rosuvastatin | 3.08 (0.92–10.3) | 0.068 | 3.33 (0.93–11.9) | 0.064 | |
| No cancer | Pitavastatin | 1.00 | 1.00 | ||
| (N = 7676) | Atorvastatin | 1.28 (1.07–1.54) | 0.007 | 1.06 (0.88–1.29) | 0.549 |
| Rosuvastatin | 1.25 (1.05–1.49) | 0.012 | 1.09 (0.90–1.32) | 0.361 | |
| Cancer | Pitavastatin | 1.00 | 1.00 | ||
| (N = 661) | Atorvastatin | 0.65 (0.35–1.21) | 0.176 | 0.92 (0.48–1.75) | 0.797 |
| Rosuvastatin | 1.21 (0.66–2.22) | 0.534 | 1.62 (0.85–3.08) | 0.145 | |
| No IS | Pitavastatin | 1.00 | 1.00 | ||
| (N = 6933) | Atorvastatin | 1.28 (1.06–1.54) | 0.011 | 1.06 (0.86–1.29) | 0.601 |
| Rosuvastatin | 1.31 (1.09–1.58) | 0.004 | 1.16 (0.95–1.42) | 0.149 | |
| IS | Pitavastatin | 1.00 | 1.00 | ||
| (N = 1404) | Atorvastatin | 0.82 (0.53–1.28) | 0.384 | 0.89 (0.57–1.40) | 0.617 |
| Rosuvastatin | 0.87 (0.57–1.33) | 0.520 | 1.01 (0.65–1.56) | 0.972 | |
| No HS | Pitavastatin | 1.00 | 1.00 | ||
| (N = 8166) | Atorvastatin | 1.22 (1.03–1.46) | 0.024 | 1.05 (0.87–1.27) | 0.582 |
| Rosuvastatin | 1.26 (1.07–1.50) | 0.007 | 1.15 (0.96–1.38) | 0.142 | |
| HS | Pitavastatin | 1.00 | 1.00 | ||
| (N = 171) | Atorvastatin | 0.56 (0.18–1.79) | 0.328 | 0.43 (0.12–1.49) | 0.183 |
| Rosuvastatin | 0.50 (0.16–1.63) | 0.251 | 0.38 (0.10–1.42) | 0.151 | |
| No HF | Pitavastatin | 1.00 | 1.00 | ||
| (N = 7768) | Atorvastatin | 1.20 (1.00–1.44) | 0.045 | 1.00 (0.82–1.21) | 0.960 |
| Rosuvastatin | 1.24 (1.04–1.48) | 0.015 | 1.08 (0.90–1.31) | 0.407 | |
| HF | Pitavastatin | 1.00 | 1.00 | ||
| (N = 569) | Atorvastatin | 1.29 (0.70–2.36) | 0.411 | 1.54 (0.83–2.87) | 0.173 |
| Rosuvastatin | 1.30 (0.72–2.34) | 0.384 | 1.82 (0.96–3.43) | 0.066 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.-T.; Lin, C.; Tsai, M.-C.; Cheng, C.-C.; Chen, S.-J.; Liou, J.-T.; Lin, W.-S.; Cheng, S.-M.; Lin, C.-S.; Tsao, T.-P. Effects of Pitavastatin, Atorvastatin, and Rosuvastatin on the Risk of New-Onset Diabetes Mellitus: A Single-Center Cohort Study. Biomedicines 2020, 8, 499. https://doi.org/10.3390/biomedicines8110499
Liu W-T, Lin C, Tsai M-C, Cheng C-C, Chen S-J, Liou J-T, Lin W-S, Cheng S-M, Lin C-S, Tsao T-P. Effects of Pitavastatin, Atorvastatin, and Rosuvastatin on the Risk of New-Onset Diabetes Mellitus: A Single-Center Cohort Study. Biomedicines. 2020; 8(11):499. https://doi.org/10.3390/biomedicines8110499
Chicago/Turabian StyleLiu, Wei-Ting, Chin Lin, Min-Chien Tsai, Cheng-Chung Cheng, Sy-Jou Chen, Jun-Ting Liou, Wei-Shiang Lin, Shu-Meng Cheng, Chin-Sheng Lin, and Tien-Ping Tsao. 2020. "Effects of Pitavastatin, Atorvastatin, and Rosuvastatin on the Risk of New-Onset Diabetes Mellitus: A Single-Center Cohort Study" Biomedicines 8, no. 11: 499. https://doi.org/10.3390/biomedicines8110499
APA StyleLiu, W.-T., Lin, C., Tsai, M.-C., Cheng, C.-C., Chen, S.-J., Liou, J.-T., Lin, W.-S., Cheng, S.-M., Lin, C.-S., & Tsao, T.-P. (2020). Effects of Pitavastatin, Atorvastatin, and Rosuvastatin on the Risk of New-Onset Diabetes Mellitus: A Single-Center Cohort Study. Biomedicines, 8(11), 499. https://doi.org/10.3390/biomedicines8110499