
The Clinical Impact of the Omicron Variant on Octogenarian Hospitalized COVID-19 Patients: The Results from CoviCamp Cohort

 , , ,
, , ,  , , , ,
, , , ,  on behalf of CoviCam Groupadd
Show full author list
on behalf of CoviCam Groupadd
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Variables and Definitions
2.3. Statistical Analysis
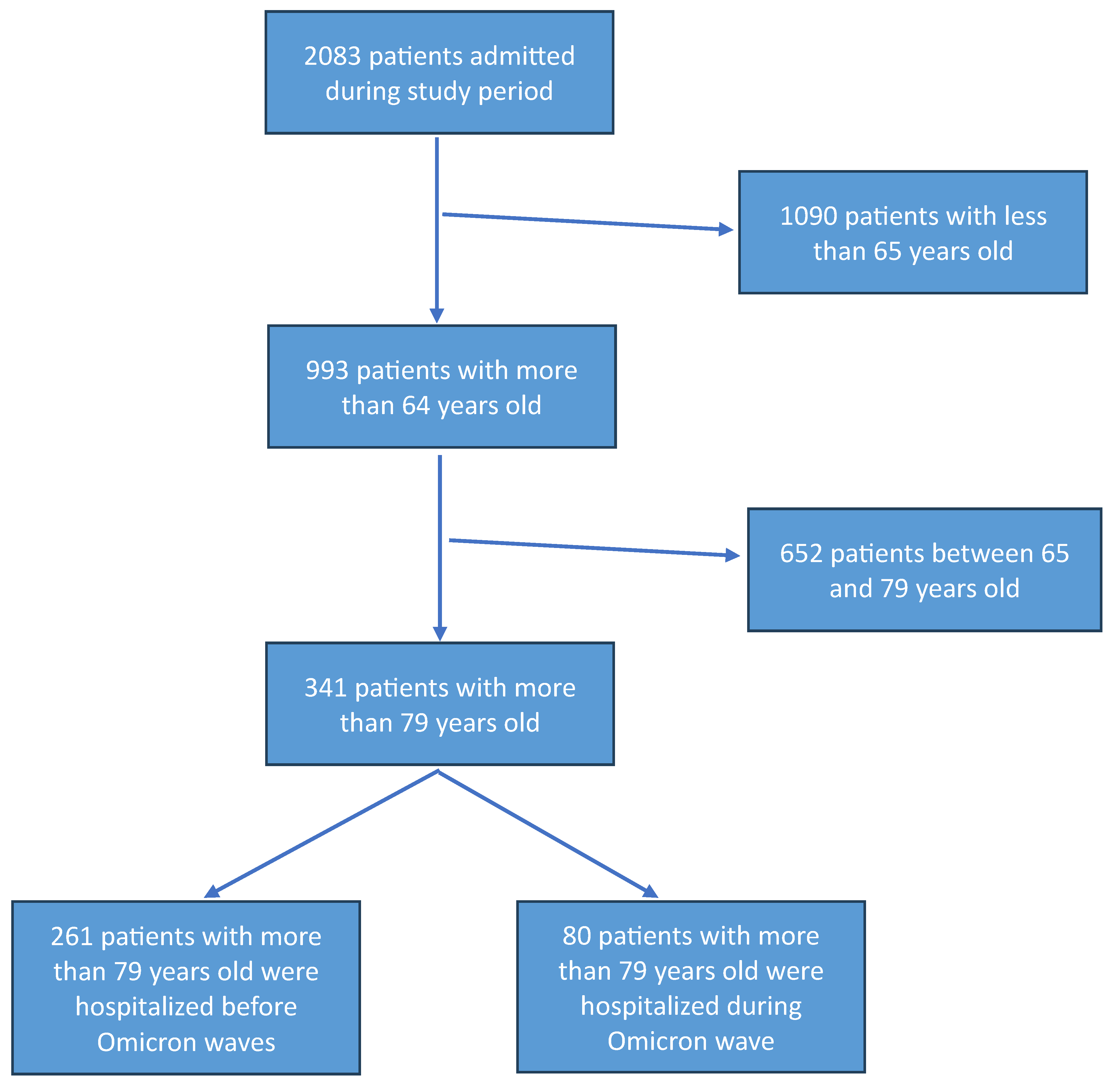
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Margolick, J.B.; Pawelec, G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef] [PubMed]
- Blomaard, L.C.; van der Linden, C.M.J.; van der Bol, J.M.; Jansen, S.W.M.; Polinder-Bos, H.A.; Willems, H.C.; Festen, J.; Barten, D.G.; Borgers, A.J.; Bos, J.C.; et al. Frailty is associated with in-hospital mortality in older hospitalised COVID-19 patients in the Netherlands: The COVID-OLD study. Age Ageing 2021, 50, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Rincon, J.M.; Buonaiuto, V.; Ricci, M.; Martín-Carmona, J.; Paredes-Ruíz, D.; Calderón-Moreno, M.; Rubio-Rivas, M.; Beato-Pérez, J.L.; Arnalich-Fernández, F.; Monge-Monge, D.; et al. Clinical characteristics and risk factors for mortality in very old patients hospitalized with COVID-19 in Spain. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, e28–e37. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; De Matteis, G.; Santoro, M.; Sabia, L.; Simeoni, B.; Candelli, M.; Ojetti, V.; Franceschi, F. Clinical characteristics and prognostic factors in COVID-19 patients aged ≥80 years. Geriatr. Gerontol. Int. 2020, 20, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Arabi, M.; Al-Najjar, Y.; Mhaimeed, N.; Salameh, M.A.; Paul, P.; AlAnni, J.; Abdelati, A.A.; Laswi, I.; Khanjar, B.; Al-Ali, D.; et al. Severity of the Omicron SARS-CoV-2 variant compared with the previous lineages: A systematic review. J. Cell. Mol. Med. 2023, 27, 1443–1464. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Fawaz, M.A.M.; Aisha, A. A comparative overview of SARS-CoV-2 and its variants of concern. Infez. Med. 2022, 30, 328–343. [Google Scholar] [CrossRef] [PubMed]
- Pisaturo, M.; Russo, A.; Pattapola, V.; Astorri, R.; Maggi, P.; Numis, F.G.; Gentile, I.; Sangiovanni, V.; Rossomando, A.; Gentile, V.; et al. Clinical Characterization of the Three Waves of COVID-19 Occurring in Southern Italy: Results of a Multicenter Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 16003. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Russo, A.; Pisaturo, M.; Palladino, R.; Maggi, P.; Numis, F.G.; Gentile, I.; Sangiovanni, V.; Esposito, V.; Punzi, R.; Calabria, G.; et al. Prognostic Value of Transaminases and Bilirubin Levels at Admission to Hospital on Disease Progression and Mortality in Patients with COVID-19-An Observational Retrospective Study. Pathogens 2022, 11, 652. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pisaturo, M.; Calò, F.; Russo, A.; Camaioni, C.; Giaccone, A.; Pinchera, B.; Gentile, I.; Simeone, F.; Iodice, A.; Maggi, P.; et al. Dementia as Risk Factor. for Severe Coronavirus Disease 2019: A Case-Control Study. Front. Aging Neurosci. 2021, 13, 698184. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grimaldi, P.; Russo, A.; Pisaturo, M.; Maggi, P.; Allegorico, E.; Gentile, I.; Sangiovanni, V.; Rossomando, A.; Pacilio, R.; Calabria, G.; et al. Clinical and epidemiological factors causing longer SARS-CoV 2 viral shedding: The results from the CoviCamp cohort. Infection 2024, 52, 439–446. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Russo, A.; Pisaturo, M.; De Luca, I.; Schettino, F.; Maggi, P.; Numis, F.G.; Gentile, I.; Sangiovanni, V.; Rossomando, A.M.; Gentile, V.; et al. Lactate dehydrogenase and PaO2/FiO2 ratio at admission helps to predict CT score in patients with COVID-19: An observational study. J. Infect. Public Health 2023, 16, 136–142. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Russo, A.; Pisaturo, M.; Zollo, V.; Martini, S.; Maggi, P.; Numis, F.G.; Gentile, I.; Sangiovanni, N.; Rossomando, A.M.; Bianco, V.; et al. Obesity as a Risk Factor of Severe Outcome of COVID-19: A Pair-Matched 1:2 Case-Control Study. J. Clin. Med. 2023, 12, 4055. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prevalenza e Distribuzione delle Varianti di SARS-CoV-2 di Interesse per la Sanità Pubblica in Italia. Available online: https://www.iss.it/documents/20126/0/Bollettino+varianti+n.15.pdf/be68a65c-b52c-2179-ac39-14bbc3292be2?t=1639148646776 (accessed on 18 June 2024).
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- IBM Corp. Released 2010: IBM SPSS Statistics for Macintosh OS, version 19.0; IBM Corp.: Armonk, NY, USA, 2010. [Google Scholar]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Adjei, S.; Hong, K.; Molinari, N.-A.M.; Bull-Otterson, L.; Ajani, U.A.; Gundlapalli, A.V.; Harris, A.M.; Hsu, J.; Kadri, S.S.; Starnes, J.; et al. Mortality Risk Among Patients Hospitalized Primarily for COVID-19 During the Omicron and Delta Variant Pandemic Periods—United States, April 2020–June 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Halfmann, P.J.; Iida, S.; Iwatsuki-Horimoto, K.; Maemura, T.; Kiso, M.; Scheaffer, S.M.; Darling, T.L.; Joshi, A.; Loeber, S.; Singh, G.; et al. SARS-CoV-2 Omicron virus causes attenuated disease in mice and hamsters. Nature 2022, 603, 687–692. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meng, B.; Abdullahi, A.; Ferreira, I.A.T.M.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 usage by SARS-CoV-2 Omicron impacts infectivity and fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hui, K.P.Y.; Ho, J.C.W.; Cheung, M.C.; Ng, K.C.; Ching, R.H.H.; Lai, K.L.; Kam, T.T.; Gu, H.; Sit, K.Y.; Hsin, M.K.Y.; et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Fericean, R.M.; Oancea, C.; Reddyreddy, A.R.; Rosca, O.; Bratosin, F.; Bloanca, V.; Citu, C.; Alambaram, S.; Vasamsetti, N.G.; Dumitru, C. Outcomes of Elderly Patients Hospitalized with the SARS-CoV-2 Omicron B.1.1.529 Variant: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 2150. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dudel, C.; Riffe, T.; Acosta, E.; van Raalte, A.; Strozza, C.; Myrskylä, M. Monitoring trends and differences in COVID-19 case-fatality rates using decomposition methods: Contributions of age structure and age-specific fatality. PLoS ONE 2020, 15, e0238904. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| At Least 80 y/o Patients During Other Waves | At Least 80 y/o Patients in Omicron Era | p Value | |
|---|---|---|---|
| Number of patients, n (%) | 261 | 80 | - |
| Age, median [IQR] | 83 [81–85] | 91 [88–92] | 0.0001 |
| Males, n (%) | 128 (49) | 33 (41.3) | 0.222 |
| Charlson Comorbidity Index, median [IQR] | 2 (1–4) | 5 (4–7) | 0.0001 |
| Hypertension, n (%) | 120 (48) | 50 (63.3) | 0.018 |
| Diabetes, n (%) | 60 (23.8) | 22 (28.8) | 0.432 |
| Overweight/Obesity, n (%) | 15 (9.4) | 2 (8.7) | 1 |
| COPD, n (%) | 31 (12.3) | 28 (36.8) | 0.0001 |
| Cardiovascular pathology, n (%) | 65 (25.7) | 37 (48.1) | 0.0001 |
| Dementia, n (%) | 15 (7.5) | 9 (12.2) | 0.221 |
| HIV, n (%) | 2 (0.8) | 0 (0) | 1 |
| Active tumor, n (%) | 19 (7.5) | 27 (35.1) | 0.0001 |
| Chronic liver disease, n (%) | 14 (5.7) | 2 (2.6) | 0.278 |
| CKD, n (%) | 21 (8.3) | 16 (21.1) | |
| Fever, n (%) | 125 (57.3) | 21 (28) | 0.0001 |
| Cough, n (%) | 65 (29.8) | 11 (15.3) | 0.015 |
| Asthenia, n (%) | 36 (17.8) | 20 (27.4) | 0.082 |
| Ageusia/Dysgeusia, n (%) | 7 (3.2) | 0 (0) | 0.196 |
| Anosmia/hyposmia, n (%) | 7 (3.2) | 0 (0) | 0.351 |
| Diarrhea, n (%) | 8 (3.7) | 6 (7.9) | 0.136 |
| Skin lesions, n (%) | 1 (0.5) | 6 (8.7) | 0.001 |
| Dyspnea, n (%) | 146 (67) | 36 (50) | 0.010 |
| P/F, median [IQR] | 214 [137–314] | 247 [202–319] | 0.044 |
| Time-to-negative swab, median [IQR] | 14 [0–21] | 14 [9–17] | 0.494 |
| Hospitalization days, median [IQR] | 14 [9–19] | 12 [9–17] | 0.054 |
| Severe/critical outcome, n (%) | 77 (36.3) | 9 (12.5) | 0.0001 |
| Death, n (%) | 27 (12.7) | 4 (5.6) | 0.124 |
| Other Waves, at Least 80 | Omicron Era, at Least 80 | p Value | |
|---|---|---|---|
| WBC, median [IQR] | 7970 [5800–10,300] | 6180 [4540–8100] | 0.0001 |
| Lymphocytes, median [IQR] | 880 [640–1251] | 1127 [659–1742] | 0.009 |
| Neu, median [IQR] | 6380 [4720–8620] | 3964 [2459–5754] | 0.0001 |
| INR, median [IQR] | 1.12 [1.04–1.24] | 1.07 [1.0–1.2] | 0.041 |
| Creatinine, median [IQR] | 0.9 [0.7–1.10] | 0.87 [0.71–1.12] | 0.741 |
| CPK, median [IQR] | 74 [42–146] | 44 [26–70] | 0.0001 |
| GPT, median [IQR] | 28 [20–51] | 23 [10–38] | 0.008 |
| Direct bilirubinemia, median [IQR] | 0.22 [0.17–0.35] | 0.29 [0.20–0.45] | 0.800 |
| Patient Mortality During Hospitalization | Other Waves, at Least 80 | Omicron Era, at Least 80 | p Value |
|---|---|---|---|
| Number of patients, n (%) | 27 (12.7) | 4 (5.6) | - |
| Age, median [IQR] | 82 [81–85] | 90 [88–96] | 0.0001 |
| Males, n (%) | 12 (44.4) | 3 (75) | 0.333 |
| Charlson Comorbidity Index, median [IQR] | 6 (5–9) | 9 (7–10) | 0.181 |
| Hypertension, n (%) | 14 (53.8) | 3 (75) | 0.613 |
| Diabetes, n (%) | 12 (46.2) | 0 (0) | 0.130 |
| Overweight/Obesity, n (%) | 2 (15.4) | 0 (0) | 1 |
| COPD, n (%) | 5 (19.2) | 2 (50) | 0.225 |
| Cardiovascular pathology, n (%) | 12 (46.2) | 3 (75) | 0.598 |
| Dementia, n (%) | 7 (38.9) | 3 (75) | 0.93 |
| HIV, n (%) | 0 (0) | 0 (0) | - |
| Active tumor, n (%) | 7 (26.9) | 2 (50) | 0.563 |
| Chronic liver disease, n (%) | 2 (7.7) | 0 (0) | 1 |
| CKD, n (%) | 6 (23.1) | 2 (50) | 0.284 |
| Fever, n (%) | 7 (35) | 0 (0) | 0.526 |
| Cough, n (%) | 4 (20) | 0 (0) | 1 |
| Asthenia, n (%) | 4 (21.1) | 2 (66.7) | 0.169 |
| Ageusia/Dysgeusia, n (%) | 0 (0) | 0 (0) | - |
| Anosmia/hyposmia, n (%) | 0 (0) | 0 (0) | - |
| Diarrhea, n (%) | 0 (0) | 0 (0) | - |
| Skin lesions, n (%) | 1 (5) | 0 (0) | 1 |
| Dyspnea, n (%) | 12 (60) | 2 (66.7) | 1 |
| Hospitalization days, median [IQR] | 8 [4–12] | 2 [1–21] | 0.464 |
| Oxygen administration mode, n (%) | |||
| Nasal cannulas/Venturi Mask | 9 (50) | 3 (75) | |
| High-flow nasal cannulas | 0 (0) | 1 (25) | 0.032 |
| CPAP/NIV | 9 (50) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grimaldi, P.; Pisaturo, M.; Russo, A.; Martini, S.; Ambrisi, F.; Milite, F.; Di Caprio, G.; Numis, F.G.; Gentile, I.; Sangiovanni, V.; et al. The Clinical Impact of the Omicron Variant on Octogenarian Hospitalized COVID-19 Patients: The Results from CoviCamp Cohort. Biomedicines 2025, 13, 1563. https://doi.org/10.3390/biomedicines13071563
Grimaldi P, Pisaturo M, Russo A, Martini S, Ambrisi F, Milite F, Di Caprio G, Numis FG, Gentile I, Sangiovanni V, et al. The Clinical Impact of the Omicron Variant on Octogenarian Hospitalized COVID-19 Patients: The Results from CoviCamp Cohort. Biomedicines. 2025; 13(7):1563. https://doi.org/10.3390/biomedicines13071563
Chicago/Turabian StyleGrimaldi, Pierantonio, Mariantonietta Pisaturo, Antonio Russo, Salvatore Martini, Francesca Ambrisi, Filomena Milite, Giovanni Di Caprio, Fabio Giuliano Numis, Ivan Gentile, Vincenzo Sangiovanni, and et al. 2025. "The Clinical Impact of the Omicron Variant on Octogenarian Hospitalized COVID-19 Patients: The Results from CoviCamp Cohort" Biomedicines 13, no. 7: 1563. https://doi.org/10.3390/biomedicines13071563
APA StyleGrimaldi, P., Pisaturo, M., Russo, A., Martini, S., Ambrisi, F., Milite, F., Di Caprio, G., Numis, F. G., Gentile, I., Sangiovanni, V., Esposito, V., Pacilio, R., Calabria, G., Pisapia, R., Carriero, C., Masullo, A., Manzillo, E., Russo, G., Parrella, R., ... Coppola, N., on behalf of CoviCam Group. (2025). The Clinical Impact of the Omicron Variant on Octogenarian Hospitalized COVID-19 Patients: The Results from CoviCamp Cohort. Biomedicines, 13(7), 1563. https://doi.org/10.3390/biomedicines13071563