

Histological Evaluation for Collagen Expression Prior to LVAD Implantation Is Useful to Estimate Weaning Success
 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Groups and Clinical Characteristics
2.2. Cardiac Tissue Preparation
2.3. RNA Isolation and cDNA Synthesis
2.4. Quantitative Real-Time Polymerase Chain Reaction
2.5. Masson–Goldner Trichrome Staining
2.6. Immunohistochemistry of Collagen I and Collagen III
2.7. Statistics
3. Results
3.1. Demographic and Clinical Characteristics
3.2. mRNA Expression of Collagen Type I and III
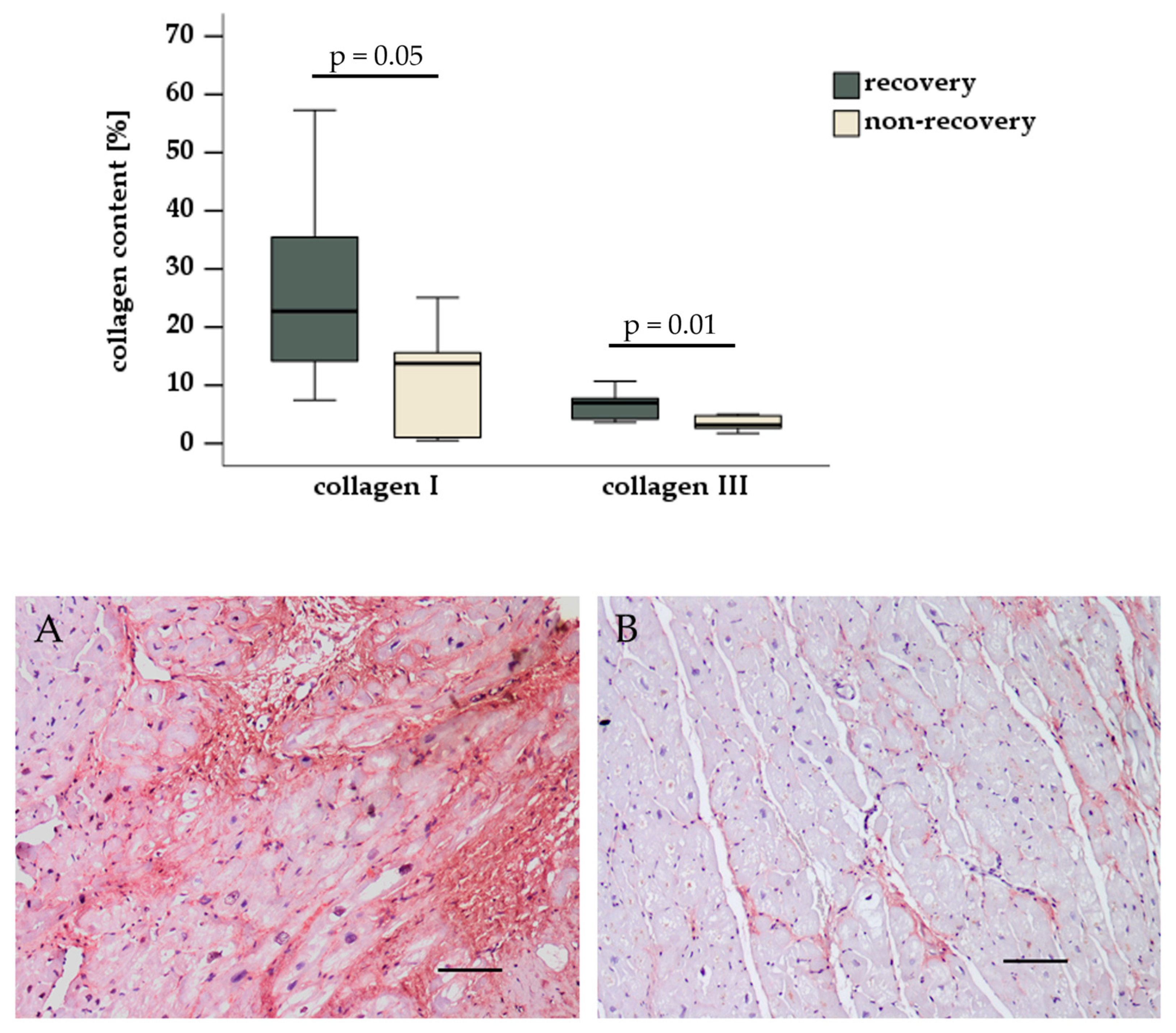
3.3. Histological and Immunohistochemical Evaluation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hrytsyna, Y.; Kneissler, S.; Kaufmann, F.; Müller, M.; Schoenrath, F.; Mulzer, J.; Sündermann, S.H.; Falk, V.; Potapov, E.; Knierim, J. Experience with a standardized protocol to predict successful explantation of left ventricular assist devices. J. Thorac. Cardiovasc. Surg. 2022, 164, 1922–1930.e2. [Google Scholar] [CrossRef] [PubMed]
- Knierim, J.; Tsyganenko, D.; Stein, J.; Mulzer, J.; Müller, M.; Hrytsyna, Y.; Schoenrath, F.; Falk, V.; Potapov, E. Results of non-elective withdrawal of continuous-flow left ventricular assist devices in selected patients. J. Heart Lung Transplant. 2023, 42, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Drakos, S.G.; Badolia, R.; Makaju, A.; Kyriakopoulos, C.P.; Wever-Pinzon, O.; Tracy, C.M.; Bakhtina, A.; Bia, R.; Parnell, T.; Taleb, I.; et al. Distinct Transcriptomic and Proteomic Profile Specifies Patients Who Have Heart Failure With Potential of Myocardial Recovery on Mechanical Unloading and Circulatory Support. Circulation 2023, 147, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, L.; Dieterlen, M.T.; Klaeske, K.; Haunschild, J.; Saeed, D.; Eifert, S.; Borger, M.A.; Jawad, K. Myostatin/AKT/FOXO Signaling Is Altered in Human Non-Ischemic Dilated Cardiomyopathy. Life 2022, 12, 1418. [Google Scholar] [CrossRef] [PubMed]
- Spampinato, R.A.; Marin-Cuartas, M.; van Kampen, A.; Fahr, F.; Sieg, F.; Strotdrees, E.; Jahnke, C.; Klaeske, K.; Wiesner, K.; Morningstar, J.E.; et al. Left ventricular fibrosis and CMR tissue characterization of papillary muscles in mitral valve prolapse patients. Int. J. Cardiovasc. Imaging 2024, 40, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.Y.; Feng, Y.; McTiernan, C.F.; Pei, W.; Moravec, C.S.; Wang, P.; Rosenblum, W.; Kormos, R.L.; Feldman, A.M. Downregulation of matrix metalloproteinases and reduction in collagen damage in the failing human heart after support with left ventricular assist devices. Circulation 2001, 104, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, B.A.; Stetson, S.J.; Perez-Verdia, A.; Youker, K.A.; Radovancevic, B.; Connelly, J.H.; Koerner, M.M.; Entman, M.E.; Frazier, O.H.; Noon, G.P.; et al. Regression of fibrosis and hypertrophy in failing myocardium following mechanical circulatory support. J. Heart Lung Transplant. 2001, 20, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, B.A.; Stetson, S.J.; Farmer, J.A.; Radovancevic, B.; Frazier, O.H.; Noon, G.P.; Entman, M.L.; Torre-Amione, G.; Youker, K.A. The implications for cardiac recovery of left ventricular assist device support on myocardial collagen content. Am. J. Surg. 2000, 180, 498–501; discussion 501–502. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. The Extracellular Matrix in Ischemic and Nonischemic Heart Failure. Circ. Res. 2019, 125, 117–146. [Google Scholar] [CrossRef] [PubMed]
- Bruggink, A.H.; van Oosterhout, M.F.; de Jonge, N.; Ivangh, B.; van Kuik, J.; Voorbij, R.H.A.M.; Cleutjens, J.P.M.; Gmelig-Meyling, F.H.J.; de Weger, R.A. Reverse remodeling of the myocardial extracellular matrix after prolonged left ventricular assist device support follows a biphasic pattern. J. Heart Lung Transplant. 2006, 25, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Klotz, S.; Foronjy, R.F.; Dickstein, M.L.; Gu, A.; Garrelds, I.M.; Jan Danser, A.H.; Oz, M.C.; D’Armiento, J.; Burkhoff, D. Mechanical unloading during left ventricular assist device support increases left ventricular collagen cross-linking and myocardial stiffness. Circulation 2005, 112, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Chaggar, P.S.; Williams, S.G.; Yonan, N.; Fildes, J.; Venkateswaran, R.; Shaw, S.M. Myocardial recovery with mechanical circulatory support. Eur. J. Heart Fail. 2016, 18, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. The extracellular matrix in myocardial injury, repair, and remodeling. J. Clin. Investig. 2017, 127, 1600–1612. [Google Scholar] [CrossRef] [PubMed]
- Lunde, I.G.; Rypdal, K.B.; Van Linthout, S.; Diez, J.; González, A. Myocardial fibrosis from the perspective of the extracellular matrix: Mechanisms to clinical impact. Matrix Biol. 2024, 134, 1–22. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Recovery Group n = 7 | Non-Recovery Group n = 7 | p Value | |
|---|---|---|---|
| Male gender | 2 (29%) | 2 (29%) | 1 |
| Age at LVAD implantation [yrs] | 57.0 ± 9.0 | 61.7 ± 6.4 | 0.14 |
| BMI [kg/m2] | 31.2 ± 7.5 | 27.1 ± 6.5 | 0.15 |
| LVEF [%] | 18.4 ± 7.3 | 16.4 ± 7.9 | 0.32 |
| NT-proBNP [ng/L] | 4619 ± 4120 | 7102 ± 3319 | 0.19 |
| NYHA classification Class III Class IV | 5 (71%) 2 (29%) | 2 (29%) 5 (71%) | 0.29 |
| Nicotine abuse Smoker Non-smoker Ex-smoker | 0 (0%) 5 (71%) 2 (29%) | 0 (0%) 5 (71%) 2 (29%) | 1 |
| Arterial hypertension | 4 (57%) | 5 (71%) | 1 |
| Coronary heart disease | 2 (29%) | 0 (0%) | 0.45 |
| Type 2 diabetes | 3 (43%) | 2 (29%) | 1 |
| Renal function eGFR [mL/min/1.73 m2] Creatinine [µmol/L] | 57.4 ± 26.0 131 ± 90 | 41.1 ± 19.8 151 ± 64 | 0.11 0.32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dieterlen, M.-T.; Schreiber, L.; Klaeske, K.; Jozwiak-Nozdrzykowska, J.; Borger, M.A.; Dashkevich, A.; Eifert, S.; Nozdrzykowski, M. Histological Evaluation for Collagen Expression Prior to LVAD Implantation Is Useful to Estimate Weaning Success. Biomedicines 2025, 13, 1515. https://doi.org/10.3390/biomedicines13071515
Dieterlen M-T, Schreiber L, Klaeske K, Jozwiak-Nozdrzykowska J, Borger MA, Dashkevich A, Eifert S, Nozdrzykowski M. Histological Evaluation for Collagen Expression Prior to LVAD Implantation Is Useful to Estimate Weaning Success. Biomedicines. 2025; 13(7):1515. https://doi.org/10.3390/biomedicines13071515
Chicago/Turabian StyleDieterlen, Maja-Theresa, Lea Schreiber, Kristin Klaeske, Joanna Jozwiak-Nozdrzykowska, Michael A. Borger, Alexey Dashkevich, Sandra Eifert, and Michal Nozdrzykowski. 2025. "Histological Evaluation for Collagen Expression Prior to LVAD Implantation Is Useful to Estimate Weaning Success" Biomedicines 13, no. 7: 1515. https://doi.org/10.3390/biomedicines13071515
APA StyleDieterlen, M.-T., Schreiber, L., Klaeske, K., Jozwiak-Nozdrzykowska, J., Borger, M. A., Dashkevich, A., Eifert, S., & Nozdrzykowski, M. (2025). Histological Evaluation for Collagen Expression Prior to LVAD Implantation Is Useful to Estimate Weaning Success. Biomedicines, 13(7), 1515. https://doi.org/10.3390/biomedicines13071515