
The Validation of the Parental Self-Efficacy Scale for Diabetes Management Among Parents of Children Wearing a Continuous Glucose Monitoring Sensor

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Data Collection
2.2. Standard Patient-Reported Outcome Measures (PROMs) Used in the Study
2.2.1. Parental Self-Efficacy Scale for Diabetes Management (PSESDM)
2.2.2. Chew Questionnaire
2.2.3. Hypoglycemia Fear Survey
2.2.4. EQ-5D-5L
2.2.5. ICECAP-A
2.2.6. EQ-5D-Y-3L
2.2.7. PedsQL Diab
2.3. Statistical Analysis
3. Results
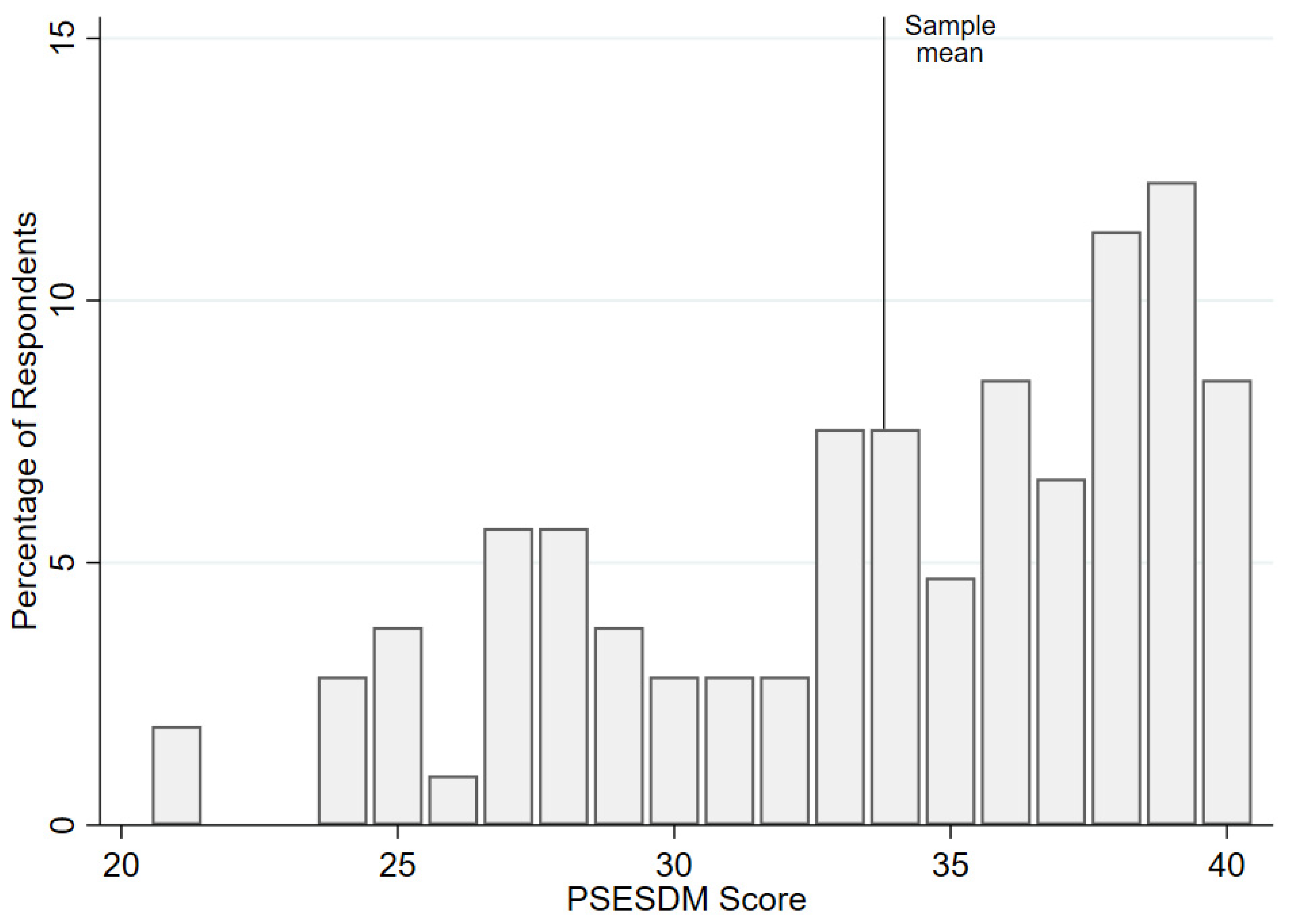
3.1. Sample Characteristics
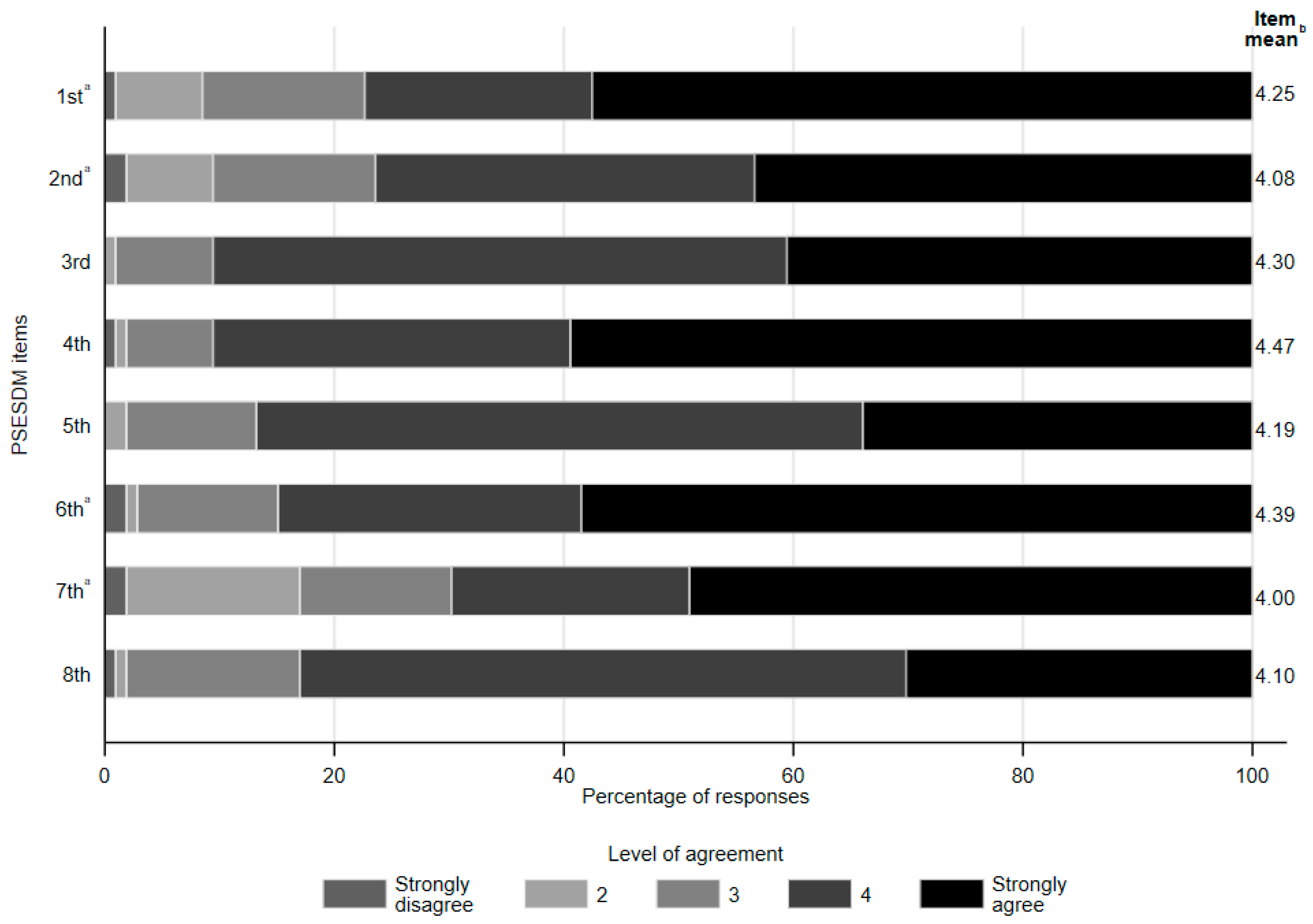
3.2. Self-Efficacy by PSESDM Items
3.3. Internal Consistency and Reliability
3.4. Associations with Socio-Demographic Characteristics, Treatment Modality, and Health Status
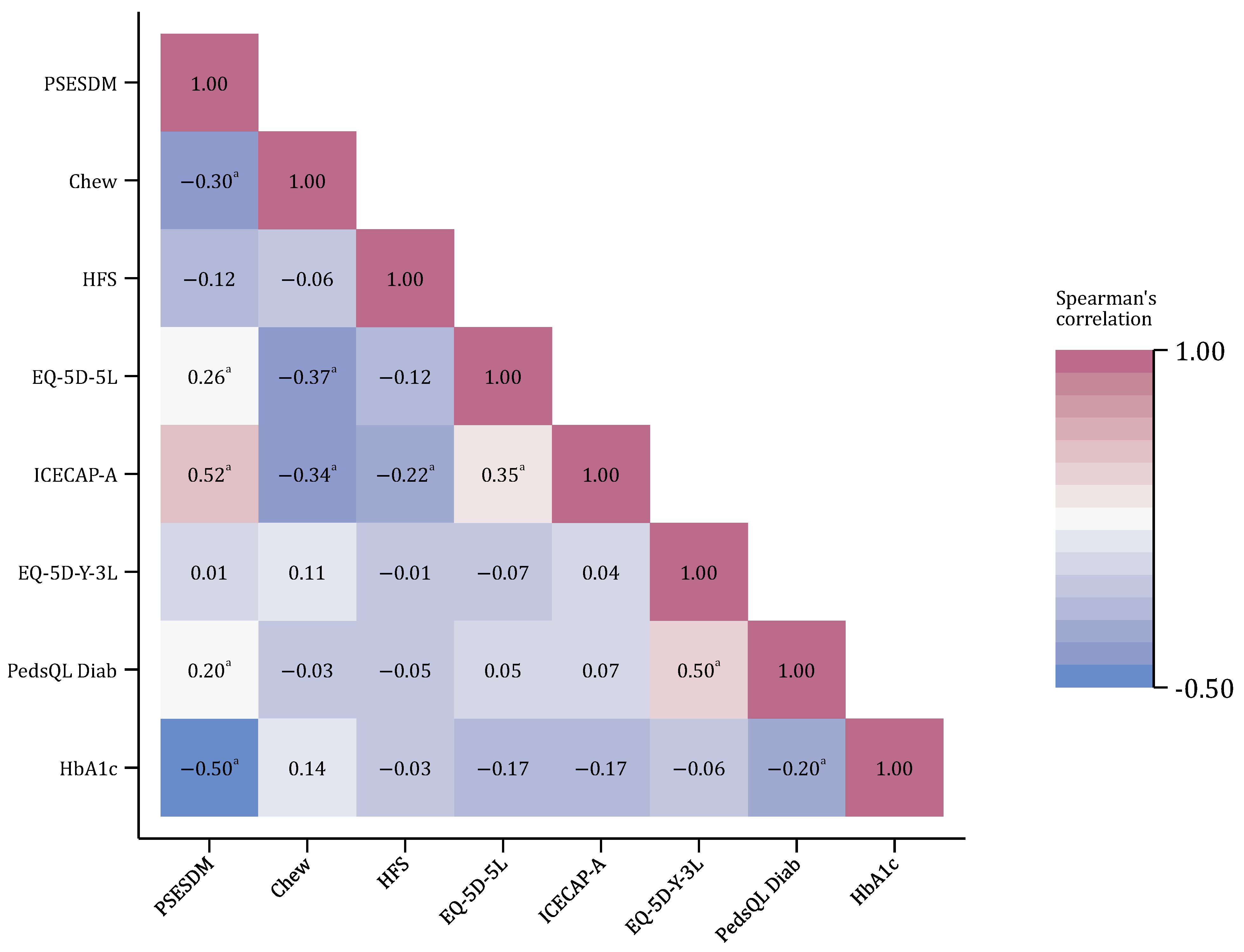
3.5. Associations with Parental Characteristics, Children’s Quality of Life, and Diabetes Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CGM | continuous glucose monitoring |
| HRQoL | health-related quality of life |
| PROM | Patient-Reported Outcome Measure |
| PSESDM | Parental Self-Efficacy Scale for Diabetes Management |
| T1DM | type 1 diabetes mellitus |
References
- Azimi, T.; Johnson, J.; Campbell, S.M.; Montesanti, S. Caregiver burden among parents of children with type 1 diabetes: A qualitative scoping review. Heliyon 2024, 10, e27539. [Google Scholar] [CrossRef]
- Kowalski, A.J. Can we really close the loop and how soon? Accelerating the availability of an artificial pancreas: A roadmap to better diabetes outcomes. Diabetes Technol. Ther. 2009, 11 (Suppl. 1), S113–S119. [Google Scholar] [CrossRef]
- Szalay, P.; Drexler, D.A.; Kovács, L. Exploring robustness in blood glucose control with unannounced meal intake for type-1 diabetes patient. Acta Polytech. Hung. 2023, 20, 27–46. [Google Scholar] [CrossRef]
- Guemes, A.; Cappon, G.; Hernandez, B.; Reddy, M.; Oliver, N.; Georgiou, P.; Herrero, P. Predicting quality of overnight glycaemic control in type 1 diabetes using binary classifiers. IEEE J. Biomed. Health Inform. 2019, 24, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Lukács, A.; Varga, B.; Kiss-Tóth, E.; Soós, A.; Barkai, L. Factors influencing the diabetes-specific health-related quality of life in children and adolescents with type 1 diabetes mellitus. J. Child Health Care 2014, 18, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Pauley, M.E.; Tommerdahl, K.L.; Snell-Bergeon, J.K.; Forlenza, G.P. Continuous glucose monitor, insulin pump, and automated insulin delivery therapies for type 1 diabetes: An update on potential for cardiovascular benefits. Curr. Cardiol. Rep. 2022, 24, 2043–2056. [Google Scholar] [CrossRef]
- Berg, C.A.; King, P.S.; Butler, J.M.; Pham, P.; Palmer, D.; Wiebe, D.J. Parental involvement and adolescents’ diabetes management: The mediating role of self-efficacy and externalizing and internalizing behaviors. J. Pediatr. Psychol. 2011, 36, 329–339. [Google Scholar] [CrossRef]
- Elbalshy, M.; Boucher, S.; Crocket, H.; Galland, B.; MacKenzie, C.; de Bock, M.I.; Jefferies, C.; Wiltshire, E.; Wheeler, B.J. Exploring parental experiences of using a do-it-yourself solution for continuous glucose monitoring among children and adolescents with type 1 diabetes: A qualitative study. J. Diabetes Sci. Technol. 2020, 14, 844–853. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Walker, R.J.; Smalls, B.L.; Hernandez-Tejada, M.A.; Campbell, J.A.; Egede, L.E. Effect of diabetes self-efficacy on glycemic control, medication adherence, self-care behaviors, and quality of life in a predominantly low-income, minority population. Ethn. Dis. 2014, 24, 349–355. [Google Scholar]
- Alwadiy, F.; Mok, E.; Dasgupta, K.; Rahme, E.; Frei, J.; Nakhla, M. Association of self-efficacy, transition readiness and diabetes distress with glycemic control in adolescents with type 1 diabetes preparing to transition to adult care. Can. J. Diabetes 2021, 45, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Leonard, B.; Skay, C.; Rheinberger, M. Self-management development in children and adolescents with diabetes: The role of maternal self-efficacy and conflict. J. Pediatr. Nurs. 1998, 13, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Streisand, R.; Swift, E.; Wickmark, T.; Chen, R.; Holmes, C.S. Pediatric parenting stress among parents of children with type 1 diabetes: The role of self-efficacy, responsibility, and fear. J. Pediatr. Psychol. 2005, 30, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.M.; Weaver, P.; Chen, R.; Streisand, R.; Holmes, C.S. A model of parental distress and factors that mediate its link with parental monitoring of youth diabetes care, adherence, and glycemic control. Health Psychol. 2016, 35, 1373–1382. [Google Scholar] [CrossRef]
- Marchante, A.N.; Pulgaron, E.R.; Daigre, A.; Patiño-Fernandez, A.M.; Sanchez, J.; Sanders, L.M.; Delamater, A.M. Measurement of parental self-efficacy for diabetes management in young children. Child. Health Care 2014, 43, 110–119. [Google Scholar] [CrossRef]
- Pulgarón, E.R.; Sanders, L.M.; Patiño-Fernandez, A.M.; Wile, D.; Sanchez, J.; Rothman, R.L.; Delamater, A.M. Glycemic control in young children with diabetes: The role of parental health literacy. Patient Educ. Couns. 2014, 94, 67–70. [Google Scholar] [CrossRef]
- Hölgyesi, Á.; Luczay, A.; Tóth-Heyn, P.; Muzslay, E.; Világos, E.; Szabó, A.J.; Baji, P.; Kovács, L.; Gulácsi, L.; Zrubka, Z.; et al. The impact of parental electronic health literacy on disease management and outcomes in pediatric type 1 diabetes mellitus: Cross-sectional clinical study. JMIR Pediatr. Parent. 2024, 7, e54807. [Google Scholar] [CrossRef]
- Gupta, O.T.; MacKenzie, M.; Burris, A.; Jenkins, B.B.; Collins, N.; Shade, M.; Santa-Sosa, E.; Stewart, S.M.; White, P.C. Camp-based multi-component intervention for families of young children with type 1 diabetes: A pilot and feasibility study. Pediatr. Diabetes 2017, 19, 761–768. [Google Scholar] [CrossRef]
- Amiri, F.; Vafa, M.; Gonder-Frederick, L.; Vajda, K.; Khamseh, M.; Abadi, A.; Salehpour, A. Evaluating fear of hypoglycemia, pediatric parenting stress, and self-efficacy among parents of children with type 1 diabetes and their correlation with glycemic control. Med. J. Islam. Repub. Iran 2018, 32, 697–703. [Google Scholar] [CrossRef]
- Pierce, J.S.; Wasserman, R.; Enlow, P.; Aroian, K.; Lee, J.; Wysocki, T. Benefit finding among parents of young children with type 1 diabetes. Pediatr. Diabetes 2019, 20, 652–660. [Google Scholar] [CrossRef]
- Wilcocks, C.P.; Enlow, P.; Wasserman, R.; Wysocki, T.; Lee, J.; Aroian, K.; Pierce, J.S. Development and evaluation of the pediatric diabetes routine questionnaire for parents of young children with type 1 diabetes. J. Clin. Psychol. Med. Settings 2023, 30, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Enlow, P.T.; Wasserman, R.; Aroian, K.; Lee, J.; Wysocki, T.; Pierce, J. Development and validation of the parent-preschoolers diabetes adjustment scale (PP-DAS). J. Pediatr. Psychol. 2019, 45, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Thorsteinsson, E.B.; Loi, N.M.; Rayner, K. Self-efficacy, relationship satisfaction, and social support: The quality of life of maternal caregivers of children with type 1 diabetes. PeerJ 2017, 5, e3961. [Google Scholar] [CrossRef]
- Albanese, A.M.; Russo, G.R.; Geller, P.A. The role of parental self-efficacy in parent and child well-being: A systematic review of associated outcomes. Child Care Health Dev. 2019, 45, 333–363. [Google Scholar] [CrossRef] [PubMed]
- Harpaz, G.; Grinshtain, Y.; Yaffe, Y. Parental self-efficacy predicted by parents’ subjective well-being and their parenting styles with possible role of help-seeking orientation from teachers. J. Psychol. 2021, 155, 571–587. [Google Scholar] [CrossRef]
- Benedetto, V.; Filipe, L.; Harris, C.; Spencer, J.; Hickson, C.; Clegg, A. Analytical frameworks and outcome measures in economic evaluations of digital health interventions: A methodological systematic review. Med. Decis. Mak. 2023, 43, 125–138. [Google Scholar] [CrossRef]
- Stanic, T.; Avsar, T.S.; Gomes, M. Economic evaluations of digital health interventions for children and adolescents: Systematic review. J. Med. Internet Res. 2023, 25, e45958. [Google Scholar] [CrossRef]
- Helter, T.M.; Coast, J.; Łaszewska, A.; Stamm, T.; Simon, J. Capability instruments in economic evaluations of health-related interventions: A comparative review of the literature. Qual. Life Res. 2020, 29, 1433–1464. [Google Scholar] [CrossRef]
- Leurent, B.; Gomes, M.; Carpenter, J.R. Missing data in trial-based cost-effectiveness analysis: An incomplete journey. Health Econ. 2018, 27, 1024–1040. [Google Scholar] [CrossRef]
- Mukherjee, K.; Gunsoy, N.B.; Kristy, R.M.; Cappelleri, J.C.; Roydhouse, J.; Stephenson, J.J.; Vanness, D.J.; Ramachandran, S.; Onwudiwe, N.C.; Pentakota, S.R.; et al. Handling missing data in health economics and outcomes research (HEOR): A systematic review and practical recommendations. PharmacoEconomics 2023, 41, 1589–1601. [Google Scholar] [CrossRef]
- Wallston, K.A.; Rothman, R.L.; Cherrington, A. Psychometric properties of the perceived diabetes self-management scale (PDSMS). J. Behav. Med. 2007, 30, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Chew, L.D.; Griffin, J.M.; Partin, M.R.; Noorbaloochi, S.; Grill, J.P.; Snyder, A.; Bradley, K.A.; Nugent, S.M.; Baines, A.D.; VanRyn, M. Validation of screening questions for limited health literacy in a large VA outpatient population. J. Gen. Intern. Med. 2008, 23, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Papp-Zipernovszky, O.; Náfrádi, L.; Schulz, P.J.; Csabai, M. So that each patient may comprehend: Measuring health literacy in hungary. Orv. Hetil. 2016, 157, 905–915. [Google Scholar] [CrossRef]
- Clarke, W.L.; Gonder-Frederick, L.A.; Snyder, A.L.; Cox, D.J. Maternal fear of hypoglycemia in their children with insulin dependent diabetes mellitus. J. Pediatr. Endocrinol. Metab. 1998, 11, 189–194. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Rencz, F.; Brodszky, V.; Gulácsi, L.; Golicki, D.; Ruzsa, G.; Pickard, A.S.; Law, E.H.; Péntek, M. Parallel valuation of the EQ-5D-3L and EQ-5D-5L by time trade-off in Hungary. Value Health 2020, 23, 1235–1245. [Google Scholar] [CrossRef]
- Al-Janabi, H.; Flynn, T.N.; Coast, J. Development of a self-report measure of capability wellbeing for adults: The ICECAP-A. Qual. Life Res. 2012, 21, 167–176. [Google Scholar] [CrossRef]
- Farkas, M.; Huynh, E.; Gulácsi, L.; Zrubka, Z.; Dobos, Á.; Kovács, L.; Baji, P.; Péntek, M. Development of population tariffs for the ICECAP-A instrument for Hungary and their comparison with the UK tariffs. Value Health 2021, 24, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Wille, N.; Badia, X.; Bonsel, G.; Burström, K.; Cavrini, G.; Devlin, N.; Egmar, A.-C.; Greiner, W.; Gusi, N.; Herdman, M.; et al. Development of the EQ-5D-Y: A child-friendly version of the EQ-5D. Qual. Life Res. 2010, 19, 875–886. [Google Scholar] [CrossRef]
- Rencz, F.; Ruzsa, G.; Bató, A.; Yang, Z.; Finch, A.P.; Brodszky, V. Value set for the EQ-5D-Y-3L in Hungary. PharmacoEconomics 2022, 40, 205–215. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Jacobs, J.R.; Gottschalk, M.; Kaufman, F.; Jones, K.L. The pedsql in type 1 and type 2 diabetes: Reliability and validity of the pediatric quality of life inventory generic core scales and type 1 diabetes module. Diabetes Care 2003, 26, 631–637. [Google Scholar] [CrossRef]
- Lukács, A.; Simon, N.; Varga, B.; Kiss-Tóth, E.; Barkai, L. Hungarian adaptation of the pediatric quality of life inventory™ 3.0 diabetes module. Orv. Hetil. 2011, 152, 1837–1842. [Google Scholar] [CrossRef] [PubMed]
- de Bock, M.; Agwu, J.C.; Deabreu, M.; Dovc, K.; Maahs, D.M.; Marcovecchio, M.L.; Mahmud, F.H.; Nóvoa-Medina, Y.; Priyambada, L.; Smart, C.E.; et al. International society for pediatric and adolescent diabetes clinical practice consensus guidelines 2024: Glycemic targets. Horm. Res. Paediatr. 2024, 97, 546–554. [Google Scholar] [PubMed]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Cohen, R.; Swerdlik, M. Psychological Testing and Assessment: An Introduction to Tests and Measurement, 7th ed.; McGraw Hill: New York, NY, USA, 2009. [Google Scholar]
- Cohen, J. Set correlation and contingency tables. Appl. Psychol. Meas. 1988, 12, 425–434. [Google Scholar] [CrossRef]
- Bassi, G.; Mancinelli, E.; Di Riso, D.; Salcuni, S. Parental stress, anxiety and depression symptoms associated with self-efficacy in paediatric type 1 diabetes: A literature review. Int. J. Environ. Res. Public Health 2020, 18, 152. [Google Scholar] [CrossRef]
- Zah, V.; Burrell, A.; Asche, C.; Zrubka, Z. Paying for digital health interventions—What evidence is needed? Acta Polytech. Hung. 2022, 19, 179–199. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| N | % | PSESDM Score | |||
|---|---|---|---|---|---|
| Mean (SD) | Median (Range) | ||||
| Total | 106 | 100 | 33.8 (5.0) | 35 (21–40) | - |
| Parents | |||||
| Sex | |||||
| Female | 84 | 79.3 | 33.6 (5.2) | 34.5 (21–40) | p = 0.667 |
| Male | 22 | 20.7 | 34.5 (4.4) | 35.5 (25–40) | Χ2(1) = 0.185 |
| Age | |||||
| 30–39 | 24 | 22.6 | 32.5 (5.9) | 32.5 (21–40) | p = 0.415 |
| 40–49 | 78 | 73.6 | 34.2 (4.8) | 35.5 (21–40) | Χ2(3) = 2.852 |
| 50–59 | 3 | 2.8 | 34.7 (2.3) | 36 (32–36) | |
| 60–69 | 1 | 0.9 | 27.0 (-) | 27(-) | |
| Education | |||||
| Primary | 4 | 3.8 | 31.3 (6.5) | 30 (25–40) | p = 0.165 |
| Secondary | 47 | 44.3 | 32.9 (5.4) | 33 (21–40) | Χ2(2) = 3.603 |
| Tertiary | 55 | 51.9 | 34.8 (4.5) | 36 (21–40) | |
| Residency | |||||
| Capital | 31 | 29.3 | 34.7 (5.0) | 36 (21–40) | p = 0.429 |
| Urban | 54 | 50.9 | 33.6 (4.6) | 34 (24–40) | Χ2(2) = 1.694 |
| Rural | 21 | 19.8 | 33.0 (6.2) | 35 (21–40) | |
| Family status | |||||
| Married | 76 | 71.7 | 34.0 (5.0) | 35.5 (21–40) | p = 0.478 |
| Domestic relationship | 14 | 13.2 | 34.9 (4.3) | 36.5 (25–40) | Χ2(4) = 3.502 |
| Single | 5 | 4.7 | 31.0 (7.8) | 27 (24–40) | |
| Divorced | 8 | 7.6 | 31.3 (4.5) | 31 (26–39) | |
| Other | 3 | 2.8 | 34.0 (5.0) | 34 (29–39) | |
| Employment | |||||
| Full-time | 71 | 67.0 | 34.6 (4.6) | 36 (21–40) | p = 0.098 |
| Part-time | 18 | 17.0 | 31.2 (5.4) | 29 (24–40) | Χ2(5) = 9.279 |
| Retired | 2 | 1.9 | 30.0 (4.2) | 30 (27–33) | |
| Unemployed | 2 | 1.9 | 30.0 (1.4) | 30 (29–31) | |
| Homemaker | 7 | 6.6 | 32.6 (7.3) | 33 (21–40) | |
| Other | 6 | 5.7 | 36.0 (5.0) | 37 (27–40) | |
| Net per capita income (EUR) | |||||
| <500 | 35 | 33.0 | 31.7 (5.5) | 32 (21–40) | p = 0.003 |
| 501–1000 | 37 | 34.9 | 34.0 (4.0) | 35 (25–40) | Χ2(3) = 13.742 |
| 1001–1500 | 11 | 10.4 | 37.4 (3.7) | 39 (27–40) | |
| >1500 | 1 | 0.9 | 27.0 (-) | 27 (-) | |
| Missing | 22 | 20.8 | - | - | |
| Children | |||||
| Sex | |||||
| Female | 52 | 49.1 | 34.8 (4.4) | 36 (25–40) | p = 0.072 |
| Male | 54 | 50.9 | 32.8 (5.5) | 33 (21–40) | Χ2(1) = 3.230 |
| Age | |||||
| 7–10 | 27 | 25.5 | 33.6 (5.3) | 35 (24–40) | p = 0.965 |
| 11–14 | 76 | 71.7 | 33.9 (5.0) | 35 (21–40) | Χ2(2) = 0.072 |
| 15–18 | 3 | 2.8 | 34.0 (6.0) | 34 (28–40) | |
| Treatment | |||||
| Pen + CGM | 55 | 51.9 | 32.9 (5.2) | 34 (21–40) | p = 0.100 |
| Pump + CGM | 51 | 48.1 | 34.7 (4.7) | 36 (21–40) | Χ2(1) = 2.709 |
| HbA1c below target (>7.0%) | |||||
| Yes | 41 | 38.7 | 36.3 (3.8) | 37 (24–40) | <0.001 |
| No | 65 | 61.3 | 32.2 (5.1) | 33 (21–40) | Χ2(1) = 1.905 |
| Item–Total Score Correlation | Corrected Item–Total Score Correlation a | Cronbach’s Alpha, If Item Is Deleted | |
|---|---|---|---|
| Item 1 | 0.733 | 0.645 | 0.842 |
| Item 2 | 0.741 | 0.647 | 0.830 |
| Item 3 | 0.678 | 0.590 | 0.846 |
| Item 4 | 0.692 | 0.629 | 0.840 |
| Item 5 | 0.743 | 0.660 | 0.837 |
| Item 6 | 0.694 | 0.596 | 0.842 |
| Item 7 | 0.791 | 0.671 | 0.832 |
| Item 8 | 0.734 | 0.622 | 0.847 |
| Full scale | - | - | 0.857 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hölgyesi, Á.; Luczay, A.; Tóth-Heyn, P.; Muzslay, E.; Világos, E.; Szabó, A.J.; Baji, P.; Kovács, L.; Gulácsi, L.; Zrubka, Z.; et al. The Validation of the Parental Self-Efficacy Scale for Diabetes Management Among Parents of Children Wearing a Continuous Glucose Monitoring Sensor. Biomedicines 2025, 13, 1309. https://doi.org/10.3390/biomedicines13061309
Hölgyesi Á, Luczay A, Tóth-Heyn P, Muzslay E, Világos E, Szabó AJ, Baji P, Kovács L, Gulácsi L, Zrubka Z, et al. The Validation of the Parental Self-Efficacy Scale for Diabetes Management Among Parents of Children Wearing a Continuous Glucose Monitoring Sensor. Biomedicines. 2025; 13(6):1309. https://doi.org/10.3390/biomedicines13061309
Chicago/Turabian StyleHölgyesi, Áron, Andrea Luczay, Péter Tóth-Heyn, Eszter Muzslay, Eszter Világos, Attila J. Szabó, Petra Baji, Levente Kovács, László Gulácsi, Zsombor Zrubka, and et al. 2025. "The Validation of the Parental Self-Efficacy Scale for Diabetes Management Among Parents of Children Wearing a Continuous Glucose Monitoring Sensor" Biomedicines 13, no. 6: 1309. https://doi.org/10.3390/biomedicines13061309
APA StyleHölgyesi, Á., Luczay, A., Tóth-Heyn, P., Muzslay, E., Világos, E., Szabó, A. J., Baji, P., Kovács, L., Gulácsi, L., Zrubka, Z., & Péntek, M. (2025). The Validation of the Parental Self-Efficacy Scale for Diabetes Management Among Parents of Children Wearing a Continuous Glucose Monitoring Sensor. Biomedicines, 13(6), 1309. https://doi.org/10.3390/biomedicines13061309