

Safety and Efficacy of Regorafenib and 5-Fluorouracil Combination Therapy in Refractory Metastatic Colorectal Cancer After Third-Line Treatment: An Institutional Experience


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Patients’ Characteristics
2.3. Treatment and Assessment
3. Results
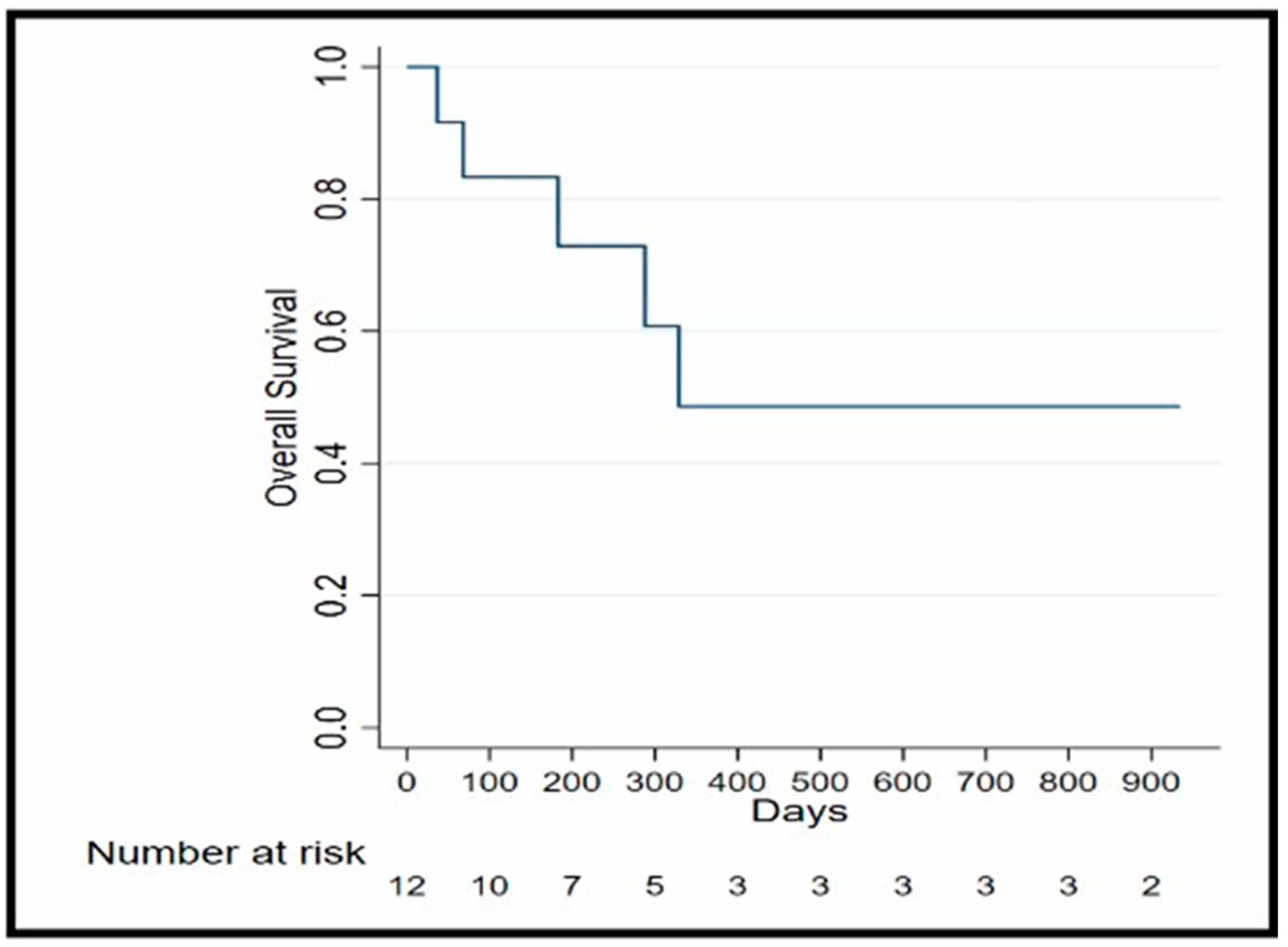
3.1. Efficacy
3.2. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Navarro, M.; Nicolas, A.; Ferrandez, A.; Lanas, A. Colorectal cancer population screening programs worldwide in 2016: An update. World J. Gastroenterol. 2016, 23, 3632. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef] [PubMed]
- Biller, L.H.; Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer. JAMA 2021, 325, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.S.; Chadda, S.D.; Zhao, Z.; Barber, B.L.; Sykes, D.P. A systematic review of treatment guidelines for metastatic colorectal cancer. Color. Dis. 2012, 14, e31–e47. [Google Scholar] [CrossRef] [PubMed]
- Haque, E.; Muhsen, I.N.; Esmail, A.; Umoru, G.; Mylavarapu, C.; Ajewole, V.B.; Abdelrahim, M. Case report: Efficacy and safety of regorafenib plus fluorouracil combination therapy in the treatment of refractory metastatic colorectal cancer. Front. Oncol. 2022, 12, 992455. [Google Scholar] [CrossRef]
- Strumberg, D.; Scheulen, M.E.; Schultheis, B.; Richly, H.; Frost, A.; Büchert, M.; Christensen, O.; Jeffers, M.; Heinig, R.; Boix, O.; et al. Regorafenib (BAY 73-4506) in advanced colorectal cancer: A phase I study. Br. J. Cancer 2012, 106, 1722–1727. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.; Esmail, A.; Abdelrahim, M. Triple-regimen of vemurafenib, irinotecan, and cetuximab for the treatment of BRAFV600E-mutant CRC: A case report and review. Front. Pharmacol. 2021, 12, 795381. [Google Scholar] [CrossRef] [PubMed]
- Sethy, C.; Kundu, C.N. 5-Fluorouracil (5-FU) resistance and the new strategy to enhance the sensitivity against cancer: Implication of DNA repair inhibition. Biomed. Pharmacother. 2021, 137, 111285. [Google Scholar] [CrossRef] [PubMed]
- García-Alfonso, P.; Martín, A.J.M.; Morán, L.O.; Alsar, J.S.; Pérez-Solero, G.T.; Codesido, M.B.; Ferrandiz, P.A.C.; Cicala, S.G. Oral drugs in the treatment of metastatic colorectal cancer. Ther. Adv. Med. Oncol. 2021, 13, 17588359211009001. [Google Scholar] [CrossRef] [PubMed]
- Crona, D.J.; Keisler, M.D.; Walko, C.M. Regorafenib:A Novel Multitargeted Tyrosine Kinase Inhibitor for Colorectal Cancer and Gastrointestinal Stromal Tumors. Ann. Pharmacother. 2013, 47, 1685–1696. [Google Scholar] [CrossRef] [PubMed]
- Cousin, S.; Cantarel, C.; Guegan, J.-P.; Gomez-Roca, C.; Metges, J.-P.; Adenis, A.; Pernot, S.; Bellera, C.; Kind, M.; Auzanneau, C.; et al. Regorafenib-Avelumab Combination in Patients with Microsatellite Stable Colorectal Cancer (REGOMUNE): A Single-arm, Open-label, Phase II Trial. Clin. Cancer Res. 2021, 27, 2139–2147. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Han, L.; Wu, S.; Qu, X.; Li, Q.; Zhao, C.; Zhou, J.; Jin, X.; Wang, Y.; Yan, D.; et al. Real-world outcomes of regorafenib combined with immune checkpoint inhibitors in patients with advanced or metastatic microsatellite stable colorectal cancer: A multicenter study. Cancer Immunol. Immunother. 2022, 71, 1443–1451. [Google Scholar] [CrossRef]
- Calcagno, F.; Lenoble, S.; Lakkis, Z.; Nguyen, T.; Limat, S.; Borg, C.; Jary, M.; Kim, S.; Nerich, V. Efficacy, Safety and Cost of Regorafenib in Patients with Metastatic Colorectal Cancer in French Clinical Practice. Clin. Med. Insights Oncol. 2016, 10, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Marks, E.I.; Tan, C.; Zhang, J.; Zhou, L.; Yang, Z.; Scicchitano, A.; El-Deiry, W.S. El-Deiry, Regorafenib with a fluoropyrimidine for metastatic colorectal cancer after progression on multiple 5-FU-containing combination therapies and regorafenib monotherapy. Cancer Biol. Ther. 2016, 16, 1710–1719. [Google Scholar] [CrossRef] [PubMed]
- Bekaii-Saab, T.; Ou, F.; Anderson, D.; Ahn, D.; Boland, P.; Ciombor, K.; Jacobs, N.; Desnoyers, R.; Cleary, J.; Meyers, J.; et al. Regorafenib dose optimization study (ReDOS): Randomized phase II trial to evaluate dosing strategies for regorafenib in refractory metastatic colorectal cancer (mCRC) (a)over-cap(sic) An ACCRU Network study. Ann. Oncol. 2018, 29 (Suppl. S5), v105. [Google Scholar] [CrossRef]
- Zanwar, S.; Ostwal, V.; Gupta, S.; Sirohi, B.; Toshniwal, A.; Shetty, N.; Banavali, S. Toxicity and early outcomes of regorafenib in multiply pre-treated metastatic colorectal adenocarcinoma-experience from a tertiary cancer centre in India. Ann. Transl. Med. 2016, 4, 74. [Google Scholar] [PubMed]
- Yoon, S.E.; Lee, S.J.; Lee, J.; Park, S.H.; Park, J.O.; Lim, H.Y.; Kang, W.K.; Park, Y.S.; Kim, S.T. The use of regorafenib for patients with refractory metastatic colorectal cancer in clinical practice. OncoTargets Ther. 2018, 12, 225–231. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Patient | Age at Therapy Initiation (Gender) | Diagnosis (Stage at Diagnosis) | Chemotherapies Prior to Rego + 5-FU (Including Maintenance Therapy) | History of Tumor Resection | Mutations | Sites of Metastasis | Comorbidities |
|---|---|---|---|---|---|---|---|
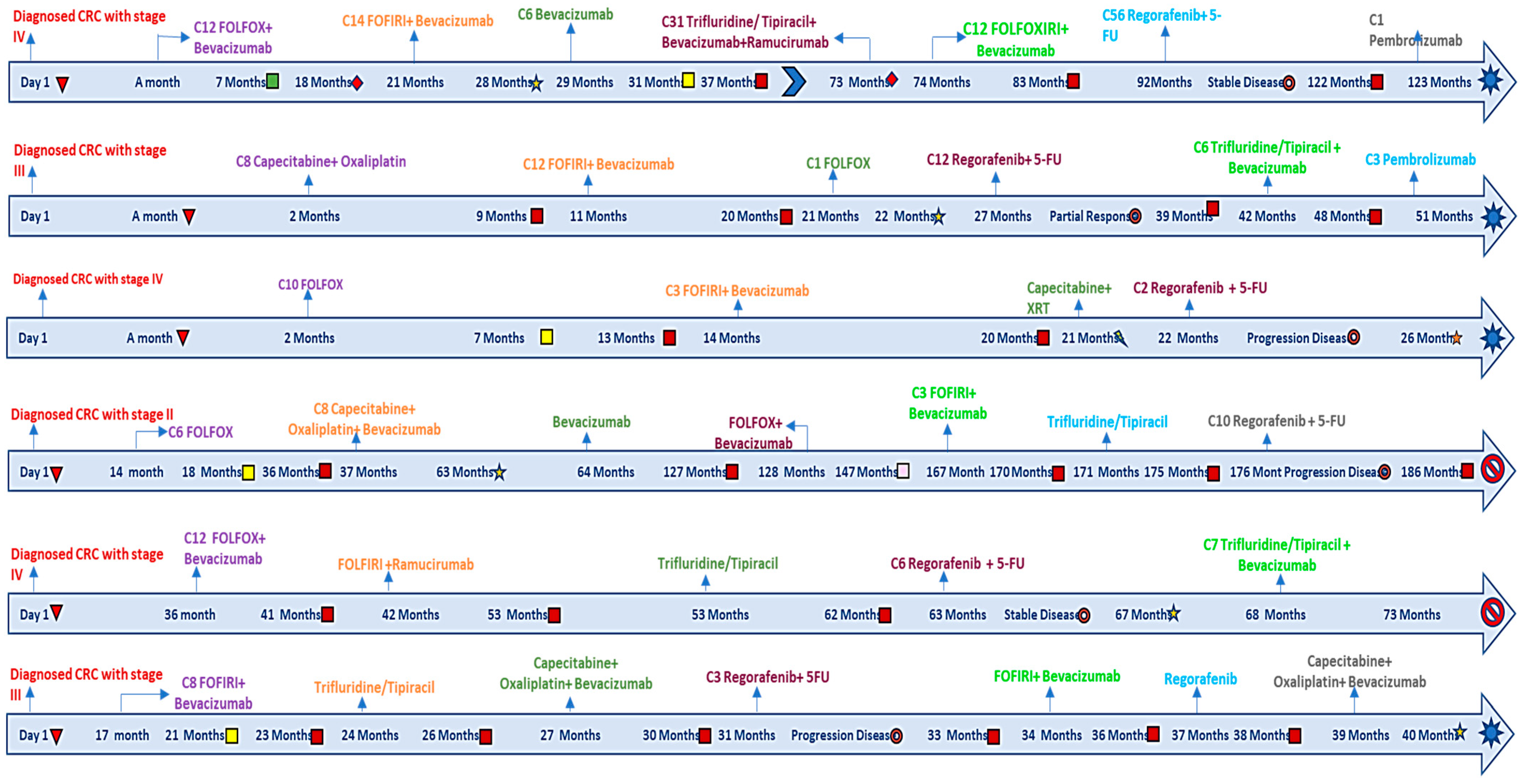
| 1 | 65 (Female) | Left-sided colon cancer. (IV) | FOLFOX + bevacizumab FOLFIRI + bevacizumab bevacizumab monotherapy Trifluridine/Tipiracil initially with bevacizumab and then Ramucirumab FOLFIRINOX + bevacizumab | Yes | KRAS-mutant (G12D) NRAS-neg BRAF-neg MSI-stable | Peritoneum, ovaries, abdominal wall, liver | Osteoarthritis |
| 2 | 48 (Male) | Left-sided colon cancer. (III) | Capecitabine + Oxaliplatin Capecitabine monotherapy FOLFIRI + bevacizumab FOLFOX + Oxaliplatin | Yes | KRAS-mutated MYC-mutated TP53-mutated NTRK 1–3-neg | Liver | Hypertension |
| 3 | 58 (Male) | Right-sided colon cancer (IV) | FOLFOX FOLFIRI + bevacizumab Restarted FOLFIRI + bevacizumab. | Yes | KRAS-mutated TP53-mutated PIK3C-mutated BRAF-neg NTRK 1–3-neg MSI-stable HER-2-neg NRAS-neg | Liver and lung | Hypertension Diabetes Mellitus |
| 4 | 46 (Male) | Left-sided colon cancer. (II) | FOLFOX Capecitabine + oxaliplatin + bevacizumab Capecitabine + bevacizumab bevacizumab FOLFOX + bevacizumab bevacizumab + 5-FU FOLFOX + bevacizumab FOLFIRI + bevacizumab Trifluridine/Tipiracil | Yes | NRAS mutation MSI-stable, FAP with pathogenic APC variant. HER2 negative. | Liver, lungs, bone, and peritoneum | None |
| 5 | 63 (Female) | Left-sided colon cancer (IV) | FOLFOX + bevacizumab FOLFIRI + ramucirumab FOLFIRI + aflibercept Trifluridine/Tipiracil 5-FU | Yes | NRAS-mutated KRAS-neg BRAF-neg MSI-Stable | Liver and lung | Hypothyroidism Nephropathy |
| 6 | 58 (Male) | Left-sided colon cancer (IV) | FOLFOX FOLFIRI + bevacizumab Trifluridine/Tipiracil Capecitabine + oxaliplatin + bevacizumab | Yes | -BRAF-neg -KRAS-mutated -NRAS-neg -HRAS-neg -MSI-Stable | Liver and lung | Hypertension Hypercholesterolemia |
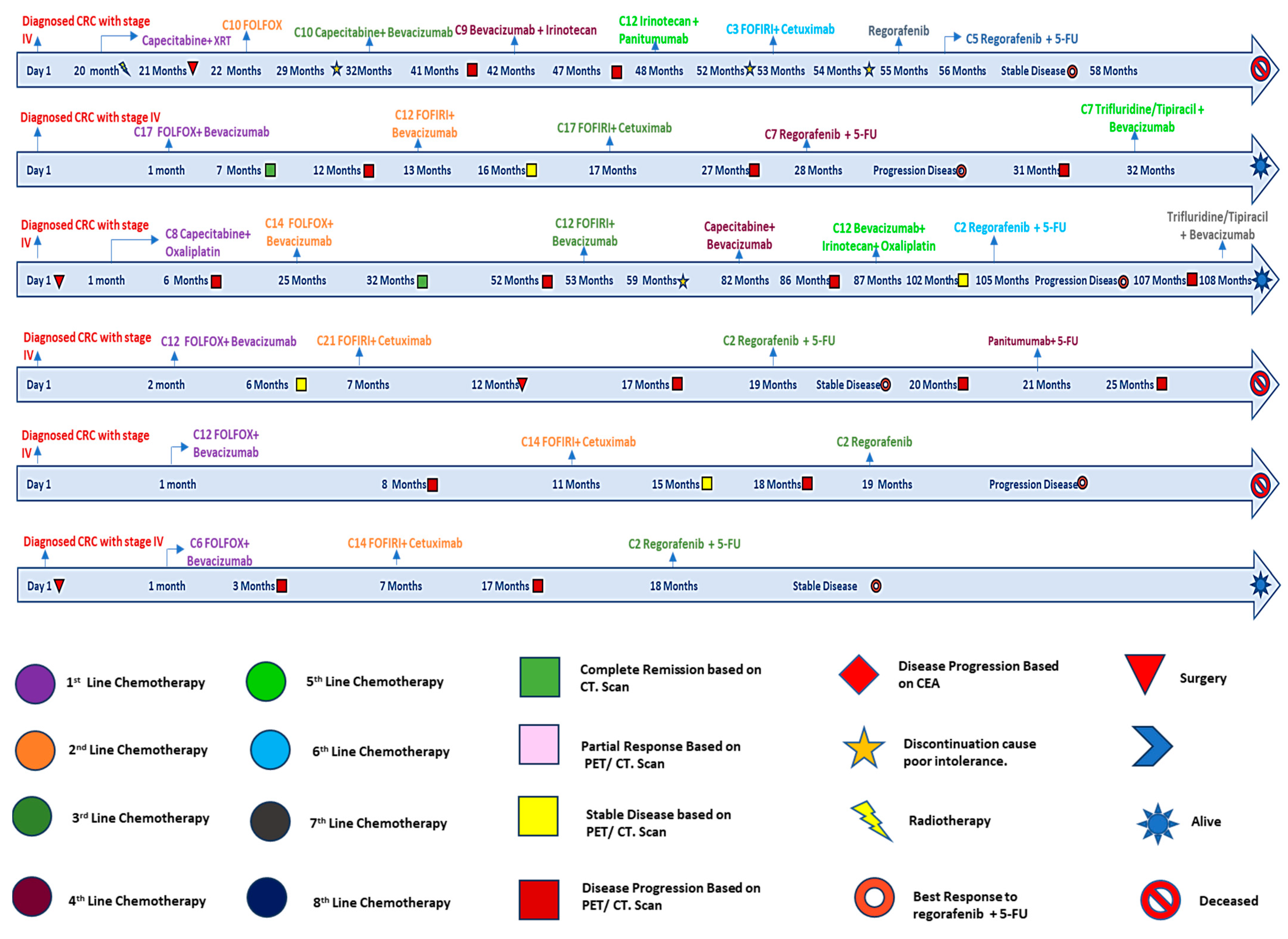
| 7 | 59 (Male) | Rectal cancer (IV) | Capecitabine FOLFOX capecitabine + bevacizumab irinotecan + bevacizumab bevacizumab panitumumab + irinotecan cetuximab + irinotecan 5-FU + irinotecan + cetuximab regorafenib monotherapy | Yes | KRAS wild type MSI stable | Liver and lung | Hypertension Gout |
| 8 | 46 (Female) | Rectal cancer (IV) | FOLFOX + bevacizumab FOLFIRI + bevacizumab FOLFIRI + cetuximab | No | BRAF D594G pMMR PIK3CA MSI stable | Lung, Liver, Bone, Supraclavicular Lymph nodes | Hypertension |
| 9 | 51 (Male) | Right-sided colon cancer (IV) | Capecitabine + oxaliplatin FOLFOX + bevacizumab FOLFIRI + bevacizumab capecitabine + bevacizumab bevacizumab + irinotecan + oxaliplatin | Yes | P53 MSS | Liver and Lung | Hypertension |
| 10 | 52 (Male) | Rectosigmoid cancer (IV) | FOLFOX + bevacizumab FOLFIRI + cetuximab | Yes | FGFR1 MYC MSS | Liver, Lung and Peritoneum | Hypertension |
| 11 | 60 (Male) | Rectal cancer (IV) | FOLFOX + bevacizumab FOLFIRI + cetuximab | No | HRAS G13C pMMR | Liver and Lymph nodes | Hypertension, Diabetes Mellitus, Asthma, Chronic Kidney Disease, Stroke |
| 12 | 40 (Female) | Sigmoid cancer (IV) | FOLFOX + bevacizumab FOLFIRI + cetuximab | Yes | PTEN pMMR MSI stable | Liver and Peritoneum | Hypertension |
| Patient # | Best Response (Time to the Best Response From Initiation in Weeks) | Progression or Discontinuation of Therapy (Time to Progression/Therapy Discontinuation) | Therapy after Rego + 5-FU | Time to the Last Follow-Up (in Months) | Status at Last Follow-Up |
|---|---|---|---|---|---|
| 1 | Stable disease (130) | Progression (130) | Pembrolizumab | 31 | Alive on other therapy |
| 2 | Partial response (53) | Progression (53) | Trifluridine/Tipiracil + bevacizumab pembrolizumab | 30 | Alive on other therapy |
| 3 | Progressive disease (7) | Progression (7) | Nivolumab + regorafenib Trifluridine/Tipiracil + bevacizumab Tolfenamic acid | 20 | Alive on other therapy |
| 4 | Progressive disease (8) | Progression (30) | Pembrolizumab + regorafenib | 9.6 | Deceased |
| 5 | Stable disease (17) | Discontinuation—Toxicity (17) | Trifluridine/Tipiracil + bevacizumab | 11 | Deceased |
| 6 | Progressive disease (13) | Progression (13) | FOLFIRI bevacizumab + oxaliplatin + capecitabine | 11.5 | Alive on other therapy |
| 7 | Stable disease (7) | Discontinuation—Toxicity (7) | None | 2 | Deceased |
| 8 | Progressive disease (13) | Progression (13) | Trifluridine/Tipiracil + bevacizumab | 4.5 | Alive on other therapy |
| 9 | Progressive disease (8) | Progression (8) | Trifluridine/Tipiracil + Bevacizumab | 8 | Alive on other therapy |
| 10 | Stable disease (6) | Progression (6.5) | Panitumumab + 5-FU | 6 | Deceased |
| 11 | Progressive disease (4) | Progression (4) | None | 1 | Deceased |
| 12 | Stable disease (7) | Discontinuation (7) | None | 5 | Alive |
| Patient # | Regorafenib Dose at Initiation | Regorafenib Dose at Last Follow-Up or Discontinuation | 5-FU Dose at Initiation (mg/m2) | 5-FU Dose at Last Follow-Up or Discontinuation (mg/m2) | Adverse Events Reported |
|---|---|---|---|---|---|
| 1 | 120 mg | 80 mg | Day 1: 400 Day 2: 2400 | Day 1: 320 Day 2: 1920 | Grade 1–2 HFS |
| 2 | 80 mg | 120 mg | Received in an outside facility | Received in an outside facility. | Well-tolerated |
| 3 | 120 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Grade 3 HTN |
| 4 | 120 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Well-tolerated |
| 5 | 120 mg | 80 mg | Day 1: 400 Day 2: 2400 | Day 1: 320 Day 2: 1920 | Grade 3 HFS |
| 6 | 120 mg | 80 mg | Day 1: 400 Day 2: 2400 | Day 1: 320 Day 2: 1920 | Grade 1–2 mucositis managed with regorafenib dose reduction to 80 mg and oral rinses, resolved in 7 days. |
| 7 | 160 mg | 160 mg | Day 1: 320 Day 2: 1920 | Day 1: 320 Day 2: 1920 | Grade 3 pneumonitis |
| 8 | 80 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Well-tolerated |
| 9 | 80 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Well-tolerated |
| 10 | 80 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Well-tolerated |
| 11 | 80 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Well-tolerated |
| 12 | 80 mg | 120 mg | Day 1: 400 Day 2: 2400 | Day 1: 400 Day 2: 2400 | Well-tolerated |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelrahim, M.; Esmail, A.; Al-Najjar, E.; Khasawneh, B.; Umoru, G.; Abdelrahim, W.; Abboud, K.; Ajewole, V.B. Safety and Efficacy of Regorafenib and 5-Fluorouracil Combination Therapy in Refractory Metastatic Colorectal Cancer After Third-Line Treatment: An Institutional Experience. Biomedicines 2025, 13, 1151. https://doi.org/10.3390/biomedicines13051151
Abdelrahim M, Esmail A, Al-Najjar E, Khasawneh B, Umoru G, Abdelrahim W, Abboud K, Ajewole VB. Safety and Efficacy of Regorafenib and 5-Fluorouracil Combination Therapy in Refractory Metastatic Colorectal Cancer After Third-Line Treatment: An Institutional Experience. Biomedicines. 2025; 13(5):1151. https://doi.org/10.3390/biomedicines13051151
Chicago/Turabian StyleAbdelrahim, Maen, Abdullah Esmail, Ebtesam Al-Najjar, Bayan Khasawneh, Godsfavour Umoru, Waseem Abdelrahim, Karen Abboud, and Veronica B. Ajewole. 2025. "Safety and Efficacy of Regorafenib and 5-Fluorouracil Combination Therapy in Refractory Metastatic Colorectal Cancer After Third-Line Treatment: An Institutional Experience" Biomedicines 13, no. 5: 1151. https://doi.org/10.3390/biomedicines13051151
APA StyleAbdelrahim, M., Esmail, A., Al-Najjar, E., Khasawneh, B., Umoru, G., Abdelrahim, W., Abboud, K., & Ajewole, V. B. (2025). Safety and Efficacy of Regorafenib and 5-Fluorouracil Combination Therapy in Refractory Metastatic Colorectal Cancer After Third-Line Treatment: An Institutional Experience. Biomedicines, 13(5), 1151. https://doi.org/10.3390/biomedicines13051151