
Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry

 , , , , , , , , and
, , , , , , , , and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Improved LVEF (HFimpEF) [3,4,12]
- (1)
- Initial LVEF ≤ 40%;
- (2)
- Follow-up LVEF > 40%;
- (3)
- An increase of ≥10 percentage points between baseline and follow-up assessments.
2.3. Guideline-Directed Medical Therapy and Etiology-Specific Interventions
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
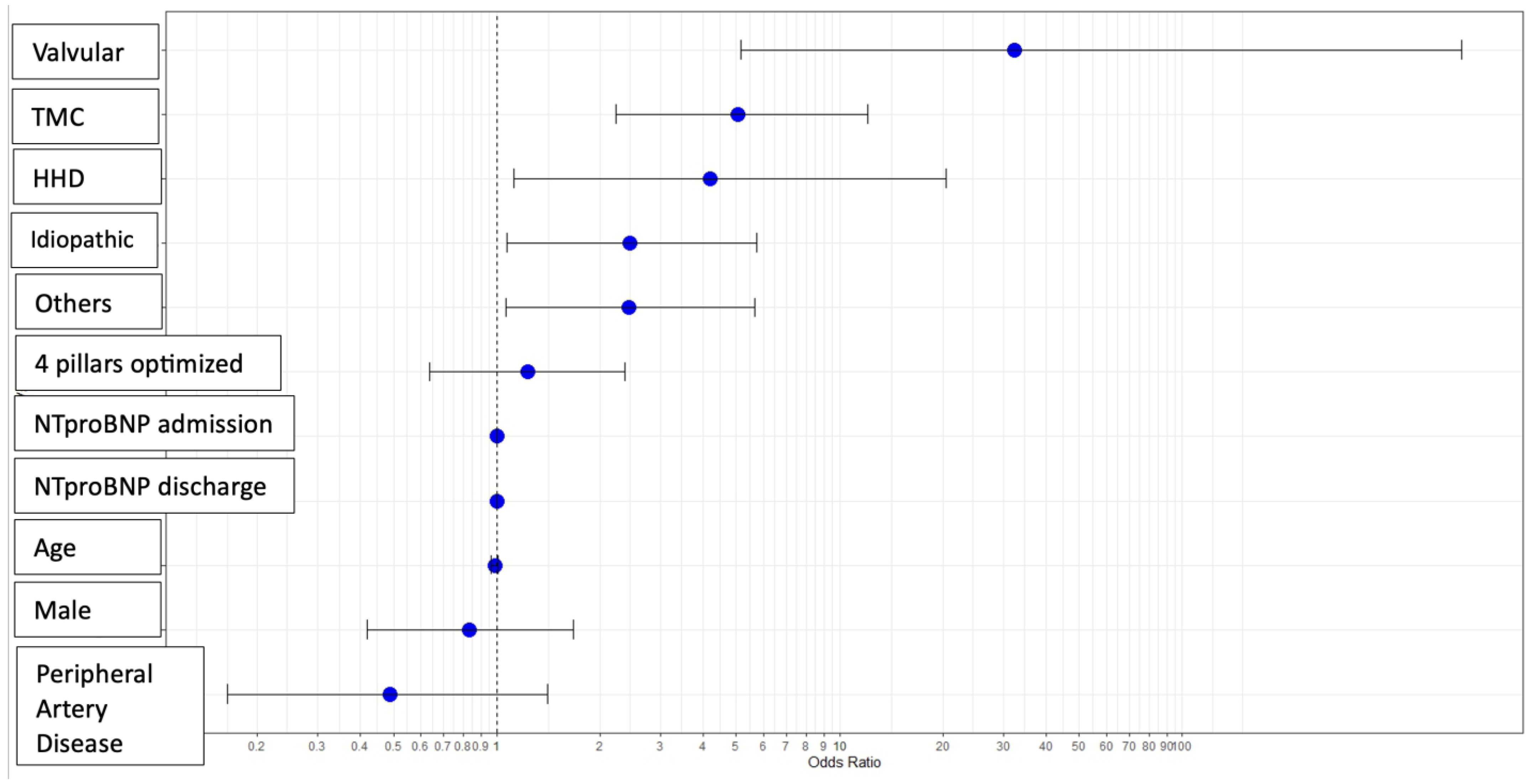
3.2. Heart Failure Etiology
- Tachycardiomyopathy: 29.3% in HFimpEF vs. 13.1% in non-HFimpEF (p = 0.006).
- Valvular: 7.6% in HFimpEF vs. 1.1% in non-HFimpEF (p = 0.05).
- Ischemic: 17.2% in HFimpEF vs. 43.9% in non-HFimpEF (p < 0.0001).
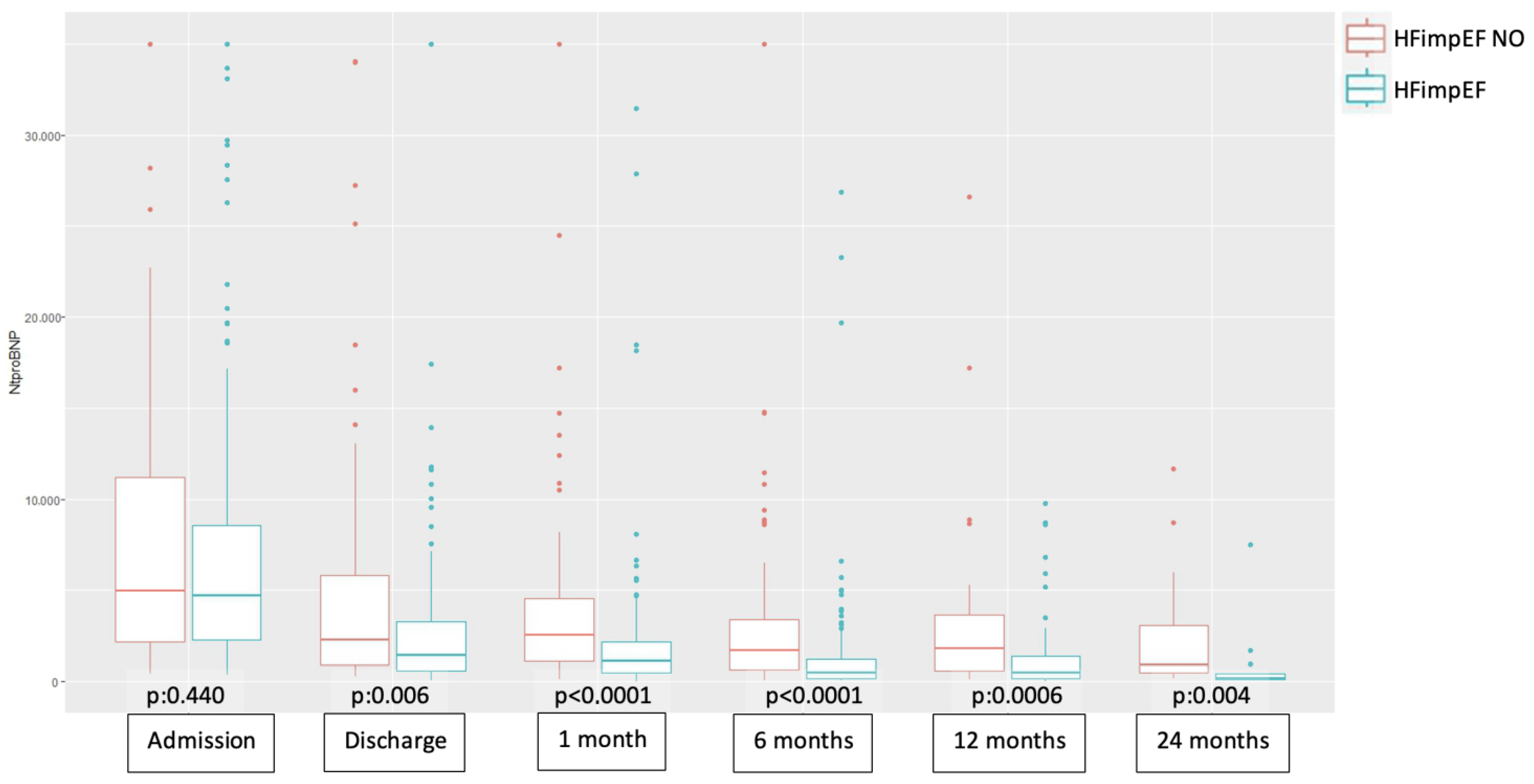
3.3. NT-proBNP Evolution During Follow-Up
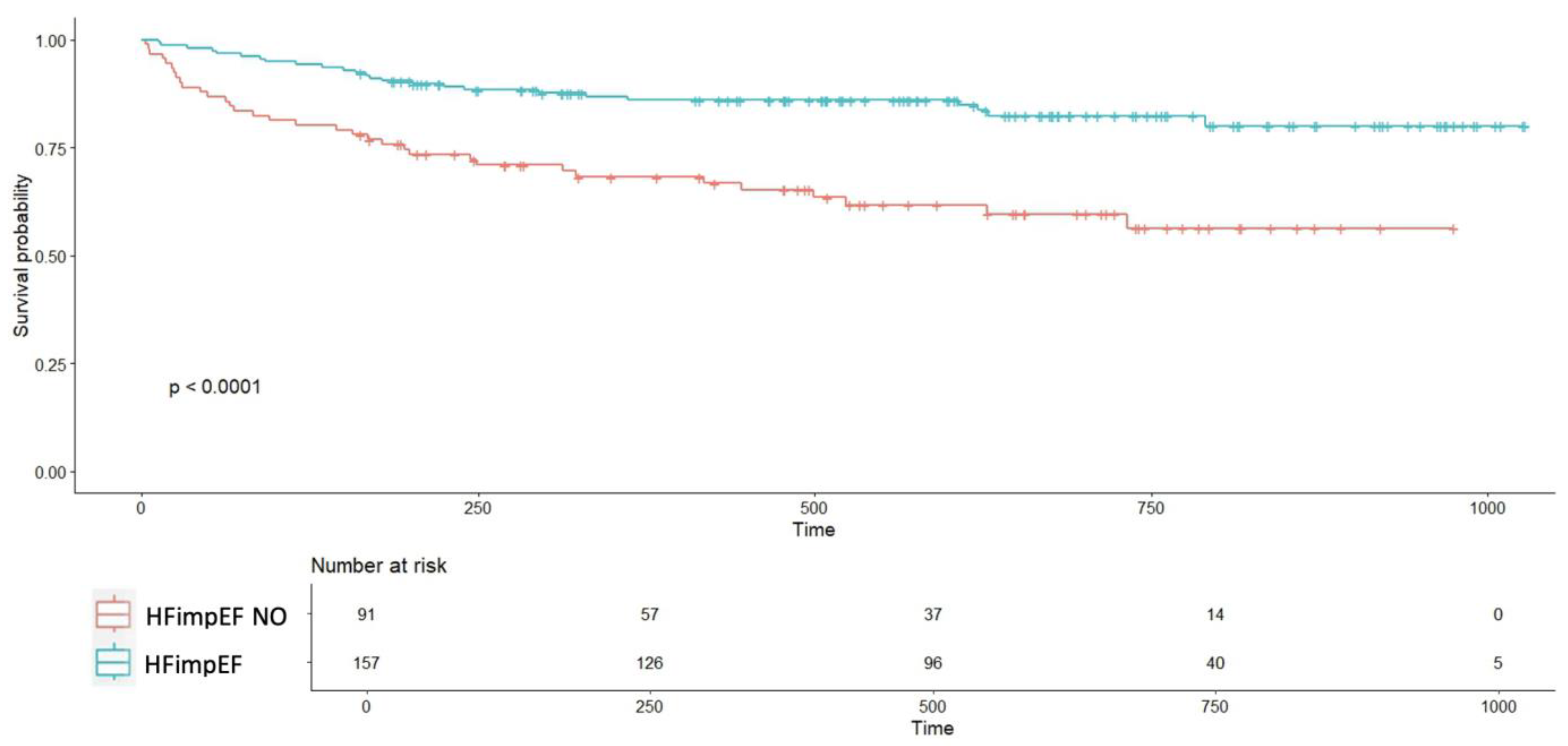
3.4. Morbidity and Mortality in HFimpEF
4. Discussion
4.1. Comparison with Previous Studies
- Basuray et al. reported a 10% recovery rate in an outpatient cohort, using a definition of LVEF > 50% that had previously been <50% [13].
- The IMPROVE-HF registry found a 29% improvement rate in outpatient settings, with an absolute LVEF increase of ≥10 points [5].
- Agra Bermejo et al. reported a 52% recovery rate at 1 year in outpatients [6].
- Abe et al. observed a 41% recovery rate among hospitalized patients, although their criteria required LVEF >50%, and these were not de novo cases [7].
4.2. Prognostic Factors
- Marcusohn et al. reported a 64% recovery rate in patients with atrial fibrillation-related tachycardiomyopathy, with ischemic heart disease and worse baseline LVEF as negative predictors [14].
- Abe et al. found valvular disease and atrial fibrillation to be associated with recovery in hospitalized HF patients with reduced LVEF [7].
4.3. Role of NT-proBNP
4.4. Morbidity and Mortality
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CAD | Coronary Artery Disease |
| CMR | Cardiac Magnetic Resonance |
| COPD | Chronic Obstructive Pulmonary Disease |
| DCM | Dilated Cardiomyopathy |
| EF | Ejection Fraction |
| ESC | European Society of Cardiology |
| HF | Heart Failure |
| HFimpEF | Heart Failure with Improved Ejection Fraction |
| HFmrEF | Heart Failure with Mildly Reduced Ejection Fraction |
| HFpEF | Heart Failure with Preserved Ejection Fraction |
| HFrEF | Heart Failure with Reduced Ejection Fraction |
| HHD | Hypertensive Heart Disease |
| LGE | Late Gadolinium Enhancement |
| LVEF | Left Ventricular Ejection Fraction |
| NT-proBNP | N-terminal Prohormone of Brain Natriuretic Peptide |
| OSA | Obstructive Sleep Apnea |
| RAAS | Renin–Angiotensin–Aldosterone System |
| SGLT2 | Sodium-Glucose Cotransporter-2 |
| TAVI | Transcatheter Aortic Valve Implantation |
| TCM | Tachycardiomyopathy |
| eGFR | Estimated Glomerular Filtration Rate |
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [PubMed]
- Tsao, C.W.; Lyass, A.; Enserro, D.; Larson, M.G.; Ho, J.E.; Kizer, J.R.; Gottdiener, J.S.; Psaty, B.M.; Vasan, R.S. Temporal Trends in the Incidence of and Mortality Associated with Heart Failure with Preserved and Reduced Ejection Fraction. JACC Heart Fail. 2018, 6, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, J.E.; Fang, J.C.; Margulies, K.B.; Mann, D.L. Heart failure with recovered left ventricular ejection fraction: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2020, 76, 719–734. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Wilcox, J.E.; Fonarow, G.C.; Yancy, C.W.; Albert, N.M.; Curtis, A.B.; Heywood, J.T.; Inge, P.J.; McBride, M.L.; Mehra, M.R.; O’Connor, C.M.; et al. Factors associated with improvement in ejection fraction in clinical practice among patients with heart failure: Findings from IMPROVE HF. Am. Heart J. 2012, 163, 49–56.e2. [Google Scholar] [CrossRef]
- Bermejo, R.A.; Babarro, E.G.; Canoa, J.N.L.; Román, A.V.; Otero, I.G.; Ayude, M.O.; Vazquez, P.P.; Rodríguez, I.G.; Castro, O.D.; Juanatey, J.R.G. Heart failure with recovered ejection fraction: Clinical characteristics, determinants and prognosis. CARDIOCHUS-CHOP registry. Cardiol. J. 2018, 25, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Yoshihisa, A.; Ichijo, Y.; Sato, Y.; Kanno, Y.; Takiguchi, M.; Yokokawa, T.; Misaka, T.; Sato, T.; Oikawa, M.; et al. Recovered Left Ventricular Ejection Fraction and Its Prognostic Impacts in Hospitalized Heart Failure Patients with Reduced Ejection Fraction. Int. Heart J. 2020, 61, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Wybraniec, M.T.; Orszulak, M.; Męcka, K.; Mizia-Stec, K. Heart Failure with Improved Ejection Fraction: Insight into the Variable Nature of Left Ventricular Systolic Function. Int. J. Environ. Res. Public Health 2022, 19, 14400. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- He, Y.; Ling, Y.; Guo, W.; Li, Q.; Yu, S.; Huang, H.; Zhang, R.; Gong, Z.; Liu, J.; Mo, L.; et al. Prevalence and Prognosis of HFimpEF Developed From Patients With Heart Failure With Reduced Ejection Fraction: Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 757596. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Esteban-Fernández, A.; Gómez-Otero, I.; López-Fernández, S.; Santamarta, M.R.; Pastor-Pérez, F.J.; Fluvià-Brugués, P.; Pérez-Rivera, J.Á.; López López, A.; García-Pinilla, J.M.; Palomas, J.L.B.; et al. Influence of the medical treatment schedule in new diagnoses patients with heart failure and reduced ejection fraction. Clin. Res. Cardiol. 2023. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Hellawell, J.L.; Margulies, K.B. Myocardial reverse remodeling. Cardiovasc. Ther. 2012, 20, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail. 2021, 23, 352–380. [Google Scholar] [CrossRef] [PubMed]
- Basuray, A.; French, B.; Ky, B.; Vorovich, E.; Olt, C.; Sweitzer, N.; Cappola, T.; Fang, J.C. Heart failure with recovered ejection fraction: Clinical description, biomarkers, and outcomes. Circulation 2014, 129, 2380–2387. [Google Scholar] [CrossRef] [PubMed]
- Marcusohn, E.; Postnikov, M.; Kobo, O.; Hellman, Y.; Mutlak, D.; Epstein, D.; Agmon, Y.; Gepstein, L.; Zukermann, R. Factors Associated with Left Ventricular Function Recovery in Patients with Atrial Fibrillation Related Cardiomyopathy. Isr. Med. Assoc. J. 2022, 24, 101–106. [Google Scholar] [PubMed]
- Givertz, M.M.; Mann, D.L. Epidemiology and nat- ural history of recovery of left ventricular function in recent onset dilated cardiomyopathies. Curr. Heart Fail. Rep. 2013, 10, 321–330. [Google Scholar] [CrossRef]
- Punnoose, L.R.; Givertz, M.M.; Lewis, E.F.; Pratibhu, P.; Stevenson, L.W.; Desai, A.S. Heart failure with recovered ejection fraction: A distinct clinical entity. J. Card. Fail. 2011, 17, 527–532. [Google Scholar] [CrossRef]
- Ghimire, A.; Fine, N.; Ezekowitz, J.A.; Howlett, J.; Youngson, E.; McAlister, F.A. Frequency, predictors, and prognosis of ejection fraction improvement in heart failure: An echocardiogram-based registry study. Eur. Heart J. 2019, 40, 2110–2117. [Google Scholar] [CrossRef]
- Kewcharoen, J.; Trongtorsak, A.; Thangjui, S.; Kanitsoraphan, C.; Prasitlumkum, N. Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction. Med. Sci. 2022, 10, 21. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Paolisso, P.; Gallinoro, E.; Belmonte, M.; Bertolone, D.T.; Bermpeis, K.; De Colle, C.; Shumkova, M.; Leone, A.; Caglioni, S.; Esposito, G.; et al. Coronary Microvascular Dysfunction in Patients With Heart Failure: Characterization of Patterns in HFrEF Versus HFpEF. Circ Heart Fail. 2024, 17, e010805. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, P.; Belmonte, M.; Gallinoro, E.; Scarsini, R.; Bergamaschi, L.; Portolan, L.; Armillotta, M.; Esposito, G.; Moscarella, E.; Benfari, G.; et al. SGLT2-inhibitors in diabetic patients with severe aortic stenosis and cardiac damage undergoing transcatheter aortic valve implantation (TAVI). Cardiovasc. Diabetol. 2024, 23, 420. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Daubert, M.A.; Adams, K.; Yow, E.; Barnhart, H.X.; Douglas, P.S.; Rimmer, S.; Norris, C.; Cooper, L.; Leifer, E.; Desvigne-Nickens, P.; et al. NT-proBNP goal achievement is associated with sig- nificant reverse remodeling and improved clinical outcomes in HFrEF. J. Am. Coll. Cardiol. Heart Fail. 2019, 7, 158–168. [Google Scholar]
- Lupón, J.; Díez-López, C.; de Antonio, M.; Domingo, M.; Zamora, E.; Moliner, P.; González, B.; Santesmases, J.; Troya, M.I.; Bayés-Genís, A. Recovered heart failure with reduced ejection fraction and outcomes: A prospective study. Eur. J. Heart Fail. 2017, 19, 1615–1623. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | HFimpEF (n = 157) | Non-HFimpEF (n = 91) | p-Value |
|---|---|---|---|
| Age (years) | 69 (58–76) | 71 (61–78) | 0.353 |
| Male (n, %) | 120 (76.43%) | 68 (74.73%) | 0.882 |
| BMI (n, %) | 26.66 (23.72–30.16) | 27.15 (23.55–31.13) | 0.527 |
| Hypertension (n, %) | 92 (58.60%) | 63 (69.23%) | 0.126 |
| Dyslipidemia (n, %) | 73 (46.50%) | 48 (52.74%) | 0.414 |
| Diabetes mellitus (n, %) | 43 (27.39%) | 34 (37.36%) | 0.135 |
| Chronic kidney disease (n, %) | 28 (17.83%) | 29 (31.87%) | 0.018 |
| Stroke (n, %) | 8 (5.12%) | 8 (8.79%) | 0.390 |
| COPD (n, %) | 11 (7.00%) | 10 (10.99%) | 0.396 |
| OSA (n, %) | 7 (4.49%) | 7 (7.69%) | 0.444 |
| Peripheral artery disease (n, %) | 9 (5.73%) | 12 (13.33%) | 0.068 |
| Alcohol use (n, %) | 44 (28.03%) | 21 (23.08%) | 0.481 |
| Smoking (n, %) | 64 (40.76%) | 26 (28.57%) | 0.074 |
| Length of hospital stay (days) | 7 (5–11) | 7 (5–10.5) | 0.805 |
| Time to therapy optimization (days) | 117 (38.25–186.25) | 110 (44.50–172.00) | 0.837 |
| Heart failure etiology (n, %) | <0.0001 | ||
| - Hypertensive | 10 (6.37%) | 3 (3.30%) | 0.453 |
| - Tachycardiomyopathy | 46 (29.30%) | 12 (13.19%) | 0.006 |
| - Ischemic | 27 (17.20%) | 40 (43.96%) | <0.0001 |
| - Idiopathic | 32 (20.38%) | 20 (21.98%) | 0.892 |
| - Valvular | 12 (7.64%) | 1 (1.10%) | 0.050 |
| - Other | 26 (19.11%) | 15 (16.48%) | 0.729 |
| 4 Pillars at discharge (n, %) | 103 (66.03%) | 53 (58.24%) | 0.277 |
| 4 Pillars after optimization (n, %) | 110 (72.37%) | 57 (64.04%) | 0.227 |
| RAAS inhibitors at discharge (n, %) | 142 (90.45%) | 76 (83.52%) | 0.158 |
| Beta blockers at discharge (n, %) | 142 (91.03%) | 88 (96.70%) | 0.150 |
| Mineralocorticoid receptor antagonists at discharge (n, %) | 130 (82.80%) | 69 (75.82%) | 0.244 |
| SGLT2 inhibitors at discharge (n, %) | 131 (83.39%) | 76 (83.52%) | 0.126 |
| RAAS inhibitors after optimization (n, %) | 139 (90.26%) | 74 (81.32%) | 0.070 |
| Beta blockers after optimization (n, %) | 147 (93.63%) | 88 (97.78%) | 0.250 |
| Mineralocorticoid receptor antagonists after optimization (n, %) | 128 (82.58%) | 74 (81.32%) | 0.939 |
| SGLT2 inhibitors after optimization (n, %) | 144 (91.72%) | 80 (88.89%) | 0.611 |
| Creatinine at discharge (mg/dL) | 1.10 (0.89–1.37) | 1.14 (0.87–1.51) | 0.361 |
| eGFR at discharge (mL/min/1.73 m2) | 65.93 (21.63) | 62.00 (24.44) | 0.217 |
| Potassium at discharge (mEq/L) | 4.2 (3.9–4.50) | 4.3 (3.9–4.85) | 0.296 |
| Hemoglobin at discharge (g/dL) | 14.35 (2.24) | 13.99(2.50) | 0.260 |
| eGFR after optimization (mL/min/1.73 m2) | 70.03 (23.33) | 63.12 (25.90) | 0.041 |
| Potassium after optimization (mEq/L) | 4.62 (0.45) | 4.55 (0.52) | 0.266 |
| LVEF at admission (% mean) | 28.90 (6.44) | 28.78 (7.38) | 0.90 |
| LVEF after optimization (% mean) | 51.58 (7.249) | 32.916 (6.60) | <2.2 × 10−16 |
| ECG rhythm on admission | 0.285 | ||
| - Sinus rhythm (n, %) | 104 (60.8%) | 67 (39.2%) | |
| - Atrial fibrillation/Flutter (n, %) | 53 (68.8%) | 24 (31.2%) | |
| Bundle branch block on admission | 0.004 | ||
| - No bundle branch block (n, %) | 121 (69.9%) | 52 (30.1%) | |
| - Left bundle branch block (n, %) | 24 (45.3%) | 29 (54.7%) | |
| - Right bundle branch block (n, %) | 10 (55.6%) | 8 (44.4%) | |
| Coronary anatomy (n,%) * | 0.268 | ||
| - Normal coronaries | 47 (62.67%) | 28 (43.8%) | |
| - Non-obstructive CAD | 18 (24%) | 19 (29.7%) | |
| - Obstructive CAD | 10 (13.33%) | 17 (26.6%) | |
| Revascularization during hospitalization (n, %) | 10 (6.37%) | 17(18.68%) | 0.005 |
| Complete revascularization (n/%) | 4 (2.55%) | 14 (15.38%) | 0.001 |
| Group | Comparison | p-Value |
|---|---|---|
| HFimpEF | Admission > Discharge | <2.2 × 10⁻16 |
| Non-HFimpEF | Admission > Discharge | 1.188 × 10⁻11 |
| HFimpEF | Discharge > 1 Month | 0.001 |
| Non-HFimpEF | Discharge > 1 Month | 0.774 |
| HFimpEF | 1 Month > 6 Months | 3.462 × 10⁻⁸ |
| Non-HFimpEF | 1 Month > 6 Months | 7.932 × 10⁻⁶ |
| HFimpEF | 6 Months > 12 Months | 0.019 |
| Non-HFimpEF | 6 Months > 12 Months | 0.133 |
| HFimpEF | 12 Months > 24 Months | 0.032 |
| Non-HFimpEF | 12 Months > 24 Months | 0.058 |
| Variable | HFimpEF (n = 157) | Non-HFimpEF (n = 91) | p |
|---|---|---|---|
| HF-related hospitalizations (n, %) | 11 (7.01%) | 26 (28.57 %) | 1.037x10−5 |
| Emergency department visits for HF (n, %) | 6(3.82%) | 6 (6.59%) | 0.507 |
| All-cause mortality (n, %) | 12 (7.64%) | 9 (9.89%) | 0.707 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donoso-Trenado, V.; Otero-García, Ó.; López-Vilella, R.; de la Fuente López, P.; Martínez-Solé, J.; Yebra-Pimentel Brea, C.; Guerrero-Cervera, B.; Adarraga Gómez, J.; Huélamo-Montoro, S.; Gallego-Latorre, G.; et al. Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry. Biomedicines 2025, 13, 1143. https://doi.org/10.3390/biomedicines13051143
Donoso-Trenado V, Otero-García Ó, López-Vilella R, de la Fuente López P, Martínez-Solé J, Yebra-Pimentel Brea C, Guerrero-Cervera B, Adarraga Gómez J, Huélamo-Montoro S, Gallego-Latorre G, et al. Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry. Biomedicines. 2025; 13(5):1143. https://doi.org/10.3390/biomedicines13051143
Chicago/Turabian StyleDonoso-Trenado, Víctor, Óscar Otero-García, Raquel López-Vilella, Pablo de la Fuente López, Julia Martínez-Solé, Carlos Yebra-Pimentel Brea, Borja Guerrero-Cervera, Javier Adarraga Gómez, Sara Huélamo-Montoro, Guillermo Gallego-Latorre, and et al. 2025. "Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry" Biomedicines 13, no. 5: 1143. https://doi.org/10.3390/biomedicines13051143
APA StyleDonoso-Trenado, V., Otero-García, Ó., López-Vilella, R., de la Fuente López, P., Martínez-Solé, J., Yebra-Pimentel Brea, C., Guerrero-Cervera, B., Adarraga Gómez, J., Huélamo-Montoro, S., Gallego-Latorre, G., García-Vega, D., Gómez-Otero, I., Martínez-Dolz, L., González-Juanatey, J. R., & Almenar Bonet, L. (2025). Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry. Biomedicines, 13(5), 1143. https://doi.org/10.3390/biomedicines13051143