
Prediction of Metabolic Parameters of Diabetic Patients Depending on Body Weight Variation Using Machine Learning Techniques


 ,
,
Abstract
1. Introduction
2. Materials and Methods
- (a)
- Dysglycemia parameters: HbA1c, fasting blood glucose, and HOMA-IR (Homeostatic Model Assessment for Insulin Resistance).
- (b)
- Dyslipidemia parameters: total cholesterol, HDL cholesterol, and triglycerides.
- (c)
- Inflammation parameters: C-reactive protein (CRP), IL-6 (Interleukin-6), TNF-α (Tumor Necrosis Factor α), leptin, and adiponectin.
- (d)
- Liver function parameters: AST (Aspartate Aminotransferase) and ALT (Alanine Aminotransferase).
- (e)
- Kidney function parameters: uric acid and creatinine.
- (a)
- Initial scatter plot: a preliminary visualization of the relationship between the two variables, providing an overview of the data distribution.
- (b)
- Outlier detection based on residuals: Identifies observations where the residuals (differences between observed and predicted values) exceed ±3 standard deviations (3σ), indicating potential outliers. An outlier is also defined as any data point where the signs of the variation in an analyzed parameter and the variation in body weight are discordant. All parameters align with this rule, except for HDL cholesterol, where, from a medical standpoint, the two variations are expected to have opposite signs.
- (c)
- Influence analysis via Cook’s distance: evaluates the influence of each observation on the fitted regression model, highlighting data points that disproportionately affect the model’s accuracy.
- (d)
- Automatic removal of problematic points: automatically filters out data points identified as outliers based on large residuals, a high Cook’s distance, or discordant signs between variables.
- (e)
- Final scatter plot (cleaned data): displays the dataset after removing the problematic observations, showcasing the cleaned data distribution.
- (f)
- Returning two data frames: the dataset with outliers removed, now prepared for regression analysis, and the problematic dataset, which consists of a separate collection of the detected outliers, which can be analyzed further if needed.
3. Results
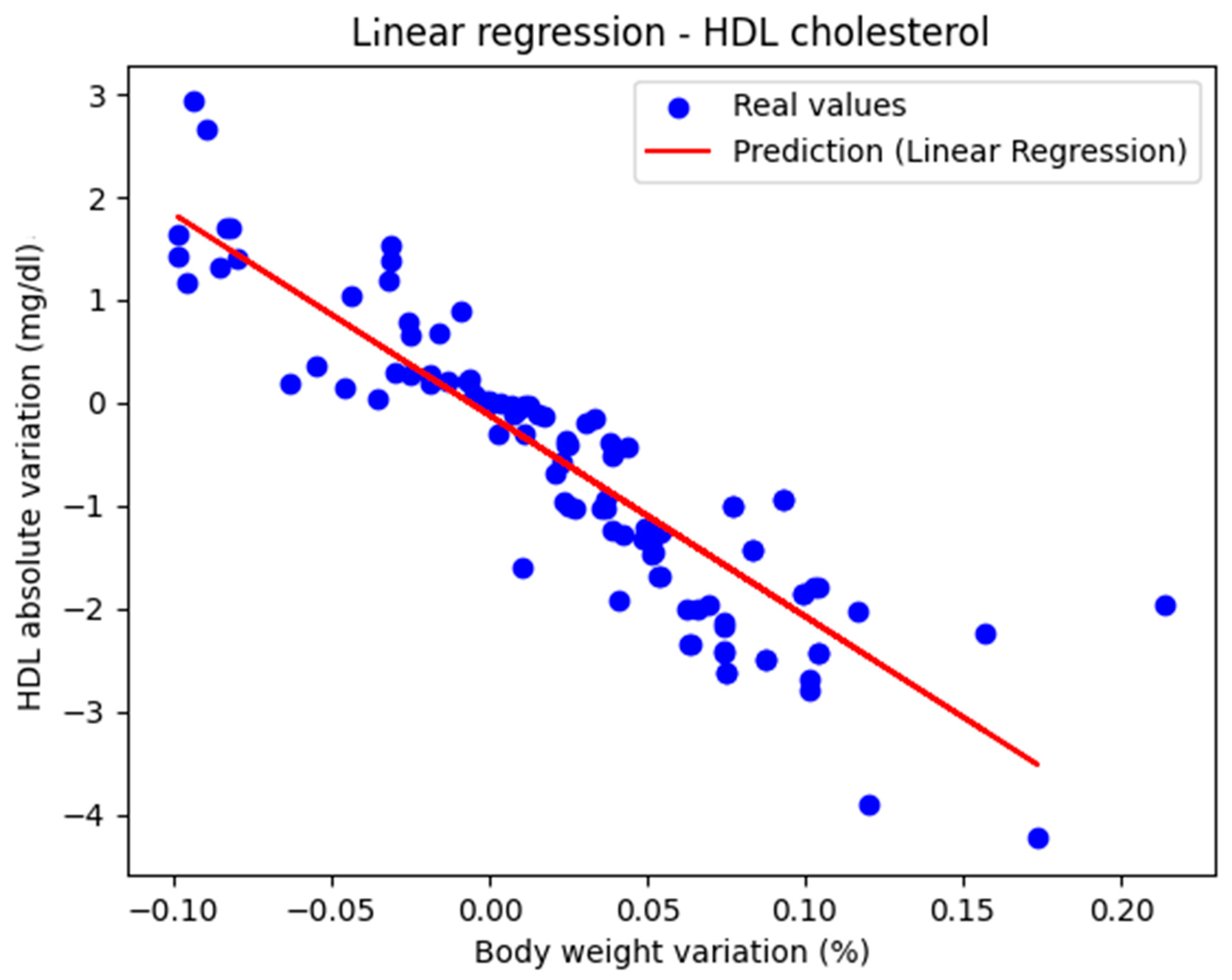
3.1. Liniar and Polynomial Regression
3.2. Gradient Boosting
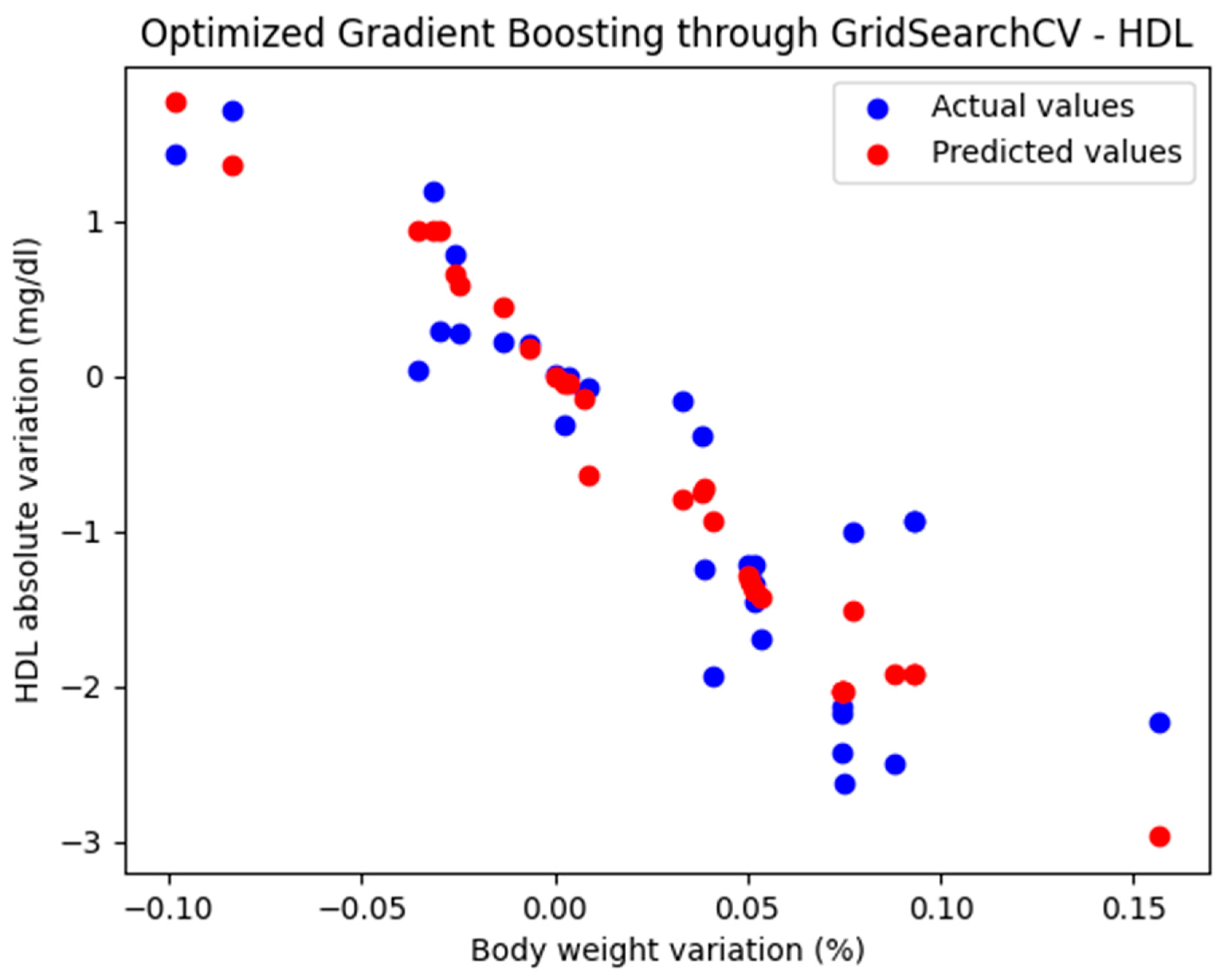
3.2.1. Optimized Gradient Boosting Model Through GridSearchCV
3.2.2. Optimized Gradient Boosting Model Through RandomizedSearchCV
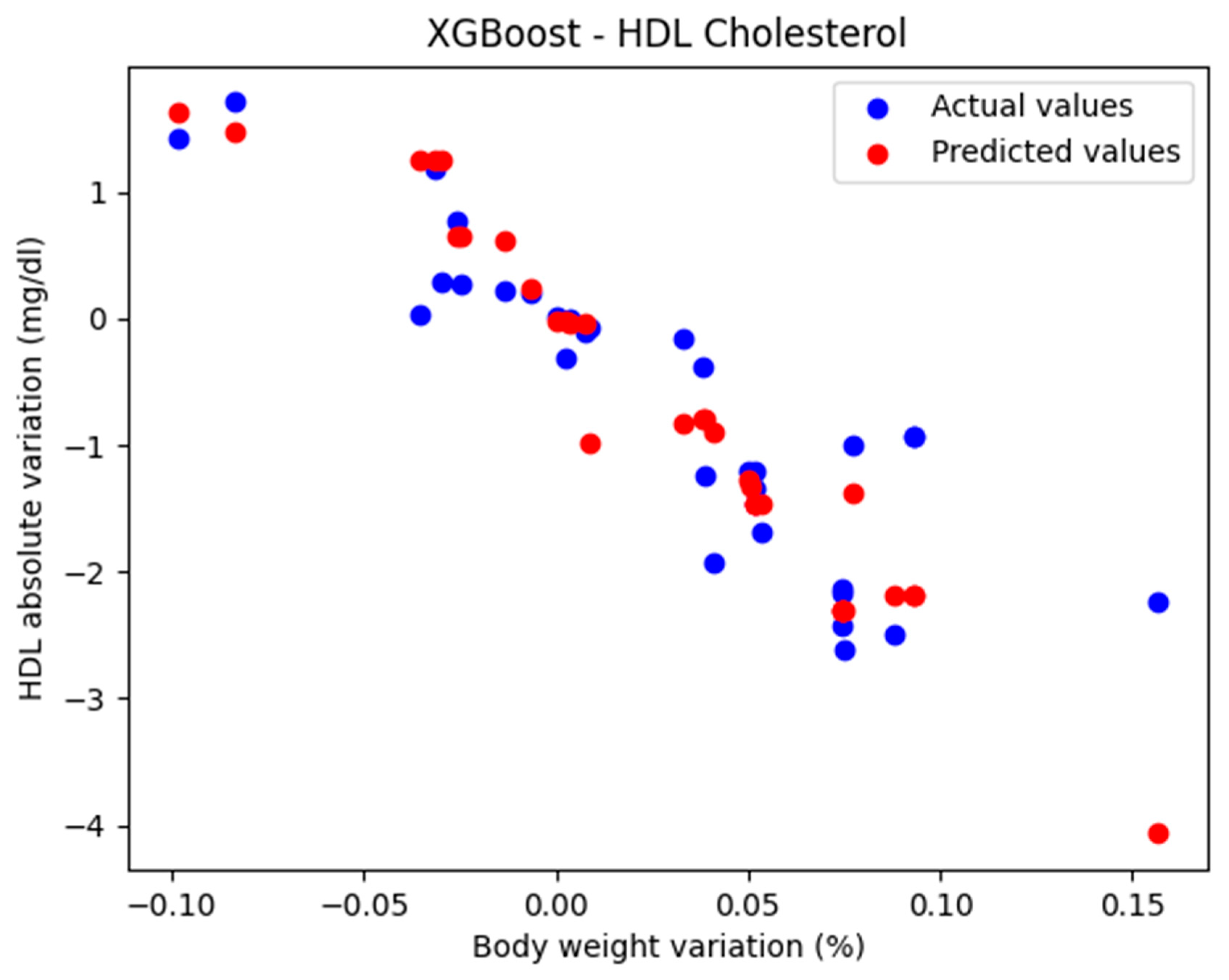
3.3. XGBoost
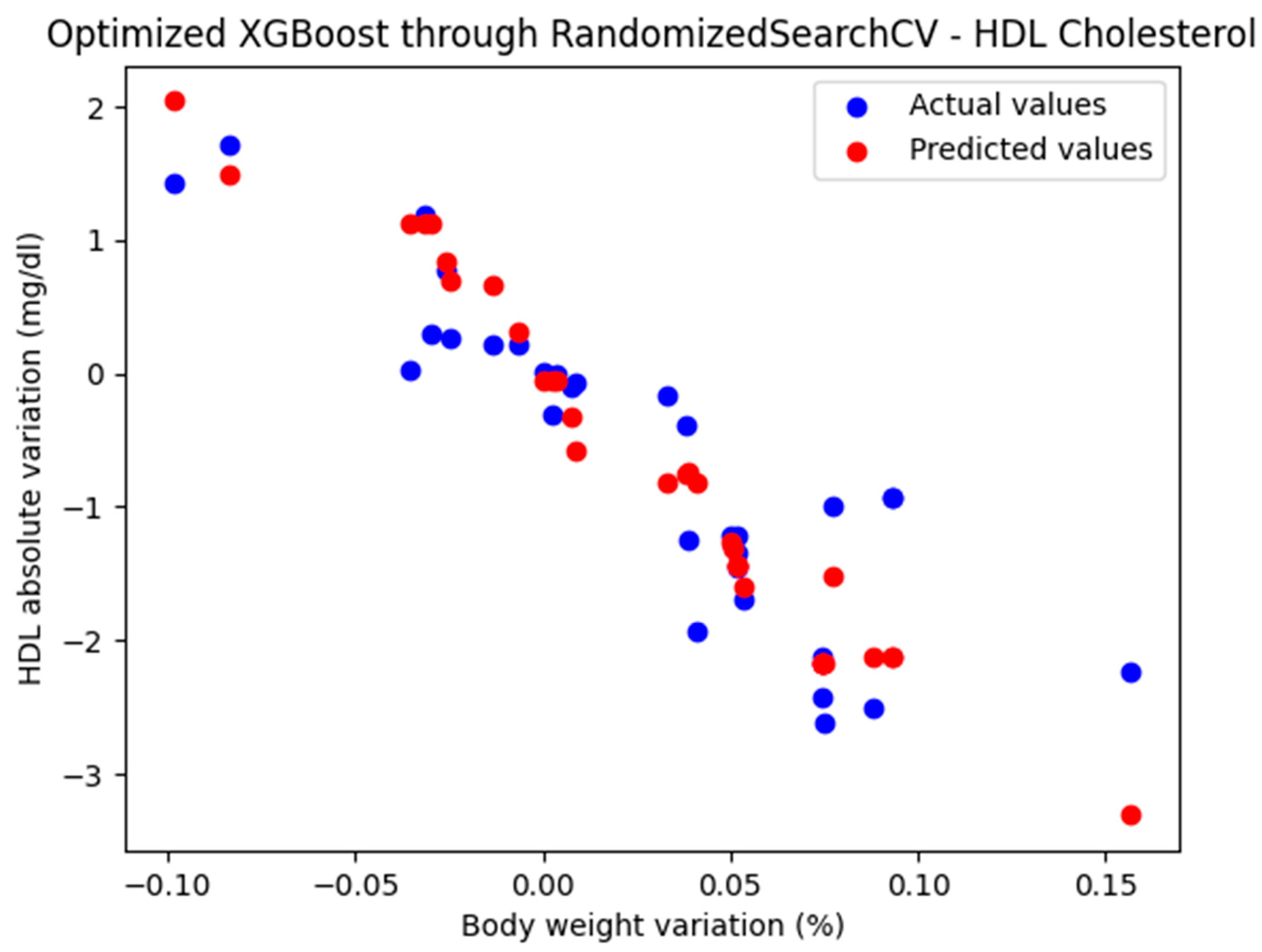
3.3.1. Optimized XGBoost Model Through RandomizedSearchCV
3.3.2. Optimized XGBoost Model Through GridSearchCV
4. Discussion
- (a)
- Blood glucose levels:
- Fasting blood glucose: Weight loss can lower fasting blood glucose levels, reducing the risk of type 2 diabetes (if prediabetic) or complications of diabetes. For every 5–10% reduction in body weight, fasting blood glucose levels decrease by 5–20 mg/dL.
- HbA1c: Tends to improve with weight loss. A 5–10% weight loss can reduce HbA1c by 0.5–2.0%.
- (b)
- Lipid profile:
- Total cholesterol: Weight loss generally reduces overall cholesterol levels. A 5–10% weight loss can lower total cholesterol levels by 5–12 mg/dL.
- LDL cholesterol (‘bad cholesterol’): Decreases with weight loss, improving cardiovascular health. A 5–10% weight loss can lower LDL levels by 5–10 mg/dL.
- HDL cholesterol (‘good cholesterol’): Typically increases with weight loss. HDL cholesterol levels increase by about 1–3 mg/dL for every 5–10% weight loss.
- Triglycerides: triglyceride levels decrease significantly—by about 20 mg/dL or more—for every 5% reduction in body weight.
- (c)
- Inflammatory markers:
- C-reactive protein (CRP): Lower CRP levels reflect reduced systemic inflammation after weight loss. A 10% weight loss can result in a 25–30% reduction in CRP levels.
- Interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α): weight loss of 10% or more can reduce these inflammatory markers by 10–20%, depending on baseline levels.
- (d)
- Liver enzymes (can also be considered inflammatory markers):
- ALT (Alanine Aminotransferase) and AST (Aspartate Aminotransferase): Weight loss improves these markers, indicating better liver health. A 5–10% weight loss can decrease ALT and AST levels by 20–30%.
- (e)
- Hormones:
- Leptin: Decreases with weight loss, reflecting a reduction in fat mass. Leptin levels decrease in proportion to the reduction in fat mass, often by 20–30% for a 10% weight loss.
- Adiponectin: increases by 20–30% with a 10% weight loss, improving metabolic health.
- Thyroid hormones (e.g., TSH): thyroid hormone levels may normalize with a 5–10% weight loss in individuals with obesity-induced thyroid dysfunction.
- (f)
- Blood pressure and related markers: although they are not direct blood markers, systolic and diastolic blood pressure decrease by approximately 1 mmHg for each kilogram of weight loss (this finding was made by studying the variation in blood pressure depending on the absolute variation in weight.
- (g)
- Markers of renal function: Creatinine and glomerular filtration rate. Improved weight management may improve renal function. It is more difficult to draw a conclusion in quantitative terms.
- (h)
- Uric acid: a 10% weight loss can lower uric acid levels by approximately 0.5–1.3 mg/dL.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MSE | Mean Squared Error |
| MAE | Mean Absolute Error |
| HbA1c | Glycosylated hemoglobin |
| HDL | High-Density Lipoprotein |
References
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.I.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Primers 2015, 1, 15019. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.E. Why does type 2 diabetes mellitus impair weight reduction in patients with obesity? A review. Obes. Pillars. 2023, 7, 100076. [Google Scholar] [CrossRef] [PubMed]
- Stanford, J.; Kaiser, M.; Ablah, E.; Dong, F.; Paull-Forney, B.; Early, J. The effect of weight loss on fasting blood sugars and hemoglobin A1c in overweight and obese diabetics and non-diabetics. J. Diabetes Mellit. 2012, 2, 126–130. [Google Scholar] [CrossRef]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, P.; Weiskirchen, R. The Role of Obesity in Type 2 Diabetes Mellitus-An Overview. Int. J. Mol. Sci. 2024, 25, 1882. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J. Weight Management: Obesity to Diabetes. Diabetes Spectr. 2017, 30, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jimenez, F.; Almahmeed, W.; Bays, H.; Cuevas, A.; Di Angelantonio, E.; le Roux, C.W.; Sattar, N.; Sun, M.C.; Wittert, G.; Pinto, F.J.; et al. Obesity and cardiovascular disease: Mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. Eur. J. Prev. Cardiol. 2022, 29, 2218–2237. [Google Scholar] [CrossRef] [PubMed]
- Safaei, M.; Sundararajan, E.A.; Driss, M.; Boulila, W.; Shapi’I, A. A systematic literature review on obesity: Understanding the causes & consequences of obesity and reviewing various machine learning approaches used to predict obesity. Comput. Biol. Med. 2021, 136, 104754. [Google Scholar]
- Kirk, D.; Kok, E.; Tufano, M.; Tekinerdogan, B.; Feskens, E.J.M.; Camps, G. Machine Learning in Nutrition Research. Adv. Nutr. 2022, 13, 2573–2589. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 8. Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47 (Suppl. S1), S145–S157. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Churuangsuk, C.; Hall, J.; Reynolds, A.; Griffin, S.J.; Combet, E.; Lean, M.E.J. Diets for weight management in adults with type 2 diabetes: An umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission. Diabetologia 2022, 65, 14–36. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dicker, D.; Alfadda, A.A.; Coutinho, W.; Cuevas, A.; Halford, J.C.; Hughes, C.A.; Iwabu, M.; Kang, J.-H.; Nawar, R.; Reynoso, R.; et al. Patient motivation to lose weight: Importance of healthcare professional support, goals and self-efficacy. Eur. J. Intern. Med. 2021, 91, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Gæde, P.; Lund-Andersen, H.; Parving, H.-H.; Pedersen, O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N. Engl. J. Med. 2008, 358, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P. The importance of weight management in type 2 diabetes mellitus. Int. J. Clin. Pract. 2014, 68, 682–691. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Espinosa-Salas, S.; Gonzalez-Arias, M. Behavior Modification for Lifestyle Improvement. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK592418/ (accessed on 30 April 2025).
- Ghelani, D.P.; Moran, L.J.; Johnson, C.; Mousa, A.; Naderpoor, N. Mobile apps for weight management: A review of the latest evidence to inform practice. Front. Endocrinol. 2020, 11, 412. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.J.; Zhang, J.; Fang, M.L.; Fukuoka, Y. A systematic review of artificial intelligence chatbots for promoting physical activity, healthy diet, and weight loss. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 160. [Google Scholar] [CrossRef] [PubMed]
- Ufholz, K.; Bhargava, D. A Review of Telemedicine Interventions for Weight Loss. Curr. Cardiovasc. Risk Rep. 2021, 15, 17. [Google Scholar] [CrossRef] [PubMed]
- Rychescki, G.G.; Dos Santos, G.R.; Bertin, C.F.; Pacheco, C.N.; Antunes, L.d.C.; Stanford, F.C.; Boaventura, B. Online Cognitive-Behavioral Therapy-Based Nutritional Intervention via Instagram for Overweight and Obesity. Nutrients 2024, 16, 4045. [Google Scholar] [CrossRef] [PubMed]
- Kurtzman, G.W.; Day, S.C.; Small, D.S.; Lynch, M.; Zhu, J.; Wang, W.; Rareshide, C.A.L.; Patel, M.S. Social Incentives and Gamification to Promote Weight Loss: The LOSE IT Randomized, Controlled Trial. J. Gen. Intern. Med. 2018, 33, 1669–1675. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grams, J.; Garvey, W.T. Weight Loss and the Prevention and Treatment of Type 2 Diabetes Using Lifestyle Therapy, Pharmacotherapy, and Bariatric Surgery: Mechanisms of Action. Curr. Obes. Rep. 2015, 4, 287–302. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metric/Method | Linear Regression | 2nd-Degree Polynomial Regression |
|---|---|---|
| MAE | 0.447 | 0.441 |
| MSE | 0.434 | 0.263 |
| R2 Score | 0.770 | 0.801 |
| Metric/Method | GBR | GBR_GS | GBR_RS |
|---|---|---|---|
| MAE | 0.437 | 0.374 | 0.379 |
| MSE | 0.424 | 0.233 | 0.235 |
| R2 Score | 0.694 | 0.825 | 0.823 |
| Metric/Method | XGB | XGB_GS | XGB_RS |
|---|---|---|---|
| MAE | 0.424 | 0.402 | 0.385 |
| MSE | 0.385 | 0.302 | 0.236 |
| R2 Score | 0.710 | 0.772 | 0.823 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vîrgolici, O.; Lixandru, D.; Mihai, A.; Ștefan, D.S.; Guja, C.; Vîrgolici, H.; Virgolici, B. Prediction of Metabolic Parameters of Diabetic Patients Depending on Body Weight Variation Using Machine Learning Techniques. Biomedicines 2025, 13, 1116. https://doi.org/10.3390/biomedicines13051116
Vîrgolici O, Lixandru D, Mihai A, Ștefan DS, Guja C, Vîrgolici H, Virgolici B. Prediction of Metabolic Parameters of Diabetic Patients Depending on Body Weight Variation Using Machine Learning Techniques. Biomedicines. 2025; 13(5):1116. https://doi.org/10.3390/biomedicines13051116
Chicago/Turabian StyleVîrgolici, Oana, Daniela Lixandru, Andrada Mihai, Diana Simona Ștefan, Cristian Guja, Horia Vîrgolici, and Bogdana Virgolici. 2025. "Prediction of Metabolic Parameters of Diabetic Patients Depending on Body Weight Variation Using Machine Learning Techniques" Biomedicines 13, no. 5: 1116. https://doi.org/10.3390/biomedicines13051116
APA StyleVîrgolici, O., Lixandru, D., Mihai, A., Ștefan, D. S., Guja, C., Vîrgolici, H., & Virgolici, B. (2025). Prediction of Metabolic Parameters of Diabetic Patients Depending on Body Weight Variation Using Machine Learning Techniques. Biomedicines, 13(5), 1116. https://doi.org/10.3390/biomedicines13051116