
Clinical Significance of Tumor Grade in Triple-Negative Breast Cancer: A Retrospective Cohort Analysis

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Inclusion and Exclusion Criteria
2.3. Demographics
2.4. Outcomes
Statistical Analysis Methods for Relapse-Free and Overall Survival
3. Results
3.1. Demographics
3.2. Association Between Grade and Demographic Variables
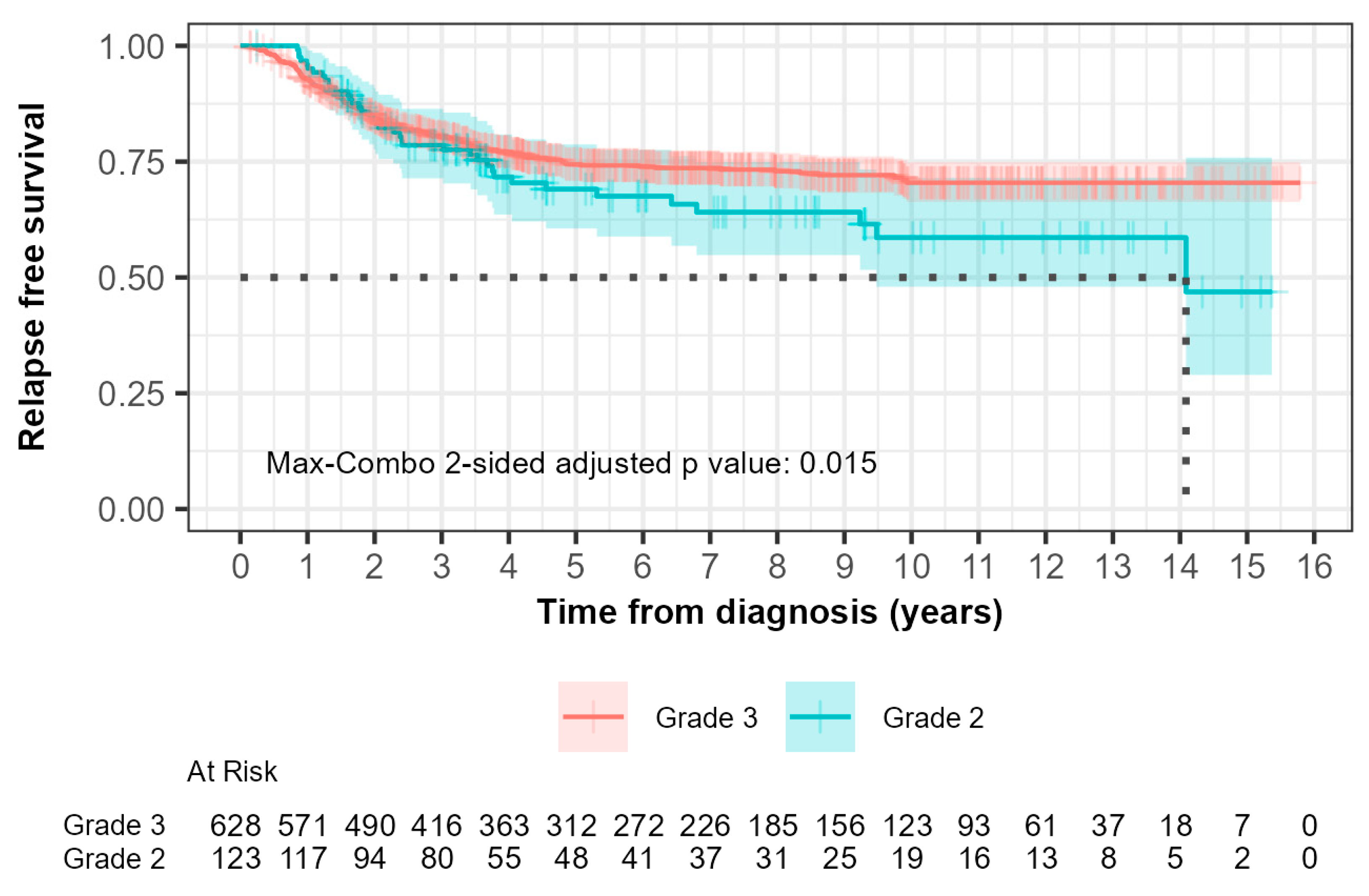
3.3. Grade and Relapse-Free Survival
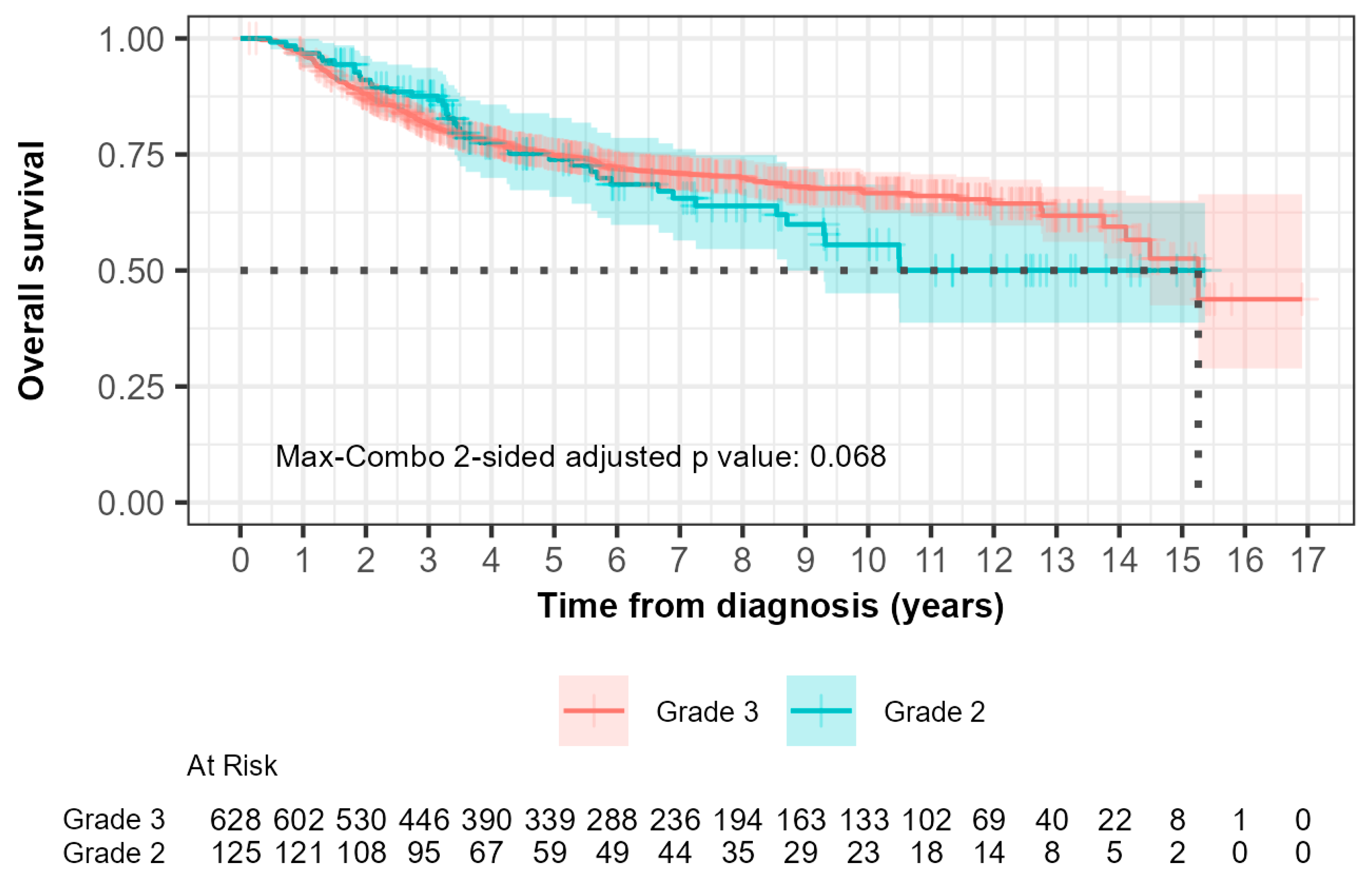
3.4. Grade and Overall Survival
3.5. Relapse-Free and Overall Survival Hazard Ratios
4. Discussion
4.1. Limitations of Our Research
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef]
- Irvin, W.J.; Carey, L.A. What is triple-negative breast cancer? Eur. J. Cancer 2008, 44, 2799–2805. [Google Scholar] [CrossRef] [PubMed]
- Elnashar, A.T.; Ali, E.-S.; Gaber, A. The prognostic value of triple negative in stage II/III breast cancer. J. Oncol. Pharm. Pract. 2012, 18, 68–75. [Google Scholar] [CrossRef]
- Hamm, C.; El-Masri, M.; Poliquin, G.; Poliquin, V.; Mathews, J.; Kanjeekal, S.; Alam, Y.; Kulkarni, S.; Elfiki, T. A single-centre chart review exploring the adjusted association between breast cancer phenotype and prognosis. Curr. Oncol. 2011, 18, 191–196. [Google Scholar] [CrossRef]
- Ovcaricek, T.; Frkovic, S.G.; Matos, E.; Mozina, B.; Borstnar, S. Triple negative breast cancer—Prognostic factors and survival. Radiol. Oncol. 2011, 45, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cortes, J.; Dent, R.; McArthur, H.; Pusztai, L.; Kümmel, S.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Overall Survival with Pembrolizumab in Early-Stage Triple-Negative Breast Cancer. N. Engl. J. Med. 2024, 391, 1981–1991. [Google Scholar] [CrossRef] [PubMed]
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B.; et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med. 2021, 384, 1529–1541. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Zagami, P.; Carey, L.A. Triple negative breast cancer: Pitfalls and progress. NPJ Breast Cancer 2022, 8, 95. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef]
- Institute of Medicine; Board on Health Sciences Policy; Board on Health Care Services; Committee on the Review of Omics-Based Tests for Predicting Patient Outcomes in Clinical Trials. Evolution of Translational Omics: Lessons Learned and the Path Forward; National Academies Press: Washington, DC, USA, 2012.
- McShane, L.M.; Cavenagh, M.M.; Lively, T.G.; Eberhard, D.A.; Bigbee, W.L.; Williams, P.M.; Mesirov, J.P.; Polley, M.Y.; Kim, K.Y.; Tricoli, J.V.; et al. Criteria for the use of omics-based predictors in clinical trials: Explanation and elaboration. BMC Med. 2013, 11, 220. [Google Scholar] [CrossRef]
- Rakha, E.A.; Reis-Filho, J.S.; Baehner, F.; Dabbs, D.J.; Decker, T.; Eusebi, V.; Fox, S.B.; Ichihara, S.; Jacquemier, J.; Lakhani, S.R.; et al. Breast Cancer Prognostic Classification in the Molecular ERa: The role of histological grade. Breast Cancer Res. 2010, 12, 207. [Google Scholar] [CrossRef]
- Bagaria, S.P.; Ray, P.S.; Sim, M.S.; Ye, X.; Shamonki, J.M.; Cui, X.; Giuliano, A.E. Personalizing breast cancer staging by the inclusion of ER, PR, and HER2. JAMA Surg. 2014, 149, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N. AJCC Cancer Staging Manual, 8th ed.; Connolly, J., D’Orsi, C.J., Yang, W.T., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 589–636. [Google Scholar]
- Hamm, C.; Fifield, B.-A.; Kay, A.; Kulkarni, S.; Gupta, R.; Mathews, J.; Ferraiuolo, R.-M.; Al-Wahsh, H.; Mailloux, E.; Hussein, A.; et al. A prospective phase II clinical trial identifying the optimal regimen for carboplatin plus standard backbone of anthracycline and taxane-based chemotherapy in triple negative breast cancer. Med. Oncol. 2022, 39, 49. [Google Scholar] [CrossRef] [PubMed]
- Upneja, S.; Hussein, A.; Moudgil, D.; Kulkarni, S.; Gupta, R.; Kay, A.; Porter, L.; Fifield, B.-A.; Ferraiuolo, R.; Hamm, C. A Retrospective Single Center Study Investigating the Clinical Significance of Grade in Triple Negative Breast Cancer. Cancer Stud. Ther. 2021, 6, 1–8. [Google Scholar]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef] [PubMed]
- LeVee, A.; Wong, M.; Flores, S.; Ruel, N.; McArthur, H.; Waisman, J.; Mortimer, J. Impact of neoadjuvant pembrolizumab adherence on pathologic complete response in triple-negative breast cancer: A real-world analysis. Oncologist 2024, 29, 566–574. [Google Scholar] [CrossRef]
- Jernström, H.; Rydén, L. Into the twilight zone—Should ER-low breast cancer be treated as triple negative breast cancer? Lancet Reg. Health Eur. 2024, 40, 100896. [Google Scholar] [CrossRef]
- Geyer, F.C.; Pareja, F.; Weigelt, B.; Rakha, E.; Ellis, I.O.; Schnitt, S.J.; Reis-Filho, J.S. The Spectrum of Triple-Negative Breast Disease: High- and Low-Grade Lesions. Am. J. Pathol. 2017, 187, 2139–2151. [Google Scholar] [CrossRef]
- Geyer, F.C.; Berman, S.H.; Marchiò, C.; Burke, K.A.; Guerini-Rocco, E.; Piscuoglio, S.; Ng, C.K.; Pareja, F.; Wen, H.Y.; Hodi, Z.; et al. Genetic analysis of microglandular adenosis and acinic cell carcinomas of the breast provides evidence for the existence of a low-grade triple-negative breast neoplasia family. Mod. Pathol. 2017, 30, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Pareja, F.; Geyer, F.C.; Marchiò, C.; Burke, K.A.; Weigelt, B.; Reis-Filho, J.S. Triple-negative breast cancer: The importance of molecular and histologic subtyping, and recognition of low-grade variants. NPJ Breast Cancer 2016, 2, 16036. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.M.; Barcenas, C.H.; Sinha, A.K.; Hsu, L.; Moulder, S.L.; Tripathy, D.; Hortobagyi, G.N.; Valero, V. Long-term survival outcomes of triple-receptor negative breast cancer survivors who are disease free at 5 years and relationship with low hormone receptor positivity. Br. J. Cancer 2018, 118, 17–23. [Google Scholar] [CrossRef]
- Johansson, A.L.V.; Trewin, C.B.; Fredriksson, I.; Reinertsen, K.V.; Russnes, H.; Ursin, G. In modern times, how important are breast cancer stage, grade and receptor subtype for survival: A population-based cohort study. Breast Cancer Res. 2021, 23, 17. [Google Scholar] [CrossRef] [PubMed]
- Park, W.K.; Chung, S.Y.; Jung, Y.J.; Ha, C.; Kim, J.W.; Nam, S.J.; Kim, S.W.; Yu, J.; Chae, B.J.; Lee, J.E.; et al. Long-term oncologic outcomes of unselected triple-negative breast cancer patients according to BRCA1/2 mutations. NPJ Precis. Oncol. 2024, 8, 96. [Google Scholar] [CrossRef]
- Lee, M.; Yoo, T.K.; Chae, B.J.; Lee, A.; Cha, Y.J.; Lee, J.; Ahn, S.G.; Kang, J. Luminal androgen receptor subtype and tumor-infiltrating lymphocytes groups based on triple-negative breast cancer molecular subclassification. Sci. Rep. 2024, 14, 11278. [Google Scholar] [CrossRef]
- Dieci, M.V.; Tsvetkova, V.; Griguolo, G.; Miglietta, F.; Mantiero, M.; Tasca, G.; Cumerlato, E.; Giorgi, C.A.; Giarratano, T.; Faggioni, G.; et al. Androgen Receptor Expression and Association With Distant Disease-Free Survival in Triple Negative Breast Cancer: Analysis of 263 Patients Treated With Standard Therapy for Stage I-III Disease. Front. Oncol. 2019, 9, 452. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) | |
|---|---|---|
| Median age at diagnosis (years) | 63 (25–99) | |
| Cancer stages | Stage I | 238 (31.3%) |
| Stage II | 396 (52.0%) | |
| Stage III | 126 (16.6%) | |
| Missing information | 1 (0.1%) | |
| Type of chemotherapy | Anthracycline based | 71 (9.3%) |
| Taxane based | 41 (5.3%) | |
| Taxane + Anthracycline-based | 268 (35.2%) | |
| Taxane/Anthracycline/Carboplatin-based | 113 (14.5%) | |
| CMF * | 9 (1.2%) | |
| No chemotherapy | 247 (32.5%) | |
| Other ** | 12 (1.5%) | |
| Type of surgery | Mastectomy | 37 (4.9%) |
| Mastectomy and ALND ¥ | 73 (22.7%) | |
| Mastectomy and SLNB § | 103 (13.5%) | |
| Lumpectomy | 18 (2.4%) | |
| Lumpectomy and ALNB | 115 (15.1%) | |
| Lumpectomy and SLNB | 297 (39.0%) | |
| None | 11 (0.1%) | |
| Other | 16 (2.1%) | |
| Missing information | 11(0.1%) | |
| BRCA status | BRCA1 positive | 77(15.6%) |
| BRCA2 positive | 19 (11.0%) | |
| BRCA unknown | 715 (73.4%) | |
| Grade 2 (n = 127) | Grade 3 (n = 634) | p-Value | |
|---|---|---|---|
| Age at diagnosis | < 0.001 1 | ||
| Median | 69.0 | 62.0 | |
| Range | 35.0–99.0 | 25.0–105.0 | |
| Size (cm) | < 0.001 1 | ||
| Median | 2.0 | 2.5 | |
| Range | 0.1–15 | 0.1–15 | |
| Missing information | 2 | 3 | |
| No. of Lymph nodes positive | 0.903 1 | ||
| Median | 0 | 0 | |
| Range | 0–21.0 | 0–35.0 | |
| Missing information | 5 | 16 | |
| Estrogen receptor status % | 0.021 2 | ||
| 0% | 119 (93.7%) | 618 (97.5%) | 0.026 2 |
| 1–9% | 7 (5.5%) | 16 (2.5%) | 0.073 2 |
| =10% | 1 (0.8%) | 0 (0%) | 0.025 2 |
| Progesterone receptor status % | 1.000 2 | ||
| 0% | 123 (96.9%) | 609 (96.1%) | 0.670 2 |
| 1–9% | 4 (3.2%) | 24 (3.8%) | 0.728 2 |
| =10% | 0 (0%) | 1 (0.1%) | 0.654 2 |
| Cancer stages | |||
| Stage 1 | 51 (40.2%) | 187 (29.5%) | |
| Stage 2 | 56 (44.1%) | 340 (53.7%) | |
| Stage 3 | 20 (15.8%) | 106 (16.8%) | |
| Missing information | 0 | 1 | |
| Chemo regimen received | 0.006 2 | ||
| Yes | 73.0 (57.9%) | 441.0 (70.3%) | |
| No | 53.0 (42.1%) | 186.0 (29.7%) | |
| N-Miss | 1 | 7 | |
| Radiation site | 0.938 2 | ||
| N-Miss | 1 | 1 | |
| No | 37 (29.4%) | 171 (27.0%) | |
| Breast | 66 (52.4%) | 334 (52.8%) | |
| Chest Wall | 22 (17.5%) | 121 (19.1%) | |
| Both | 1 (0.8%) | 7 (1.1%) | |
| Hormone therapy | 0.035 2 | ||
| Yes | 9 (7.1%) | 20 (3.2%) | |
| No | 118 (92.9%) | 614 (96.9%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramanan, N.; Malik, M.-n.; Upneja, S.; Farooq, H.; Kulkarni, S.; Gupta, R.; Mathews, J.; Nasser, A.; Bocicariu, A.; Arayan, L.; et al. Clinical Significance of Tumor Grade in Triple-Negative Breast Cancer: A Retrospective Cohort Analysis. Biomedicines 2025, 13, 1100. https://doi.org/10.3390/biomedicines13051100
Ramanan N, Malik M-n, Upneja S, Farooq H, Kulkarni S, Gupta R, Mathews J, Nasser A, Bocicariu A, Arayan L, et al. Clinical Significance of Tumor Grade in Triple-Negative Breast Cancer: A Retrospective Cohort Analysis. Biomedicines. 2025; 13(5):1100. https://doi.org/10.3390/biomedicines13051100
Chicago/Turabian StyleRamanan, Neya, Mah-noor Malik, Sarang Upneja, Haniya Farooq, Swati Kulkarni, Rasna Gupta, John Mathews, Abdullah Nasser, Alina Bocicariu, Laurice Arayan, and et al. 2025. "Clinical Significance of Tumor Grade in Triple-Negative Breast Cancer: A Retrospective Cohort Analysis" Biomedicines 13, no. 5: 1100. https://doi.org/10.3390/biomedicines13051100
APA StyleRamanan, N., Malik, M.-n., Upneja, S., Farooq, H., Kulkarni, S., Gupta, R., Mathews, J., Nasser, A., Bocicariu, A., Arayan, L., Porter, L., Fifield, B.-A., Luo, R., Brackstone, M., & Hamm, C. (2025). Clinical Significance of Tumor Grade in Triple-Negative Breast Cancer: A Retrospective Cohort Analysis. Biomedicines, 13(5), 1100. https://doi.org/10.3390/biomedicines13051100