

The Impact of a Single Hip Manipulation on Quadriceps Activity and Performance: A Randomized Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
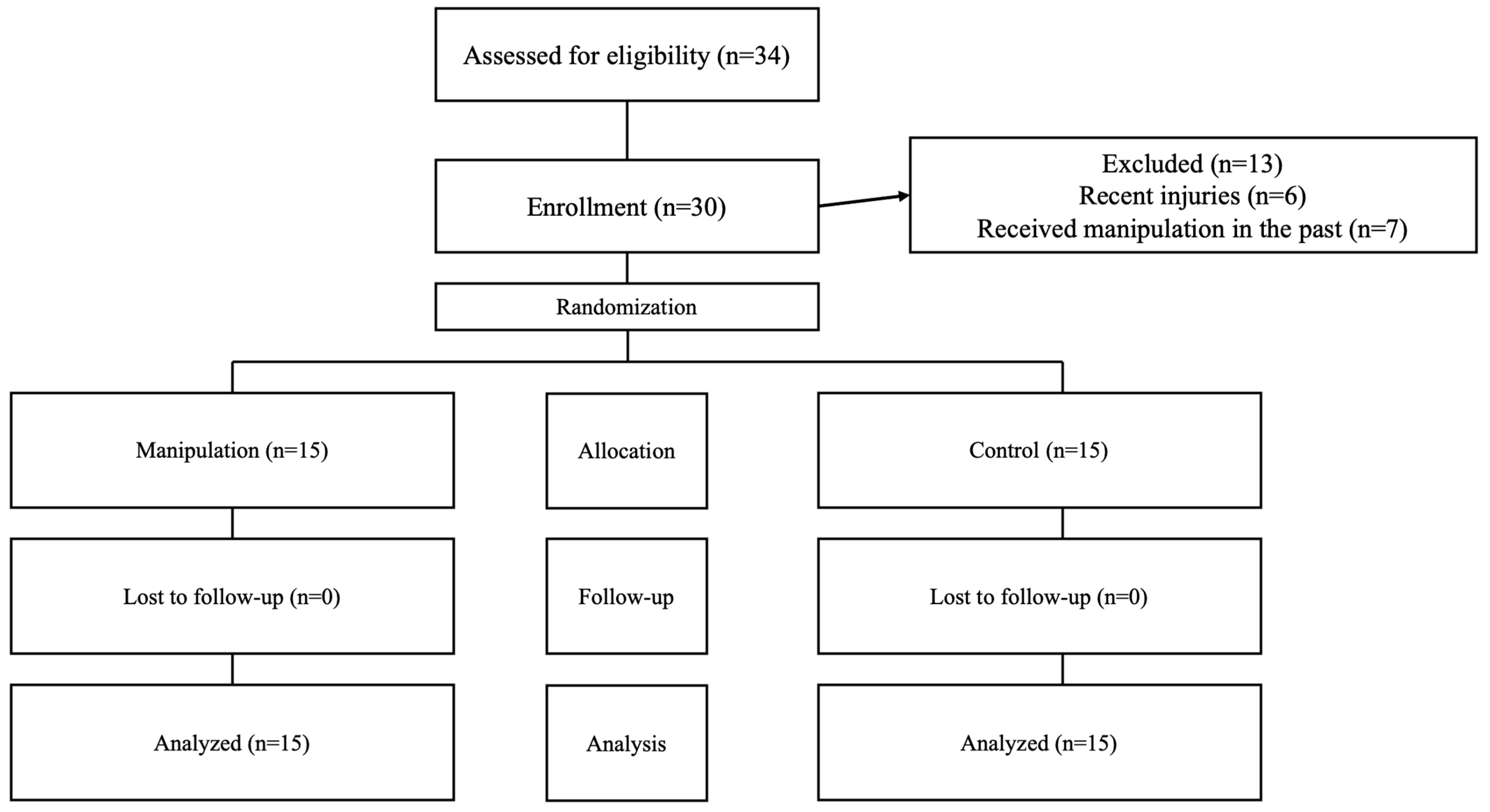
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.4.1. Surface Electromyography
2.4.2. Isometric Knee Extension Strength
2.5. Sample Size
2.6. Randomization
2.7. Blinding
2.8. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Snoeker, B.; Turkiewicz, A.; Magnusson, K.; Frobell, R.; Yu, D.; Peat, G.; Englund, M. Risk of Knee Osteoarthritis after Different Types of Knee Injuries in Young Adults: A Population-Based Cohort Study. Br. J. Sports Med. 2020, 54, 725–730. [Google Scholar] [CrossRef]
- Gage, B.E.; McIlvain, N.M.; Collins, C.L.; Fields, S.K.; Dawn Comstock, R. Epidemiology of 6.6 Million Knee Injuries Presenting to United States Emergency Departments From 1999 Through 2008. Acad. Emerg. Med. 2012, 19, 378–385. [Google Scholar] [CrossRef]
- Culvenor, A.G.; Segal, N.A.; Guermazi, A.; Roemer, F.; Felson, D.T.; Nevitt, M.C.; Lewis, C.E.; Stefanik, J.J. Sex-Specific Influence of Quadriceps Weakness on Worsening Patellofemoral and Tibiofemoral Cartilage Damage: A Prospective Cohort Study. Arthritis Care Res. 2019, 71, 1360–1365. [Google Scholar] [CrossRef] [PubMed]
- Øiestad, B.E.; Juhl, C.B.; Eitzen, I.; Thorlund, J.B. Knee Extensor Muscle Weakness Is a Risk Factor for Development of Knee Osteoarthritis. A Systematic Review and Meta-Analysis. Osteoarthr. Cartil. 2015, 23, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Lepley, A.S.; Gribble, P.A.; Thomas, A.C.; Tevald, M.A.; Sohn, D.H.; Pietrosimone, B.G. Quadriceps Neural Alterations in Anterior Cruciate Ligament Reconstructed Patients: A 6-month Longitudinal Investigation. Scand. J. Med. Sci. Sports 2015, 25, 828–839. [Google Scholar] [CrossRef]
- Whittaker, J.L.; Roos, E.M. A Pragmatic Approach to Prevent Post-Traumatic Osteoarthritis after Sport or Exercise-Related Joint Injury. Best Pract. Res. Clin. Rheumatol. 2019, 33, 158–171. [Google Scholar] [CrossRef]
- Pietrosimone, B.G.; McLeod, M.M.; Lepley, A.S. A Theoretical Framework for Understanding Neuromuscular Response to Lower Extremity Joint Injury. Sports Health A Multidiscip. Approach 2012, 4, 31–35. [Google Scholar] [CrossRef]
- Blasimann, A.; Koenig, I.; Baert, I.; Baur, H.; Vissers, D. Which Assessments Are Used to Analyze Neuromuscular Control by Electromyography after an Anterior Cruciate Ligament Injury to Determine Readiness to Return to Sports? A Systematic Review. BMC Sports Sci. Med. Rehabil. 2021, 13, 142. [Google Scholar] [CrossRef]
- Nagelli, C.; Di Stasi, S.; Tatarski, R.; Chen, A.; Wordeman, S.; Hoffman, J.; Hewett, T.E. Neuromuscular Training Improves Self-Reported Function and Single-Leg Landing Hip Biomechanics in Athletes After Anterior Cruciate Ligament Reconstruction. Orthop. J. Sports Med. 2020, 8, 2325967120959347. [Google Scholar] [CrossRef]
- Malloy, P.; Wichman, D.M.; Garcia, F.; Espinoza-Orías, A.; Chahla, J.; Nho, S.J. Impaired Lower Extremity Biomechanics, Hip External Rotation Muscle Weakness, and Proximal Femoral Morphology Predict Impaired Single-Leg Squat Performance in People With FAI Syndrome. Am. J. Sports Med. 2021, 49, 2984–2993. [Google Scholar] [CrossRef]
- Cashman, G.E. The Effect of Weak Hip Abductors or External Rotators on Knee Valgus Kinematics in Healthy Subjects: A Systematic Review. J. Sport Rehabil. 2012, 21, 273–284. [Google Scholar] [CrossRef]
- Alzahrani, A.M.; Alzhrani, M.; Alshahrani, S.N.; Alghamdi, W.; Alqahtani, M.; Alzahrani, H. Is Hip Muscle Strength Associated with Dynamic Knee Valgus in a Healthy Adult Population? A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7669. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.-D.; Boling, M.C.; Levine, B.; Shultz, S.J. Relationships Between Lower Extremity Alignment and the Quadriceps Angle. Clin. J. Sport Med. 2009, 19, 201–206. [Google Scholar] [CrossRef]
- Ford, K.; Nguyen, A.-D.; Dischiavi, S.; Hegedus, E.; Zuk, E.; Taylor, J. An Evidence-Based Review of Hip-Focused Neuromuscular Exercise Interventions to Address Dynamic Lower Extremity Valgus. Open Access J. Sports Med. 2015, 6, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.-D.; Huang, W.-S.; Lai, P.-T. Muscle Activation of Vastus Medialis Oblique and Vastus Lateralis in Sling-Based Exercises in Patients with Patellofemoral Pain Syndrome: A Cross-Over Study. Evid.-Based Complement. Altern. Med. 2015, 2015, 740315. [Google Scholar] [CrossRef]
- Reiman, M.P.; Bolgla, L.A.; Loudon, J.K. A Literature Review of Studies Evaluating Gluteus Maximus and Gluteus Medius Activation during Rehabilitation Exercises. Physiother. Theory Pract. 2012, 28, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, A.M.; Pasanen, K.; Krosshaug, T.; Vasankari, T.; Kannus, P.; Heinonen, A.; Kujala, U.M.; Avela, J.; Perttunen, J.; Parkkari, J. Association between Frontal Plane Knee Control and Lower Extremity Injuries: A Prospective Study on Young Team Sport Athletes. BMJ Open Sport Exerc. Med. 2018, 4, e000311. [Google Scholar] [CrossRef]
- Vahtrik, D.; Gapeyeva, H.; Aibast, H.; Ereline, J.; Kums, T.; Haviko, T.; Märtson, A.; Schneider, G.; Pääsuke, M. Quadriceps Femoris Muscle Function Prior and after Total Knee Arthroplasty in Women with Knee Osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2017–2025. [Google Scholar] [CrossRef]
- Khayambashi, K.; Mohammadkhani, Z.; Ghaznavi, K.; Lyle, M.A.; Powers, C.M. The Effects of Isolated Hip Abductor and External Rotator Muscle Strengthening on Pain, Health Status, and Hip Strength in Females With Patellofemoral Pain: A Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2012, 42, 22–29. [Google Scholar] [CrossRef]
- Chang, W.-D.; Huang, W.-S.; Lee, C.-L.; Lin, H.-Y.; Lai, P.-T. Effects of Open and Closed Kinetic Chains of Sling Exercise Therapy on the Muscle Activity of the Vastus Medialis Oblique and Vastus Lateralis. J. Phys. Ther. Sci. 2014, 26, 1363–1366. [Google Scholar] [CrossRef]
- Chen, S.; Chang, W.-D.; Wu, J.-Y.; Fong, Y.-C. Electromyographic Analysis of Hip and Knee Muscles during Specific Exercise Movements in Females with Patellofemoral Pain Syndrome. Medicine 2018, 97, e11424. [Google Scholar] [CrossRef] [PubMed]
- Bolgla, L.A.; Boling, M.C. An Update for the Conservative Management of Patellofemoral Pain Syndrome: A Systematic Review of the Literature from 2000 to 2010. Int. J. Sports Phys. Ther. 2011, 6, 112–125. [Google Scholar] [PubMed]
- Fukuda, T.Y.; Rossetto, F.M.; Magalhães, E.; Bryk, F.F.; Garcia Lucareli, P.R.; De Almeida Carvalho, N.A. Short-Term Effects of Hip Abductors and Lateral Rotators Strengthening in Females With Patellofemoral Pain Syndrome: A Randomized Controlled Clinical Trial. J. Orthop. Sports Phys. Ther. 2010, 40, 736–742. [Google Scholar] [CrossRef]
- Studnicki, R.; Tomaszewsk, U.; Hansdorfer-Korzon, R.; Kawczyński, A. Comparing the Acute Effects of Diagonal Mobilization and Nordic Hamstring Curls on Knee Flexion and Extension Strength: A Randomized, Double-Blinded Parallel Study in Young Soccer Players. Appl. Sci. 2024, 14, 8610. [Google Scholar] [CrossRef]
- LaPelusa, A.; Bordoni, B. High-Velocity Low-Amplitude Manipulation Techniques; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Evans, D.W. Mechanisms and Effects of Spinal High-Velocity, Low-Amplitude Thrust Manipulation: Previous Theories. J. Manip. Physiol. Ther. 2002, 25, 251–262. [Google Scholar] [CrossRef]
- Niazi, I.K.; Navid, M.S.; Merkle, C.; Amjad, I.; Kumari, N.; Trager, R.J.; Holt, K.; Haavik, H. A Randomized Controlled Trial Comparing Different Sites of High-Velocity Low Amplitude Thrust on Sensorimotor Integration Parameters. Sci. Rep. 2024, 14, 1159. [Google Scholar] [CrossRef]
- Silva Neto, J.B.; Ismania, C.; de Freitas, D.G.; Cazarini Jr, C.; Martin, R.L.; Fukuda, T.Y. The Effect of a Single High Velocity Low Amplitude Hip Mobilization on Strength in Subjects with Knee Injuries. Musculoskelet. Sci. Pract. 2019, 44, 102051. [Google Scholar] [CrossRef]
- Lawrence, M.A.; Raymond, J.T.; Look, A.E.; Woodard, N.M.; Schicker, C.M.; Swanson, B.T. Effects of Tibiofibular and Ankle Joint Manipulation on Hip Strength and Muscle Activation. J. Manip. Physiol. Ther. 2020, 43, 406–417. [Google Scholar] [CrossRef]
- Studnicki, R.; Naderza, W.; Niespodziński, B.; Hansdorfer-Korzon, R.; Kawczyński, A. Effects of Shoulder Manipulation on Electromyography Measures in Archery Athletes during Recovery from Fatigue: A Comparison between Sexes. Retos 2024, 60, 720–729. [Google Scholar] [CrossRef]
- Studnicki, R.; Szymczyk, P.; Adamczewski, T.; Studzińska, K.; Hansdorfer-Korzon, R.; Silva, A.F.; Kawczyński, A. Manual Traction Is Effective in Alleviating Lumbosacral Spine Pain: Evidence from a Randomized Controlled Trial. Heliyon 2024, 10, e31013. [Google Scholar] [CrossRef]
- Stensgaard Stoltze, J.; Rasmussen, J.; Skipper Andersen, M. On the Biomechanical Relationship between Applied Hip, Knee and Ankle Joint Moments and the Internal Knee Compressive Forces. Int. Biomech. 2018, 5, 63–74. [Google Scholar] [CrossRef]
- Merkow, R.P.; Kaji, A.H.; Itani, K.M.F. The CONSORT Framework. JAMA Surg. 2021, 156, 877–878. [Google Scholar] [CrossRef]
- Studnicki, R.; Skup, K.; Sochaj, M.; Niespodziński, B.; Aschenbrenner, P.; Laskowski, R.; Łuczkiewicz, P. Hip Manipulation Increases Electromyography Amplitude and Hip Joint Performance: A Double-Blind Randomized Controlled Study. Life 2024, 14, 1353. [Google Scholar] [CrossRef]
- Sugiura, Y.; Hatanaka, Y.; Arai, T.; Sakurai, H.; Kanada, Y. Estimations of One Repetition Maximum and Isometric Peak Torque in Knee Extension Based on the Relationship Between Force and Velocity. J. Strength Cond. Res. 2016, 30, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Maroco, J. Análise Estatística Com Utilização Do SPSS [Statistical Analysis with SPSS]; Edições Silabo: Lisbon, Portugal, 2012. [Google Scholar]
- Richardson, J.T.E. Eta Squared and Partial Eta Squared as Measures of Effect Size in Educational Research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Robinault, L.; Holobar, A.; Crémoux, S.; Rashid, U.; Niazi, I.K.; Holt, K.; Lauber, J.; Haavik, H. The Effects of Spinal Manipulation on Motor Unit Behavior. Brain Sci. 2021, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Gyer, G.; Michael, J.; Inklebarger, J.; Tedla, J.S. Spinal Manipulation Therapy: Is It All about the Brain? A Current Review of the Neurophysiological Effects of Manipulation. J. Integr. Med. 2019, 17, 328–337. [Google Scholar] [CrossRef]
- Roberts, A.; Harris, K.; Outen, B.; Bukvic, A.; Smith, B.; Schultz, A.; Bergman, S.; Mondal, D. Osteopathic Manipulative Medicine: A Brief Review of the Hands-On Treatment Approaches and Their Therapeutic Uses. Medicines 2022, 9, 33. [Google Scholar] [CrossRef]
- Pickar, J.G.; Bolton, P.S. Spinal Manipulative Therapy and Somatosensory Activation. J. Electromyogr. Kinesiol. 2012, 22, 785–794. [Google Scholar] [CrossRef]
- Bevilaqua Grossi, D.; Pedro, V.M.; Bérzin, F. Análise Funcional Dos Estabilizadores Patelares. Acta Ortop. Bras. 2004, 12, 99–104. [Google Scholar] [CrossRef]
- Carr, J.C.; Stock, M.S.; Hernandez, J.M.; Ortegon, J.R.; Mota, J.A. Additional Insight into Biarticular Muscle Function: The Influence of Hip Flexor Fatigue on Rectus Femoris Activity at the Knee. J. Electromyogr. Kinesiol. 2018, 42, 36–43. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Experimental Group (n = 15) | Control Group (n = 15) | |
|---|---|---|
| Men (n) | 11 | 11 |
| Women (n) | 4 | 4 |
| Age (years) | 21.9 ± 1.7 | 22.1 ± 1.8 |
| Height (cm) | 178.3 ± 9.7 | 181.5 ± 9.5 |
| Body mass (kg) | 74.4 ± 11.6 | 76.6 ± 16.2 |
| Body mass index (kg/m2) | 20.8 | 21.1 |
| Knee extension (Nm) | 218.7 | 215 |
| Fat tissue (%) | 15.9 | 15.6 |
| Outcomes | Experimental Group (n = 15) | Control Group (n = 15) |
|---|---|---|
| VL mean amplitude of EMGRMS (µV) | ||
| Pre | 372.5 ± 211.8 | 414.1 ± 235.5 |
| Post | 397.5 ± 216.7 | 381.4 ± 215.4 |
| Within-group difference (p-value|d) | p = 0.125|d = 0.117, trivial ES | p = 0.048 *|d = −0.145, trivial ES |
| VM mean amplitude of EMGRMS (µV) | ||
| Pre | 377.4 ± 191.6 | 521.3 ± 267.5 |
| Post | 473.0 ± 175.7 | 414.3 ± 211.6 |
| Within-group difference (p-value|d) | p < 0.001 *|d = 0.521, small ES | p < 0.001 *|d = −0.447, small ES |
| RF mean amplitude of EMGRMS (µV) | ||
| Pre | 264.7 ± 103.5 | 340.4 ± 142.3 |
| Post | 292.2 ± 89.6 | 313.7 ± 131.9 |
| Within-group difference (p-value|d) | p = 0.086|d = 0.285, small ES | p = 0.096|d = −0.195, trivial ES |
| VL max amplitude of EMGRMS (µV) | ||
| Pre | 526.2 ± 268.5 | 542.2 ± 314.0 |
| Post | 526.3 ± 294.5 | 497.9 ± 275.1 |
| Within-group difference (p-value|d) | p = 0.995|d < 0.001, trivial ES | p = 0.193|d = −0.150, trivial ES |
| VM max amplitude of EMGRMS (µV) | ||
| Pre | 600.2 ± 315.1 | 737.3 ± 491.4 |
| Post | 688.3 ± 308.6 | 608.3 ± 388.8 |
| Within-group difference (p-value|d) | p = 0.019 *|d = 0.283, small ES | p = 0.001 *|d = −0.293, small ES |
| RF max amplitude of EMGRMS (µV) | ||
| Pre | 341.7 ± 122.9 | 436.5 ± 180.7 |
| Post | 374.9 ± 115.8 | 400.0 ± 166.0 |
| Within-group difference (p-value|d) | p = 0.101|d = 0.278, small ES | p = 0.072|d = −0.211, small ES |
| VL median frequency of raw SEMG signal power spectrum (EMGMED, Hz) | ||
| Pre | 51.9 ± 7.2 | 55.5 ± 7.7 |
| Post | 55.2 ± 4.9 | 56.5 ± 7.2 |
| Within-group difference (p-value|d) | p = 0.017 *|d = 0.545, small ES | p = 0.458|d = 0.134, trivial ES |
| VM median frequency of raw SEMG signal power spectrum (EMGMED, Hz) | ||
| Pre | 53.9 ± 11.3 | 55.4 ± 6.7 |
| Post | 55.3 ± 6.1 | 54.1 ± 6.1 |
| Within-group difference (p-value|d) | p = 0.484|d = 0.161, small ES | p = 0.495|d = −0.203, small ES |
| RL median frequency of raw SEMG signal power spectrum (EMGMED, Hz) | ||
| Pre | 76.2 ± 16.0 | 77.3 ± 14.7 |
| Post | 75.3 ± 17.2 | 79.9 ± 13.8 |
| Within-group difference (p-value|d) | p = 0.592|d = −0.054, trivial ES | p = 0.127|d = 0.182, trivial ES |
| Outcomes | Experimental Group (n = 15) | Control Group (n = 15) |
|---|---|---|
| VL/VM ratio—mean amplitude of EMGRMS (µV) | ||
| Pre | 1.18 ± 0.73 | 0.85 ± 0.36 |
| Post | 0.83 ± 0.28 | 0.98 ± 0.40 |
| Within-group difference (p-value|d) | p = 0.007|d = −0.693, moderate ES | p = 0.878|d = 0.342, small ES |
| VL/VM ratio—max amplitude of EMGRMS (µV) | ||
| Pre | 1.16 ± 0.99 | 0.83 ± 0.37 |
| Post | 0.83 ± 0.28 | 0.91 ± 0.39 |
| Within-group difference (p-value|d) | p = 0.044|d = −0.520, small ES | p = 0.412|d = 0.211, small ES |
| VL/VM ratio—median frequency of raw SEMG signal power spectrum (EMGMED, Hz) | ||
| Pre | 1.09 ± 0.37 | 1.09 ± 0.37 |
| Post | 1.07 ± 0.15 | 1.08 ± 0.42 |
| Within-group difference (p-value|d) | p = 0.674|d = −0.077, trivial ES | p = 0.833|d = −0.025, trivial ES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Studnicki, R.; Sochaj, M.; Skup, K.; Niespodziński, B.; Aschenbrenner, P.; Laskowski, R.; Łuczkiewicz, P. The Impact of a Single Hip Manipulation on Quadriceps Activity and Performance: A Randomized Study. Biomedicines 2025, 13, 900. https://doi.org/10.3390/biomedicines13040900
Studnicki R, Sochaj M, Skup K, Niespodziński B, Aschenbrenner P, Laskowski R, Łuczkiewicz P. The Impact of a Single Hip Manipulation on Quadriceps Activity and Performance: A Randomized Study. Biomedicines. 2025; 13(4):900. https://doi.org/10.3390/biomedicines13040900
Chicago/Turabian StyleStudnicki, Rafał, Monika Sochaj, Karol Skup, Bartłomiej Niespodziński, Piotr Aschenbrenner, Radosław Laskowski, and Piotr Łuczkiewicz. 2025. "The Impact of a Single Hip Manipulation on Quadriceps Activity and Performance: A Randomized Study" Biomedicines 13, no. 4: 900. https://doi.org/10.3390/biomedicines13040900
APA StyleStudnicki, R., Sochaj, M., Skup, K., Niespodziński, B., Aschenbrenner, P., Laskowski, R., & Łuczkiewicz, P. (2025). The Impact of a Single Hip Manipulation on Quadriceps Activity and Performance: A Randomized Study. Biomedicines, 13(4), 900. https://doi.org/10.3390/biomedicines13040900