


The Association Between Severity of Constipation and Oral Frailty Index-8 in the JUSTICE-TOKYO Study: A Cross-Sectional Study
 , ,
, ,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
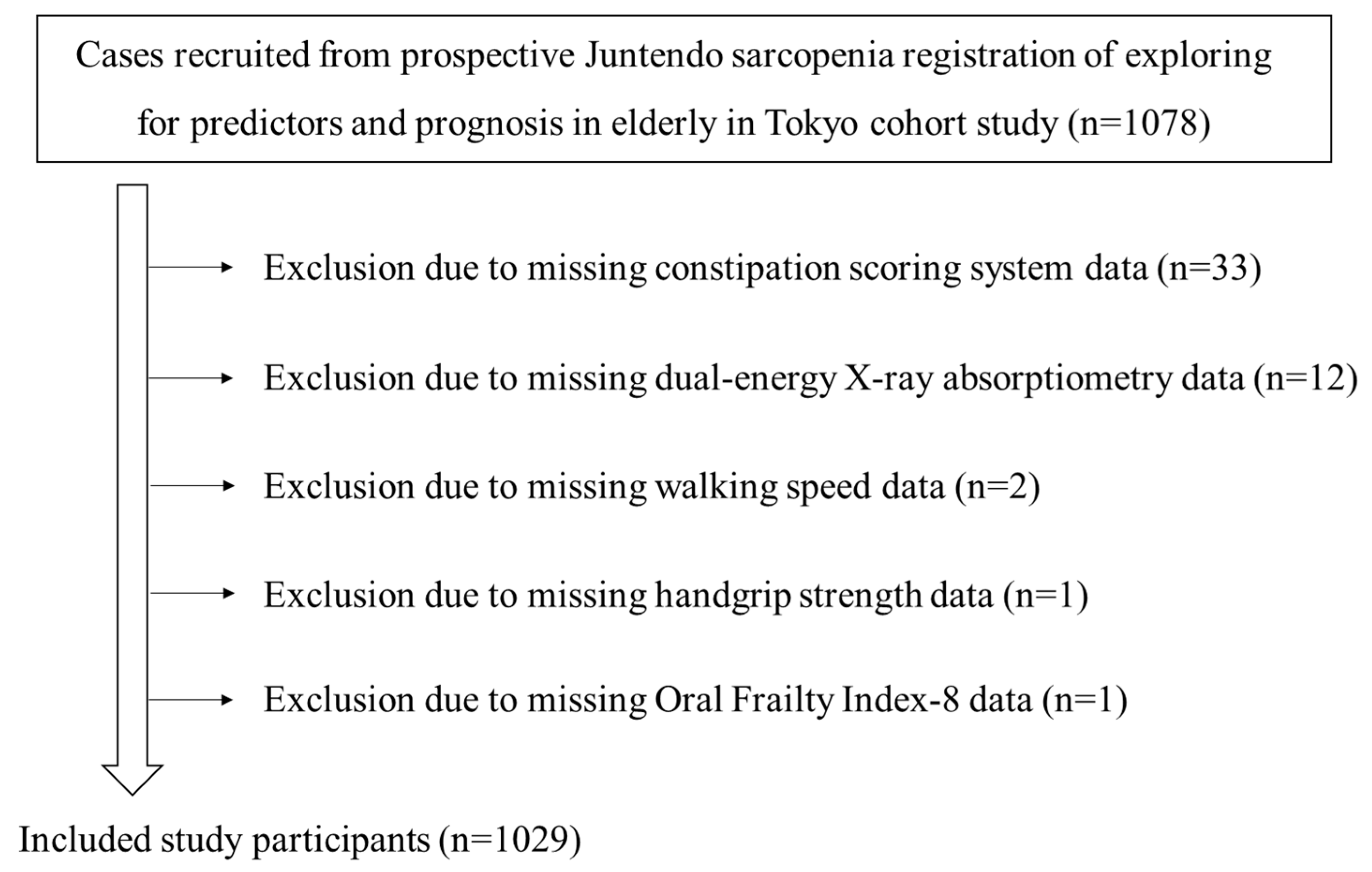
2.1. Study Cohort
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Measurement of Baseline Variables
2.5. Endpoint
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Correlation Between CSS and Various Clinical Parameters (UVA)
3.3. Association Between CSS and Other Variables (MRA)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suares, N.C.; Ford, A.C. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: Systematic review and meta-analysis. Am. J. Gastroenterol. 2011, 106, 1582–1591. [Google Scholar] [CrossRef] [PubMed]
- Gallegos-Orozco, J.F.; Foxx-Orenstein, A.E.; Sterler, S.M.; Stoa, J.M. Chronic constipation in the elderly. Am. J. Gastroenterol. 2012, 107, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Tamura, A.; Tomita, T.; Oshima, T.; Toyoshima, F.; Yamasaki, T.; Okugawa, T.; Kondo, T.; Kono, T.; Tozawa, K.; Ikehara, H.; et al. Prevalence and Self-Recognition of Chronic Constipation: Results of an Internet Survey. J. Neurogastroenterol. Motil. 2016, 22, 677–685. [Google Scholar] [CrossRef]
- Wald, A.; Scarpignato, C.; Kamm, M.A.; Mueller-Lissner, S.; Helfrich, I.; Schuijt, C.; Bubeck, J.; Limoni, C.; Petrini, O. The burden of constipation on quality of life: Results of a multinational survey. Aliment. Pharmacol. Ther. 2007, 26, 227–236. [Google Scholar] [CrossRef]
- Belsey, J.; Greenfield, S.; Candy, D.; Geraint, M. Systematic review: Impact of constipation on quality of life in adults and children. Aliment. Pharmacol. Ther. 2010, 31, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Tomita, T.; Kazumori, K.; Baba, K.; Zhao, X.; Chen, Y.; Miwa, H. Impact of chronic constipation on health-related quality of life and work productivity in Japan. J. Gastroenterol. Hepatol. 2021, 36, 1529–1537. [Google Scholar] [CrossRef]
- Honkura, K.; Tomata, Y.; Sugiyama, K.; Kaiho, Y.; Watanabe, T.; Zhang, S.; Sugawara, Y.; Tsuji, I. Defecation frequency and cardiovascular disease mortality in Japan: The Ohsaki cohort study. Atherosclerosis 2016, 246, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Choung, R.S.; Rey, E.; Locke, G.R., III; Schleck, C.D.; Baum, C.; Zinsmeister, A.R.; Talley, N.J. Chronic constipation and co-morbidities: A prospective population-based nested case-control study. United Eur. Gastroenterol. J. 2016, 4, 142–151. [Google Scholar] [CrossRef]
- Chang, J.Y.; Locke, G.R., III; McNally, M.A.; Halder, S.L.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J. Impact of functional gastrointestinal disorders on survival in the community. Am. J. Gastroenterol. 2010, 105, 822–832. [Google Scholar] [CrossRef]
- Sumida, K.; Molnar, M.Z.; Potukuchi, P.K.; Thomas, F.; Lu, J.L.; Yamagata, K.; Kalantar-Zadeh, K.; Kovesdy, C.P. Constipation and risk of death and cardiovascular events. Atherosclerosis 2019, 281, 114–120. [Google Scholar] [CrossRef]
- Passmore, A.P. Economic aspects of pharmacotherapy for chronic constipation. Pharmacoeconomics 1995, 7, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Satake, S.; Arai, H. The revised Japanese version of the Cardiovascular Health Study criteria (revised J-CHS criteria). Geriatr. Gerontol. Int. 2020, 20, 992–993. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef]
- Matsuno, K.; Asaoka, D.; Sugano, K.; Takahashi, K.; Miyauchi, K. Rationale and design of Juntendo Sarcopenia Registration to explore the predictors and prognosis of sarcopenia and frailty in the elderly in TOKYO (JUSTICE-TOKYO). Geriatr. Gerontol. Int. 2024, 24, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Soen, S.; Fukunaga, M.; Sugimoto, T.; Sone, T.; Fujiwara, S.; Endo, N.; Gorai, I.; Shiraki, M.; Hagino, H.; Hosoi, T.; et al. Diagnostic criteria for primary osteoporosis: Year 2012 revision. J. Bone Miner. Metab. 2013, 31, 247–257. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Tanaka, T.; Hirano, H.; Ohara, Y.; Nishimoto, M.; Iijima, K. Oral Frailty Index-8 in the risk assessment of new-onset oral frailty and functional disability among community-dwelling older adults. Arch. Gerontol. Geriatr. 2021, 94, 104340. [Google Scholar] [CrossRef] [PubMed]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Agachan, F.; Chen, T.; Pfeifer, J.; Reissman, P.; Wexner, S.D. A constipation scoring system to simplify evaluation and management of constipated patients. Dis. Colon Rectum 1996, 39, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Sugishita, K.; Sugishita, M.; Hemmi, I.; Asada, T.; Tanigawa, T. A Validity and Reliability Study of the Japanese Version of the Geriatric Depression Scale 15 (GDS-15-J). Clin. Gerontol. 2017, 40, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Kakuta, E.; Yamashita, N.; Katsube, T.; Kushiyama, Y.; Suetsugu, H.; Furuta, K.; Kinoshita, Y. Abdominal symptom-related QOL in individuals visiting an outpatient clinic and those attending an annual health check. Intern. Med. 2011, 50, 1517–1522. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. Nihon Koshu Eisei Zasshi 2003, 50, 1117–1124. [Google Scholar]
- Kusunoki, H.; Hasegawa, Y.; Nagasawa, Y.; Shojima, K.; Yamazaki, H.; Mori, T.; Tsuji, S.; Wada, Y.; Tamaki, K.; Nagai, K.; et al. Oral Frailty and Its Relationship with Physical Frailty in Older Adults: A Longitudinal Study Using the Oral Frailty Five-Item Checklist. Nutrients 2024, 17, 17. [Google Scholar] [CrossRef]
- Asaoka, D.; Takeda, T.; Inami, Y.; Abe, D.; Shimada, Y.; Matsumoto, K.; Ueyama, H.; Matsumoto, K.; Komori, H.; Akazawa, Y.; et al. The Association Between Frailty and Abdominal Symptoms: A Hospital-Based Cross-Sectional Study. Intern. Med. 2020, 59, 1677–1685. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Huang, S.S.; Yen, C.W.; Kabasawa, Y.; Lee, C.H.; Huang, H.L. Physical Frailty and Oral Frailty Associated with Late-Life Depression in Community-Dwelling Older Adults. J. Pers. Med. 2022, 12, 459. [Google Scholar] [CrossRef] [PubMed]
- Asaoka, D.; Takeda, T.; Inami, Y.; Abe, D.; Shimada, Y.; Matsumoto, K.; Ueyama, H.; Matsumoto, K.; Komori, H.; Akazawa, Y.; et al. Association between the severity of constipation and sarcopenia in elderly adults: A single-center university hospital-based, cross-sectional study. Biomed. Rep. 2021, 14, 2. [Google Scholar] [CrossRef]
- Park, H.; Lim, J.; Baek, J.Y.; Lee, E.; Jung, H.W.; Jang, I.Y. Status of Constipation and Its Association with Sarcopenia in Older Adults: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 11083. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.B. Associations between physical activity and constipation in adult Americans: Results from the National Health and Nutrition Examination Survey. Neurogastroenterol. Motil. 2020, 32, e13789. [Google Scholar] [CrossRef] [PubMed]
- Lucak, S.; Lunsford, T.N.; Harris, L.A. Evaluation and Treatment of Constipation in the Geriatric Population. Clin. Geriatr. Med. 2021, 37, 85–102. [Google Scholar] [CrossRef]
- Rao, S.S.; Bharucha, A.E.; Chiarioni, G.; Felt-Bersma, R.; Knowles, C.; Malcolm, A.; Wald, A. Anorectal Disorders. Gastroenterology 2016, 150, 1430–1442.e4. [Google Scholar] [CrossRef]
- Yamamoto, S.; Ohashi, W.; Yamaguchi, Y.; Igari, H.; Koshino, A.; Sugiyama, T.; Nagao, K.; Tamura, Y.; Izawa, S.; Mano, M.; et al. Factors Associated with Defecation Satisfaction among Japanese Adults with Chronic Constipation. J. Clin. Med. 2024, 13, 3216. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Osadnik, C.; Phu, S.; Morita, A.A.; Duque, G.; Probst, V.S. Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef]
- Gürsoy Coşkun, G.; Andac-Ozturk, S.; Arslan Ulukan, Z. Comparison of constipation and nutritional status with disease-related parameters in chronic obstructive pulmonary disease patients. Int. J. Clin. Pract. 2021, 75, e14451. [Google Scholar] [CrossRef]
- Shen, Z.; Qiu, B.; Chen, L.; Zhang, Y. Common gastrointestinal diseases and chronic obstructive pulmonary disease risk: A bidirectional Mendelian randomization analysis. Front. Genet. 2023, 14, 1256833. [Google Scholar] [CrossRef]
- Kagiali, S.; Inal-Ince, D.; Cakmak, A.; Calik-Kutukcu, E.; Saglam, M.; Vardar-Yagli, N.; Tekerlek, H.; Sonbahar-Ulu, H.; Arikan, H.; Bozdemir-Ozel, C.; et al. Daily living activities, exercise capacity, cognition, and balance in COPD patients with and without frailty. Ir. J. Med. Sci. 2022, 191, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Labour and Welfare. 2022. Available online: https://www.mhlw.go.jp/english/database/db-hss/cslc-report2022.html (accessed on 26 December 2024).

{kind=link}
| Patient profile |
| Age (years) |
| Sex (male/female) |
| Body mass index (kg/m2) |
| Brinkman Index: the number of cigarettes smoked per day multiplied by the number of years of smoking |
| Alcohol drinking habits: 0, 1, and 2 indicate rarely, 1–4 days per week, and 5–7 days per week, respectively |
| QOL (EQ-5D): 0 and 100 indicate worst and perfect health, respectively |
| History of falls |
| History of day care use |
| SMI (kg/m2), measured using DXA scanning (GE Healthcare, Madison, WI, USA) |
| Handgrip strength (kg) |
| Walking speed (m/s) |
| Comorbidities |
| Cerebral infarction/hemorrhage |
| Myocardial infarction |
| Hospitalization for heart failure |
| Interstitial pneumonia |
| Chronic hepatic disease |
| History of malignant disease |
| Hypertension |
| Diabetes mellitus |
| Atrial fibrillation |
| Osteoporosis: diagnosed according to the criteria of the Japanese Society for Bone and Mineral Research |
| Frailty: diagnosed using the J-CHS criteria, adapted from the original Cardiovascular Health Study criteria |
| Sarcopenia: defined using the diagnostic algorithm recommended by the Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment |
| Use of therapeutic agents |
| Statins |
| Acid secretion suppressants |
| Laxatives |
| Non-steroidal anti-inflammatory drugs |
| Number of oral medicines |
| Oral function |
| Oral frailty: evaluated based on the Oral Frailty Index-8 (OFI-8) score using an 8-point scale |
| Dysphagia: assessed based on the 10-item Eating Assessment Tool (EAT-10) |
| Severity of constipation |
| CSS score (frequency of bowel movements, painful evacuation, incomplete evacuation, abdominal pain, length of time per attempt, assistance for evacuation, unsuccessful attempts at evacuation per 24 h, and duration of constipation). The overall CSS score (i.e., the sum of the point scores for each item) ranged from 0–30, with higher scores indicating worse constipation symptoms. |
| Neuropsychological examination |
| Mini-Mental State Examination (MMSE) |
| 15-item Geriatric Depression Scale (GDS-15) |
| Abdominal symptom-related QOL scores |
| This self-administered questionnaire (the Izumo scale) includes 15 items in five domains (i.e., reflux, upper abdominal pain, fullness, constipation, and diarrhea). Each item is scored using a Likert scale (range: 0–5). Domain-specific QOL impairment on the Izumo scale is ranked from 0 (indicating no QOL impairment) to 15 (indicating severe QOL impairment). |
| Pulmonary function |
| SpO2 (%) |
| The impact of COPD on the health status was evaluated based on the CAT, consisting of eight items. A CAT score ≥10 indicates severe symptoms. |
| Nutritional status |
| Hypozincemia was defined as treatment with zinc acetate hydrate (Novelzin® Tablets; Nobelpharma K.K., Tokyo, Japan) or serum zinc levels < 80 µg/dL. |
| The CONUT score (range: 0–12) was used to investigate the objective nutritional status. This score was calculated using the serum albumin levels, total cholesterol levels, and total lymphocyte count. |
| The DVS comprises 10 food-based components. |
| Patient profile | |
| Mean age (years) | 78.3 ± 6.1 ** |
| Sex | |
| Male | 450 (43.7) * |
| Female | 579 (56.3) * |
| Body mass index (kg/m2) | 22.9 ± 3.9 ** |
| Brinkman Index | 355.9 ± 615.1 ** |
| Alcohol drinking habit | 0.5 ± 0.8 ** |
| QOL (EQ-5D) | 74.9 ± 17.0 ** |
| History of falls | 207 (20.1) * |
| History of day care use | 94 (9.1) * |
| SMI | 6.3 ± 0.9 ** |
| Handgrip strength (kg) | 25.9 ± 8.5 ** |
| Walking speed (m/s) | 1.2 ± 0.4 ** |
| Comorbidities | |
| Cerebral infarction/hemorrhage | 80 (7.8) * |
| Myocardial infarction | 47 (4.6) * |
| Hospitalization for heart failure | 42 (4.1) * |
| Interstitial pneumonia | 55 (5.3) * |
| Chronic hepatic disease | 126 (12.2) * |
| History of malignant disease | 55 (5.3) * |
| Hypertension | 606 (58.9) * |
| Diabetes mellitus | 319 (31.0) * |
| Atrial fibrillation | 88 (8.6) * |
| Osteoporosis | 337 (32.8) * |
| Frailty | 174 (16.9) * |
| Sarcopenia | 223 (21.7) * |
| Use of therapeutic agents | |
| Statins | 430 (41.8) * |
| Acid secretion suppressants | 562 (54.6) * |
| Laxatives | 226 (22.0) * |
| Non-steroidal anti-inflammatory drugs | 76 (7.4) * |
| Number of oral medicines | 6.1 ± 3.5 ** |
| Oral function | |
| Oral Frailty Index-8 | 3.9 ± 2.4 ** |
| EAT-10 | 1.6 ± 3.6 ** |
| Severity of constipation | |
| CSS score | 3.4 ± 3.7 ** |
| Neuropsychological examination | |
| MMSE | 26.5 ± 3.1 ** |
| GDS-15 | 4.2 ± 3.0 ** |
| Abdominal symptom-related QOL scores | |
| Reflux | 1.8 ± 2.4 ** |
| Upper abdominal pain | 1.1 ± 2.0 ** |
| Fullness | 1.6 ± 2.4 ** |
| Constipation | 2.2 ± 2.6 ** |
| Diarrhea | 2.1 ± 2.6 ** |
| Pulmonary function | |
| SpO2 (%) | 97.2 ± 2.4 ** |
| CAT | 8.6 ± 6.6 ** |
| Nutritional status | |
| Hypozincemia | 807 (78.4) * |
| CONUT score | 1.0 ± 1.2 ** |
| DVS | 3.7 ± 2.2 ** |
| Patient profile | r, η | p-Value |
| Age (years) | 0.083 | 0.007 † |
| Sex (female) | 0.008 | 0.792 |
| Body mass index (kg/m2) | −0.033 | 0.291 |
| Brinkman Index | 0.016 | 0.673 |
| Alcohol drinking habit | −0.036 | 0.246 |
| QOL (EQ-5D) | −0.251 | <0.001 † |
| History of falls | 0.166 | <0.001 † |
| History of day care use | 0.143 | <0.001 † |
| SMI | −0.037 | 0.236 |
| Handgrip strength (kg) | −0.086 | 0.006 † |
| Walking speed (m/s) | −0.154 | <0.001 † |
| Comorbidities | ||
| Cerebral infarction/hemorrhage | 0.055 | 0.077 |
| Myocardial infarction | 0.000 | 0.987 |
| Hospitalization for heart failure | 0.003 | 0.923 |
| Interstitial pneumonia | 0.032 | 0.312 |
| Chronic hepatic disease | 0.045 | 0.147 |
| History of malignant disease | 0.030 | 0.336 |
| Hypertension | 0.052 | 0.094 |
| Diabetes mellitus | 0.011 | 0.718 |
| Atrial fibrillation | 0.049 | 0.114 |
| Osteoporosis | 0.013 | 0.667 |
| Frailty | 0.193 | <0.001 † |
| Sarcopenia | 0.075 | 0.017 † |
| Use of therapeutic agents | ||
| Statins | 0.009 | 0.761 |
| Acid secretion suppressants | 0.054 | 0.086 |
| Laxatives | 0.314 | <0.001 † |
| Non-steroidal anti-inflammatory drugs | 0.001 | 0.975 |
| Number of oral medicines | 0.153 | <0.001 † |
| Oral function | ||
| Oral Frailty Index-8 | 0.294 | <0.001 † |
| EAT-10 | 0.291 | <0.001 † |
| Neuropsychological examination | ||
| MMSE | −0.063 | 0.049 † |
| GDS-15 | 0.285 | <0.001 † |
| Abdominal symptom-related QOL scores | ||
| Reflux | 0.285 | <0.001 † |
| Upper abdominal pain | 0.279 | <0.001 † |
| Fullness | 0.337 | <0.001 † |
| Constipation | 0.694 | <0.001 † |
| Diarrhea | 0.307 | <0.001 † |
| Pulmonary function | ||
| SpO2 (%) | −0.014 | 0.645 |
| CAT | 0.329 | <0.001 † |
| Nutritional status | ||
| Hypozincemia | 0.054 | 0.085 |
| CONUT score | 0.282 | <0.001 † |
| DVS | −0.124 | <0.001 † |
| Covariates | β | t | 95% CI | p-Value |
| Oral Frailty Index-8 | 0.065 | 2.461 | 0.020, 0.181 | 0.014 † |
| EAT-10 | 0.061 | 2.294 | 0.009, 0.112 | 0.022 † |
| Sarcopenia | 0.050 | 2.176 | 0.045, 0.866 | 0.030 † |
| Laxative | 0.126 | 5.246 | 0.711, 1.561 | <0.001 † |
| QOL score related to constipation | 0.625 | 22.613 | 0.830, 0.9987 | <0.001 † |
| QOL score related to diarrhea | −0.064 | −2.404 | −0.165, −0.017 | 0.016 † |
| CAT | 0.061 | 2.217 | 0.004, 0.064 | 0.027 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeda, T.; Asaoka, D.; Kiko, H.; Kanazawa, T.; Nomura, O.; Oki, S.; Hojo, M.; Sugano, K.; Matsuno, K.; Inoshita, H.; et al. The Association Between Severity of Constipation and Oral Frailty Index-8 in the JUSTICE-TOKYO Study: A Cross-Sectional Study. Biomedicines 2025, 13, 813. https://doi.org/10.3390/biomedicines13040813
Takeda T, Asaoka D, Kiko H, Kanazawa T, Nomura O, Oki S, Hojo M, Sugano K, Matsuno K, Inoshita H, et al. The Association Between Severity of Constipation and Oral Frailty Index-8 in the JUSTICE-TOKYO Study: A Cross-Sectional Study. Biomedicines. 2025; 13(4):813. https://doi.org/10.3390/biomedicines13040813
Chicago/Turabian StyleTakeda, Tsutomu, Daisuke Asaoka, Hiroyuki Kiko, Takuya Kanazawa, Osamu Nomura, Shotaro Oki, Mariko Hojo, Koji Sugano, Kei Matsuno, Hiroyuki Inoshita, and et al. 2025. "The Association Between Severity of Constipation and Oral Frailty Index-8 in the JUSTICE-TOKYO Study: A Cross-Sectional Study" Biomedicines 13, no. 4: 813. https://doi.org/10.3390/biomedicines13040813
APA StyleTakeda, T., Asaoka, D., Kiko, H., Kanazawa, T., Nomura, O., Oki, S., Hojo, M., Sugano, K., Matsuno, K., Inoshita, H., Nishizaki, Y., Yanagisawa, N., Shinohara, M., Nagahara, A., & Miyauchi, K. (2025). The Association Between Severity of Constipation and Oral Frailty Index-8 in the JUSTICE-TOKYO Study: A Cross-Sectional Study. Biomedicines, 13(4), 813. https://doi.org/10.3390/biomedicines13040813