

Calciphylaxis Following Parathyroidectomy in Chronic Kidney Disease Patients—Case Report and Literature Review

 , ,
, , 
Abstract
1. Introduction
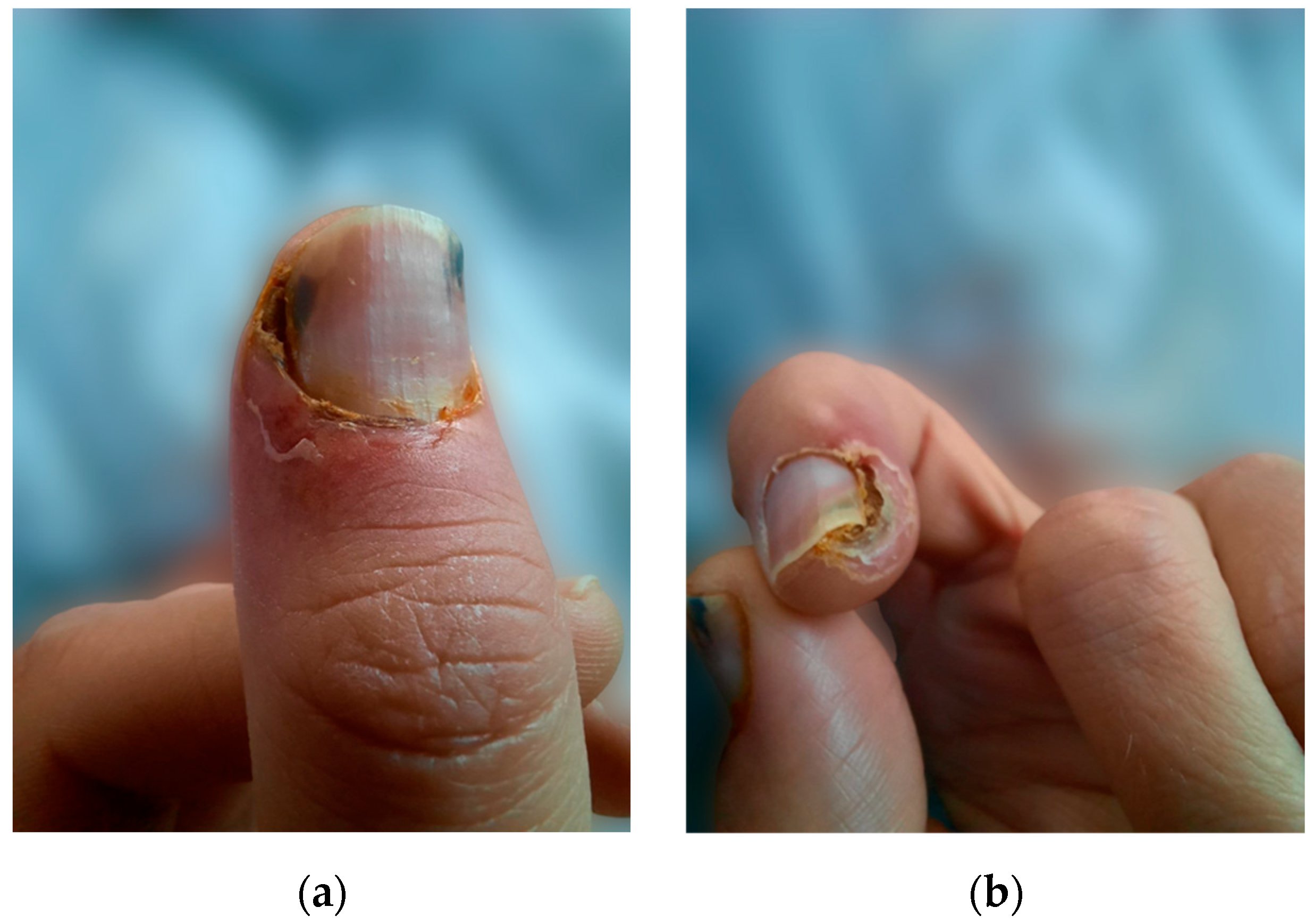
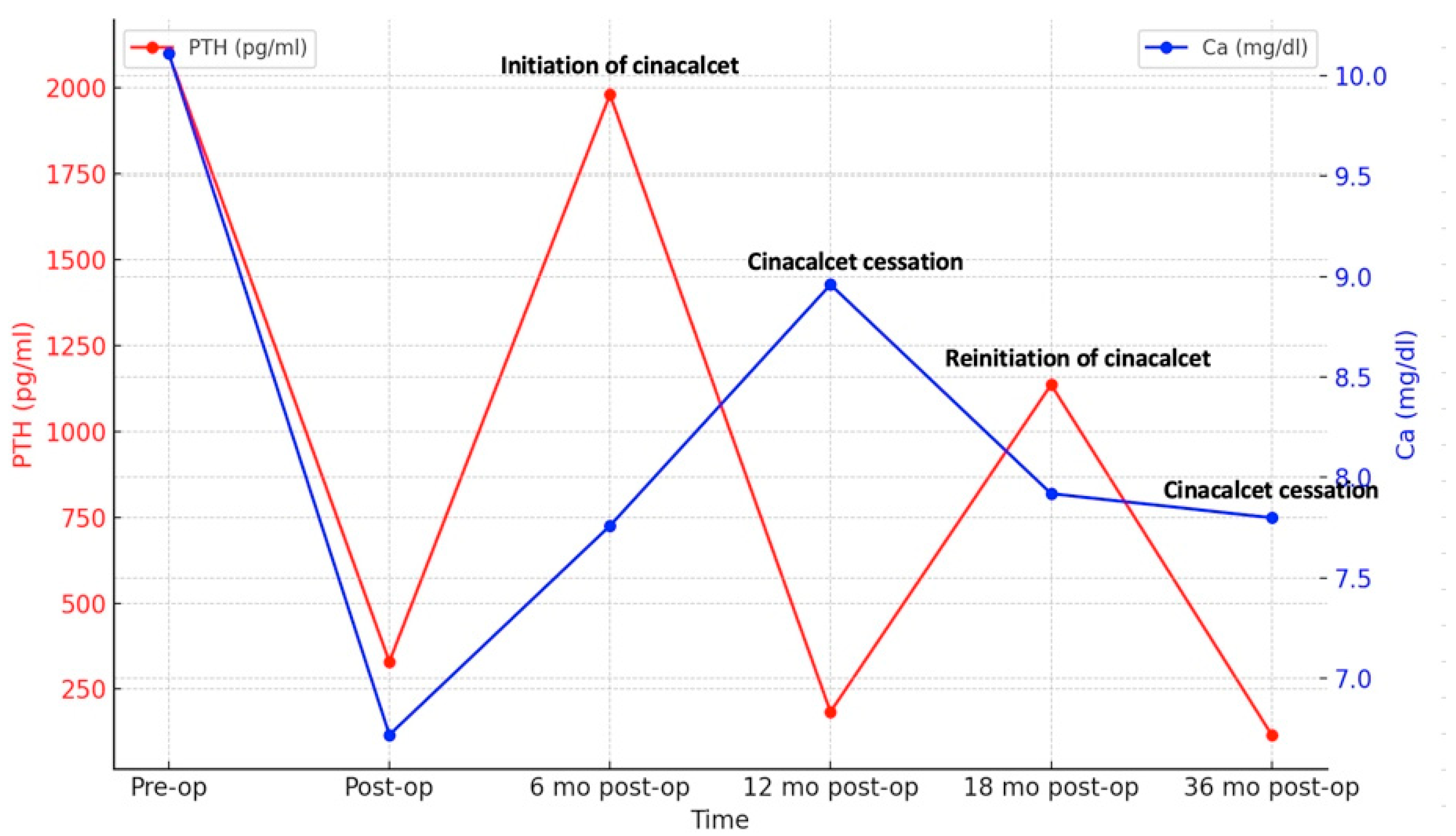
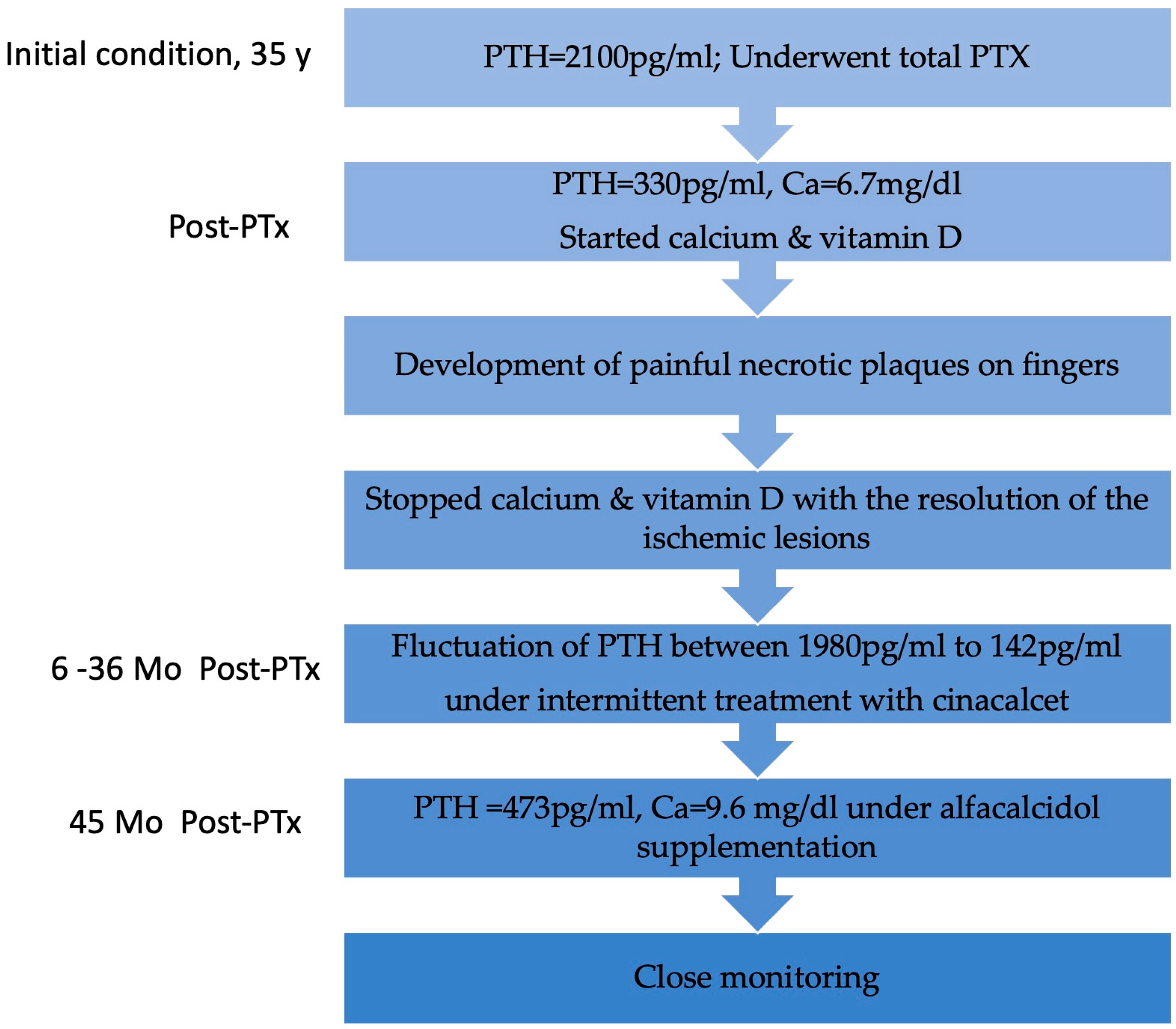
2. Case Report
3. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CUA | calcific uremic arteriopathy |
| CKD | chronic kidney disease |
| KTR | kidney transplant recipient |
| HD | hemodialysis |
| PTx | parathyroidectomy |
| PTH | parathormone |
| Ca | calcium |
| P | phosphate |
| MGP | matrix G1a protein |
| ESRD | end-stage renal disease |
| RRT | renal replacement therapy |
| CKD-MBD | chronic kidney disease-mineral bone disorder |
| DXA | dual X-ray absorptiometry |
| BMD-DXA | bone mineral density-dual X-ray absorptiometry |
| BMP | bone morphogenetic protein |
| iPTH | intact parathormone |
| DM | diabetes mellitus |
| SHPT | secondary hyperparathyroidism |
| STS | sodium thiosulfate |
| NKF-KDOQI | National Kidney Foundation-Kidney Disease Outcomes Quality Initiative |
References
- Liu, Y.; Zhang, X. Early Diagnosis Strategy of Calciphylaxis in Dialysis Patients. Ren. Fail. 2023, 45, 2264407. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Bulteel, N.; Alfonzo, A.; Gupta, S. Successful Treatment of Severe Calciphylaxis in a Renal Transplant Patient with Previous Total Parathyroidectomy. J. R. Coll. Physicians Edinb. 2023, 53, 207–211. [Google Scholar] [CrossRef]
- Nigwekar, S.U.; Wolf, M.; Sterns, R.H.; Hix, J.K. Calciphylaxis from Nonuremic Causes: A Systematic Review. Clin. J. Am. Soc. Nephrol. 2008, 3, 1139–1143. [Google Scholar] [CrossRef]
- Chinnadurai, R.; Huckle, A.; Hegarty, J.; Kalra, P.A.; Sinha, S. Calciphylaxis in End-Stage Kidney Disease: Outcome Data from the United Kingdom Calciphylaxis Study. J. Nephrol. 2021, 34, 1537–1545. [Google Scholar] [CrossRef]
- Nigwekar, S.U.; Kroshinsky, D.; Nazarian, R.M.; Goverman, J.; Malhotra, R.; Jackson, V.A.; Kamdar, M.M.; Steele, D.J.R.; Thadhani, R.I. Calciphylaxis: Risk Factors, Diagnosis, and Treatment. Am. J. Kidney Dis. 2015, 66, 133. [Google Scholar] [CrossRef]
- Gallo Marin, B.; Aghagoli, G.; Hu, S.L.; Massoud, C.M.; Robinson-Bostom, L. Calciphylaxis and Kidney Disease: A Review. Am. J. Kidney Dis. 2023, 81, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Nigwekar, S.U.; Solid, C.A.; Ankers, E.; Malhotra, R.; Eggert, W.; Turchin, A.; Thadhani, R.I.; Herzog, C.A. Quantifying a Rare Disease in Administrative Data: The Example of Calciphylaxis. J. Gen. Intern. Med. 2014, 29 (Suppl. 3), 724–731. [Google Scholar] [CrossRef]
- Sanha, V.; Vidori, L.; Pachi, B.C.; Marchezi, L.V.; Meinerz, G. A Rare Case of Post-Parathyroidectomy Calciphylaxis in a Young Patient With End-Stage Renal Disease: A Case Report and Literature Review. Cureus 2023, 15, e42937. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, X.; Xie, X.; Yang, X.; Liu, H.; Tang, R.; Liu, B. Risk Factors for Calciphylaxis in Chinese Hemodialysis Patients: A Matched Case-Control Study. Ren. Fail. 2021, 43, 406. [Google Scholar] [CrossRef]
- Nagy, E.; Sobh, M.M.; Abdalbary, M.; Elnagar, S.; Elrefaey, R.; Shabaka, S.; Elshabrawy, N.; Shemies, R.; Tawfik, M.; Santos, C.G.S.; et al. Is Adynamic Bone Always a Disease? Lessons from Patients with Chronic Kidney Disease. J. Clin. Med. 2022, 11, 7130. [Google Scholar] [CrossRef]
- Mori, K.; Shoji, T.; Nakatani, S.; Uedono, H.; Ochi, A.; Yoshida, H.; Imanishi, Y.; Morioka, T.; Tsujimoto, Y.; Kuro-O, M.; et al. Differential Associations of Fetuin-A and Calcification Propensity with Cardiovascular Events and Subsequent Mortality in Patients Undergoing Hemodialysis. Clin. Kidney J. 2024, 17, sfae042. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Chu, X.L.; Cao, J.H.; Peng, Y.H. Correlation of Serum Klotho, Fetuin-A, and MGP Levels with Coronary Artery Calcification in Maintenance Hemodialysis Patients. Clinics 2024, 79, 100417. [Google Scholar] [CrossRef]
- Wahab, M.A.; Al Kanhal, F. Calciphylaxis after Parathyroidectomy in Chronic Renal Failure. Saudi J. Kidney Dis. Transpl. 2008, 19, 854–860. [Google Scholar]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [PubMed]
- Poch, E.; Almirall, J.; Alsina, M.; del Río, R.; Cases, A.; Revert, L. Calciphylaxis in a Hemodialysis Patient: Appearance after Parathyroidectomy during a Psoriatic Flare. Am. J. Kidney Dis. 1992, 19, 285–288. [Google Scholar] [CrossRef]
- Oikawa, S.; Osajima, A.; Tamura, M.; Murata, K.; Yasuda, H.; Anai, H.; Kabashima, N.; Matsushima, Y.; Nakamoto, M.; Nakashima, Y. Development of Proximal Calciphylaxis with Penile Involvement after Parathyroidectomy in a Patient on Hemodialysis. Intern. Med. 2004, 43, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Matstusoka, S.; Tominaga, Y.; Uno, N.; Goto, N.; Sato, T.; Katayama, A.; Haba, T.; Uchida, K.; Kobayashi, K.; Nakao, A. Calciphylaxis: A Rare Complication of Patients Who Required Parathyroidectomy for Advanced Renal Hyperparathyroidism. World J. Surg. 2005, 29, 632–635. [Google Scholar] [CrossRef]
- Bonilla, L.A.; Dickson-Witmer, D.; Witmer, D.R.; Kirby, W. Calciphylaxis Mimicking Inflammatory Breast Cancer. Breast J. 2007, 13, 514–516. [Google Scholar] [CrossRef]
- Katikaneni, M.; Lwin, L.; Villanueva, H.; Yoo, J. Calciphylaxis and Subtotal Parathyroidectomy: A Double-Edged Sword. Hemodial. Int. 2013, 17 (Suppl. 1), S33–S36. [Google Scholar] [CrossRef]
- Bashir, S.O.; Aamer, M.A.; Omer, H.A.; Morsy, M.D. Penile Calcific Uremic Arteriolopathy Occurring Postparathyroidectomy in a Hemodialysis Patient. Saudi J. Kidney Dis. Transpl. 2016, 27, 1265–1269. [Google Scholar] [CrossRef]
- Karmegam, S.; Shetty, A. Calciphylaxis after Parathyroidectomy. Hemodial. Int. 2017, 21 (Suppl. 2), S62–S66. [Google Scholar] [CrossRef] [PubMed]
- Hristov, I.; Elena, A.; Radu, D. Severe Calcific Uremic Arteriolopathy Lessions and Acute Hypocalcemia after Parathyroidectomy for Secondary Hyperparathyroidism in Haemodialysis Patients: Case Series. Endocr. Abstr. 2023, 90, EP191. [Google Scholar] [CrossRef]
- Nasr, R.; Ghazanfar, H. Parathyroidectomy as a Cure for Calciphylaxis in a Non-Dialysis Chronic Kidney Disease Patient? Am. J. Case Rep. 2019, 20, 1170. [Google Scholar] [CrossRef] [PubMed]
- Roza, K.; George, J.C.; Bermudez, M.; Mehta, Z. Uremic Calciphylaxis #325. J. Palliat. Med. 2017, 20, 424–425. [Google Scholar] [CrossRef]
- Colboc, H.; Moguelet, P.; Bazin, D.; Carvalho, P.; Dillies, A.S.; Chaby, G.; Maillard, H.; Kottler, D.; Goujon, E.; Jurus, C.; et al. Localization, Morphologic Features, and Chemical Composition of Calciphylaxis-Related Skin Deposits in Patients With Calcific Uremic Arteriolopathy. JAMA Dermatol. 2019, 155, 789–796. [Google Scholar] [CrossRef]
- Mizuiri, S.; Nishizawa, Y.; Yamashita, K.; Ono, K.; Naito, T.; Tanji, C.; Usui, K.; Doi, S.; Masaki, T.; Shigemoto, K. Relationship of Matrix Gla Protein and Vitamin K with Vascular Calcification in Hemodialysis Patients. Ren. Fail. 2019, 41, 770–777. [Google Scholar] [CrossRef]
- Panchal, S.; Holtermann, K.; Trivedi, N.; Regunath, H.; Yerram, P. Calciphylaxis: An Analysis of Concomitant Factors, Treatment Effectiveness and Prognosis in 30 Patients. Int. J. Nephrol. Renov. Dis. 2020, 13, 65. [Google Scholar] [CrossRef]
- Hill Gallant, K.M.; Spiegel, D.M. Calcium Balance in Chronic Kidney Disease. Curr. Osteoporos. Rep. 2017, 15, 214. [Google Scholar] [CrossRef]
- Rothe, H.; Brandenburg, V.; Haun, M.; Kollerits, B.; Kronenberg, F.; Ketteler, M.; Wanner, C. Ecto-5’-Nucleotidase CD73 (NT5E), Vitamin D Receptor and FGF23 Gene Polymorphisms May Play a Role in the Development of Calcific Uremic Arteriolopathy in Dialysis Patients—Data from the German Calciphylaxis Registry. PLoS ONE 2017, 12, e0172407. [Google Scholar] [CrossRef]
- King, B.J.; el-Azhary, R.A.; McEvoy, M.T.; Shields, R.C.; McBane, R.D.; McCarthy, J.T.; Davis, M.D.P. Direct Oral Anticoagulant Medications in Calciphylaxis. Int. J. Dermatol. 2017, 56, 1065–1070. [Google Scholar] [CrossRef]
- Musso, C.G.; Enz, P.A.; Kowalczuk, A.; Cozzolino, M.; Brandenburg, V.; Nigwekar, S. Differential Diagnosis of Calciphylaxis in Chronic Dialysis Patients. Int. Urol. Nephrol. 2020, 52, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.J. Calciphylaxis: Diagnosis, Pathogenesis, and Treatment. Adv. Ski. Wound Care 2019, 32, 205–215. [Google Scholar] [CrossRef]
- Carsote, M.; Nistor, C. Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism. Diagnostics 2023, 13, 1953. [Google Scholar] [CrossRef]
- Miedziaszczyk, M.; Idasiak-Piechocka, I.; Wisniewski, O.W.; Lacka, K. A Systematic Review of the Pharmacotherapy of Secondary Hyperparathyroidism (SHPT) in Grades 3-5 Chronic Kidney Disease (CKD). Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Deen, J.; Schaider, H. The Use of Cinacalcet for the Treatment of Calciphylaxis in Patients with Chronic Kidney Disease: A Comprehensive Review. Australas. J. Dermatol. 2019, 60, e186–e194. [Google Scholar] [CrossRef]
- Negri, A.L.; Bover, J.; Vervloet, M.; Cozzolino, M. New Calcimimetics for Secondary Hyperparathyroidism in CKD G5D: Do They Offer Advantages? J. Nephrol. 2024, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sprague, S.M. Painful Skin Ulcers in a Hemodialysis Patient. Clin. J. Am. Soc. Nephrol. 2014, 9, 166–173. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Kongnatthasate, K.; Praditpornsilpa, K.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Treatment of Calciphylaxis in CKD: A Systematic Review and Meta-Analysis. Kidney Int. Rep. 2018, 4, 231. [Google Scholar] [CrossRef]
- Nigwekar, S.U.; Zhao, S.; Wenger, J.; Hymes, J.L.; Maddux, F.W.; Thadhani, R.I.; Chan, K.E. A Nationally Representative Study of Calcific Uremic Arteriolopathy Risk Factors. J. Am. Soc. Nephrol. 2016, 27, 3421–3429. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BMD-DXA | L1-L4 Z-Score | Femoral Neck Z-Score | Forearm Z-Score |
|---|---|---|---|
| 2021 | −1.4 | −1.8 | NA 1 |
| 2024 | −1.3 | −0.7 | −5.8 |
| Author | M/F | Age (y) | Type of RRT | HD/Pdvintage | PTx Indication | Pre-PTx PTH (pg/mL) | Type of PTx | Post-PTx PTH (pg/mL) | Distribution of the Lesions | Time After PTx | Diagnostic Methods | Risk Factors | Therapeutic Approach After PTx |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Poch et al., 1992 [15] | M | 62 | HD | 8 y | SHPT, severe signs of osteodystrophy | 1205 | Subtotal PTx | 213 | Distal lower and upper extremities | 3 mo | Skin biopsy | Autoimmune conditions, prolonged application of topical therapies for psoriasis; deficiency of protein C; calcium supplementation for hypocalcemia | Calcitriol; calcium supplements; topical treatment for psoriatic lesions; transferred to PD 3 months later |
| Oikawa et al., 2004 [16] | M | 32 | PD-HD | 13 y | SHPT | Unknown | PTx (not specified) | 63 during the onset of symptoms | Back, lower abdominal wall, lower extremities, penile and scrotal involvement | 2 y | Skin biopsy; X-ray; 99mTc-methylene disphosphonate; CT scan | Obesity followed by marked weight loss, corticosteroid medication | Hyperbaric oxygen for whole body; prostaglandin E1; continuous hemodiafiltration and endotoxin absorption; antibiotics; catecholamines; analgesics and narcotics |
| Matstusoka et al., 2005 [17] | F | 57 | HD | 24 y | SHPT | Unknown | Total PTx with forearm autograft | 120 | Lower extremities | Unknown | Skin biopsy | Unknown | Medical and dermatological treatment |
| M | 42 | HD | 15 y | SHPT | Unknown | Total PTx with forearm autograft | 705 | Trunk and extremities | 3 y | Skin biopsy | Unknown | Low calcium dialysate, calcitonin agent, bisphosphonates | |
| F | 48 | HD | 16 y | SHPT | Unknown | Total PTx with forearm autograft | 180 | Lower extremities | Unknown | Skin biopsy | Unknown | Medical and dermatological treatment | |
| Bonilla et al., 2007 [18] | F | 59 | HD | unknown | Calciphylaxis | Unknown | Subtotal PTx | Unknown | Breast | Unknown | Skin biopsy | Anticoagulation (specific type not mentioned) | Fine-needle aspiration; total mastectomy (because of the nonhealing wound and severe breast pain); another PTx |
| Wahab et al., 2008 [13] | M | 33 | HD | 9 y | SHPT | 3489 | Subtotal PTx | 47 | Distal lower extremities | 7 w | Skin biopsy | Unknown | Dermatological treatment, antibiotics, skin grafting |
| Katikaneni et al., 2013 [19] | F | 62 | HD | 5 y | Calciphylaxis | 1513 | Subtotal PTx | 406 | Breast, thigh, and lower abdominal wall | 16 mo | Skin biopsy | Obesity; DM2; calciphylaxis prior to PTx, calcium supplementation and vitamin D analog for hypocalcemia | 25 g of STS 3 times weekly; high calcium dialysate, sevelamer carbonate |
| Bashir et al., 2016 [20] | M | 46 | HD | 14 y | SHPT, Pathological fractures | 2000 | Subtotal PTx | 891 | Penile | 2 w | CT scan | Calcium supplementation and vitamin D analog for hypocalcemia | Low calcium dialysate; high dose of sevelamer; local antibiotic; traditional treatment (honey, local herbs) |
| Karmegam and Shetty, 2017 [21] | M | 60 | HD | 2.5 y | HPT and osteopenia | 4191 | Subtotal PTx | 184 | Lower extremity and buttocks | 4 w | Skin biopsy | DM2, prednisone usage for pain relief | Wound care; antibiotics; increased duration of HD session; 25 g STS with all HD sessions; high-dose oral calcium and vitamin D supplements; oral opiods, topical lidocaine, gabapentine; prednisone |
| Sanha et al., 2023 [8] | F | 26 | HD | 4 y | Brown tumor due to SHPT | >2000 | Total PTx with forearm autograft | 43 (on the first postoperative day), 118 (4 weeks later) | Distal lower extremities | 3 w | Clinical diagnosis (negative early biopsy) | No risk factors mentioned | Wound care; pain management; antibiotics, STS |
| Hristov et al., 2023 [22] | M | 46 | HD | 8 y | SHPT | >1400 | Subtotal PTx | values of 120–250 | Unknown | Unknown | Unknown | Unknown | Surgical debridement; antibiotics; discontinuation of anti-vitamin K; nutritional support |
| M | 49 | HD | 11 y | SHPT | >1400 | Subtotal PTx | values of 120–250 | Unknown | Unknown | Unknown | Unknown | Surgical debridment; antibiotics; discontinuation of anti-vitamin K; nutritional support | |
| Smith et al., 2023 [2] | F | 60 | KTx | 7 y | SHPT | 396 | Total PTx | <9 | Left lower leg | 3 y | Histopathology | DM, anticoagulation with anti-vitamin K | Limb amputation; STS, discotinuation of anti-vitamin K; vitamin K2 supplementation |
| Our study, 2024 | M | 36 | HD-DP-HD | 16 y | SHPT | 2100 | Total PTx | 330 | Distal upper extremities | 8 w | Clinical diagnosis | Calcium supplementation and vitamin D analog for hypocalcemia | Discontinuation of calcium supplementation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akad, N.; Bilha, S.C.; Apetrii, M.; Akad, F.; Bilha, M.; Hogas, M.; Hogas, S.; Ungureanu, M.-C.; Preda, C.; Covic, A. Calciphylaxis Following Parathyroidectomy in Chronic Kidney Disease Patients—Case Report and Literature Review. Biomedicines 2025, 13, 715. https://doi.org/10.3390/biomedicines13030715
Akad N, Bilha SC, Apetrii M, Akad F, Bilha M, Hogas M, Hogas S, Ungureanu M-C, Preda C, Covic A. Calciphylaxis Following Parathyroidectomy in Chronic Kidney Disease Patients—Case Report and Literature Review. Biomedicines. 2025; 13(3):715. https://doi.org/10.3390/biomedicines13030715
Chicago/Turabian StyleAkad, Nada, Stefana Catalina Bilha, Mugurel Apetrii, Fawzy Akad, Madalina Bilha, Mihai Hogas, Simona Hogas, Maria-Christina Ungureanu, Cristina Preda, and Adrian Covic. 2025. "Calciphylaxis Following Parathyroidectomy in Chronic Kidney Disease Patients—Case Report and Literature Review" Biomedicines 13, no. 3: 715. https://doi.org/10.3390/biomedicines13030715
APA StyleAkad, N., Bilha, S. C., Apetrii, M., Akad, F., Bilha, M., Hogas, M., Hogas, S., Ungureanu, M.-C., Preda, C., & Covic, A. (2025). Calciphylaxis Following Parathyroidectomy in Chronic Kidney Disease Patients—Case Report and Literature Review. Biomedicines, 13(3), 715. https://doi.org/10.3390/biomedicines13030715