
Residual TPO Content of Photopolymerized Additively Manufactured Dental Occlusal Splint Materials

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schweiger, J.; Edelhoff, D.; Guth, J.F. 3D Printing in Digital Prosthetic Dentistry: An Overview of Recent Developments in Additive Manufacturing. J. Clin. Med. 2021, 10, 2010. [Google Scholar] [CrossRef]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef]
- Kessler, A.; Hickel, R.; Reymus, M. 3D Printing in Dentistry-State of the Art. Oper. Dent. 2020, 45, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Wealleans, J.; Ray, J. Endodontic applications of 3D printing. Int. Endod. J. 2018, 51, 1005–1018. [Google Scholar] [CrossRef] [PubMed]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, J.N. Additive Technology: Update on Current Materials and Applications in Dentistry. J. Prosthodont. 2017, 26, 156–163. [Google Scholar] [CrossRef]
- Bencharit, S.; Staffen, A.; Yeung, M.; Whitley, D.; Laskin, D.M.; Deeb, G.R. In Vivo Tooth-Supported Implant Surgical Guides Fabricated With Desktop Stereolithographic Printers: Fully Guided Surgery Is More Accurate Than Partially Guided Surgery. J. Oral. Maxillofac. Surg. 2018, 76, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.H.; Lonic, D.; Lo, L.J. 3D printing in orthognathic surgery—A literature review. J. Formos. Med. Assoc. 2018, 117, 547–558. [Google Scholar] [CrossRef]
- Kouhi, M.; de Souza Araujo, I.J.; Asa’ad, F.; Zeenat, L.; Bojedla, S.S.R.; Pati, F.; Zolfagharian, A.; Watts, D.C.; Bottino, M.C.; Bodaghi, M. Recent advances in additive manufacturing of patient-specific devices for dental and maxillofacial rehabilitation. Dent. Mater. 2024, 40, 700–715. [Google Scholar] [CrossRef]
- Lutz, A.M.; Hampe, R.; Roos, M.; Lumkemann, N.; Eichberger, M.; Stawarczyk, B. Fracture resistance and 2-body wear of 3-dimensional-printed occlusal devices. J. Prosthet. Dent. 2019, 121, 166–172. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, L.; Wu, D.; Yu, C.; Fan, S.; Cai, B. Effectiveness of exercise therapy versus occlusal splint therapy for the treatment of painful temporomandibular disorders: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 6122–6132. [Google Scholar] [CrossRef]
- Hardy, R.S.; Bonsor, S.J. The efficacy of occlusal splints in the treatment of bruxism: A systematic review. J. Dent. 2021, 108, 103621. [Google Scholar] [CrossRef] [PubMed]
- Reymus, M.; Hickl, R.; Keßler, A. Accuracy of CAD/CAM-fabricated bite splints: Milling vs. 3D printing. Clin. Oral Investig. 2020, 24, 4607–4615. [Google Scholar] [CrossRef]
- Cole, D.; Bencharit, S.; Carrico, C.K.; Arias, A.; Tufekci, E. Evaluation of fit for 3D-printed retainers compared with thermoform retainers. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 592–599. [Google Scholar] [CrossRef]
- Kessler, A.; Reichl, F.X.; Folwaczny, M.; Hogg, C. Monomer release from surgical guide resins manufactured with different 3D printing devices. Dent. Mater. 2020, 36, 1486–1492. [Google Scholar] [CrossRef] [PubMed]
- Alifui-Segbaya, F.; Bowman, J.; White, A.R.; Varma, S.; Lieschke, G.J.; George, R. Toxicological assessment of additively manufactured methacrylates for medical devices in dentistry. Acta Biomater. 2018, 78, 64–77. [Google Scholar] [CrossRef]
- Ikemura, K.; Endo, T. A review of the development of radical photopolymerization initiators used for designing light-curing dental adhesives and resin composites. Dent. Mater. J. 2010, 29, 481–501. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Lin, L.D.; Wu, M.T.; Chan, C.P.; Chang, H.H.; Lee, M.S.; Sun, T.Y.; Jeng, P.Y.; Yeung, S.Y.; Lin, H.J.; et al. Effects of Camphorquinone on Cytotoxicity, Cell Cycle Regulation and Prostaglandin E2 Production of Dental Pulp Cells: Role of ROS, ATM/Chk2, MEK/ERK and Hemeoxygenase-1. PLoS ONE 2015, 10, e0143663. [Google Scholar] [CrossRef]
- Wedekind, L.; Güth, J.-F.; Schweiger, J.; Kollmuss, M.; Reichl, F.-X.; Edelhoff, D.; Högg, C. Elution behavior of a 3D-printed, milled and conventional resin-based occlusal splint material. Dent. Mater. 2021, 37, 701–710. [Google Scholar] [CrossRef]
- Kim, G.T.; Go, H.B.; Yu, J.H.; Yang, S.Y.; Kim, K.M.; Choi, S.H.; Kwon, J.S. Cytotoxicity, Colour Stability and Dimensional Accuracy of 3D Printing Resin with Three Different Photoinitiators. Polymers 2022, 14, 979. [Google Scholar] [CrossRef]
- Dumur, F. Recent advances on carbazole-based photoinitiators of polymerization. Eur. Polym. J. 2020, 125, 109503. [Google Scholar] [CrossRef]
- de Oliveira, D.; Rocha, M.G.; Correa, I.C.; Correr, A.B.; Ferracane, J.L.; Sinhoreti, M.A.C. The effect of combining photoinitiator systems on the color and curing profile of resin-based composites. Dent. Mater. 2016, 32, 1209–1217. [Google Scholar] [CrossRef]
- Schneider, L.F.; Cavalcante, L.M.; Prahl, S.A.; Pfeifer, C.S.; Ferracane, J.L. Curing efficiency of dental resin composites formulated with camphorquinone or trimethylbenzoyl-diphenyl-phosphine oxide. Dent. Mater. 2012, 28, 392–397. [Google Scholar] [CrossRef]
- Duan, H.; Leng, K.; Xu, X.; Li, Q.; Liu, D.; Han, Y.; Gao, J.; Yu, Q.; Wang, Z. Monoacylphosphine oxides with substituents in the phosphonyl moiety as Norrish I photoinitiators: Synthesis, photoinitiattion properties and mechanism. J. Photochem. Photobiol. A Chem. 2021, 421, 113517. [Google Scholar] [CrossRef]
- Manojlovic, D.; Dramicanin, M.D.; Lezaja, M.; Pongprueksa, P.; Van Meerbeek, B.; Miletic, V. Effect of resin and photoinitiator on color, translucency and color stability of conventional and low-shrinkage model composites. Dent. Mater. 2016, 32, 183–191. [Google Scholar] [CrossRef]
- Almeida, S.M.; Meereis, C.T.W.; Leal, F.B.; Carvalho, R.V.; Boeira, P.O.; Chisini, L.A.; Cuevas-Suarez, C.E.; Lima, G.S.; Piva, E. Evaluation of alternative photoinitiator systems in two-step self-etch adhesive systems. Dent. Mater. 2020, 36, e29–e37. [Google Scholar] [CrossRef] [PubMed]
- ISO 10993-17; Biological Evaluation of Medical Devices—Part 17: Toxicological Risk Assessment of Medical Device Constituents. International Organization for Standardization: Geneva, Switzerland, 2023.
- Statement—Suitability of the Photoinitiator TPO in Dentistry; VDDI—German Dental Manufacturers, FIDE—European Dental Industry: Cologne, Germany, 2024.
- ISO 10993-18; Biological Evaluation of Medical Devices–Part 18: Chemical Characterization of Medical Device Materials within a Risk Management Process. International Organization for Standardization: Geneva, Switzerland, 2020.
- Kowalska, A.; Sokolowski, J.; Bociong, K. The Photoinitiators Used in Resin Based Dental Composite—A Review and Future Perspectives. Polymers 2021, 13, 470. [Google Scholar] [CrossRef] [PubMed]
- Eshmawi, Y.T.; Al-Zain, A.O.; Eckert, G.J.; Platt, J.A. Variation in composite degree of conversion and microflexural strength for different curing lights and surface locations. J. Am. Dent. Assoc. 2018, 149, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Fujioka-Kobayashi, M.; Miron, R.J.; Lussi, A.; Gruber, R.; Ilie, N.; Price, R.B.; Schmalz, G. Effect of the degree of conversion of resin-based composites on cytotoxicity, cell attachment, and gene expression. Dent. Mater. 2019, 35, 1173–1193. [Google Scholar] [CrossRef] [PubMed]
- Pongprueksa, P.; Miletic, V.; Janssens, H.; Van Landuyt, K.L.; De Munck, J.; Godderis, L.; Van Meerbeek, B. Degree of conversion and monomer elution of CQ/amine and TPO adhesives. Dent. Mater. 2014, 30, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Randolph, L.D.; Palin, W.M.; Watts, D.C.; Genet, M.; Devaux, J.; Leloup, G.; Leprince, J.G. The effect of ultra-fast photopolymerisation of experimental composites on shrinkage stress, network formation and pulpal temperature rise. Dent. Mater. 2014, 30, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Miletic, V.; Santini, A. Optimizing the concentration of 2,4,6-trimethylbenzoyldiphenylphosphine oxide initiator in composite resins in relation to monomer conversion. Dent. Mater. J. 2012, 31, 717–723. [Google Scholar] [CrossRef]
- AlSheikh, R. Color stability of Lucirin-photo-activated resin composite after immersion in different staining solutions: A spectrophotometric study. Clin. Cosmet. Investig. Dent. 2019, 11, 297–311. [Google Scholar] [CrossRef] [PubMed]
- Arikawa, H.; Takahashi, H.; Kanie, T.; Ban, S. Effect of various visible light photoinitiators on the polymerization and color of light-activated resins. Dent. Mater. 2009, 28, 454–460. [Google Scholar] [CrossRef]
- Popal, M.; Volk, J.; Leyhausen, G.; Geurtsen, W. Cytotoxic and genotoxic potential of the type I photoinitiators BAPO and TPO on human oral keratinocytes and V79 fibroblasts. Dent. Mater. 2018, 34, 1783–1796. [Google Scholar] [CrossRef]
- Stansbury, J.W. Dimethacrylate network formation and polymer property evolution as determined by the selection of monomers and curing conditions. Dent. Mater. 2012, 28, 13–22. [Google Scholar] [CrossRef]
- Fonseca, A.S.; Labruna Moreira, A.D.; de Albuquerque, P.P.; de Menezes, L.R.; Pfeifer, C.S.; Schneider, L.F. Effect of monomer type on the CC degree of conversion, water sorption and solubility, and color stability of model dental composites. Dent. Mater. 2017, 33, 394–401. [Google Scholar] [CrossRef]
- Wulff, J.; Schweikl, H.; Rosentritt, M. Cytotoxicity of printed resin-based splint materials. J. Dent. 2022, 120, 104097. [Google Scholar] [CrossRef]
- Zeng, B.; Cai, Z.; Lalevée, J.; Yang, Q.; Lai, H.; Xiao, P.; Liu, J.; Xing, F. Cytotoxic and cytocompatible comparison among seven photoinitiators-triggered polymers in different tissue cells. Toxicol. In Vitro 2021, 72, 105103. [Google Scholar] [CrossRef]
- Alkhudhairy, F.; Vohra, F.; Naseem, M.; Owais, M.M.; Amer, A.H.B.; Almutairi, K.B. Color stability and degree of conversion of a novel dibenzoyl germanium derivative containing photo-polymerized resin luting cement. J. Appl. Biomater. Funct. Mater. 2020, 18, 2280800020917326. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Khosravani, M.R.; Reinicke, T. On the environmental impacts of 3D printing technology. Appl. Mater. Today 2020, 20, 100689. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| HPLC—Uncured Resins | UPLC—Cured Specimens | ||||
|---|---|---|---|---|---|
| Time [min] | Methanol [%] | Water [%] | Time [min] | Acetonitrile [%] | Water [%] |
| 0 | 70 | 30 | 0 | 30 | 70 |
| 0.5 | 70 | 30 | 0.5 | 30 | 70 |
| 14.5 | 95 | 5 | 6 | 50 | 50 |
| 15 | 70 | 30 | 7 | 50 | 50 |
| 20 | 70 | 30 | 16 | 90 | 10 |
| 17 | 30 | 70 | |||
| 20 | 30 | 70 | |||
| TPO (MSDS) | Printer | Cleaning (IFU) | Post-Curing (IFU) | |
|---|---|---|---|---|
| LuxaPrint Ortho Plus (DMG) | 1–2% | Asiga MAX UV | 2 + 2 min with isopropanol in an ultrasonic bath | 2 × 2000 flashes |
| FREEPRINT splint 2.0 (DETAX) | 1–5% | Asiga MAX UV | 2 + 3 min with isopropanol in an ultrasonic bath | 2 × 2000 flashes |
| optiprint splint (dentona) | <2.5% | Asiga MAX UV | 2 + 3 min with isopropanol in an ultrasonic bath | 2 × 2000 flashes |
| KeySplint Soft (Keystone) | <3% | rapidshape D20 II | 2 + 3 min with isopropanol in an ultrasonic bath | 2 × 2000 flashes |
| FREEPRINT ortho (DETAX) | 1–2.5% | Asiga MAX UV | 5 + 3 min with isopropanol in an ultrasonic bath | 2 × 2000 flashes |
| V-Print splint comfort (VOCO) | 1–5% | Asiga MAX UV | 2 + 3 min with isopropanol in an ultrasonic bath | 2 × 2000 flashes |
| LuxaPrint Ortho Plus (DMG) | FREEPRINT Splint 2.0 (DETAX) | Optiprint Splint (Dentona) | KeySplint Soft (Keystone) | FREEPRINT Ortho (DETAX) | V-Print Splint Comfort (VOCO) | |
|---|---|---|---|---|---|---|
| Liquid resin TPO [%] | 1.04 | 1.47 | 1.18 | 1.19 | 1.19 | 1.00 |
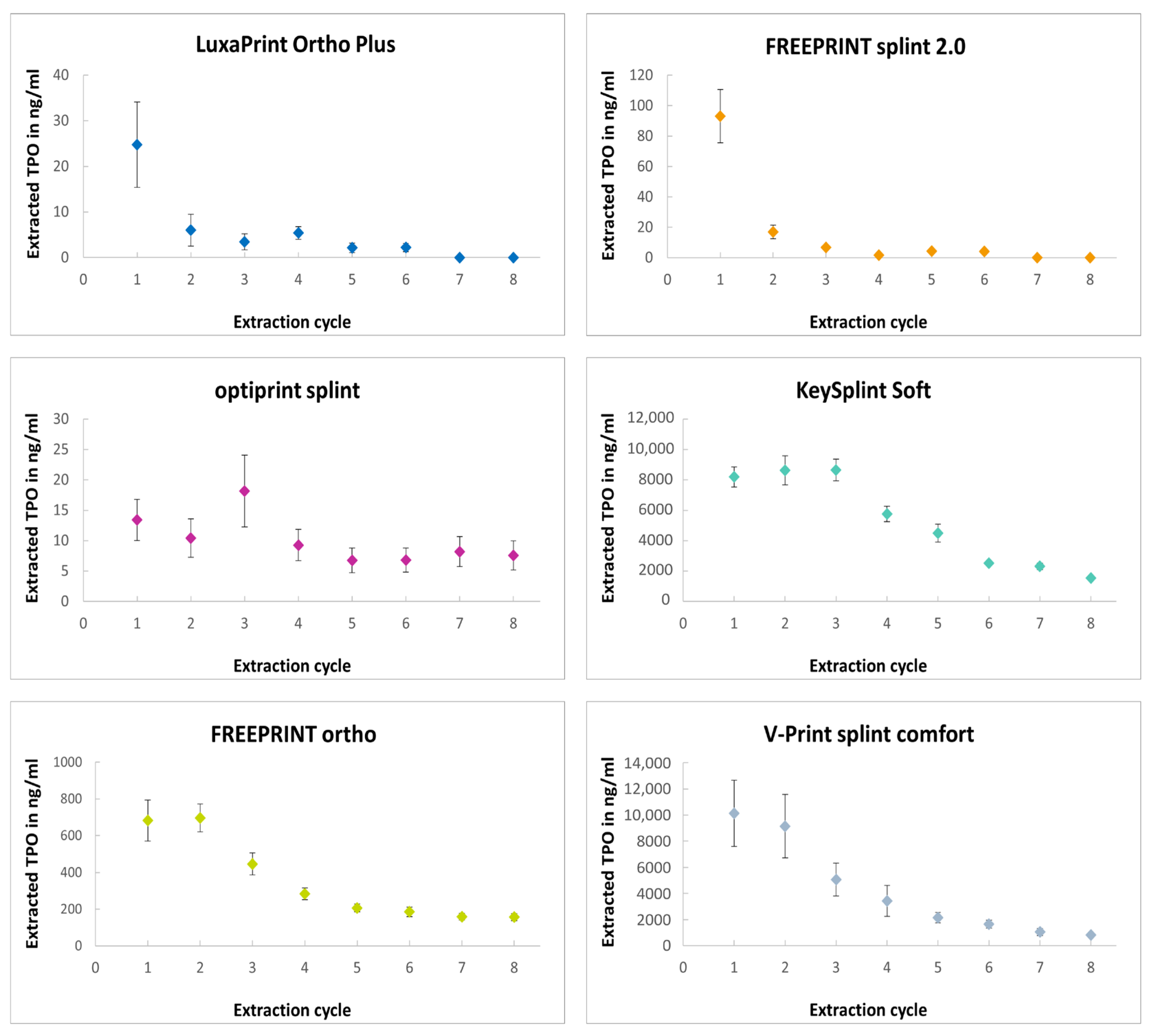
| Total TPO, 8 × 72 h [ng/mL] | 44.0 ± 17.1 a | 127.4 ± 25.3 ab | 80.6 ± 21.1 ab | 42,083.5 ± 3175.2 c | 2813.2 ± 348.0 bc | 33,424.6 ± 8357.9 c |
| Maximum TPO, 72 h [ng/mL] | 24.8 ± 9.4 a | 93.2 ± 17.5 ab | 18.1 ± 5.9 ab | 8640.4 ± 714.1 c | 696.0 ± 76.3 bc | 10,135.2 ± 2542.2 c |
| Maximum TPO, 24 h [ng/mL] | 8.3 ± 3.1 | 31.1 ± 5.8 | 6.0 ± 2.0 | 2880.1 ± 283.0 | 232.0 ± 25.4 | 3378.4 ± 847.4 |
| Daily exposition, 10 kg bw [µg/kg bw/d] | 0.025 ± 0.009 | 0.093 ± 0.017 | 0.018 ± 0.006 | 8.640 ± 0.849 | 0.696 ± 0.076 | 10.135 ± 2.542 |
| Margin of Safety (MoS) | 1115 > 1 | 299 > 1 | 1543 > 1 | 3 > 1 | 40 > 1 | 3 > 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Messer-Hannemann, P.; Wienhold, M.; Esbak, H.; Brunner, A.; Schönebaum, A.; Schwendicke, F.; Effenberger, S. Residual TPO Content of Photopolymerized Additively Manufactured Dental Occlusal Splint Materials. Biomedicines 2025, 13, 44. https://doi.org/10.3390/biomedicines13010044
Messer-Hannemann P, Wienhold M, Esbak H, Brunner A, Schönebaum A, Schwendicke F, Effenberger S. Residual TPO Content of Photopolymerized Additively Manufactured Dental Occlusal Splint Materials. Biomedicines. 2025; 13(1):44. https://doi.org/10.3390/biomedicines13010044
Chicago/Turabian StyleMesser-Hannemann, Philipp, Max Wienhold, Hoda Esbak, Alexander Brunner, Andreas Schönebaum, Falk Schwendicke, and Susanne Effenberger. 2025. "Residual TPO Content of Photopolymerized Additively Manufactured Dental Occlusal Splint Materials" Biomedicines 13, no. 1: 44. https://doi.org/10.3390/biomedicines13010044
APA StyleMesser-Hannemann, P., Wienhold, M., Esbak, H., Brunner, A., Schönebaum, A., Schwendicke, F., & Effenberger, S. (2025). Residual TPO Content of Photopolymerized Additively Manufactured Dental Occlusal Splint Materials. Biomedicines, 13(1), 44. https://doi.org/10.3390/biomedicines13010044