
Evaluation of Inflammatory Markers and Clinical Outcomes in COVID-19 Patients with Concurrent Clostridioides difficile Infection: A Comparative Cohort Analysis
 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection and Laboratory Measurements
2.3. Inflammatory Indices and Clinical Definitions
2.4. Statistical Analysis
3. Results
Patient Demographics
4. Discussion
4.1. Analysis of Findings
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19) [Updated 2023 Aug 18]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554776/ (accessed on 13 November 2024).
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bai, Y.; Ning, K. How does severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) achieve immune evasion?: A narrative review. Medicine 2024, 103, e37780. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bilasy, S.E.; Wahyuni, T.S.; Ibrahim, M.; El-Shamy, A. What SARS-CoV-2 Variants Have Taught Us: Evolutionary Challenges of RNA Viruses. Viruses 2024, 16, 139. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Machkovech, H.M.; Hahn, A.M.; Garonzik Wang, J.; Grubaugh, N.D.; Halfmann, P.J.; Johnson, M.C.; Lemieux, J.E.; O’Connor, D.H.; Piantadosi, A.; Wei, W.; et al. Persistent SARS-CoV-2 infection: Significance and implications. Lancet Infect Dis. 2024, 24, e453–e462. [Google Scholar] [CrossRef] [PubMed]
- Ghafari, M.; Hall, M.; Golubchik, T.; Ayoubkhani, D.; House, T.; MacIntyre-Cockett, G.; Fryer, H.R.; Thomson, L.; Nurtay, A.; Kemp, S.A.; et al. Prevalence of persistent SARS-CoV-2 in a large community surveillance study. Nature 2024, 626, 1094–1101. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gawey, B.J.; Khanna, S. Clostridioides difficile Infection: Landscape and Microbiome Therapeutics. Gastroenterol. Hepatol. (N. Y.) 2023, 19, 319–328. [Google Scholar] [PubMed] [PubMed Central]
- Sehgal, K.; Khanna, S. Gut microbiome and Clostridioides difficile infection: A closer look at the microscopic interface. Therap. Adv. Gastroenterol. 2021, 14, 1756284821994736. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Buddle, J.E.; Fagan, R.P. Pathogenicity and virulence of Clostridioides difficile. Virulence 2023, 14, 2150452. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Reveles, K.R.; Frei, A.L.; Strey, K.A.; Young, E.H. Prevalence and Health Outcomes of Clostridioides difficile Infection During the Coronavirus Disease 2019 Pandemic in a National Sample of United States Hospital Systems. Open Forum Infect Dis. 2022, 9, ofac441. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deda, X.; Elfert, K.; Gandhi, M.; Malik, A.; Elromisy, E.; Guevara, N.; Nayudu, S.; Bechtold, M. Clostridioides difficile Infection in COVID-19 Hospitalized Patients: A Nationwide Analysis. Gastroenterol. Res. 2023, 16, 234–239. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Webb, B.J.; Subramanian, A.; Lopansri, B.; Goodman, B.; Jones, P.B.; Ferraro, J.; Stenehjem, E.; Brown, S.M. Antibiotic Exposure and Risk for Hospital-Associated Clostridioides difficile Infection. Antimicrob. Agents Chemother. 2020, 64, e02169-19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gupta, A.; Khanna, S. Community-acquired Clostridium difficile infection: An increasing public health threat. Infect Drug Resist. 2014, 7, 63–72. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Azimirad, M.; Noori, M.; Raeisi, H.; Yadegar, A.; Shahrokh, S.; Asadzadeh Aghdaei, H.; Bentivegna, E.; Martelletti, P.; Petrosillo, N.; Zali, M.R. How Does COVID-19 Pandemic Impact on Incidence of Clostridioides difficile Infection and Exacerbation of Its Gastrointestinal Symptoms? Front. Med. 2021, 8, 775063. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Silva, M.J.A.; Ribeiro, L.R.; Gouveia, M.I.M.; Marcelino, B.D.R.; Santos, C.S.D.; Lima, K.V.B.; Lima, L.N.G.C. Hyperinflammatory Response in COVID-19: A Systematic Review. Viruses 2023, 15, 553. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mehta, P.; Fajgenbaum, D.C. Is severe COVID-19 a cytokine storm syndrome: A hyperinflammatory debate. Curr. Opin. Rheumatol. 2021, 33, 419–430. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Madan, R.; Petri, W.A., Jr. Immune responses to Clostridium difficile infection. Trends Mol. Med. 2012, 18, 658–666. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Solomon, K. The host immune response to Clostridium difficile infection. Ther. Adv. Infect. Dis. 2013, 1, 19–35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wu, Z.; Cao, Y.; Liu, Z.; Geng, N.; Pan, W.; Zhu, Y.; Shi, H.; Song, Q.; Liu, B.; Ma, Y. Study on the predictive value of laboratory inflammatory markers and blood count-derived inflammatory markers for disease severity and prognosis in COVID-19 patients: A study conducted at a university-affiliated infectious disease hospital. Ann. Med. 2024, 56, 2415401. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Açıksarı, G.; Koçak, M.; Çağ, Y.; Altunal, L.N.; Atıcı, A.; Çelik, F.B.; Bölen, F.; Açıksarı, K.; Çalışkan, M. Prognostic Value of Inflammatory Biomarkers in Patients with Severe COVID-19: A Single-Center Retrospective Study. Biomark. Insights 2021, 16, 11772719211027022. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abrishami, A.; Eslami, V.; Arab-Ahmadi, M.; Alahyari, S.; Azhideh, A.; Sanei-Taheri, M. Prognostic value of inflammatory biomarkers for predicting the extent of lung involvement and final clinical outcome in patients with COVID-19. J. Res. Med. Sci. 2021, 26, 115. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Del Sole, F.; Farcomeni, A.; Loffredo, L.; Carnevale, R.; Menichelli, D.; Vicario, T.; Pignatelli, P.; Pastori, D. Features of severe COVID-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 50, e13378. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yakout, A.; Bi, Y.; Harris, D.M. Clostridioides difficile: A Concise Review of Best Practices and Updates. J. Prim Care Community Health 2024, 15, 21501319241249645. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stoian, M.; Andone, A.; Boeriu, A.; Bândilă, S.R.; Dobru, D.; Laszlo, S.Ș.; Corău, D.; Arbănași, E.M.; Russu, E.; Stoian, A. COVID-19 and Clostridioides difficile Coinfection Analysis in the Intensive Care Unit. Antibiotics 2024, 13, 367. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zouridis, S.; Sangha, M.; Feustel, P.; Richter, S. Clostridium difficile Infection Rates During the Pandemic in New York Capital Area: A Single-Center Study. Cureus 2023, 15, e37576. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maslennikov, R.; Ivashkin, V.; Ufimtseva, A.; Poluektova, E.; Ulyanin, A. Clostridioides difficile co-infection in patients with COVID-19. Future Microbiol. 2022, 17, 653–663. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Awan, R.U.; Gangu, K.; Nguyen, A.; Chourasia, P.; Borja Montes, O.F.; Butt, M.A.; Muzammil, T.S.; Afzal, R.M.; Nabeel, A.; Shekhar, R.; et al. COVID-19 and Clostridioides difficile Coinfection Outcomes among Hospitalized Patients in the United States: An Insight from National Inpatient Database. Infect Dis. Rep. 2023, 15, 279–291. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Merchante, N.; Chico, P.; Márquez-Saavedra, E.; Riera, G.; Herrero, R.; González-de-la-Aleja, P.; Aller, A.I.; Rodríguez, J.C.; Rodríguez-Fernández, M.; Ramos, J.M.; et al. Impact of COVID19 pandemic on the incidence of health-care associated Clostridioides difficile infection. Anaerobe 2022, 75, 102579. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Manea, E.; Jipa, R.; Milea, A.; Roman, A.; Neagu, G.; Hristea, A. Healthcare-associated Clostridioides difficile infection during the COVID-19 pandemic in a tertiary care hospital in Romania. Rom. J. Intern Med. 2021, 59, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Karampatakis, T.; Tsergouli, K.; Kandilioti, E.; Nikopoulou, A.; Katsifa, H.; Kachrimanidou, M. Implication of COVID-19 pandemic on the incidence of Clostridioides difficile infection in a Greek tertiary hospital. J. Med. Microbiol. 2023, 72, 001689. [Google Scholar] [CrossRef] [PubMed]
- Maldonado-Barrueco, A.; Moreno-Ramos, F.; Díaz-Pollán, B.; Loeches-Yagüe, B.; Rico-Nieto, A.; García-Rodríguez, J.; Ruiz-Carrascoso, G. Increase of healthcare-onset Clostridioides difficile infection in adult population since SARS-CoV-2 pandemic: A retrospective cohort study in a tertiary care hospital from 2019 to 2022. Anaerobe 2024, 86, 102836. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | COVID + CDI (n = 92) | COVID-Only (n = 108) | p-Value |
|---|---|---|---|
| Age (years) | 67.3 ± 13.1 | 64.9 ± 11.9 | 0.18 |
| Male Gender (%) | 58.7% | 54.6% | 0.53 |
| BMI (kg/m2) | 28.4 ± 4.9 | 27.2 ± 4.5 | 0.07 |
| Hypertension (%) | 76.1% | 64.8% | 0.09 |
| Diabetes Mellitus (%) | 51.1% | 39.8% | 0.1 |
| Chronic Kidney Disease (%) | 29.3% | 18.5% | 0.08 |
| ICU Admission (%) | 39.1% | 22.2% | 0.01 |
| Mechanical Ventilation (%) | 26.1% | 12.0% | 0.008 |
| In-hospital Mortality (%) | 23.9% | 11.1% | 0.01 |
| Vaccine Status (fully vaccinated) | 43, (46.74%) | 68, (62.96%) | 0.03 |
| Use of Antivirals | 68, (73.91%) | 77, (71.30%) | 0.69 |
| Use of Systemic Anti-inflammation Agents | 36, (39.13%) | 33, (30.56%) | 0.16 |
| Marker | COVID + CDI (n = 92) | COVID-Only (n = 108) | p-Value |
|---|---|---|---|
| CRP (mg/L) | 87.4 ± 27.8 | 68.9 ± 23.1 | <0.001 |
| IL-6 (pg/mL) | 62.1 ± 19.4 | 48.7 ± 15.6 | <0.001 |
| Ferritin (µg/L) | 524 ± 145 | 420 ± 132 | 0.002 |
| NLR | 7.6 ± 2.5 | 5.9 ± 2.0 | <0.001 |
| Albumin (g/L) | 30.4 ± 5.2 | 33.8 ± 5.7 | <0.001 |
| Platelet (×10⁹/L) | 205 ± 58 | 228 ± 61 | 0.004 |
| CAR | 2.90 ± 0.83 | 2.05 ± 0.69 | <0.001 |
| PNI | 34.1 ± 4.8 | 38.7 ± 5.3 | <0.001 |
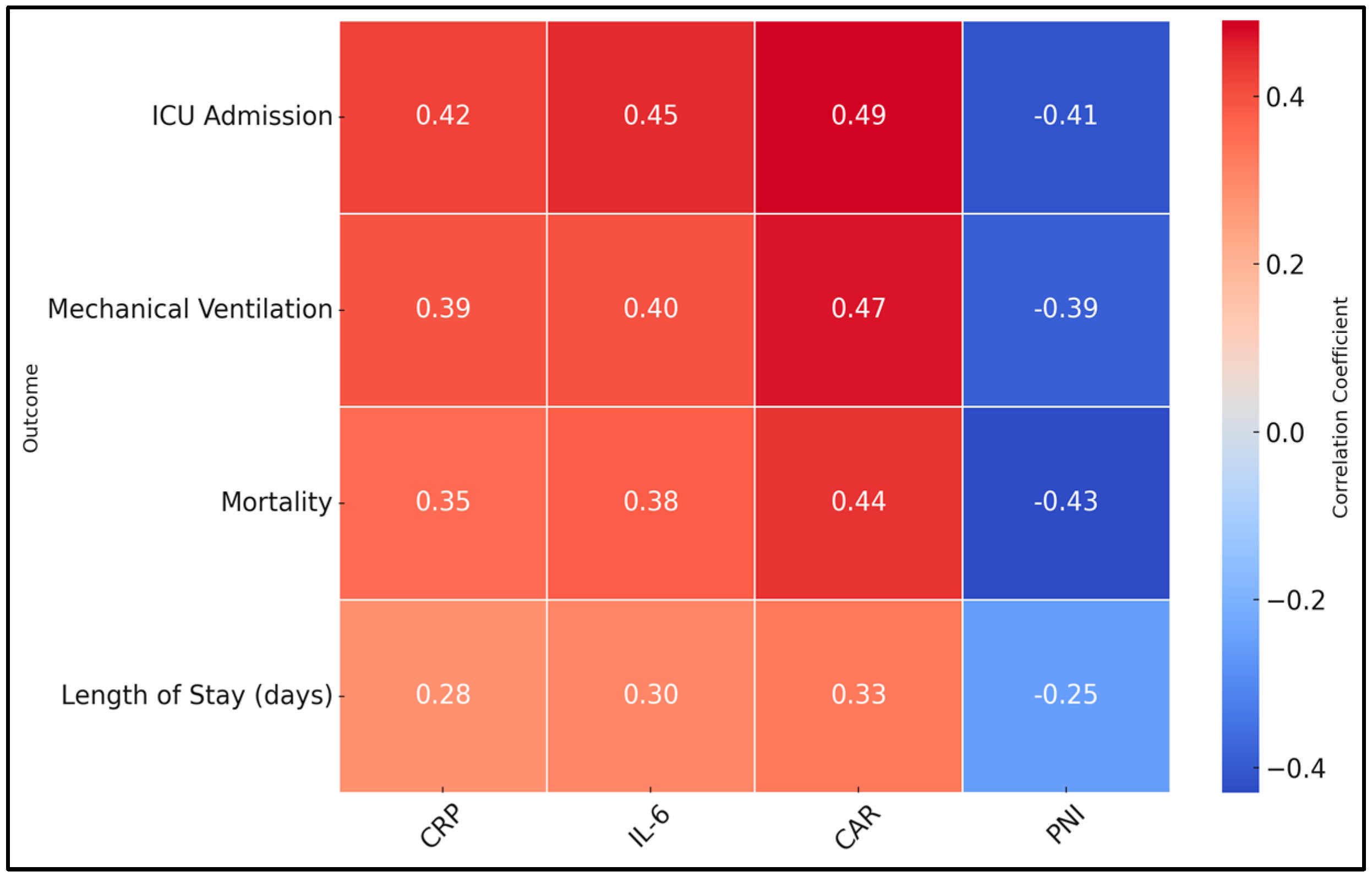
| Outcome | r (CRP) | p-Value | r (IL-6) | p-Value | r (CAR) | p-Value | r (PNI) | p-Value |
|---|---|---|---|---|---|---|---|---|
| ICU Admission | 0.42 | <0.001 | 0.45 | <0.001 | 0.49 | <0.001 | −0.41 | <0.001 |
| Mechanical Ventilation | 0.39 | <0.001 | 0.4 | <0.001 | 0.47 | <0.001 | −0.39 | <0.001 |
| Mortality | 0.35 | <0.001 | 0.38 | <0.001 | 0.44 | <0.001 | −0.43 | <0.001 |
| Length of Stay (days) | 0.28 | 0.003 | 0.3 | 0.002 | 0.33 | 0.001 | −0.25 | 0.008 |
| Variable | Severe (n = 36) * | Non-Severe (n = 56) | p-Value |
|---|---|---|---|
| CRP (mg/L) | 94.1 ± 28.9 | 82.3 ± 25.7 | 0.04 |
| IL-6 (pg/mL) | 67.0 ± 20.5 | 58.9 ± 18.4 | 0.03 |
| CAR | 3.10 ± 0.81 | 2.77 ± 0.84 | 0.04 |
| PNI | 32.9 ± 4.5 | 35.0 ± 4.8 | 0.03 |
| Mortality (%) | 38.90% | 14.30% | 0.007 |
| Length of Stay (days) | 18.5 ± 6.4 | 13.9 ± 5.2 | 0.001 |
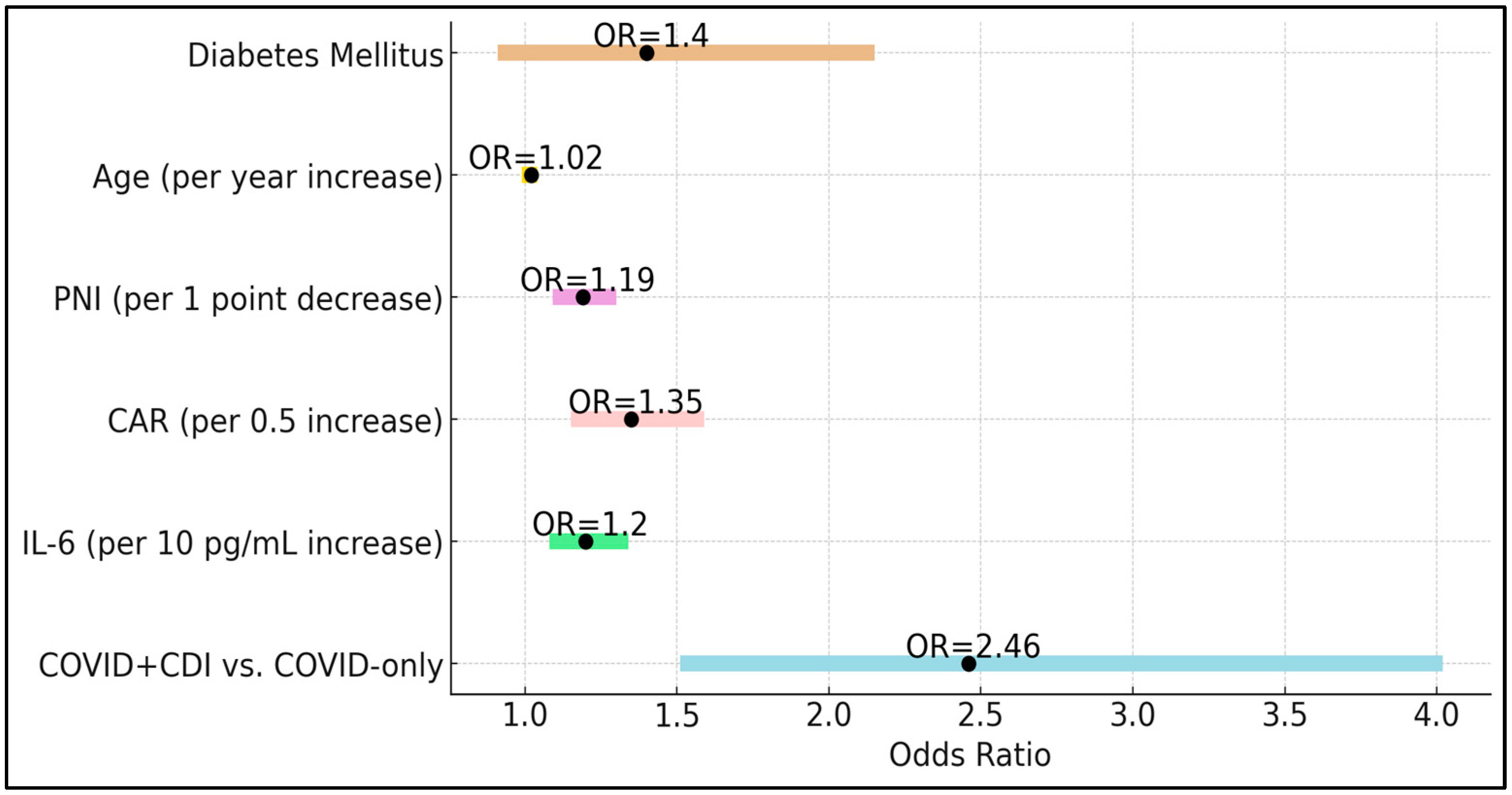
| Variables | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| COVID + CDI vs. COVID-only | 2.46 | 1.51–4.02 | <0.001 |
| IL-6 (per 10 pg/mL increase) | 1.2 | 1.08–1.34 | 0.001 |
| CAR (per 0.5 increase) | 1.35 | 1.15–1.59 | <0.001 |
| PNI (per 1-point decrease) | 1.19 | 1.09–1.30 | <0.001 |
| Age (per year increase) | 1.02 | 0.99–1.04 | 0.2 |
| Diabetes Mellitus | 1.4 | 0.91–2.15 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ignuta, F.; Vlad, A.; Cerbulescu, T.; Loredana, S.; Bratosin, F.; Rosca, O.; Stelea, L.; Nistor, D. Evaluation of Inflammatory Markers and Clinical Outcomes in COVID-19 Patients with Concurrent Clostridioides difficile Infection: A Comparative Cohort Analysis. Biomedicines 2025, 13, 111. https://doi.org/10.3390/biomedicines13010111
Ignuta F, Vlad A, Cerbulescu T, Loredana S, Bratosin F, Rosca O, Stelea L, Nistor D. Evaluation of Inflammatory Markers and Clinical Outcomes in COVID-19 Patients with Concurrent Clostridioides difficile Infection: A Comparative Cohort Analysis. Biomedicines. 2025; 13(1):111. https://doi.org/10.3390/biomedicines13010111
Chicago/Turabian StyleIgnuta, Flavia, Adrian Vlad, Teodor Cerbulescu, Stana Loredana, Felix Bratosin, Ovidiu Rosca, Lavinia Stelea, and Daciana Nistor. 2025. "Evaluation of Inflammatory Markers and Clinical Outcomes in COVID-19 Patients with Concurrent Clostridioides difficile Infection: A Comparative Cohort Analysis" Biomedicines 13, no. 1: 111. https://doi.org/10.3390/biomedicines13010111
APA StyleIgnuta, F., Vlad, A., Cerbulescu, T., Loredana, S., Bratosin, F., Rosca, O., Stelea, L., & Nistor, D. (2025). Evaluation of Inflammatory Markers and Clinical Outcomes in COVID-19 Patients with Concurrent Clostridioides difficile Infection: A Comparative Cohort Analysis. Biomedicines, 13(1), 111. https://doi.org/10.3390/biomedicines13010111