
Pancreatic and Hepatic Injury in COVID-19: A Worse Prognosis in NAFLD Patients?

 , ,
, ,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Pancreatic Injury in COVID-19
2.1. Epidemiological Evidence of Pancreatic Injury
2.2. SARS-CoV-2 Infection and Endocrine Pancreas: A New Cause of Diabetes Mellitus?
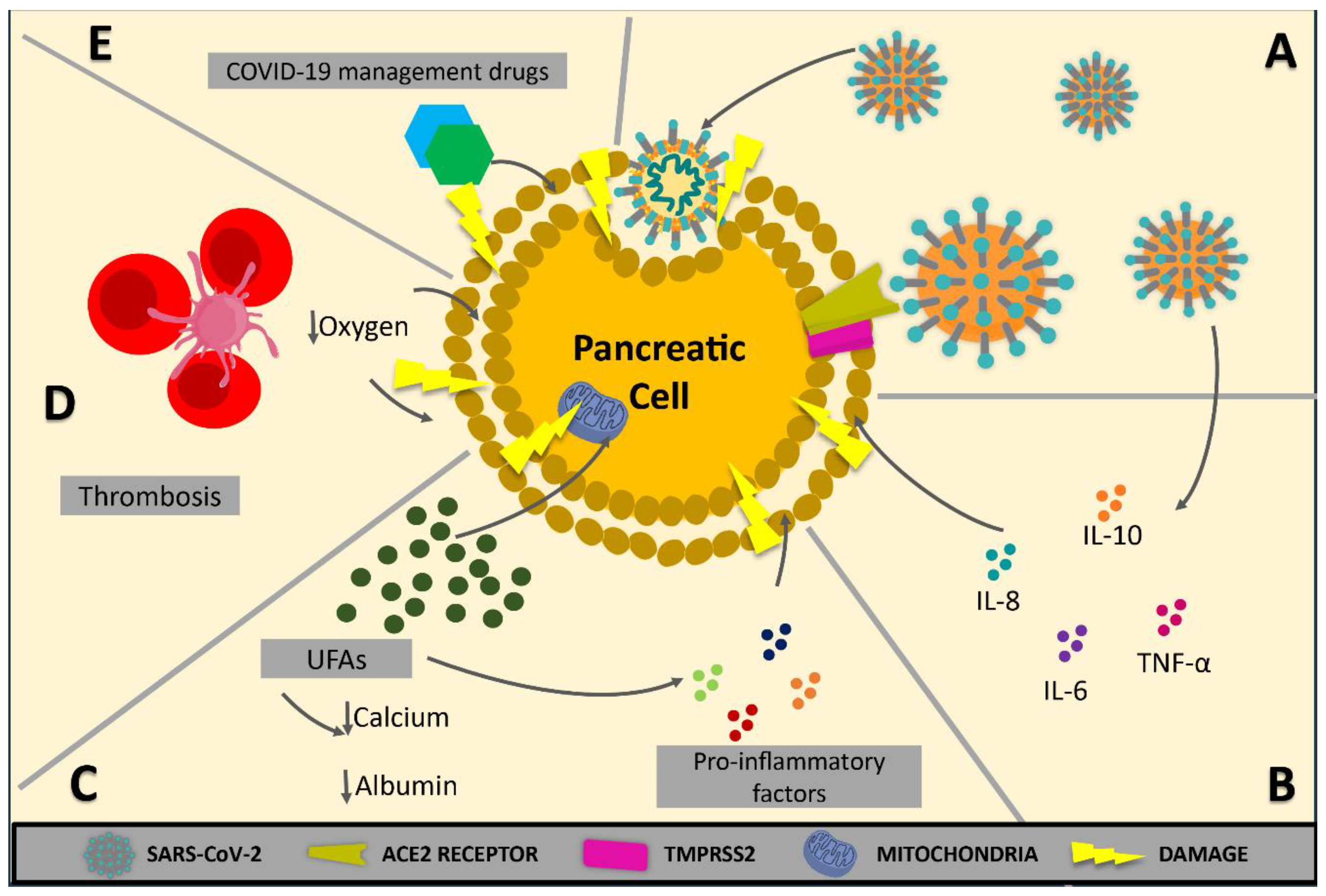
2.3. Pathophysiological Mechanisms
3. Hepatic Injury in COVID-19
3.1. Epidemiological Evidence of Hepatic Injury
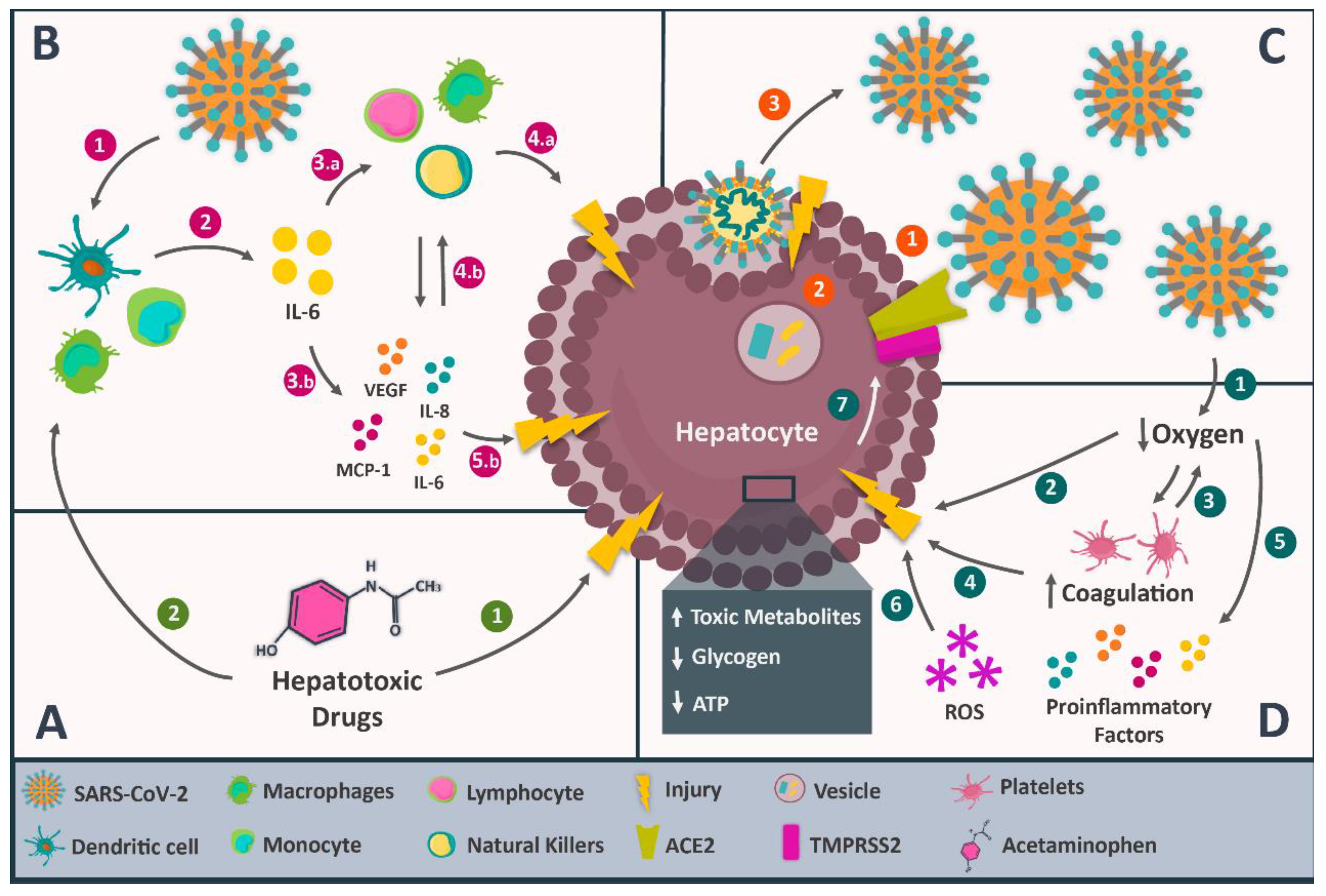
3.2. Pathophysiological Mechanisms
3.2.1. Direct Viral Damage
3.2.2. Dysregulation of the Immune Response
3.2.3. Hypoxic and Ischemic Liver Injury
3.2.4. Drug-Induced Liver Injury during the Treatment of COVID-19
4. Hepatic Injury in COVID-19 Patients with Pre-Existing NAFLD/NASH
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jones, D.L.; Baluja, M.Q.; Graham, D.W.; Corbishley, A.; McDonald, J.E.; Malham, S.K.; Hillary, L.S.; Connor, T.R.; Gaze, W.H.; Moura, I.B.; et al. Shedding of SARS-CoV-2 in Feces and Urine and Its Potential Role in Person-to-Person Transmission and the Environment-Based Spread of COVID-19. Sci. Total Environ. 2020, 749, 141364. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Kumar, P.; Tevethia, H.V.; Premkumar, M.; Arab, J.P.; Candia, R.; Talukdar, R.; Sharma, M.; Qi, X.; Rao, P.N.; et al. Systematic Review with Meta-Analysis: Liver Manifestations and Outcomes in COVID-19. Aliment. Pharmacol. Ther. 2020, 52, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Lagana, S.M.; Kudose, S.; Iuga, A.C.; Lee, M.J.; Fazlollahi, L.; Remotti, H.E.; Del Portillo, A.; De Michele, S.; de Gonzalez, A.K.; Saqi, A.; et al. Hepatic Pathology in Patients Dying of COVID-19: A Series of 40 Cases Including Clinical, Histologic, and Virologic Data. Mod. Pathol. 2020, 33, 2147–2155. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.A.; Schattenberg, J.M. Liver Injury in COVID-19: The Current Evidence. United Eur. Gastroenterol. J. 2020, 8, 509–519. [Google Scholar] [CrossRef] [PubMed]
- de-Madaria, E.; Capurso, G. COVID-19 and Acute Pancreatitis: Examining the Causality. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 3–4. [Google Scholar] [CrossRef]
- Huang, R.; Zhu, L.; Wang, J.; Xue, L.; Liu, L.; Yan, X.; Huang, S.; Li, Y.; Yan, X.; Zhang, B.; et al. Clinical Features of Patients With COVID-19 With Nonalcoholic Fatty Liver Disease. Hepatol. Commun. 2020, 4, 1758–1768. [Google Scholar] [CrossRef]
- Steenblock, C.; Schwarz, P.E.H.; Ludwig, B.; Linkermann, A.; Zimmet, P.; Kulebyakin, K.; Tkachuk, V.A.; Markov, A.G.; Lehnert, H.; de Angelis, M.H.; et al. COVID-19 and Metabolic Disease: Mechanisms and Clinical Management. Lancet Diabetes Endocrinol. 2021, 9, 786–798. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.E.; Wong, V.W.-S.; Rinella, M. Non-Alcoholic Fatty Liver Disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD Development and Therapeutic Strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef]
- Kumar-M, P.; Mishra, S.; Jha, D.K.; Shukla, J.; Choudhury, A.; Mohindra, R.; Mandavdhare, H.S.; Dutta, U.; Sharma, V. Coronavirus Disease (COVID-19) and the Liver: A Comprehensive Systematic Review and Meta-Analysis. Hepatol. Int. 2020, 14, 711–722. [Google Scholar] [CrossRef]
- Lei, F.; Liu, Y.-M.; Zhou, F.; Qin, J.-J.; Zhang, P.; Zhu, L.; Zhang, X.-J.; Cai, J.; Lin, L.; Ouyang, S.; et al. Longitudinal Association Between Markers of Liver Injury and Mortality in COVID-19 in China. Hepatology 2020, 72, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 Expression in Pancreas May Cause Pancreatic Damage After SARS-CoV-2 Infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients With Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Bruno, G.; Fabrizio, C.; Santoro, C.R.; Buccoliero, G.B. Pancreatic Injury in the Course of Coronavirus Disease 2019: A Not-so-Rare Occurrence. J. Med. Virol. 2021, 93, 74–75. [Google Scholar] [CrossRef] [PubMed]
- Kataria, S.; Sharif, A.; Ur Rehman, A.; Ahmed, Z.; Hanan, A. COVID-19 Induced Acute Pancreatitis: A Case Report and Literature Review. Cureus 2020, 12, e9169. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.M.; Yvamoto, E.Y.; Marzinotto, M.A.N.; de Sá Teixeira, A.C.; Carrilho, F.J. SARS-CoV-2 Leading to Acute Pancreatitis: An Unusual Presentation. Braz. J. Infect. Dis. 2020, 24, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Kumaran, N.K.; Karmakar, B.K.; Taylor, O.M. Coronavirus Disease-19 (COVID-19) Associated with Acute Necrotising Pancreatitis (ANP). BMJ Case Rep. 2020, 13, e237903. [Google Scholar] [CrossRef]
- Rabice, S.R.; Altshuler, P.C.; Bovet, C.; Sullivan, C.; Gagnon, A.J. COVID-19 Infection Presenting as Pancreatitis in a Pregnant Woman: A Case Report. Case Rep. Womens Health 2020, 27, e00228. [Google Scholar] [CrossRef]
- Cerda-Contreras, C.; Nuzzolo-Shihadeh, L.; Camacho-Ortiz, A.; Perez-Alba, E. Baricitinib as Treatment for COVID-19: Friend or Foe of the Pancreas? Clin. Infect. Dis. 2020, 73, e3977–e3978. [Google Scholar] [CrossRef]
- Akarsu, C.; Karabulut, M.; Aydin, H.; Sahbaz, N.A.; Dural, A.C.; Yegul, D.; Peker, K.D.; Ferahman, S.; Bulut, S.; Dönmez, T.; et al. Association between Acute Pancreatitis and COVID-19: Could Pancreatitis Be the Missing Piece of the Puzzle about Increased Mortality Rates? J. Investig. Surg. 2020, 35, 119–125. [Google Scholar] [CrossRef]
- Juhász, M.F.; Ocskay, K.; Kiss, S.; Hegyi, P.; Párniczky, A. Insufficient Etiological Workup of COVID-19-Associated Acute Pancreatitis: A Systematic Review. World J. Gastroenterol. 2020, 26, 6270–6278. [Google Scholar] [CrossRef] [PubMed]
- McNabb-Baltar, J.; Jin, D.X.; Grover, A.S.; Redd, W.D.; Zhou, J.C.; Hathorn, K.E.; McCarty, T.R.; Bazarbashi, A.N.; Shen, L.; Chan, W.W. Lipase Elevation in Patients With COVID-19. Am. J. Gastroenterol. 2020, 115, 1286–1288. [Google Scholar] [CrossRef] [PubMed]
- Barlass, U.; Wiliams, B.; Dhana, K.; Adnan, D.; Khan, S.R.; Mahdavinia, M.; Bishehsari, F. Marked Elevation of Lipase in COVID-19 Disease: A Cohort Study. Clin. Transl. Gastroenterol. 2020, 11, e00215. [Google Scholar] [CrossRef] [PubMed]
- Rasch, S.; Herner, A.; Schmid, R.M.; Huber, W.; Lahmer, T. High Lipasemia Is Frequent in COVID-19 Associated Acute Respiratory Distress Syndrome. Pancreatology 2021, 21, 306–311. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, P.; Wang, M.; Wang, J.; Chen, J.; Yuan, W.; Li, M.; Xie, Z.; Dong, W.; Li, H.; et al. The Clinical Data from 19 Critically Ill Patients with Coronavirus Disease 2019: A Single-Centered, Retrospective, Observational Study. J. Public Health 2020, 30, 361–364. [Google Scholar] [CrossRef]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Acute Pancreatitis Classification Working Group Classification of Acute Pancreatitis—2012: Revision of the Atlanta Classification and Definitions by International Consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef]
- Jayanta, S.; Gupta, R.; Singh, M.P.; Patnaik, I.; Kumar, A.; Kochhar, R. Coronavirus Disease 2019 and the Pancreas. Pancreatology 2020, 20, 1567–1575. [Google Scholar] [CrossRef]
- Yang, J.K.; Feng, Y.; Yuan, M.Y.; Yuan, S.Y.; Fu, H.J.; Wu, B.Y.; Sun, G.Z.; Yang, G.R.; Zhang, X.L.; Wang, L.; et al. Plasma Glucose Levels and Diabetes Are Independent Predictors for Mortality and Morbidity in Patients with SARS. Diabet. Med. 2006, 23, 623–628. [Google Scholar] [CrossRef]
- Gentile, S.; Strollo, F.; Mambro, A.; Ceriello, A. COVID-19, Ketoacidosis and New-Onset Diabetes: Are There Possible Cause and Effect Relationships among Them? Diabetes Obes. Metab. 2020, 22, 2507–2508. [Google Scholar] [CrossRef]
- Rubino, F.; Amiel, S.A.; Zimmet, P.; Alberti, G.; Bornstein, S.; Eckel, R.H.; Mingrone, G.; Boehm, B.; Cooper, M.E.; Chai, Z.; et al. New-Onset Diabetes in COVID-19. N. Engl. J. Med. 2020, 383, 789–790. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Rubino, F.; Khunti, K.; Mingrone, G.; Hopkins, D.; Birkenfeld, A.L.; Boehm, B.; Amiel, S.; Holt, R.I.; Skyler, J.S.; et al. Practical Recommendations for the Management of Diabetes in Patients with COVID-19. Lancet Diabetes Endocrinol. 2020, 8, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in People with Diabetes: Understanding the Reasons for Worse Outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Madan, K.; Mohan, A.; Tiwari, P.; Hadda, V. Diabetes in COVID-19: Steroid Effect. J. Med. Virol. 2021, 93, 4166. [Google Scholar] [CrossRef] [PubMed]
- Sosale, A.; Sosale, B.; Kesavadev, J.; Chawla, M.; Reddy, S.; Saboo, B.; Misra, A. Steroid Use during COVID-19 Infection and Hyperglycemia—What a Physician Should Know. Diabetes Metab. Syndr. 2021, 15, 102167. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.L.; Weiss, R.E. Steroid-induced Diabetes: A Clinical and Molecular Approach to Understanding and Treatment. Diabetes Metab. Res. 2014, 30, 96–102. [Google Scholar] [CrossRef]
- Cheung, N.W. Steroid-Induced Hyperglycaemia in Hospitalised Patients: Does It Matter? Diabetologia 2016, 59, 2507–2509. [Google Scholar] [CrossRef] [PubMed]
- Keerthi, B.Y.; Sushmita, G.; Khan, E.A.; Thomas, V.; Cheryala, V.; Shah, C.; Kumar, G.R.; Haritha, V. New Onset Diabetes Mellitus in Post-COVID-19 Patients. J. Fam. Med. Prim. Care 2022, 11, 5961–5968. [Google Scholar] [CrossRef]
- Sathish, T.; Kapoor, N.; Cao, Y.; Tapp, R.J.; Zimmet, P. Proportion of Newly Diagnosed Diabetes in COVID-19 Patients: A Systematic Review and Meta-Analysis. Diabetes Obes. Metab. 2021, 23, 870–874. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue Distribution of ACE2 Protein, the Functional Receptor for SARS Coronavirus. A First Step in Understanding SARS Pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of Angiotensin-Converting Enzyme 2 (ACE2) in COVID-19. Crit. Care 2020, 24, 422. [Google Scholar] [CrossRef] [PubMed]
- Abramczyk, U.; Nowaczyński, M.; Słomczyński, A.; Wojnicz, P.; Zatyka, P.; Kuzan, A. Consequences of COVID-19 for the Pancreas. Int. J. Mol. Sci. 2022, 23, 864. [Google Scholar] [CrossRef]
- Cure, E.; Cumhur Cure, M. COVID-19 May Affect the Endocrine Pancreas by Activating Na+/H+ Exchanger 2 and Increasing Lactate Levels. J. Endocrinol. Investig. 2020, 43, 1167–1168. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-K.; Lin, S.-S.; Ji, X.-J.; Guo, L.-M. Binding of SARS Coronavirus to Its Receptor Damages Islets and Causes Acute Diabetes. Acta Diabetol. 2010, 47, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Muus, C.; Luecken, M.D.; Eraslan, G.; Waghray, A.; Heimberg, G.; Sikkema, L.; Kobayashi, Y.; Vaishnav, E.D.; Subramanian, A.; Smilie, C.; et al. Integrated Analyses of Single-Cell Atlases Reveal Age, Gender, and Smoking Status Associations with Cell Type-Specific Expression of Mediators of SARS-CoV-2 Viral Entry and Highlights Inflammatory Programs in Putative Target. biorXiv 2020. [Google Scholar] [CrossRef]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ Distribution of Severe Acute Respiratory Syndrome (SARS) Associated Coronavirus (SARS-CoV) in SARS Patients: Implications for Pathogenesis and Virus Transmission Pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical Predictors of Mortality Due to COVID-19 Based on an Analysis of Data of 150 Patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, Clinical Course, and Outcomes of Critically Ill Adults with COVID-19 in New York City: A Prospective Cohort Study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Hegyi, P.; Szakács, Z.; Sahin-Tóth, M. Lipotoxicity and Cytokine Storm in Severe Acute Pancreatitis and COVID-19. Gastroenterology 2020, 159, 824–827. [Google Scholar] [CrossRef]
- Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 Induces Cytokine Storm with High Mortality. Inflamm. Regen. 2020, 40, 37. [Google Scholar] [CrossRef]
- de Oliveira, C.; Khatua, B.; Noel, P.; Kostenko, S.; Bag, A.; Balakrishnan, B.; Patel, K.S.; Guerra, A.A.; Martinez, M.N.; Trivedi, S.; et al. Pancreatic Triglyceride Lipase Mediates Lipotoxic Systemic Inflammation. J. Clin. Investig. 2020, 130, 1931–1947. [Google Scholar] [CrossRef] [PubMed]
- Pandanaboyana, S.; Moir, J.; Leeds, J.S.; Oppong, K.; Kanwar, A.; Marzouk, A.; Belgaumkar, A.; Gupta, A.; Siriwardena, A.K.; Haque, A.R.; et al. SARS-CoV-2 Infection in Acute Pancreatitis Increases Disease Severity and 30-Day Mortality: COVID PAN Collaborative Study. Gut 2021, 70, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Navina, S.; Acharya, C.; DeLany, J.P.; Orlichenko, L.S.; Baty, C.J.; Shiva, S.S.; Durgampudi, C.; Karlsson, J.M.; Lee, K.; Bae, K.T.; et al. Lipotoxicity Causes Multisystem Organ Failure and Exacerbates Acute Pancreatitis in Obesity. Sci. Transl. Med. 2011, 3, 107ra110. [Google Scholar] [CrossRef]
- El-Kurdi, B.; Khatua, B.; Rood, C.; Snozek, C.; Cartin-Ceba, R.; Singh, V.P. Lipotoxicity in COVID-19 Study Group Mortality From Coronavirus Disease 2019 Increases With Unsaturated Fat and May Be Reduced by Early Calcium and Albumin Supplementation. Gastroenterology 2020, 159, 1015–1018.e4. [Google Scholar] [CrossRef] [PubMed]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The Vascular Endothelium: The Cornerstone of Organ Dysfunction in Severe SARS-CoV-2 Infection. Crit. Care 2020, 24, 353. [Google Scholar] [CrossRef] [PubMed]
- Rotar, O.; Khomiak, I.; Polanskyy, O.; Muskovsky, Y.; Railianu, S.; Fishbach, M. Case Report of Fatal Acute Necrotizing Pancreatitis in Patient with COVID-19: We Should Be Aware Of Hemorrhagic Complications. J. Pancreas 2020, 21, 167–171. [Google Scholar]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement Associated Microvascular Injury and Thrombosis in the Pathogenesis of Severe COVID-19 Infection: A Report of Five Cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- van Haren, F.M.P.; Sleigh, J.W.; Pickkers, P.; Van der Hoeven, J.G. Gastrointestinal Perfusion in Septic Shock. Anaesth. Intensive Care 2007, 35, 679–694. [Google Scholar] [CrossRef]
- Hackert, T.; Hartwig, W.; Fritz, S.; Schneider, L.; Strobel, O.; Werner, J. Ischemic Acute Pancreatitis: Clinical Features of 11 Patients and Review of the Literature. Am. J. Surg. 2009, 197, 450–454. [Google Scholar] [CrossRef]
- Nitsche, C.J.; Jamieson, N.; Lerch, M.M.; Mayerle, J.V. Drug Induced Pancreatitis. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 143–155. [Google Scholar] [CrossRef]
- Morrison, A.R.; Johnson, J.M.; Ramesh, M.; Bradley, P.; Jennings, J.; Smith, Z.R. Acute Hypertriglyceridemia in Patients with COVID-19 Receiving Tocilizumab. J. Med. Virol. 2020, 92, 1791–1792. [Google Scholar] [CrossRef] [PubMed]
- Flaig, T.; Douros, A.; Bronder, E.; Klimpel, A.; Kreutz, R.; Garbe, E. Tocilizumab-Induced Pancreatitis: Case Report and Review of Data from the FDA Adverse Event Reporting System. J. Clin. Pharm. Ther. 2016, 41, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Badalov, N.; Baradarian, R.; Iswara, K.; Li, J.; Steinberg, W.; Tenner, S. Drug-Induced Acute Pancreatitis: An Evidence-Based Review. Clin. Gastroenterol. Hepatol. 2007, 5, 648–661.e3. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Miyagi, K.; Otsuki, M.; Higure, Y.; Nishiyama, N.; Kinjo, T.; Nakamatsu, M.; Haranaga, S.; Tateyama, M.; Fujita, J. Acute Hypertriglyceridaemia Caused by Tocilizumab in a Patient with Severe COVID-19. Intern. Med. 2020, 59, 2945–2949. [Google Scholar] [CrossRef] [PubMed]
- Elkhouly, M.A.; Salazar, M.J.; Simons-Linares, C.R. Hypertriglyceridemia-Associated Drug-Induced Acute Pancreatitis. Pancreas 2019, 48, 22–35. [Google Scholar] [CrossRef]
- Reyes, J.V.; Patel, B.M.; Malik, F.; Gonzalez, M.O. Non-Steroidal Anti-Inflammatory Drug-Induced Acute Pancreatitis: A Case Report. Cureus 2019, 11, e5926. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, J.; Rizwan, T.; Malik, F.; Akhter, R.; Malik, M.; Ahmad, J.; Khan, A.W.; Chaudhary, M.A.; Usman, M.S. COVID-19 and Liver Injury: A Systematic Review and Meta-Analysis. Cureus 2020, 12, e9424. [Google Scholar] [CrossRef] [PubMed]
- Abdulla, S.; Hussain, A.; Azim, D.; Abduallah, E.H.; Elawamy, H.; Nasim, S.; Kumar, S.; Naveed, H. COVID-19-Induced Hepatic Injury: A Systematic Review and Meta-Analysis. Cureus 2020, 12, e10923. [Google Scholar] [CrossRef]
- Parohan, M.; Yaghoubi, S.; Seraji, A. Liver Injury Is Associated with Severe Coronavirus Disease 2019 (COVID-19) Infection: A Systematic Review and Meta-Analysis of Retrospective Studies. Hepatol Res 2020, 50, 924–935. [Google Scholar] [CrossRef]
- Wu, Z.-H.; Yang, D.-L. A Meta-Analysis of the Impact of COVID-19 on Liver Dysfunction. Eur. J. Med. Res. 2020, 25, 54. [Google Scholar] [CrossRef]
- Shokri Afra, H.; Amiri-Dashatan, N.; Ghorbani, F.; Maleki, I.; Rezaei-Tavirani, M. Positive Association between Severity of COVID-19 Infection and Liver Damage: A Systematic Review and Meta-Analysis. Gastroenterol. Hepatol. Bed Bench 2020, 13, 292–304. [Google Scholar] [PubMed]
- Youssef, M.; Hussein, M.H.; Attia, A.S.; Elshazli, R.M.; Omar, M.; Zora, G.; Farhoud, A.S.; Elnahla, A.; Shihabi, A.; A Toraih, E.; et al. COVID-19 and Liver Dysfunction: A Systematic Review and Meta-Analysis of Retrospective Studies. J. Med. Virol. 2020, 92, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, H.; Guo, X.; Yoshida, E.M.; Mendez-Sanchez, N.; Levi Sandri, G.B.; Teschke, R.; Romeiro, F.G.; Shukla, A.; Qi, X. Incidence, Risk Factors, and Prognosis of Abnormal Liver Biochemical Tests in COVID-19 Patients: A Systematic Review and Meta-Analysis. Hepatol. Int. 2020, 14, 621–637. [Google Scholar] [CrossRef] [PubMed]
- Bangash, M.N.; Patel, J.; Parekh, D. COVID-19 and the Liver: Little Cause for Concern. Lancet Gastroenterol. Hepatol. 2020, 5, 529–530. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xiao, S.-Y. Hepatic Involvement in COVID-19 Patients: Pathology, Pathogenesis, and Clinical Implications. J. Med. Virol. 2020, 92, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Fan, J.-G. Characteristics and Mechanism of Liver Injury in 2019 Coronavirus Disease. J. Clin. Transl. Hepatol. 2020, 8, 13–17. [Google Scholar] [CrossRef]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.-Y. Pathological Study of the 2019 Novel Coronavirus Disease (COVID-19) through Postmortem Core Biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, S.; Liu, H.; Li, W.; Lin, F.; Jiang, L.; Li, X.; Xu, P.; Zhang, L.; Zhao, L.; et al. SARS-CoV-2 Infection of the Liver Directly Contributes to Hepatic Impairment in Patients with COVID-19. J. Hepatol. 2020, 73, 807–816. [Google Scholar] [CrossRef]
- Uhlén, M.; Fagerberg, L.; Hallström, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, Å.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Proteomics. Tissue-Based Map of the Human Proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef]
- Li, M.-Y.; Li, L.; Zhang, Y.; Wang, X.-S. Expression of the SARS-CoV-2 Cell Receptor Gene ACE2 in a Wide Variety of Human Tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef]
- Chai, X.; Hu, L.; Zhang, Y.; Han, W.; Lu, Z.; Ke, A.; Zhou, J.; Shi, G.; Fang, N.; Fan, J.; et al. Specific ACE2 Expression in Cholangiocytes May Cause Liver Damage After 2019-nCoV Infection. biorXiv 2020. [Google Scholar] [CrossRef]
- Guan, G.W.; Gao, L.; Wang, J.W.; Wen, X.J.; Mao, T.H.; Peng, S.W.; Zhang, T.; Chen, X.M.; Lu, F.M. Exploring the mechanism of liver enzyme abnormalities in patients with novel coronavirus-infected pneumonia. Zhonghua Gan Zang Bing Za Zhi 2020, 28, 100–106. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal Liver Function Tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of Inflammatory Markers with the Severity of COVID-19: A Meta-Analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, S.; Xu, M.; Yu, P.; Zheng, S.; Duan, Z.; Liu, J.; Chen, Y.; Li, J. Risk Factors Related to Hepatic Injury in Patients with Corona Virus Disease 2019. MedRxiv 2020. [Google Scholar] [CrossRef]
- Payen, D.; Cravat, M.; Maadadi, H.; Didelot, C.; Prosic, L.; Dupuis, C.; Losser, M.-R.; De Carvalho Bittencourt, M. A Longitudinal Study of Immune Cells in Severe COVID-19 Patients. Front. Immunol. 2020, 11, 580250. [Google Scholar] [CrossRef]
- Tian, D.; Ye, Q. Hepatic Complications of COVID-19 and Its Treatment. J. Med. Virol. 2020, 92, 1818–1824. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Wang, R.S.; Qu, G.Q.; Wang, Y.Y.; Liu, P.; Zhu, Y.Z.; Fei, G.; Ren, L.; Zhou, Y.W.; Liu, L. Gross Examination Report of a COVID-19 Death Autopsy. Fa Yi Xue Za Zhi 2020, 36, 21–23. [Google Scholar] [CrossRef]
- Zhou, J.; Chu, H.; Li, C.; Wong, B.H.-Y.; Cheng, Z.-S.; Poon, V.K.-M.; Sun, T.; Lau, C.C.-Y.; Wong, K.K.-Y.; Chan, J.Y.-W.; et al. Active Replication of Middle East Respiratory Syndrome Coronavirus and Aberrant Induction of Inflammatory Cytokines and Chemokines in Human Macrophages: Implications for Pathogenesis. J. Infect. Dis. 2014, 209, 1331–1342. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; June, C.H. Cytokine Release Syndrome in Severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Ramiro, S.; Mostard, R.L.M.; Magro-Checa, C.; van Dongen, C.M.P.; Dormans, T.; Buijs, J.; Gronenschild, M.; de Kruif, M.D.; van Haren, E.H.J.; van Kraaij, T.; et al. Historically Controlled Comparison of Glucocorticoids with or without Tocilizumab versus Supportive Care Only in Patients with COVID-19-Associated Cytokine Storm Syndrome: Results of the CHIC Study. Ann. Rheum. Dis. 2020, 79, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Ji, P.; Pang, J.; Zhong, Z.; Li, H.; He, C.; Zhang, J.; Zhao, C. Clinical Characteristics of 3062 COVID-19 Patients: A Meta-analysis. J. Med. Virol. 2020, 92, 1902–1914. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Belani, P.; Schefflein, J.; Kihira, S.; Rigney, B.; Delman, B.N.; Mahmoudi, K.; Mocco, J.; Majidi, S.; Yeckley, J.; Aggarwal, A.; et al. COVID-19 Is an Independent Risk Factor for Acute Ischemic Stroke. AJNR Am. J. Neuroradiol. 2020, 41, 1361–1364. [Google Scholar] [CrossRef]
- Fu, J.; Zhou, B.; Zhang, L.; Balaji, K.S.; Wei, C.; Liu, X.; Chen, H.; Peng, J.; Fu, J. Expressions and Significances of the Angiotensin-Converting Enzyme 2 Gene, the Receptor of SARS-CoV-2 for COVID-19. Mol. Biol. Rep. 2020, 47, 4383–4392. [Google Scholar] [CrossRef]
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef]
- Eassawy, M.M.T.; Salem, A.A.; Ismail, A.F.M. Biochemical Study on the Protective Effect of Curcumin on Acetaminophen and Gamma-irradiation Induced Hepatic Toxicity in Rats. Environ. Toxicol. 2020, 36, 748–763. [Google Scholar] [CrossRef]
- Muhović, D.; Bojović, J.; Bulatović, A.; Vukčević, B.; Ratković, M.; Lazović, R.; Smolović, B. First Case of Drug-Induced Liver Injury Associated with the Use of Tocilizumab in a Patient with COVID-19. Liver Int. 2020, 40, 1901–1905. [Google Scholar] [CrossRef]
- Falcão, M.B.; Pamplona de Góes Cavalcanti, L.; Filgueiras Filho, N.M.; Antunes de Brito, C.A. Case Report: Hepatotoxicity Associated with the Use of Hydroxychloroquine in a Patient with COVID-19. Am. J. Trop. Med. Hyg. 2020, 102, 1214–1216. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ling, Y.; Xi, X.; Liu, P.; Li, F.; Li, T.; Shang, Z.; Wang, M.; Shen, Y.; Lu, H. Efficacies of lopinavir/ritonavir and abidol in the treatment of novel coronavirus pneumonia. Chin. J. Infect. Dis. 2020, 38, 86–89. [Google Scholar]
- Zampino, R.; Mele, F.; Florio, L.L.; Bertolino, L.; Andini, R.; Galdo, M.; De Rosa, R.; Corcione, A.; Durante-Mangoni, E. Liver Injury in Remdesivir-Treated COVID-19 Patients. Hepatol. Int. 2020, 14, 881–883. [Google Scholar] [CrossRef]
- Ye, H.; Nelson, L.J.; Gómez Del Moral, M.; Martínez-Naves, E.; Cubero, F.J. Dissecting the Molecular Pathophysiology of Drug-Induced Liver Injury. World J. Gastroenterol. 2018, 24, 1373–1385. [Google Scholar] [CrossRef] [PubMed]
- Vinken, M.; Maes, M.; Vanhaecke, T.; Rogiers, V. Drug-Induced Liver Injury: Mechanisms, Types and Biomarkers. Curr. Med. Chem. 2013, 20, 3011–3021. [Google Scholar] [CrossRef]
- Mushtaq, K.; Khan, M.U.; Iqbal, F.; Alsoub, D.H.; Chaudhry, H.S.; Ata, F.; Iqbal, P.; Elfert, K.; Balaraju, G.; Almaslamani, M.; et al. NAFLD Is a Predictor of Liver Injury in COVID-19 Hospitalized Patients but Not of Mortality, Disease Severity on the Presentation or Progression—The Debate Continues. J. Hepatol. 2021, 74, 482–484. [Google Scholar] [CrossRef]
- Hashemi, N.; Viveiros, K.; Redd, W.D.; Zhou, J.C.; McCarty, T.R.; Bazarbashi, A.N.; Hathorn, K.E.; Wong, D.; Njie, C.; Shen, L.; et al. Impact of Chronic Liver Disease on Outcomes of Hospitalized Patients with COVID-19: A Multicentre United States Experience. Liver Int. 2020, 40, 2515–2521. [Google Scholar] [CrossRef]
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Non-Alcoholic Fatty Liver Diseases in Patients with COVID-19: A Retrospective Study. J. Hepatol. 2020, 73, 451–453. [Google Scholar] [CrossRef]
- Yao, R.; Zhu, L.; Wang, J.; Liu, J.; Xue, R.; Xue, L.; Liu, L.; Li, C.; Zhao, H.; Cheng, J.; et al. Risk of Severe Illness of COVID-19 Patients with NAFLD and Increased NAFLD Fibrosis Scores. J. Clin. Lab. Anal. 2021, 35, e23880. [Google Scholar] [CrossRef]
- Boettler, T.; Newsome, P.N.; Mondelli, M.U.; Maticic, M.; Cordero, E.; Cornberg, M.; Berg, T. Care of Patients with Liver Disease during the COVID-19 Pandemic: EASL-ESCMID Position Paper. JHEP Rep. 2020, 2, 100113. [Google Scholar] [CrossRef]
- Portincasa, P.; Krawczyk, M.; Machill, A.; Lammert, F.; Di Ciaula, A. Hepatic Consequences of COVID-19 Infection. Lapping or Biting? Eur. J. Intern. Med. 2020, 77, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Arrese, M.; Cabrera, D.; Kalergis, A.M.; Feldstein, A.E. Innate Immunity and Inflammation in NAFLD/NASH. Dig. Dis. Sci. 2016, 61, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Krenkel, O.; Tacke, F. Macrophages in Nonalcoholic Fatty Liver Disease: A Role Model of Pathogenic Immunometabolism. Semin. Liver Dis. 2017, 37, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Kumar, A.; Anikhindi, S.; Bansal, N.; Singla, V.; Shivam, K.; Arora, A. Effect of COVID-19 on Pre-Existing Liver Disease: What Hepatologist Should Know? J. Clin. Exp. Hepatol. 2021, 11, 484–493. [Google Scholar] [CrossRef]
- Lefere, S.; Tacke, F. Macrophages in Obesity and Non-Alcoholic Fatty Liver Disease: Crosstalk with Metabolism. JHEP Rep. 2019, 1, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.; Gerber, P.A.; Cavelti-Weder, C.; Licht, L.; Kotb, R.; Al Dweik, R.; Cherfane, M.; Bornstein, S.R.; Perakakis, N. Liver, NAFLD and COVID-19. Horm. Metab. Res. 2022, 54, 522–531. [Google Scholar] [CrossRef]
- Targher, G.; Mantovani, A.; Byrne, C.D.; Wang, X.-B.; Yan, H.-D.; Sun, Q.-F.; Pan, K.-H.; Zheng, K.I.; Chen, Y.-P.; Eslam, M.; et al. Risk of Severe Illness from COVID-19 in Patients with Metabolic Dysfunction-Associated Fatty Liver Disease and Increased Fibrosis Scores. Gut 2020, 69, 1545–1547. [Google Scholar] [CrossRef]
- Portincasa, P.; Krawczyk, M.; Smyk, W.; Lammert, F.; Di Ciaula, A. COVID-19 and Non-alcoholic Fatty Liver Disease: Two Intersecting Pandemics. Eur. J. Clin. Investig. 2020, 50, e13338. [Google Scholar] [CrossRef]
- Gao, B.; Tsukamoto, H. Inflammation in Alcoholic and Nonalcoholic Fatty Liver Disease: Friend or Foe? Gastroenterology 2016, 150, 1704–1709. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and Nonalcoholic Fatty Liver Disease: From Pathophysiology to Therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef]
- Nardo, A.D.; Schneeweiss-Gleixner, M.; Bakail, M.; Dixon, E.D.; Lax, S.F.; Trauner, M. Pathophysiological Mechanisms of Liver Injury in COVID-19. Liver Int. 2021, 41, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.; Silverstein, A.; Flores, M.; Cao, K.; Kumagai, H.; Mehta, H.H.; Yen, K.; Kim, S.-J.; Cohen, P. Host Mitochondrial Transcriptome Response to SARS-CoV-2 in Multiple Cell Models and Clinical Samples. Sci. Rep. 2021, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Boeckmans, J.; Rodrigues, R.M.; Demuyser, T.; Piérard, D.; Vanhaecke, T.; Rogiers, V. COVID-19 and Drug-Induced Liver Injury: A Problem of Plenty or a Petty Point? Arch. Toxicol. 2020, 94, 1367–1369. [Google Scholar] [CrossRef] [PubMed]
- Ferron, P.-J.; Gicquel, T.; Mégarbane, B.; Clément, B.; Fromenty, B. Treatments in COVID-19 Patients with Pre-Existing Metabolic Dysfunction-Associated Fatty Liver Disease: A Potential Threat for Drug-Induced Liver Injury? Biochimie 2020, 179, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.A.; Kunte, A.R. Interleukin-6: An Early Predictive Marker for Severity of Acute Pancreatitis. Indian. J. Crit. Care Med. 2017, 21, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, A.; van de Peppel, I.P.; Bodewes, F.A.J.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J.; et al. Abnormal Liver Function Tests in Patients With COVID-19: Relevance and Potential Pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Esteban, J.; Manzano-Nuñez, R.; Broquetas, T.; Serra-Matamala, I.; Bassegoda, O.; Soriano-Varela, A.; Espín, G.; Castillo, J.; Bañares, J.; Carrión, J.A.; et al. Impact of the COVID-19 Pandemic on the Care and Outcomes of People with NAFLD-Related Cirrhosis. JHEP Rep. 2022, 4, 100574. [Google Scholar] [CrossRef]
- Canillas, L.; Broquetas, T.; Carrión, J.A.; Pagano, G.; Soriano, A.; Garrido, E.; Fernández, R.; Viu, A.; Romero, J.; Díaz, G.; et al. Follow-up Evaluation of Patients with Liver Test Abnormalities Detected during SARS-CoV2 Infection. J. Viral Hepat. 2022, 29, 823–834. [Google Scholar] [CrossRef]
- Sachdeva, S.; Khandait, H.; Kopel, J.; Aloysius, M.M.; Desai, R.; Goyal, H. NAFLD and COVID-19: A Pooled Analysis. SN Compr. Clin. Med. 2020, 2, 2726–2729. [Google Scholar] [CrossRef]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and Diabetes as High-risk Factors for Severe Coronavirus Disease 2019 (COVID-19). Diabetes Metab Res Rev 2021, 37, e3377. [Google Scholar] [CrossRef]
- Prins, G.H.; Olinga, P. Potential Implications of COVID-19 in Non-Alcoholic Fatty Liver Disease. Liver Int. 2020, 40, 2568. [Google Scholar] [CrossRef] [PubMed]
- Guillot, A.; Tacke, F. Liver Macrophages: Old Dogmas and New Insights. Hepatol. Commun. 2019, 3, 730–743. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Authors [Ref] | Study Design | Total Number of Patients | Number of Patients with AP | AP, According to RAC | Observations |
|---|---|---|---|---|---|
| Kataria et al. [15] | Case report | 1 Female (49Y) | - | 1 | CT scan: edematous pancreas with diffuse enlargement † |
| Alves et al. [16] | Case report | 1 Female (56Y) | - | 1 | CT scan: tail parenchymal enlargement and surrounding retroperitoneal fat stranding † |
| Kumaran et al. [17] | Case report | 1 Female (67Y) | - | 1 | CT scan: necrotising Pancreatitis † |
| Rabice et al. [18] | Case report | 1 Female (36Y) (P) | 1 | - | Lipase was at 875 U/L; an abdominal ultrasound did not show the pancreas due to bowel gas |
| Cerda-Contreras et al. [19] | Case report | 1 Female (72Y) (S) | - | 1 | Patient received baricitinib * and dexamethasone CT scan: pancreatic oedema. No information regarding abdominal pain |
| Akarsu et al. [20] | Prospective study | 316 | - | 40 (12.6%) | 7.9% (n = 15) of patients with severe symptoms and 32.5% (n = 25) of patients in critical status Δ |
| Juhász et al. [21] | Systematic review | 19 | 6 (32.5%) | 5 (26.3%) | Studies included contained data on 11 COVID-19 patients with AP Δ |
| Authors [Ref] | Sample | Patients with Altered Pancreatic Enzymes | Amylase (U/L) (Mean ± SD) | Lipase (U/L) (Mean ± SD) | Observations |
|---|---|---|---|---|---|
| Wang et al. [13] | n = 52 | n = 9 (17.3%) | 115 ± 25 | 71 ± 34 | Normal Amylase range 0–90 U/L and Normal Lipase range 0–70 U/L |
| Bruno et al. [14] | n = 70 | n = 6 (8.5%) | 338.3 ± 246.6 | 1509 ± 1163 | Hyperlipasemia was defined as an elevated lipase level above the ULN (>393 U/L). All patients meet these criteria. |
| McNabb-Baltar et al. [22] | n = 71 | n = 9 (12.1%) | NP | 151.8 ± 148.4 | Hyperlipasemia was defined as an elevated lipase level above the ULN (>60 U/L). Two patients (2.8%) developed hyperlipasemia greater than three times the ULN (>180 U/L). |
| Barlass et al. [23] | n = 83 | n = 14 (16.8%) | NP | NA | High lipase was defined as levels greater than three times the ULN (>156 U/L) |
| Rasch et al. [24] | n = 38 | n = 12 (31.6%) | NP | 422 (186–1127) * | Patients with lipase activity at least three times greater than the ULN (>180 U/L) |
| Zhang et al. [25] | n = 19 | n = 19 (100%) | 64.3 (56.4–94.6) * (mg/L) | NP | - |
| Authors [Ref]/ N° Studies Included | Participants | Liver Function Tests (Mean Differences between Severe Cases Versus Non-Severe Cases) |
|---|---|---|
| Ahmed et al. [67] N° = 27 | Total = 8817 Severe cases = 2900 Non-severe cases = 7184 | ALT (WMD: 7.19 U/L; 95% CI: 4.90 to 9.48; p < 0.001; I2 = 69%) AST (WMD: 9.02 U/L; 95% CI: 6.89 to 11.15; p < 0.001; I2 = 73%) BIL (WMD: 1.78 μmol/L; 95% CI: 0.86 to 2.70; p < 0.001; I2 = 82%) ALB (WMD: −4.16 g/L; 95% CI: −5.97 to −2.35; p < 0.001; I2 = 95%) |
| Abdulla et al. [68] N° = 12 | Total = 6976 Subgroup analysis: Severe cases = 131 Non-severe cases = 334 | ALT (WMD: 31.66 U/L; 95% CI: 25.07, 38.25; p < 0.0001; I2 = 55.64%) AST (WMD: 41.79 U/L; 95% CI: 32.85, 50.72; p < 0.0001; I2 = 51.43%) BIL (WMD: 9.97 μmol/L; 95% CI: 8.46 to 11.48; p < 0.0001; I2 = 98%) ALB (WMD: 34.03 g/L; 95% CI: 27.42 to 40.63; p < 0.0001; I2 = 96.83%) |
| Parohan et al. [69] N° = 20 | Total = 3428 Severe cases = 1455 Mild cases = 1973 | AST (WMD: 8.84 U/L; 95% CI: 5.97 to 11.71; p < 0.001) ALT (WMD: 7.35 U/L; 95% CI: 4.77 to 9.93; p < 0.001) BIL (WMD: 2.30 mmol/L; 95% CI: 1.24 to 3.36; p < 0.001) ALB (WMD: −4.24 g/L; 95% CI: −6.20 to −2.28; p < 0.001) |
| Wu and Yang [70] N° = 13 | Total = 3722 Severe cases = 721 Non-severe cases: 1968 Dead/Alive: 285/748 | AST (WMD:3.35 U/L; 95% CI: 2.07 to 4.64; p < 0.001) BIL (WMD: 1.18 μmol/L; 95% CI: 0.78 to 1.58; p < 0.001) Liver dysfunction and mortality of COVID-19 patients: OR = 1.98; 95% CI: 1.39 to 2.82; p = 0.0002 Liver dysfunction and severity of COVID-19 patients: AST (OR = 4.48; 95% CI 3.24 to 7.21; p < 0.001) BIL (OR = 1.91; 95% CI: 1.40 to 2.60; p < 0.001) |
| Shokri Afra H. et al. [71] N° = 24 | 4246 patients Severe cases: 1635 Non-severe cases: 2611 | ALT (SMD: 1.40 U/L; 95% CI: 0.93 to 1.88; p < 0.05; I2 = 96.5%) AST (SMD: 2.11 U/L; 95% CI: 1.40 to 2.83; p < 0.05; I2 = 97.9%) BIL (SMD: 1.08 μmol/L; 95% CI: 0.44 to 1.72; p = 0.001; I2 = 97.7%) ALP (SMD: 0.31; 95% CI: −1.57 to 2.20; p = 0.74) |
| Youssef et al. [72] N° = 20 | Total = 3428 patients Severe cases = 1241 Non-severe cases: 2187 | Prothrombin time (SMD: 0.69; 95% CI: 0.57 to 0.81; p < 0.001) AST (SMD: 0.36; 95% CI: 0.27 to 0.44; p < 0.001) ALT (SMD: 0.44; 95% CI: 0.35 to 0.52; p < 0.001) BIL (SMD: 0.40; 95% CI: 0.31 to 0.50; p < 0.001) ALB (SMD: −0.68; 95% CI: −0.7 to −0.58; p < 0.001) |
| Kumar-M et al. [10] N° = 128 | - | BIL (SMD: 0.43 μmol/L; 95% CI: 0.26 to 0.61; p < 0.05; I2 = 66%) ALB (SMD: −1.05 g/L; 95% CI: −1.27 to −0.83; p < 0.05; I2 = 77%) GGT (SMD: 0.76; 95% CI: 0.40 to 1.12; p < 0.05; I2 = 82%) Liver dysfunction and severity of COVID-19 patients: BIL (RR = 1.82; 95% CI: 1.22 to 2.73; p < 0.05; I2 = 66%) ALB (RR = 2.65; 95% CI: 1.38 to 5.07; p < 0.05; I2 = 79%) GGT (RR = 2.31; 95% CI: 1.6 to 3.33; p < 0.05; I2 = 55%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mengual-Moreno, E.; Nava, M.; Manzano, A.; Ariza, D.; D’Marco, L.; Castro, A.; Marquina, M.A.; Hernández, M.; Corredor-Pereira, C.; Checa-Ros, A.; et al. Pancreatic and Hepatic Injury in COVID-19: A Worse Prognosis in NAFLD Patients? Biomedicines 2024, 12, 283. https://doi.org/10.3390/biomedicines12020283
Mengual-Moreno E, Nava M, Manzano A, Ariza D, D’Marco L, Castro A, Marquina MA, Hernández M, Corredor-Pereira C, Checa-Ros A, et al. Pancreatic and Hepatic Injury in COVID-19: A Worse Prognosis in NAFLD Patients? Biomedicines. 2024; 12(2):283. https://doi.org/10.3390/biomedicines12020283
Chicago/Turabian StyleMengual-Moreno, Edgardo, Manuel Nava, Alexander Manzano, Daniela Ariza, Luis D’Marco, Ana Castro, María A. Marquina, Marlon Hernández, Carlos Corredor-Pereira, Ana Checa-Ros, and et al. 2024. "Pancreatic and Hepatic Injury in COVID-19: A Worse Prognosis in NAFLD Patients?" Biomedicines 12, no. 2: 283. https://doi.org/10.3390/biomedicines12020283
APA StyleMengual-Moreno, E., Nava, M., Manzano, A., Ariza, D., D’Marco, L., Castro, A., Marquina, M. A., Hernández, M., Corredor-Pereira, C., Checa-Ros, A., & Bermúdez, V. (2024). Pancreatic and Hepatic Injury in COVID-19: A Worse Prognosis in NAFLD Patients? Biomedicines, 12(2), 283. https://doi.org/10.3390/biomedicines12020283