

Post-COVID-19 Symptoms in Adults with Asthma—Systematic Review

Abstract
:
1. Introduction
Objective/Review Questions
- What are the long-term symptoms (lasting at least 12 weeks) caused by SARS-CoV-2 infection among patients with asthma?
- Are the long-term symptoms (lasting at least 12 weeks) caused by SARS-CoV-2 in patients diagnosed with asthma different from those of patients without asthma?
- What does the evidence tell us about the long-term consequences for lung function, asthma symptoms, intensity of pharmacological treatment, physical fitness, and mental health of adults with asthma after SARS-CoV-2 infection?
- Does asthma control before SARS-CoV-2 infection and asthma phenotype influence the severity of the disease, lung function, and the severity of long-term symptoms after infection?
2. Methodology
2.1. Searches
2.2. Types of Included Studies
- Studies focusing on COVID-19 symptoms lasting <12 weeks from the onset of the disease or only on the pathophysiology of COVID-19 in asthma.
- Age of the participants <18 years.
- Studies without evidence of laboratory confirmation of SARS-CoV-2 infection in participants.
- Studies without information about asthma diagnosis in participants.
- Secondary analysis (i.e., systematic review or meta-analysis); however, their reference lists have been manually searched for potentially relevant studies.
- Literature in languages other than English.
2.3. The Condition Being Studied and the Population of Patients
2.4. Comparator(s)/Control
2.5. Main Outcome(s)
2.6. Additional Results
- Pulmonary function of people with asthma 12 weeks after SARS-CoV-2 infection [forced vital capacity (FVC); forced expiratory volume in the first second (FEV1); FEV1/FVC ratio; total lung capacity (TLC), residual volume (RV), and vital capacity (VC)].
- Severity of symptoms within 12 weeks after COVID-19 infection [dyspnoea: Modified Medical Research Council dyspnoea scale (mMRC), asthma control test (ACT), asthma control questionnaire (ACQ); Asthma Quality of Life Questionnaire for asthma (AQLQ)]; Depression scale, the number of cases with decreased asthma control after COVID-19.
- Modification of the intensity of asthma pharmacological treatment after COVID-19 infection.
2.7. Data Extraction (Selection and Coding)
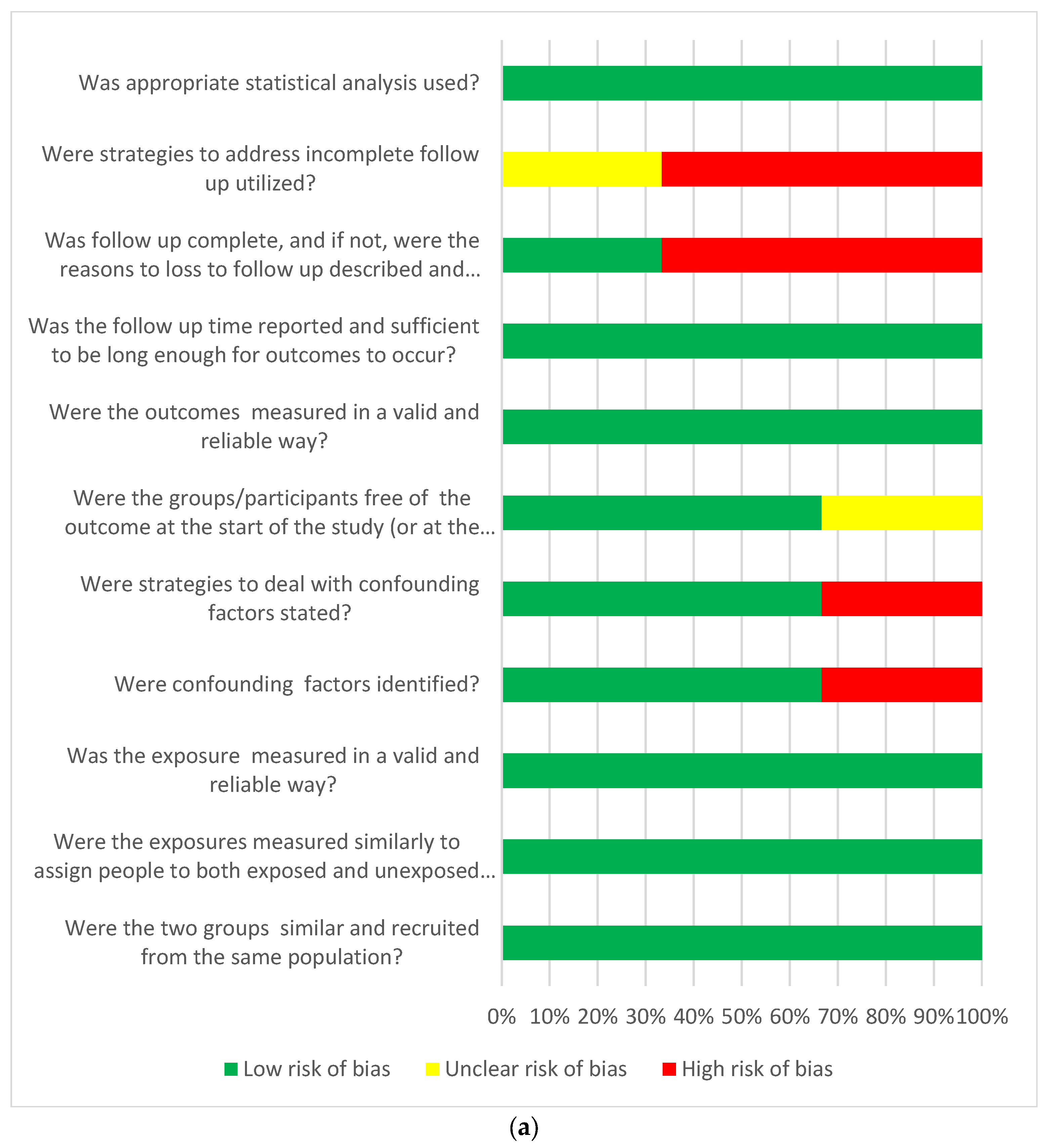
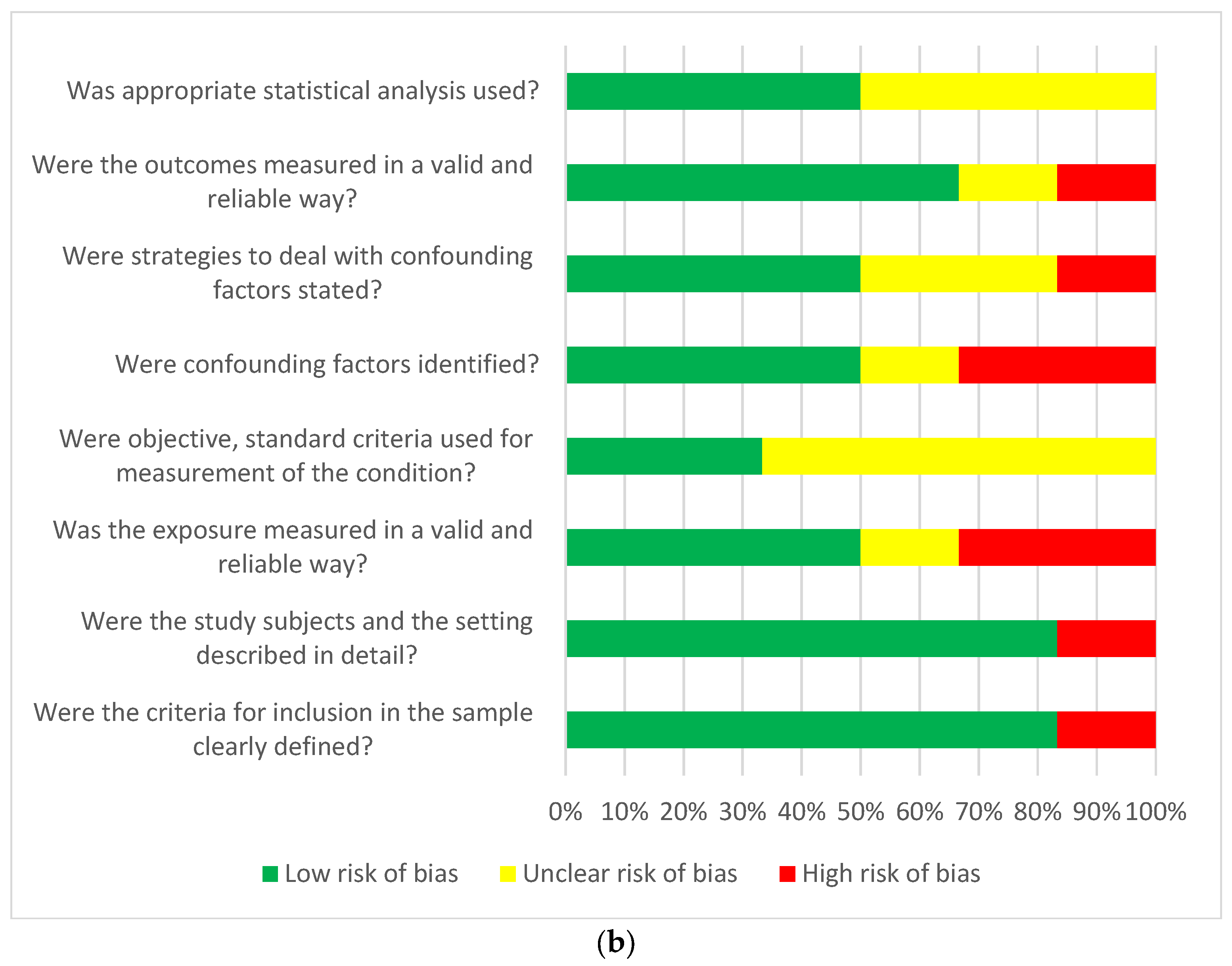
2.8. Evaluation of Risk of Bias (Quality)
2.9. Strategy for Data Synthesis
3. Results
Methodological Quality of Included Studies
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Asthma GINA Global Strategy for Asthma Management and Prevention Global Initiative for Asthma (GINA) What’s New in GINA 2021? Available online: www.ginasthma.org (accessed on 21 November 2022).
- Nassoro, D.D.; Mujwahuzi, L.; Mwakyula, I.H.; Possi, M.K.; Lyantagaye, S.L. Asthma and COVID-19: Emphasis on Adequate Asthma Control. Can. Respir. J. 2021, 2021, 9621572. [Google Scholar] [CrossRef] [PubMed]
- Adir, Y.; Saliba, W.; Beurnier, A.; Humbert, M. Asthma and COVID-19: An update. Eur. Respir. Rev. 2021, 30, 210152. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Marcello, R.K.; Dolle, J.; Grami, S.; Adule, R.; Li, Z.; Tatem, K.; Anyaogu, C.; Apfelroth, S.; Ayinla, R.; Boma, N.; et al. Characteristics and outcomes of COVID-19 patients in New York City’s public hospital system. PLoS ONE 2020, 15, e0243027. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Lombardi, C.; Micheletto, C.; Roca, E.; Bigni, B.; Furci, F.; Girelli, D.; Senna, G.; Crisafulli, E. Asthmatic patients in COVID-19 outbreak: Few cases despite many cases. J. Allergy Clin. Immunol. 2020, 146, 541–542. [Google Scholar] [CrossRef] [PubMed]
- Beurnier, A.; Jutant, E.-M.; Jevnikar, M.; Boucly, A.; Pichon, J.; Preda, M.; Frank, M.; Laurent, J.; Richard, C.; Monnet, X.; et al. Characteristics and outcomes of asthmatic patients with COVID-19 pneumonia who require hospitalisation. Eur. Respir. J. 2020, 56, 2001875. [Google Scholar] [CrossRef]
- Laorden, D.; Domínguez-Ortega, J.; Carpio, C.; Barranco, P.; Villamañán, E.; Romero, D.; Quirce, D.; Alvarez-Sala, S.; Camperos, R.; De Agrela, I.; et al. Long COVID outcomes in an asthmatic cohort and its implications for asthma control. Respir. Med. 2023, 207, 107902. [Google Scholar] [CrossRef]
- Liu, S.; Cao, Y.; Du, T.; Zhi, Y. Prevalence of Comorbid Asthma and Related Outcomes in COVID-19: A Systematic Review and Meta-Analysis. J. Allergy Clin. Immunol. Pract. 2020, 9, 693–701. [Google Scholar] [CrossRef]
- Zhu, Z.; Hasegawa, K.; Ma, B.; Fujiogi, M.; Camargo, C.A., Jr.; Liang, L. Association of asthma and its genetic predisposition with the risk of severe COVID-19. J. Allergy Clin. Immunol. 2021, 146, 327–329.e4. [Google Scholar] [CrossRef]
- Lee, B.; Lewis, G.; Agyei-Manu, E.; Atkins, N.; Bhattacharyya, U.; Dozier, M.; Rostron, J.; Sheikh, A.; McQuillan, R.; Theodoratou, E. Risk of serious COVID-19 outcomes among adults and children with moderate-to-severe asthma: A systematic review and meta-analysis. Eur. Respir. Rev. 2022, 31, 220066. [Google Scholar] [CrossRef] [PubMed]
- Kermani, N.Z.; Song, W.J.; Badi, Y.; Versi, A.; Guo, Y.; Sun, K.; Bhavsar, P.; Howarth, P.; Dahlen, S.-E.; Sterk, P.; et al. Sputum ACE2, TMPRSS2 and FURIN gene expression in severe neutrophilic asthma. Respir. Res. 2021, 22, 10. [Google Scholar] [PubMed]
- Peters, M.C.; Fahy, J.V. Erratum: COVID-19–related Genes in Sputum Cells in Asthma: Relationship to Demographic Features and Corticosteroids. Am. J. Respir. Crit. Care Med. Am. Thorac. Soc. 2020, 202, 1744–1746. [Google Scholar]
- Coronavirus (COVID-19): Long-Term Health Effects. Available online: https://www.gov.uk/government/publications/covid-19-long-term-health-effects/covid-19-long-term-health-effects (accessed on 21 November 2022).
- Akbarialiabad, H.; Taghrir, M.H.; Abdollahi, A.; Ghahramani, N.; Kumar, M.; Paydar, S.; Razani, B.; Mwangi, J.; Asadi-Poota, A.A.; Malekmakan, L.; et al. Long COVID, a comprehensive systematic scoping review. Infection 2021, 49, 1163–1186. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Arora, U.; Kumar, A.; Wig, N. The “post-COVID” syndrome: How deep is the damage? J. Med. Virol. 2021, 93, 673–674. [Google Scholar] [PubMed]
- Cabrera Martimbianco, A.L.; Pacheco, R.L.; Bagattini, Â.M.; Riera, R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, e14357. [Google Scholar]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef]
- Chiner-Vives, E.; Cordovilla-Pérez, R.; de la Rosa-Carrillo, D.; García-Clemente, M.; Izquierdo-Alonso, J.L.; Otero-Candelera, R.; Pérez-de Llano, L.; Sellares-Torres, J.; de Granda-Orive, J.I. Short and Long-Term Impact of COVID-19 Infection on Previous Respiratory Diseases. Arch. Bronconeumol. 2022, 58, 39–50. [Google Scholar] [CrossRef]
- Garcia-Pachon, E.; Grau-Delgado, J.; Soler-Sempere, M.J.; Zamora-Molina, L.; Baeza-Martinez, C.; Ruiz-Alcaraz, S.; Padilla-Navas, I. Low prev-alence of Covid-19 syndrome in patients with asthma. J. Infect. 2021, 82, 276–316. [Google Scholar]
- Adeloye, D.; Elneima, O.; Daines, L.; Poinasamy, K.; Quint, J.K.; Walker, S.; E Brightling, C.; Siddiqui, S.; Hurst, J.R.; Chalmers, J.D.; et al. The long-term sequelae of COVID-19: An international consensus on research priorities for patients with pre-existing and new-onset airways disease. Lancet Respir. Med. 2021, 9, 1467–1478. [Google Scholar] [CrossRef] [PubMed]
- Covidence. Available online: https://www.covidence.org/ (accessed on 21 November 2022).
- Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 21 November 2022).
- Fernández-De-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Rodríuez-Jiménez, J.; Palacios-Ceña, M.; Velasco-Arribas, M.; Guijarro, C.; I De-La-Llave-Rincón, A.; Fuensalida-Novo, S.; Elvira-Martínez, C.M.; et al. Long-term post-COVID symptoms and associated risk factors in previously hospitalized patients: A multicenter study. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef] [PubMed]
- Munker, D.; Veit, T.; Barton, J.; Mertsch, P.; Mümmler, C.; Osterman, A.; Khatamzas, E.; Barnikel, M.; Hellmuth, J.C.; Münchhoff, M.; et al. Pulmonary function impairment of asymptomatic and persistently symptomatic patients 4 months after COVID-19 according to disease severity. Infection 2022, 50, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Bobkova, P.; Spiridonova, E.; Shikhaleva, A.; Gamirova, A.; Blyuss, O.; Nekliudov, N.; Bugaeva, P.; Andreeva, M.; DunnGalvin, A.; et al. Incidence and risk factors for persistent symptoms in adults previously hospitalized for COVID-19. Clin. Exp. Allergy 2021, 51, 1107–1120. [Google Scholar] [CrossRef] [PubMed]
- Maestre-Muñiz, M.M.; Arias, Á.; Mata-Vázquez, E.; Martín-Toledano, M.; López-Larramona, G.; Ruiz-Chicote, A.M.; Lucendo, A.J. Long-term outcomes of patients with coronavirus disease 2019 at one year after hospital discharge. J. Clin. Med. 2021, 10, 2945. [Google Scholar] [CrossRef] [PubMed]
- Faverio, P.; Luppi, F.; Rebora, P.; Busnelli, S.; Stainer, A.; Catalano, M.; Pesci, A. Supplementary Material for: Six-Month Pulmonary Impairment after Severe COVID-19: A Prospective, Multicentre Follow-Up Study. Respiration 2021, 100, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.; Moore, D.; Jauregui, E.; Andy-Nweye, A.; Mahdavinia, M. Five-month Outcomes for Asthmatics with COVID-19 and Associations with Atopy and Inhaled Corticosteroids Use. J. Allergy Clin. Immunol. 2021, 147, AB149. [Google Scholar] [CrossRef]
- Eggert, L.E.; He, Z.; Collins, W.; Lee, A.S.; Dhondalay, G.; Jiang, S.Y.; Fitzpatrick, J.; Snow, T.T.; Pinsky, B.A.; Artandi, M.; et al. Asthma phenotypes, associated comorbidities, and long-term symptoms in COVID-19. Allergy Eur. J. Allergy Clin. Immunol. 2022, 77, 173–185. [Google Scholar]
- Philip, K.E.J.; Buttery, S.; Williams, P.; Vijayakumar, B.; Tonkin, J.; Cumella, A.; Renwick, L.; Ogden, L.; Quint, J.K.; Johnston, S.L.; et al. Impact of COVID-19 on people with asthma: A mixed methods analysis from a UK wide survey. BMJ Open Respir. Res. 2022, 9, e001056. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Infection Survey, Antibody and Vaccination Data for the UK: 13 May 2021. Available online: www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19infectionsurveyantibodydatafortheuk/13may2021 (accessed on 21 November 2022).
- Matsuyama, S.; Kawase, M.; Nao, N.; Shirato, K.; Ujike, M.; Kamitani, W.; Fukushi, S. The Inhaled Steroid Ciclesonide Blocks SARS-CoV-2 RNA Replication by Targeting the Viral Replication-Transcription Complex in Cultured Cells. J. Virol. 2020, 95, 10–1128. [Google Scholar]
- Choi, Y.J.; Park, J.Y.; Lee, H.S.; Suh, J.; Song, J.Y.; Byun, M.K.; Park, H.J. Effect of asthma and asthma medication on the prognosis of patients with COVID-19. Eur. Respir. J. 2021, 57, 2002226. [Google Scholar]
- Green, I.; Merzon, E.; Vinker, S.; Golan-Cohen, A.; Magen, E. COVID-19 Susceptibility in Bronchial Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 684–692.e1. [Google Scholar] [CrossRef]
- Izquierdo, J.L.; Almonacid, C.; González, Y.; Del Rio-Bermudez, C.; Ancochea, J.; Cárdenas, R.; Lumbreras, S.; Soriano, J.B. The impact of COVID-19 on patients with asthma. Eur. Respir. J. 2020, 57, 2003142. [Google Scholar] [CrossRef]
- Hussein, M.H.; Elshazli, R.M.; Attia, A.S.; Nguyen, T.P.; Aboueisha, M.; Munshi, R.; Toraih, E.A.; Fawzy, M.S.; Kandil, E. Asthma and COVID-19; different entities, same outcome: A meta-analysis of 107,983 patients. J. Asthma 2020, 59, 851–858. [Google Scholar] [CrossRef]
- Mahdavinia, M.; Foster, K.J.; Jauregui, E.; Moore, D.; Adnan, D.; Andy-Nweye, A.B.; Bishehsari, F. Clinical Communications Asthma prolongs intubation in COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 2388–2391. [Google Scholar] [CrossRef]
- Ferastraoaru, D.; Hudes, G.; Jerschow, E.; Jariwala, S.; Karagic, M.; de Vos, G.; Rosenstreich, D.; Ramesh, M. Eosinophilia in Asthma Patients Is Protective Against Severe COVID-19 Illness. J. Allergy Clin. Immunol. Pract. 2021, 9, 1152–1162.e3. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article [Reference] | Study Type Age | Study Country Study Period | Total Number of Cases n= | COVID-19 and Asthma + Patients n= | Male n = (%) | Female n = (%) | COVID-19 Diagnosis | Asthma Diagnosis | Persistent Post-COVID-19 Symptoms, n (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Eggert et al. (2022) [32] | Prospective cohort study N/A | USA 1 March–30 September 2020 | 6976 | Hospitalized = 100 Not Hospitalized = 498 | COVID−19 Asthma + Hospitalized = 42 (42.0%) Not Hospitalized = 202 (40.6%) COVID−19 Asthma- Hospitalized = 247 (48.9%) Not Hospitalized = 2144 (47.7%) | COVID−19 Asthma + Hospitalized = 58 (58.0%) Not Hospitalized = 296 (59.4%) COVID−19 Asthma-Hospitalized = 258 (51.1%) Not Hospitalized = 2336 (52.0%) | Positive diagnosis by authorized SARS-CoV-2 nucleic acid amplification test from either nasal, nasopharyngeal swab, or bronchoalveolar lavage | Using an institutional informatics platform, we comprehensively characterized a cohort of patients who tested positive for SARSCoV-2 and further categorized them by baseline asthma diagnosis using the International Classification of Disease (ICD-9/10) diagnostic codes and hospitalization status; 24 Patients were categorized as having allergic asthma if they had at least one ICD-10 code for a coexisting allergic disorder the GINA 2020 guidelines | Symptoms at:
| ||
| Fernández-de-las-Peñas et al. (2021) [26] | Cross-sectional study Age, mean (SD), years Asthmatic: 55 (17) Non-asthmatic: 55 (16.5) | Spain 30 March–31 May 2020 | 400 | Asthmatic (n = 61) Non-asthmatic (n = 122) | Asthmatic: 15 (24.6%) Non-asthmatic: 30 (24.6%) | Asthmatic: 46 (75.4%) Non-asthmatic: 92 (75.4%) | Positive diagnosis of SARS-CoV-2 by RT-PCR technique and radiological findings | Assessed by the 2019 Global Initiative for Asthma (GINA) guidelines | Asthmatic [%] | Non-asthmatic [%] | |
| Dyspnoea on exertion | 75.4 | 58.2 | |||||||||
| Fatigue | 65.6 | 61.5 | |||||||||
| Dyspnoea rest | 34.4 | 27.8 | |||||||||
| Memory loss | 18 | 16.4 | |||||||||
| Skin rashes | 13.1 | 10.6 | |||||||||
| Concentration loss | 13.1 | 11.4 | |||||||||
| Cognitive Blunting—Brain fog | 9.9 | 8.2 | |||||||||
| Gastrointestinal Disorders Diarrhoea | 3.3 | 4.1 | |||||||||
| Tachycardia-palpitations | 9.8 | 6.5 | |||||||||
| Ocular Disorders | 6.6 | 7.2 | |||||||||
| Ageusia/hypogeusia | 1.6 | 2.5 | |||||||||
| Anosmia/hyposmia | 6.6 | 1.6 | |||||||||
| Throat pain | 3.3 | 2.5 | |||||||||
| Depressive symptoms | 27.9 | 22.1 | |||||||||
| Anxiety symptoms | 14.75 | 11.5 | |||||||||
| Poor sleep quality | 54.1 | 41.8 | |||||||||
| Philip et al. (2022) [33] | Cross-sectional study Median age: 50–59 years | UK October 2020 | 4500 | Had COVID-19: 471 Not sure if had COVID-19: 972 | All survey respondents: 856 (19.12%) Not sure if had COVID-19: 190 (19.59%) Had COVID-19: 84 (17.99%) | All survey respondents: 3618 (80.79%) Not sure if had COVID-19: 778 (80.21%) Had COVID-19: 382 (81.80%) | Self-reported COVID-19 | Self-reported asthma | 261 patients with long-COVID-19 (56.13%). Compared with those who had not had long-COVID-19 and those who were not sure, a higher proportion of individuals who reported that they had long COVID-19 described their breathing as worse or much worse (73.7% vs. 34.8%, p < 0.001), an increase in reliever inhaler use (67.8% vs. 34.8%, p < 0.001), and that their asthma management was worse or much worse (59.6% vs. 25.6, p < 0.001). | ||
| Pachon et al. (2021) [22] | Prospective cohort study Age > 14 years | Spain 3 March–11 December 2020 | 2995 | 74 | 32 (43%) | 42 (57%) | Positive diagnosis of SARS-CoV-2 by RT-PCR technique | Assessed by international GINA recommendations (https://ginasthma.org/) | n [%] | ||
| Post-COVID-19 syndrome at 3 months in patients with asthma | 7 (9.5%) | ||||||||||
| Dyspnoea | 1 | ||||||||||
| Fatigue | 3 | ||||||||||
| Anosmia/Hyposmia | 1 | ||||||||||
| Cough | 2 | ||||||||||
| Munker et al. (2021) [27] | Prospective cohort study The mean age: 49.6 ± 17.4 | Germany March–August 2020 | 76 | 9 | 33 (46.1%) | 43 (53.9%) | Confirmed SARS-CoV-2 infection (PCR) or positive Anti-SARS-CoV-2 Immunoglobulin G (IgG) titer | NR | Univariate regression analysis for patients with bronchial asthma | ||
| DLCOcSB | p > 0.05. | ||||||||||
| TLC | |||||||||||
| FVC | |||||||||||
| FEV1 | |||||||||||
| Munblit et al. (2021) [28] | Prospective cohort study The median age 56 years (IQR, 46–66; range, 18–100 years) | Russia 8 April–10 July 2020 | 2649 | 121 | 1296 (48.9%) | 1353 (51.1%) | Positive diagnosis of SARS-CoV-2 by RT-PCR and/or clinically confirmed infection | NR | Asthma and chronic pulmonary disease were not associated with persistent symptoms overall, but asthma was associated with neurological (1.95, 1.25 to 2.98) and mood and behavioural changes (2.02, 1.24 to 3.18), and chronic pulmonary disease was associated with chronic fatigue (1.68, 1.21 to 2.32). | ||
| Maestre-Muñiz et al. (2021) [29] | Cross-sectional study Mean age (SD): 65.1 years (17.5) | Spain 15 March–10 May 2021 | 543 | 39 | NR | NR | Laboratory-confirmed COVID-19 | Assessed by the Global Initiative for Asthma (GINA)’s treatment steps for adults | Asthma developed during the year after acute COVID-19 recovery (n = 2; 0.4%). Patients with asthma alive after one year/at baseline n = 39/51 (76.5%). Treatment intensification (n = 8, 20.5%). | ||
| Faverio et al. (2021) [30] | Prospective, observational cohort study Median interquartile range age: 61.1 years | Italy March–June 2020 | All: 312 Oxygen group:71 CPAP group: 144 IMV group: 97 | Asthma in: Oxygen group:9 CPAP group: 4 IMV group: 4 | 229 (73%) | 83 (27%) | Diagnosis of SARS-CoV-2 infection by positive PCR on nasal-pharyngeal swab or on bronchoalveolar lavage in case of double negative nasal-pharyngeal swabs performed at least 24 h apart | N/A | Patients with asthma presented higher odds of altered DLCO (OR = 4.86, 95% CI: 1.09; 21.68); odds of chest X-ray alterations in patients with asthma haven’t been higher (OR = 2.79; 95% CI: 0.58; 13.29). | ||
| Foster et al. (2021) [31] | Prospective cohort study N/A | USA February–April 2020 | 76 | 76 | NR | NR | N/A | History of asthma | Stratified by asthma severity, 66.6% of subjects with intermittent, 50.0% with mild persistent and 68.4% with moderate/severe persistent asthma experienced exacerbations (p = 0.78). The asthma exacerbation rate in patients who took inhaled corticosteroids (ICS+LABA) (n = 25, 53.3%) or ICS alone (n = 13, 55.2%) did not differ from those who were not taking ICS (n = 38, 52.6%), (p = 0.82). 42.3% of asthma patients with a history of allergic rhinitis versus 64.5% of nonallergic patients experienced an exacerbation (p = 0.086). | ||
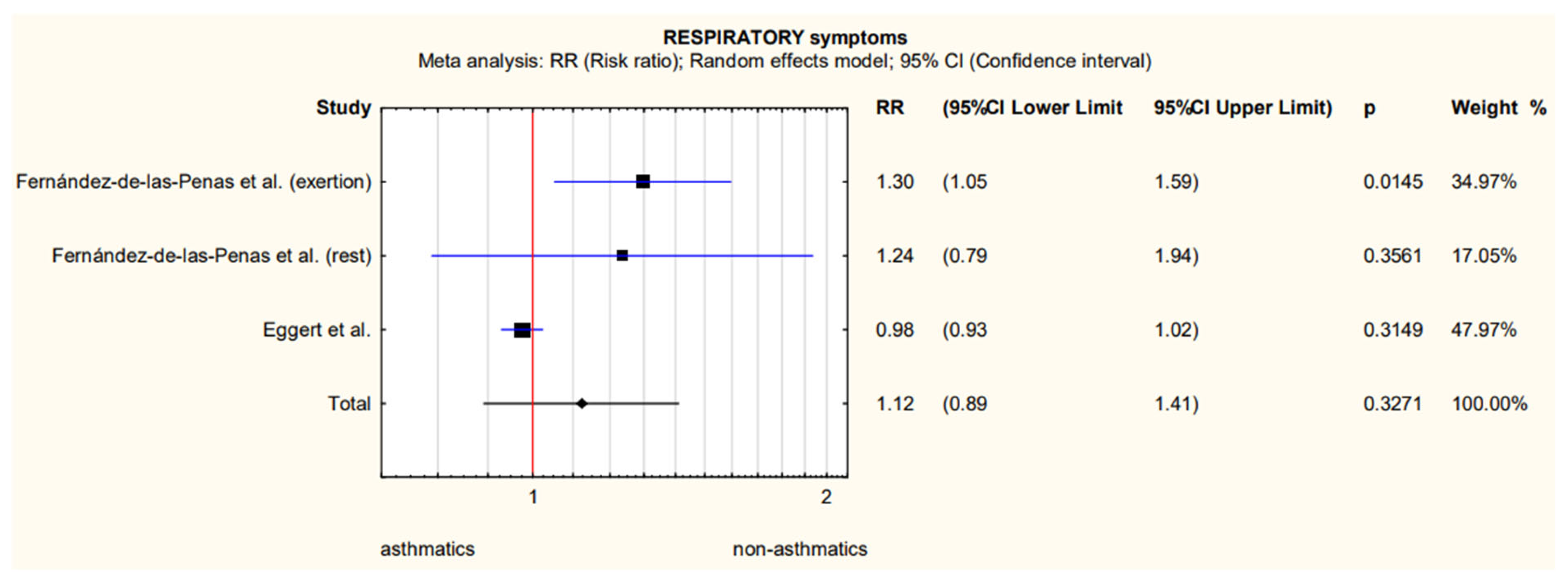
| Q | df | p | T2 | 95% CI (T2) | I2 | 95% CI (I2) |
|---|---|---|---|---|---|---|
| 7.73 | 2 | 0.021 | 0.0280 | 0.0016–0.1161 | 74.13% | 13.72–92.24% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaszuba, M.; Madej, N.; Pilinski, R.; Sliwka, A. Post-COVID-19 Symptoms in Adults with Asthma—Systematic Review. Biomedicines 2023, 11, 2268. https://doi.org/10.3390/biomedicines11082268
Kaszuba M, Madej N, Pilinski R, Sliwka A. Post-COVID-19 Symptoms in Adults with Asthma—Systematic Review. Biomedicines. 2023; 11(8):2268. https://doi.org/10.3390/biomedicines11082268
Chicago/Turabian StyleKaszuba, Marek, Natalia Madej, Rafal Pilinski, and Agnieszka Sliwka. 2023. "Post-COVID-19 Symptoms in Adults with Asthma—Systematic Review" Biomedicines 11, no. 8: 2268. https://doi.org/10.3390/biomedicines11082268
APA StyleKaszuba, M., Madej, N., Pilinski, R., & Sliwka, A. (2023). Post-COVID-19 Symptoms in Adults with Asthma—Systematic Review. Biomedicines, 11(8), 2268. https://doi.org/10.3390/biomedicines11082268