
Insights into Healthcare Professionals’ Perceptions and Attitudes toward Nanotechnological Device Application: What Is the Current Situation in Glioblastoma Research?

 ,
, 
 ,
,  , , ,
, , ,  , , ,
, , ,
Abstract
1. Introduction
2. Glioblastoma and Its Current Treatments
3. Risk Perception of Nanotechnological Devices Application
4. Materials and Methods
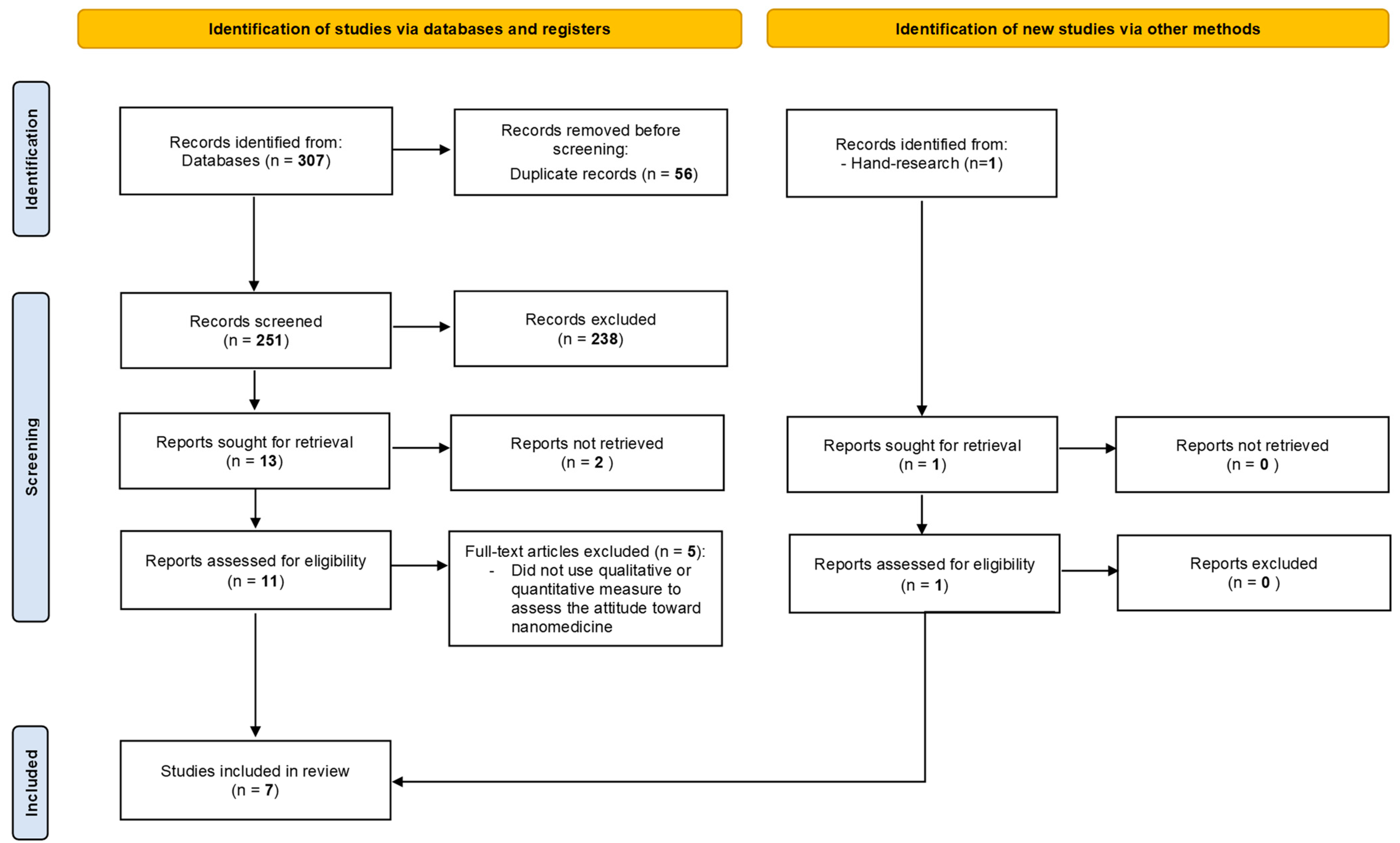
4.1. Search Strategy and Eligibility Criteria
4.2. Study Selection
4.3. Synthesis Analysis
5. Results
5.1. Study Characteristics
5.2. Healthcare Professionals’ Attitude toward Nanomedicine
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Omuro, A.; DeAngelis, L.M. Glioblastoma and Other Malignant Gliomas: A Clinical Review. JAMA 2013, 310, 1842–1850. [Google Scholar] [CrossRef] [PubMed]
- Wirsching, H.-G.; Galanis, E.; Weller, M. Chapter 23—Glioblastoma. In Handbook of Clinical Neurology; Berger, M.S., Weller, M., Eds.; Gliomas; Elsevier: Amsterdam, The Netherlands, 2016; Volume 134, pp. 381–397. [Google Scholar]
- Ostrom, Q.T.; Bauchet, L.; Davis, F.G.; Deltour, I.; Fisher, J.L.; Langer, C.E.; Pekmezci, M.; Schwartzbaum, J.A.; Turner, M.C.; Walsh, K.M.; et al. The Epidemiology of Glioma in Adults: A “State of the Science” Review. Neuro-Oncol. 2014, 16, 896–913. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Sarkaria, J.N.; Hu, L.S.; Parney, I.F.; Pafundi, D.H.; Brinkmann, D.H.; Laack, N.N.; Giannini, C.; Burns, T.C.; Kizilbash, S.H.; Laramy, J.K.; et al. Is the Blood-Brain Barrier Really Disrupted in All Glioblastomas? A Critical Assessment of Existing Clinical Data. Neuro-Oncol. 2018, 20, 184–191. [Google Scholar] [CrossRef]
- Mittal, K.R.; Pharasi, N.; Sarna, B.; Singh, M.; Rachana; Haider, S.; Singh, S.K.; Dua, K.; Jha, S.K.; Dey, A.; et al. Nanotechnology-Based Drug Delivery for the Treatment of CNS Disorders. Transl. Neurosci. 2022, 13, 527–546. [Google Scholar] [CrossRef] [PubMed]
- Manser, T. Teamwork and Patient Safety in Dynamic Domains of Healthcare: A Review of the Literature. Acta Anaesthesiol. Scand. 2009, 53, 143–151. [Google Scholar] [CrossRef]
- Sangaleti, C.; Schveitzer, M.C.; Peduzzi, M.; Zoboli, E.L.C.P.; Soares, C.B. Experiences and Shared Meaning of Teamwork and Interprofessional Collaboration among Health Care Professionals in Primary Health Care Settings: A Systematic Review. JBI Evid. Synth. 2017, 15, 2723–2788. [Google Scholar] [CrossRef]
- Schmutz, J.B.; Meier, L.L.; Manser, T. How Effective Is Teamwork Really? The Relationship between Teamwork and Performance in Healthcare Teams: A Systematic Review and Meta-Analysis. BMJ Open 2019, 9, e028280. [Google Scholar] [CrossRef]
- McGuier, E.A.; Aarons, G.A.; Byrne, K.A.; Campbell, K.A.; Keeshin, B.; Rothenberger, S.D.; Weingart, L.R.; Salas, E.; Kolko, D.J. Associations between Teamwork and Implementation Outcomes in Multidisciplinary Cross-Sector Teams Implementing a Mental Health Screening and Referral Protocol. Implement. Sci. Commun. 2023, 4, 13. [Google Scholar] [CrossRef]
- Batash, R.; Asna, N.; Schaffer, P.; Francis, N.; Schaffer, M. Glioblastoma Multiforme, Diagnosis and Treatment; Recent Literature Review. Curr. Med. Chem. 2017, 24, 3002–3009. [Google Scholar] [CrossRef] [PubMed]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of Brain Metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Ampie, L.; Woolf, E.C.; Dardis, C. Immunotherapeutic Advancements for Glioblastoma. Front. Oncol. 2015, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Colman, H. Adult Gliomas. CONTINUUM Lifelong Learn. Neurol. 2020, 26, 1452. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing Percent Resection and Residual Volume Thresholds Affecting Survival and Recurrence for Patients with Newly Diagnosed Intracranial Glioblastoma. Neuro-Oncol. 2014, 16, 113–122. [Google Scholar] [CrossRef]
- Vivas-Buitrago, T.; Domingo, R.A.; Tripathi, S.; De Biase, G.; Brown, D.; Akinduro, O.O.; Ramos-Fresnedo, A.; Sabsevitz, D.S.; Bendok, B.R.; Sherman, W.; et al. Influence of Supramarginal Resection on Survival Outcomes after Gross-Total Resection of IDH-Wild-Type Glioblastoma. J. Neurosurg. 2022, 136, 1–8. [Google Scholar] [CrossRef]
- Guerrini, F.; Roca, E.; Spena, G. Supramarginal Resection for Glioblastoma: It Is Time to Set Boundaries! A Critical Review on a Hot Topic. Brain Sci. 2022, 12, 652. [Google Scholar] [CrossRef]
- Buatti, J.; Ryken, T.; Smith, M.; Sneed, P.; Suh, J.; Mehta, M.; Olson, J. Radiation Therapy of Pathologically Confirmed Newly Diagnosed Glioblastoma in Adults. J. Neuro-Oncol. 2008, 89, 313–337. [Google Scholar] [CrossRef]
- Ziu, M.; Kim, B.Y.S.; Jiang, W.; Ryken, T.; Olson, J.J. The Role of Radiation Therapy in Treatment of Adults with Newly Diagnosed Glioblastoma Multiforme: A Systematic Review and Evidence-Based Clinical Practice Guideline Update. J. Neurooncol. 2020, 150, 215–267. [Google Scholar] [CrossRef]
- Janjua, T.I.; Rewatkar, P.; Ahmed-Cox, A.; Saeed, I.; Mansfeld, F.M.; Kulshreshtha, R.; Kumeria, T.; Ziegler, D.S.; Kavallaris, M.; Mazzieri, R.; et al. Frontiers in the Treatment of Glioblastoma: Past, Present and Emerging. Adv. Drug Deliv. Rev. 2021, 171, 108–138. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.B.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of Radiotherapy with Concomitant and Adjuvant Temozolomide versus Radiotherapy Alone on Survival in Glioblastoma in a Randomised Phase III Study: 5-Year Analysis of the EORTC-NCIC Trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Lukas, R.V.; Wainwright, D.A.; Ladomersky, E.; Sachdev, S.; Sonabend, A.M.; Stupp, R. Newly Diagnosed Glioblastoma: A Review on Clinical Management. Oncology 2019, 33, 91–100. [Google Scholar]
- Parisi, S.; Corsa, P.; Raguso, A.; Perrone, A.; Cossa, S.; Munafò, T.; Sanpaolo, G.; Donno, E.; Clemente, M.A.; Piombino, M.; et al. Temozolomide and Radiotherapy versus Radiotherapy Alone in High Grade Gliomas: A Very Long Term Comparative Study and Literature Review. Biomed. Res. Int. 2015, 2015, 620643. [Google Scholar] [CrossRef]
- Kaka, N.; Hafazalla, K.; Samawi, H.; Simpkin, A.; Perry, J.; Sahgal, A.; Das, S. Progression-Free but No Overall Survival Benefit for Adult Patients with Bevacizumab Therapy for the Treatment of Newly Diagnosed Glioblastoma: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1723. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.-C.; Hu, Z.-Q.; Long, J.-H.; Zhu, G.-M.; Wang, Y.; Jia, Y.; Zhou, J.; Ouyang, Y.; Zeng, Z. Clinical Implications of Tumor-Infiltrating Immune Cells in Breast Cancer. J. Cancer 2019, 10, 6175–6184. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.C.; Ashley, D.M.; López, G.Y.; Malinzak, M.; Friedman, H.S.; Khasraw, M. Management of Glioblastoma: State of the Art and Future Directions. CA A Cancer J. Clin. 2020, 70, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Suchorska, B.; Weller, M.; Tabatabai, G.; Senft, C.; Hau, P.; Sabel, M.C.; Herrlinger, U.; Ketter, R.; Schlegel, U.; Marosi, C.; et al. Complete Resection of Contrast-Enhancing Tumor Volume Is Associated with Improved Survival in Recurrent Glioblastoma—Results from the DIRECTOR Trial. Neuro-Oncol. 2015, 18, 549–556. [Google Scholar] [CrossRef]
- Ryu, S.; Buatti, J.M.; Morris, A.; Kalkanis, S.N.; Ryken, T.C.; Olson, J.J. The Role of Radiotherapy in the Management of Progressive Glioblastoma: A Systematic Review and Evidence-Based Clinical Practice Guideline. J. Neurooncol. 2014, 118, 489–499. [Google Scholar] [CrossRef]
- Lombardi, G.; Salvo, G.L.D.; Brandes, A.A.; Eoli, M.; Rudà, R.; Faedi, M.; Lolli, I.; Pace, A.; Daniele, B.; Pasqualetti, F.; et al. Regorafenib Compared with Lomustine in Patients with Relapsed Glioblastoma (REGOMA): A Multicentre, Open-Label, Randomised, Controlled, Phase 2 Trial. Lancet Oncol. 2019, 20, 110–119. [Google Scholar] [CrossRef]
- Wick, W.; Gorlia, T.; Bendszus, M.; Taphoorn, M.; Sahm, F.; Harting, I.; Brandes, A.A.; Taal, W.; Domont, J.; Idbaih, A.; et al. Lomustine and Bevacizumab in Progressive Glioblastoma. N. Engl. J. Med. 2017, 377, 1954–1963. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Klockow, J.L.; Zhang, M.; Lafortune, F.; Chang, E.; Jin, L.; Wu, Y.; Daldrup-Link, H.E. Glioblastoma multiforme (GBM): An overview of current therapies and mechanisms of resistance. Pharmacol Res. 2021, 171, 105780. [Google Scholar] [CrossRef]
- Allan, J.; Belz, S.; Hoeveler, A.; Hugas, M.; Okuda, H.; Patri, A.; Rauscher, H.; Silva, P.; Slikker, W.; Sokull-Kluettgen, B.; et al. Regulatory Landscape of Nanotechnology and Nanoplastics from a Global Perspective. Regul. Toxicol. Pharmacol. 2021, 122, 104885. [Google Scholar] [CrossRef] [PubMed]
- Schulte, P.A.; Geraci, C.L.; Murashov, V.; Kuempel, E.D.; Zumwalde, R.D.; Castranova, V.; Hoover, M.D.; Hodson, L.; Martinez, K.F. Occupational Safety and Health Criteria for Responsible Development of Nanotechnology. J. Nanopart. Res. 2014, 16, 2153. [Google Scholar] [CrossRef]
- Slovic, P.; Fischhoff, B.; Lichtenstein, S. Why Study Risk Perception? Risk Anal. 1982, 2, 83–93. [Google Scholar] [CrossRef]
- Fischoff, B.; Lichtenstein, S. Don’t Attribute This to Reverend Bayes. Psychol. Bull. 1978, 85, 239–243. [Google Scholar] [CrossRef]
- Tversky, A.; Kahneman, D. Judgment under Uncertainty: Heuristics and Biases. Science 1974, 185, 1124–1131. [Google Scholar] [CrossRef]
- Kahneman, D.; Tversky, A. Prospect Theory: An Analysis of Decision under Risk. Econometrica 1979, 47, 263–291. [Google Scholar] [CrossRef]
- Sjöberg, L.; Winroth, E. Risk, Moral Value of Actions, and Mood. Scand. J. Psychol. 1986, 27, 191–208. [Google Scholar] [CrossRef]
- Sjöberg, L. Emotions and Risk Perception. Risk Manag. 2007, 9, 223–237. [Google Scholar] [CrossRef]
- Brown, V.J. Risk Perception: It’s Personal. Environ. Health Perspect. 2014, 122, A276–A279. [Google Scholar] [CrossRef]
- Lee, C.-J.; Scheufele, D.A.; Lewenstein, B.V. Public Attitudes toward Emerging Technologies: Examining the Interactive Effects of Cognitions and Affect on Public Attitudes toward Nanotechnology. Sci. Commun. 2005, 27, 240–267. [Google Scholar] [CrossRef]
- Cacciatore, M.A.; Scheufele, D.A.; Corley, E. From Enabling Technology to Applications: The Evolution of Risk Perceptions about Nanotechnology. Public Underst. Sci. 2011, 20, 385–404. [Google Scholar] [CrossRef]
- Ganesh Pillai, R.; Bezbaruah, A.N. Perceptions and Attitude Effects on Nanotechnology Acceptance: An Exploratory Framework. J. Nanopart. Res. 2017, 19, 41. [Google Scholar] [CrossRef]
- George, S.; Kaptan, G.; Lee, J.; Frewer, L. Awareness on Adverse Effects of Nanotechnology Increases Negative Perception among Public: Survey Study from Singapore. J. Nanopart. Res. 2014, 16, 2751. [Google Scholar] [CrossRef]
- Kim, Y.-R.; Lee, E.J.; Park, S.H.; Kwon, H.J.; An, S.S.A.; Son, S.W.; Seo, Y.R.; Pie, J.-E.; Yoon, M.; Kim, J.H.; et al. Interactive Survey of Consumer Awareness of Nanotechnologies and Nanoparticles in Consumer Products in South Korea. Int. J. Nanomed. 2014, 9, 11–20. [Google Scholar] [CrossRef]
- Larsson, S.; Jansson, M.; Boholm, Å. Expert Stakeholders’ Perception of Nanotechnology: Risk, Benefit, Knowledge, and Regulation. J. Nanopart. Res. 2019, 21, 57. [Google Scholar] [CrossRef]
- Chaturvedi, V.K.; Singh, A.; Singh, V.K.; Singh, M.P. Cancer Nanotechnology: A New Revolution for Cancer Diagnosis and Therapy. Curr. Drug Metab. 2019, 20, 416–429. [Google Scholar] [CrossRef]
- Nasir, A.; Khan, A.; Li, J.; Naeem, M.; Khalil, A.A.K.; Khan, K.; Qasim, M. Nanotechnology, A Tool for Diagnostics and Treatment of Cancer. Curr. Top. Med. Chem. 2021, 21, 1360–1376. [Google Scholar] [CrossRef]
- Lam, F.C.; Salehi, F.; Kasper, E.M. Integrating Nanotechnology in Neurosurgery, Neuroradiology, and Neuro-Oncology Practice-The Clinicians’ Perspective. Front. Bioeng. Biotechnol. 2022, 10, 801822. [Google Scholar] [CrossRef]
- Karthikeyan, H.; Vishnu Priya, V.; Gayathri, R. Awareness on Use of Nanoparticles among Medical Professionals. Drug Invent. Today 2018, 10, 1906–1909. [Google Scholar]
- Maldhure, S.; Sonwani, V.; Ambad, R.; Chandi, D.H. Awareness about Nanotechnology among Upcoming Clinicians in Vidarbha, Maharashtra. J. Pharm. Res. Int. 2021, 33, 126–131. [Google Scholar] [CrossRef]
- Ibrahim, N. Hospital Workers Perceptions about Nano-Technology. Eur. J. Oncol. Pharm. 2011, 5, 35–36. [Google Scholar]
- Friedman, A.; Nasir, A. Nanotechnology and Dermatology Education in the United States: Data from a Pilot Survey. J. Drugs Dermatol. 2011, 10, 1037–1041. [Google Scholar] [PubMed]
- Nassani, N.; El-Douaihy, Y.; Khotsyna, Y.; Shwe, T.; El-Sayegh, S. Knowledge, Perceptions, and Attitudes of Medical Residents Towards Nanomedicine: Defining the Gap. Med. Sci. Educ. 2020, 30, 179–186. [Google Scholar] [CrossRef]
- Xenaki, V.; Costea, D.E.; Marthinussen, M.C.; Cimpan, M.R.; Åstrøm, A.N. Use of Nanomaterials in Dentistry: Covariates of Risk and Benefit Perceptions among Dentists and Dental Hygienists in Norway. Acta Odontol. Scand. 2020, 78, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Xenaki, V.; Marthinussen, M.C.; Costea, D.E.; Breivik, K.; Lie, S.A.; Cimpan, M.R.; Åstrøm, A.N. Predicting Intention of Norwegian Dental Health-Care Workers to Use Nanomaterials: An Application of the Augmented Theory of Planned Behavior. Eur. J. Oral Sci. 2021, 129, e12821. [Google Scholar] [CrossRef] [PubMed]
- El Saghir, N.S.; Charara, R.N.; Kreidieh, F.Y.; Eaton, V.; Litvin, K.; Farhat, R.A.; Khoury, K.E.; Breidy, J.; Tamim, H.; Eid, T.A. Global Practice and Efficiency of Multidisciplinary Tumor Boards: Results of an American Society of Clinical Oncology International Survey. JGO 2015, 1, 57–64. [Google Scholar] [CrossRef]
- Gaudino, S.; Giordano, C.; Magnani, F.; Cottonaro, S.; Infante, A.; Sabatino, G.; La Rocca, G.; Della Pepa, G.M.; D’Alessandris, Q.G.; Pallini, R.; et al. Neuro-Oncology Multidisciplinary Tumor Board: The Point of View of the Neuroradiologist. J. Pers. Med. 2022, 12, 135. [Google Scholar] [CrossRef]
- Ajzen, I. From Intentions to Actions: A Theory of Planned Behavior. In Action Control: From Cognition to Behavior; Kuhl, J., Beckmann, J., Eds.; SSSP Springer Series in Social Psychology; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. ISBN 978-3-642-69746-3. [Google Scholar]
- Barton, A.E.; Borchard, G.; Wacker, M.G.; Pastorin, G.; Saleem, I.Y.; Chaudary, S.; Elbayoumi, T.; Zhao, Z.; Flühmann, B. Need for Expansion of Pharmacy Education Globally for the Growing Field of Nanomedicine. Pharmacy 2022, 10, 17. [Google Scholar] [CrossRef]


{kind=link}
| Treatment | Strengths | Weaknesses |
|---|---|---|
| Newly diagnosed Glioblastoma | ||
| Surgery |
|
|
| Radiation therapy (RT) |
|
|
| Temozolomide (TMZ) chemotherapy |
|
|
| Tumor-treating fields (TTFields) |
|
|
| Bevacizumab |
|
|
| Recurrent Glioblastoma | ||
| Further surgical resection |
|
|
| Re-irradiation |
|
|
| Lomustine |
|
|
| Regorafenib |
|
|
| First Author | Year | Country | Study Design | Recruitment Setting | Sample Size | Age | Job Profile | Previous Use or Literacy in Nanomaterials | Type of Measure | No. of Items | Theoretical Framework | Aim of the Study |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Maldhure, S. | 2021 | India | Cross-sectional | Datta Meghe Medical College and Shalinitai Meghe Hospital | 56 | Not reported | Residents from the Departments of Medicine, Psychiatry, Dermatology, General Surgery, Orthopedics, Ophthalmology, ENT, Pediatrics and Obstetrics, Gynecology | 14.3% | Self-administered questionnaire | 8 | Not reported | Collect information on awareness and knowledge about nanotechnology in upcoming clinicians. |
| Xenaki, V. | 2019 | Norway | Cross-sectional | Public Dental Health Service in Norway | 791 | 22–70 | Dentists and dental hygienists | 46% | Self-administered questionnaire | 20 | Not reported | Assess whether socio-demographic factors, familiarity with nanotechnology, and social trust are associated with dental healthcare workers’ perceived risks and benefits of the use of nanomaterials in dentistry and whether those associations varied according to the professional status. |
| Xenaki, V. | 2020 | Norway | Cross-sectional | Public dental healthcare service | 851 | 41.5 ± 11.9 | Dentists and dental hygienists | 54% | Self- administered an online questionnaire | 28 | Theory of Planned Behavior (TPB) | Predict the intention of dental healthcare workers to use nanomaterials in the future and explore whether the augmented TPB model operates equivalently across the professional groups of dentists and dental hygienists. |
| Nassani, N. | 2019 | USA | Cross-sectional | Staten IslandUniversity Hospital | 70 | 29(range 25–35) | Postgraduate training internal medicine residents | 8% | Self-administered questionnaire | 35 | Not reported | Evaluate the perception, knowledge, and attitude of medical residents toward nanomedicine. |
| Karthikeyan, H. | 2018 | India | Cross-sectional | Not reported | 70 | Not reported | Students in undergraduate and postgraduate teaching faculties and practitioners in dentistry and medicine | Not reported | Self- administered an online questionnaire | Not reported | Not reported | Create awareness of nanoparticles and their usage among professionals. |
| Ibrahim, N | 2011 | Saudi Arabia | Cross-sectional | Riyadh Military Hospital | 300 | 18–60 | Hospital employees and trainees | Not reported | Self-administered questionnaire | 9 | Not reported | Measure hospital workers’ awareness, perceptions, and preferences of nanotechnology and correlate them with existing demographic data. |
| Friedman, A. and Nasir, A. | 2011 | USA | Cross-sectional | Department of Dermatology | 23 | Not reported | Faculty and chief residents of dermatology training programs | 30.4% | Self- administered an online questionnaire | 21 | Absent | Obtain specific information regarding dermatology knowledge, attitudes, and perceptions of nanotechnology. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ragucci, F.; Sireci, F.; Cavallieri, F.; Rossi, J.; Biagini, G.; Tosi, G.; Lucchi, C.; Molina-Pena, R.; Ferreira, N.H.; Zarur, M.; et al. Insights into Healthcare Professionals’ Perceptions and Attitudes toward Nanotechnological Device Application: What Is the Current Situation in Glioblastoma Research? Biomedicines 2023, 11, 1854. https://doi.org/10.3390/biomedicines11071854
Ragucci F, Sireci F, Cavallieri F, Rossi J, Biagini G, Tosi G, Lucchi C, Molina-Pena R, Ferreira NH, Zarur M, et al. Insights into Healthcare Professionals’ Perceptions and Attitudes toward Nanotechnological Device Application: What Is the Current Situation in Glioblastoma Research? Biomedicines. 2023; 11(7):1854. https://doi.org/10.3390/biomedicines11071854
Chicago/Turabian StyleRagucci, Federica, Francesca Sireci, Francesco Cavallieri, Jessica Rossi, Giuseppe Biagini, Giovanni Tosi, Chiara Lucchi, Rodolfo Molina-Pena, Natalia Helen Ferreira, Mariana Zarur, and et al. 2023. "Insights into Healthcare Professionals’ Perceptions and Attitudes toward Nanotechnological Device Application: What Is the Current Situation in Glioblastoma Research?" Biomedicines 11, no. 7: 1854. https://doi.org/10.3390/biomedicines11071854
APA StyleRagucci, F., Sireci, F., Cavallieri, F., Rossi, J., Biagini, G., Tosi, G., Lucchi, C., Molina-Pena, R., Ferreira, N. H., Zarur, M., Ferreiros, A., Bourgeois, W., Berger, F., Abal, M., Rousseau, A., Boury, F., Alvarez-Lorenzo, C., Garcion, E., Pisanello, A., ... Valzania, F. (2023). Insights into Healthcare Professionals’ Perceptions and Attitudes toward Nanotechnological Device Application: What Is the Current Situation in Glioblastoma Research? Biomedicines, 11(7), 1854. https://doi.org/10.3390/biomedicines11071854