
Prevalence and Contextual Factors of Juvenile Fibromyalgia in a Population-Based Italian Sample of Children and Adolescents



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
- relationship with peers (“very good”, “quite good”, “quite bad”, “very bad”, “don’t know”);
- relationship with parents (“very good”, “quite good”, “quite bad”, “very bad”, “don’t know”);
- school performance (“very good”, “quite good”, “quite bad”, “very bad”, “don’t know”);
- being bullied (“yes”, “no”, “don’t know”).
- pain in the previous week, in each of the identified body areas for FM (“yes”, “no”);
- severity of the pain (VAS: from 0—no pain to 10—very severe);
- level of severity fatigue, waking unrefreshed, and cognitive symptoms experienced over the previous week using the following scale: “no symptoms”, “slight or mild problems, generally mild or intermittent”, “moderate, considerable problems, often present and/or at a moderate level”, “severe, pervasive, continuous, life-disturbing problems”);
- other symptoms (fatigue, difficulties in sleeping, difficulties in thinking and remembering, difficulties in studying, headache, anxiety and nervousness, depression or melancholy, diarrhea or constipation, abdominal pain or bloating, itching, rash or hives, skin’s sensitivity to the sun, nausea or heartburn, cold hands and feet, swelling sensation in the hands, palpitations, chest pain, dizziness, shortness of breath, cramps, muscle weakness in the legs, mild fever, painful menstruation, muscle stiffness especially in the morning, shaking of the legs in bed, tingling, numbness, pain modulation by physical activities, pain modulation by weather factors, pain modulation by anxiety or stress; for each, “yes”, “no”);
- having had road accidents (“yes”, “no”);
- having had injury in the leisure time that led to persistent pain (“yes”, “no”);
- having had surgery (“yes”, “no”).
- cohabiting parents (“yes”, “no”);
- suffering from diffuse pain (“yes”, “no”);
- having had a diagnosis of fibromyalgia (“yes”, “no”);
- using or having used psychotropic drugs (“yes”, “no”).
2.3. Selection of Children Who Met Fibromyalgia Criteria
- for 2010 and 2016 ACR criteria, waking unrefreshed, cognition, fatigue. For each of them, the level of severity over the past week was considered: “0” for no problem, “1” for slight or mild problems, generally mild or intermittent, “2” for moderate, considerable problems, often present and/or at a moderate level, “3” for severe, pervasive, continuous, life-disturbing problems;
- for 2010 ACR criteria, somatic symptoms in general: “0” for no symptoms, “1” for few symptoms, “2” for a moderate number of symptoms, “3” for a great deal of symptoms;
- for 2016 ACR criteria, the number of the following symptoms the patient has been suffering during the previous 6 months (“0” for no, “1” for yes): headaches, pain or cramps in lower abdomen, depression.
- WPI ≥ 7 and SSS score ≥ 5 or WPI ranged between 3 and 6 and SSS score ≥ 9,
- symptoms have been present at a similar level for at least 3 months,
- he/she does not have a disorder that would otherwise explain the pain.
- WPI ≥ 7 and SSS score ≥ 5 or WPI ranged 4–6 and SSS score ≥ 9,
- generalized pain, defined as pain in at least 4 of 5 regions (not including jaw, chest, and abdominal pain),
- symptoms have been lasting for at least 3 months.
2.4. Statistical Analyses
3. Results
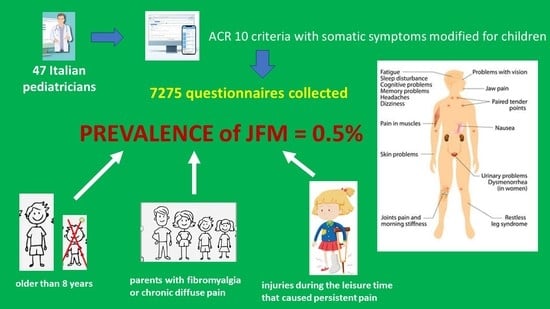
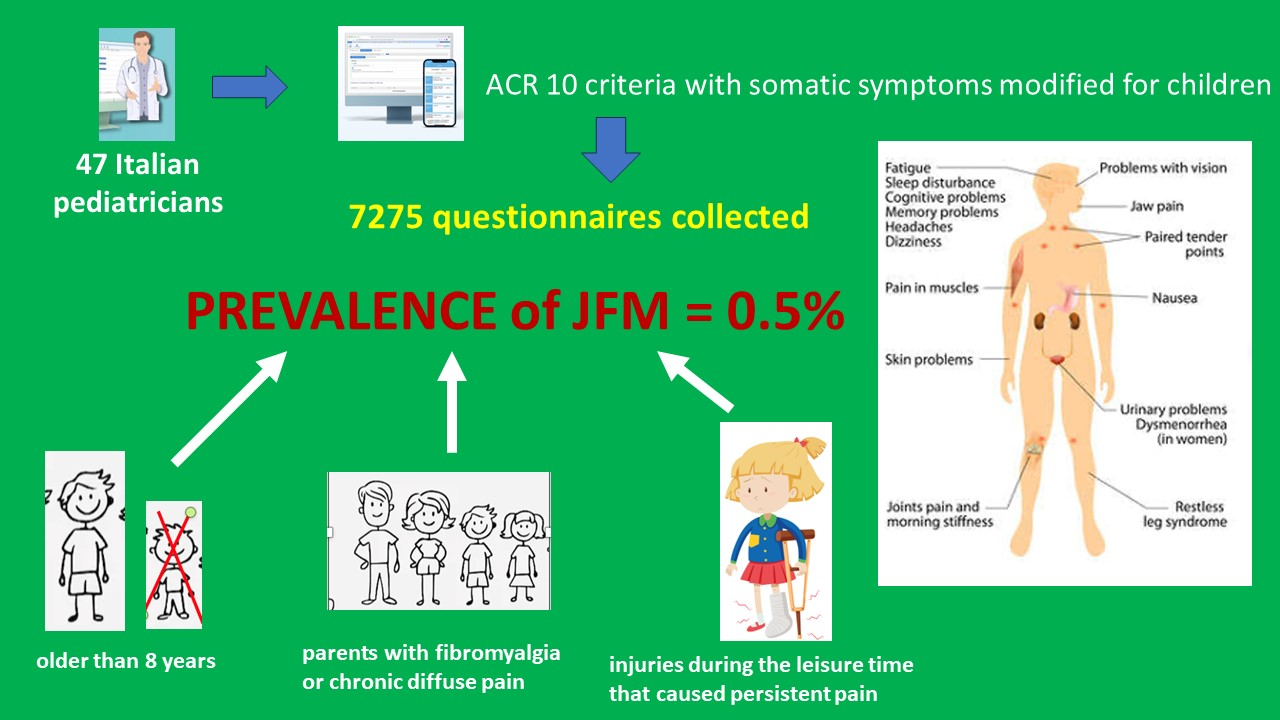
3.1. Prevalence of JFM
3.2. Association with Contextual Factors: Predictors of Compliance with ACR Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnold, L.M.; Clauw, D.J.; McCarberg, B.H.; Fibro Collaborative. Improving the recognition and diagnosis of fibromyalgia. Mayo Clin. Proc. 2011, 86, 457–464. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Kashikar-Zuck, S.; King, C.; Ting, T.V.; Arnold, L.M. Juvenile Fibromyalgia: Different from the Adult Chronic Pain Syndrome? Curr. Rheumatol. Rep. 2016, 18, 19. [Google Scholar] [CrossRef]
- Yunus, M.B.; Masi, A.T. Juvenile primary fibromyalgia syndrome. A clinical study of thirty-three patients and matched normal controls. Arthritis Rheum. 1985, 28, 138–145. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, V.; Abbasciano, V.; Soliman, A.T.; Soliman, N.; Di Maio, S.; Fiscina, B.; Kattamis, C. The juvenile fibromyalgia syndrome (JFMS): A poorly defined disorder. Acta Biomed. 2019, 90, 134–148. [Google Scholar] [CrossRef] [PubMed]
- Kashikar-Zuck, S.; Cunningham, N.; Sil, S.; Bromberg, M.H.; Lynch-Jordan, A.M.; Strotman, D.; Peugh, J.; Noll, J.; Ting, T.V.; Powers, S.W.; et al. Long-term outcomes of adolescents with juvenile-onset fibromyalgia in early adulthood. Pediatrics 2014, 133, e592–e600. [Google Scholar] [CrossRef] [PubMed]
- Walitt, B.; Fitzcharles, M.A.; Hassett, A.L.; Katz, R.S.; Häuser, W.; Wolfe, F. The longitudinal outcome of fibromyalgia: A study of 1555 patients. J. Rheumatol. 2011, 38, 2238–2246. [Google Scholar] [CrossRef]
- Kashikar-Zuck, S.; Zafar, M.; Barnett, K.A.; Aylward, B.S.; Strotman, D.; Slater, S.K.; Allen, J.R.; Lecates, S.L.; Kabbouche, M.A.; Ting, T.V.; et al. Quality of life and emotional functioning in youth with chronic migraine and juvenile fibromyalgia. Clin. J. Pain. 2013, 29, 1066–1072. [Google Scholar] [CrossRef]
- Kashikar-Zuck, S.; Johnston, M.; Ting, T.V.; Graham, B.T.; Lynch-Jordan, A.M.; Verkamp, E.; Passo, M.; Schikler, K.N.; Hashkes, P.J.; Spalding, S.; et al. Relationship between school absenteeism and depressive symptoms among adolescents with juvenile fibromyalgia. J. Pediatr. Psychol. 2010, 35, 996–1004. [Google Scholar] [CrossRef]
- Clark, P.; Burgos-Vargas, R.; Medina-Palma, C.; Lavielle, P.; Marina, F.F. Prevalence of fibromyalgia in children: A clinical study of Mexican children. J. Rheumatol. 1998, 25, 2009–2014. [Google Scholar]
- Buskila, D.; Press, J.; Gedalia, A.; Klein, M.; Neumann, L.; Boehm, R.; Sukenik, S. Assessment of nonarticular tenderness and prevalence of fibromyalgia in children. J. Rheumatol. 1993, 20, 368–370. [Google Scholar] [PubMed]
- Weir, P.T.; Harlan, G.A.; Nkoy, F.L.; Jones, S.S.; Hegmann, K.T.; Gren, L.H.; Lyon, J.L. The incidence of fibromyalgia and its associated comorbidities: A population-based retrospective cohort study based on International Classification of Diseases, 9th Revision codes. Clin. Rheumatol. 2006, 12, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Sil, S.; Lynch-Jordan, A.; Ting, T.V.; Peugh, J.; Noll, J.; Kashikar-Zuck, S. Influence of family environment on long-term psychosocial functioning of adolescents with juvenile fibromyalgia. Arthritis Care Res. 2013, 65, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Gerloni, V.; Ghirardini, M.; Fantini, F. Assessment of nonarticular tenderness and prevalence of primary fibromyalgia syndrome in healthy Italian school children. Arthritis Reum. 1998, 41, S267. [Google Scholar]
- Ting, T.V.; Barnett, K.; Lynch-Jordan, A.; Whitacre, C.; Henrickson, M.; Kashikar-Zuck, S. 2010 American College of Rheumatology Adult Fibromyalgia Criteria for Use in an Adolescent Female Population with Juvenile Fibromyalgia. J. Pediatr. 2016, 169, 181–187.e1. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.L.; Tress, J.; Sherry, D.D. Trends in Medicalization of Children with Amplified Musculoskeletal Pain Syndrome. Pain Med. 2017, 18, 825–831. [Google Scholar] [CrossRef]
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part. II. Arthritis Rheum. 2008, 58, 26–35. [Google Scholar] [CrossRef]
- Eraso, R.N.; Bradford, N.J.; Fontenot, C.N.; Espinoza, L.R.; Gedalia, A. Fibromyalgia syndrome in young children: Onset at age 10 years and younger. Clin. Exp. Rheumatol. 2007, 25, 639–644. [Google Scholar]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.M.; Janeway, D.; Baum, J. Fibromyalgia syndrome in children and adolescents: Clinical features at presentation and status at follow-up. Pediatrics 1998, 101, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Gedalia, A.; García, C.O.; Molina, J.F.; Bradford, N.J.; Espinoza, L.R. Fibromyalgia syndrome: Experience in a pediatric rheumatology clinic. Clin. Exp. Rheumatol. 2000, 18, 415–419. [Google Scholar]
- Uziel, Y.; Chapnick, G.; Jaber, L.; Nemet, D.; Hashkes, P.J. Five-year outcome of children with “growing pains”: Correlations with pain threshold. J. Pediatr. 2010, 156, 838–840. [Google Scholar] [CrossRef] [PubMed]
- Buskila, D.; Neumann, L.; Hazanov, I.; Carmi, R. Familial aggregation in the fibromyalgia syndrome. Semin. Arthritis Rheum. 1996, 26, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Hudson, J.I.; Hess, E.V.; Ware, A.E.; Fritz, D.A.; Auchenbach, M.B.; Starck, L.O.; Keck, P.E., Jr. Family study of fibromyalgia. Arthritis Rheum. 2004, 50, 944–952. [Google Scholar] [CrossRef]
- Roizenblatt, S.; Tufik, S.; Goldenberg, J.; Pinto, L.R.; Hilario, M.O.; Feldman, D. Juvenile fibromyalgia: Clinical and polysomnographic aspects. J. Rheumatol. 1997, 24, 579–585. [Google Scholar]
- Nelson, S.; Cunningham, N.; Peugh, J.; Jagpal, A.; Arnold, L.M.; Lynch-Jordan, A.; Kashikar-Zuck, S. Clinical Profiles of Young Adults with Juvenile-Onset Fibromyalgia with and Without a History of Trauma. Arthritis Care Res. 2017, 69, 1636–1643. [Google Scholar] [CrossRef]
- Sendur, O.F.; Gurer, G.; Bozbas, G.T. The frequency of hypermobility and its relationship with clinical findings of fibromyalgia patients. Clin. Rheumatol. 2007, 26, 485–487. [Google Scholar] [CrossRef]
- Imbierowicz, K.; Egle, U.T. Childhood adversities in patients with fibromyalgia and somatoform pain disorder. Eur. J. Pain. 2003, 7, 113–119. [Google Scholar] [CrossRef]
- Schanberg, L.E.; Keefe, F.J.; Lefebvre, J.C.; Kredich, D.W.; Gil, K.M. Social context of pain in children with Juvenile Primary Fibromyalgia Syndrome: Parental pain history and family environment. Clin. J. Pain. 1998, 14, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Kashikar-Zuck, S.; Lynch, A.M.; Slater, S.; Graham, T.B.; Swain, N.F.; Noll, R.B. Family factors, emotional functioning, and functional impairment in juvenile fibromyalgia syndrome. Arthritis Rheum. 2008, 59, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Kashikar-Zuck, S.; Lynch, A.M.; Graham, T.B.; Swain, N.F.; Mullen, S.M.; Noll, R.B. Social functioning and peer relationships of adolescents with juvenile fibromyalgia syndrome. Arthritis Rheum. 2007, 57, 474–480. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Whole Sample n = 7275 n (%) | 2010 ACR | 2016 ACR | |||||
|---|---|---|---|---|---|---|---|---|
| Positive n = 38 n (%) | Negative n = 7237 n (%) | p * | Positive n = 4 n (%) | Negative n = 7271 n (%) | p * | |||
| Sex | Male | 3750 (51.5) | 16 (42.1%) | 3734 (51.6) | 0.258 | 1 (25%) | 3749 (51.6) | 0.360 |
| Female | 3525 (48.5) | 22 (57.9%) | 3503 (48.4) | 3 (75%) | 3522 (48.4) | |||
| Age | <8 years old | 3521 (48.3) | 7 (18.4%) | 3505 (48.4) | <0.001 | 3511 (48.3) | 1 (25%) | 0.626 |
| ≥8 years old | 3763 (51.7) | 31 (81.6%) | 3732 (51.6) | 3760 (51.7) | 3 (75%) | |||
| Areas with pain over the previous week | Shoulder girdle, left | 32 (0.4) | 5 (13.2) | 27 (0.4) | <0.001 | 2 (50) | 30 (0.4) | <0.001 |
| Shoulder girdle, right | 38 (0.5) | 5 (13.2) | 33 (0.5) | <0.001 | 2 (50) | 36 (0.5) | <0.001 | |
| Upper arm, left | 36 (0.5) | 5 (13.2) | 31 (0.4) | <0.001 | 3 (75) | 33 (0.5) | <0.001 | |
| Upper arm, right | 33 (0.5) | 11 (28.9) | 22 (0.3) | <0.001 | 3 (75) | 30 (0.4) | <0.001 | |
| Lower arm, left | 6 (0.1) | 1 (2.6) | 5 (0,1) | 0.031 | 0 (0) | 6 (0.1) | 1 | |
| Lower arm, right | 11 (0.2) | 1 (2.6) | 10 (0.1) | 0.056 | 0 (0) | 11 (0.2) | 1 | |
| Hip (buttock, trochanter), left | 23 (0.3) | 4 (10.5) | 19 (0.3) | <0.001 | 1 (25) | 22 (0.3) | 0.013 | |
| Hip (buttock, trochanter), right | 32 (0.4) | 6 (15.8) | 26 (0.4) | <0.001 | 1 (25) | 31 (0.4) | 0.017 | |
| Upper leg, left | 48 (0.7) | 8 (21.1) | 40 (0.6) | <0.001 | 1 (25) | 47 (0.6) | 0.026 | |
| Upper leg, right | 54 (0.8) | 9 (23.7) | 45 (0.6) | <0.001 | 1 (25) | 53 (0.7) | 0.029 | |
| Lower leg, left | 253 (3.5) | 18 (47.4) | 235 (3.2) | <0.001 | 3 (75) | 250 (3.4) | <0.001 | |
| Lower leg, right | 291 (4) | 20 (52.6) | 271 (3.7) | <0.001 | 3 (75) | 288 (4) | <0.001 | |
| Jaw, left | 22 (0.3) | 6 (15.8) | 16 (0.2) | <0.001 | 1 (25) | 21 (0.3) | 0.012 | |
| Jaw, right | 18 (0.2) | 5 (13.2) | 13 (0.2) | <0.001 | 0 (0) | 18 (0.2) | 1 | |
| Chest | 112 (1.5) | 11 (28.9) | 101 (1.4) | <0.001 | 0 (0) | 112 (1.5) | 1 | |
| Abdomen | 264 (3.6) | 20 (52.6) | 244 (3.4) | <0.001 | 3 (75) | 261 (3.6) | <0.001 | |
| Upper back | 57 (0.8) | 11 (28.9) | 46 (0.6) | <0.001 | 2 (50) | 55 (0.8) | <0.001 | |
| Lower back | 98 (1.3) | 11 (28.9) | 87 (1.2) | <0.001 | 2 (50) | 98 (1.3) | 1 | |
| Neck | 124 (1.7) | 12 (31.6) | 112 (1.5) | <0.001 | 0 (0) | 124 (1.7) | 1 | |
| Fatigue | No symptoms | 6564 (90.2) | 1 (2.6) | 5916 (81.7) | <0.001 | 0 (0) | 5917 (81.4) | 0.001 |
| Slight or mild problems, generally mild or intermittent | 593 (8.2) | 16 (42.1) | 578 (8) | <0.001 | 2 (50) | 592 (8.1) | 0.036 | |
| Moderate, considerable problems, often present and/or at a moderate level | 107 (1.5) | 20 (52.6) | 87 (1.2) | <0.001 | 2 (50) | 105 (1.4) | 0.001 | |
| Severe, pervasive, continuous, life-disturbing problems | 10 (0.1) | 1 (2.6) | 9 (0.1) | 0.051 | 0 (0) | 10 (0.1) | 1 | |
| Waking unrefreshed | No symptoms | 5724 (78.7) | 2 (5.3) | 5053 (69.8) | <0.001 | 0 (0) | 5054 (69.5) | 0.088 |
| Slight or mild problems, generally mild or intermittent | 1265 (17.4) | 8 (21.1) | 1261 (17.4) | 0.668 | 2 (50) | 1269 (17.5) | 0.607 | |
| Moderate, considerable problems, often present and/or at a moderate level | 241 (3.3) | 22 (57.9) | 219 (3) | <0.001 | 1 (25) | 239 (3.3) | 0.006 | |
| Severe, pervasive, continuous, life-disturbing problems | 45 (0.6) | 6 (15.8) | 39 (0.5) | <0.001 | 1 (25) | 44 (0.6) | 0.025 | |
| Cognitive symptoms | No symptoms | 6201 (85.3) | 4 (10.5) | 5490 (75.9) | <0.001 | 0 (0) | 5494 (75.6) | 0.004 |
| Slight or mild problems, generally mild or intermittent | 831 (11.4) | 17 (44.7) | 815 (11.3) | <0.001 | 2 (50) | 830 (11.4) | 0.067 | |
| Moderate, considerable problems, often present and/or at a moderate level | 206 (2.8) | 12 (31.6) | 195 (2.7) | <0.001 | 2 (50) | 205 (2.8) | 0.005 | |
| Severe, pervasive, continuous, life-disturbing problems | 37 (0.5) | 5 (13.2) | 32 (0.4) | <0.001 | 0 | 37 (0.5) | 1 | |
| Variables | 2010 ACR Criteria | 2016 ACR Criteria | Whole Sample | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive n = 38 | Negative n = 7237 | p * | Positive n = 4 | Negative n = 7271 | p * | |||||||
| Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | Mean ± SD | Median (IQR) | |||
| WPI | 4.5 ± 1.6 | 4 (3–5) | 0.2 ± 0.6 | 0 (0) | <0.001 | 6.5 ± 1.7 | 7 (4.7–7.7) | 0.2 ± 0.6 | 0 (0) | <0.001 | 0.2 ± 0.65 | 0 (0) |
| SSS score | 7.5 ± 1.4 | 7 (7–8) | 1.2 ± 1.5 | 1 (0–2) | <0.001 | 7.2 ± 1.3 | 7 (6.2–8.5) | 1.2 ± 1.6 | 1 (0–2) | <0.001 | 1.2 ± 1.6 | 1 (0–2) |
| VAS score | 5.8 ± 1.4 | 6 (5–7) | 3.3 ± 1.8 | 3 (2–5) | <0.001 | 6.2 ± 0.9 | 6.5 (5.2–7) | 3.3 ± 1.8 | 3 (2–5) | 0.003 | 3.3 ± 1.78 | 3 (2–5) |
| Symptom count | 12.5 ± 4.5 | 11 (9.7–15) | 2.6 ± 2.5 | 2 (1–4) | <0.001 | 11.2 ± 1.7 | 11.5 (9.5–12.7) | 2.7 ± 2.6 | 2 (1–4) | <0.001 | 2.7 ± 2.6 | 2 (1–4) |
| Somatic Symptoms | Whole Sample n = 7275 n (%) | 2010 ACR | 2016 ACR | ||||
|---|---|---|---|---|---|---|---|
| Positive n = 38 n (%) | Negative n = 7237 n (%) | p * | Positive n = 4 n (%) | Negative n = 7271 n (%) | p * | ||
| Fatigue | 2739 (37.6) | 36 (94.7) | 2192 (30.3) | <0.001 | 3 (75) | 2224 (30.6) | 0.009 |
| Difficulties in sleeping | 1513 (20.8) | 26 (68.4) | 1487 (20.5) | <0.001 | 1 (25) | 1512 (20.8) | 1 |
| Difficulties in thinking and remembering | 398 (5.5) | 14 (36.8) | 384 (5.3) | <0.001 | 1 (25) | 397 (5.5) | 0.202 |
| Difficulties in studying | 689 (9.5) | 24 (63.2) | 665 (9.2) | <0.001 | 3 (75) | 686 (9.4) | 0.003 |
| Headache | 2213 (28.5) | 34 (89.5) | 2038 (28.2) | <0.001 | 4 (100) | 2209 (30.4) | 0.009 |
| Anxiety and nervousness | 1529 (21) | 33 (86.8) | 1495 (20.7) | <0.001 | 3 (75) | 1525 (21) | 0.031 |
| Depression, melancholy | 214 (2.9) | 22 (57.9) | 192 (2.7) | <0.001 | 2 (50) | 212 (2.9) | 0.005 |
| Diarrhea, constipation | 3004 (41.3) | 30 (78.9) | 2974 (41.1) | <0.001 | 3 (75) | 3001 (41.3) | 0.313 |
| Abdominal pain or bloating | 817 (11.2) | 26 (68.4) | 791 (10.9) | <0.001 | 2 (50) | 815 (11.2) | 0.065 |
| Itching | 925 (12.7) | 16 (42.1) | 909 (12.6) | <0.001 | 1 (25) | 924 (12.7) | 1 |
| Rash, hives | 1106 (15.2) | 10 (26.3) | 1096 (15.1) | 0.068 | 1 (25) | 1105 (15.2) | 1 |
| Skin’s sensitivity to the sun | 274 (3.8) | 3 (7.9) | 271 (3.7) | 0.171 | 0 (0) | 274 (3.8) | 1 |
| Nausea, heartburn | 430 (5.9) | 15 (39.5) | 415 (5.7) | <0.001 | 1 (25) | 429 (5.9) | 0.216 |
| Cold hands and feet | 808 (11.1) | 17 (44.7) | 791 (10.9) | <0.001 | 1 (25) | 807 (11.1) | 0.376 |
| Swelling sensation in the hands | 24 (0.3) | 2 (5.3) | 22 (0.3) | 0.007 | 0 (0 | 24 (0.3) | 1 |
| Palpitations | 139 (1.9) | 8 (21.1) | 131 (1.8) | <0.001 | 1 (25) | 138 (1.9) | 0.074 |
| Chest pain | 169 (2.3) | 15 (39.5) | 154 (2.1) | <0.001 | 2 (50) | 167 (2.3) | 0.003 |
| Dizziness | 120 (1.6) | 8 (21.1) | 112 (1.5) | <0.001 | 1 (25) | 119 (1.6) | 0.064 |
| Shortness of breath | 163 (2.2) | 11 (28.9) | 152 (2.1) | <0.001 | 1 (25) | 162 (2.2) | 0.087 |
| Cramps | 256 (3.5) | 15 (39.5) | 241 (3.3) | <0.001 | 1 (25) | 255 (3.5) | 0.134 |
| Muscle weakness in the legs | 311 (4.3) | 23 (60.5) | 288 (4) | <0.001 | 0 (0) | 307 (4.2) | <0.001 |
| Mild fever | 891 (12.2) | 14 (36.8) | 877 (12.1) | <0.001 | 2 (50) | 889 (12.2) | 0.076 |
| Painful menstruation | 172 (2.3 *) | 1 (31.6 #) | 162 (2.2 °) | <0.001 | 0 (0) | 174 (2.4 ^) | 1 |
| Muscle stiffness, especially in the morning | 31 (0.4) | 5 (13.2) | 26 (0.4) | <0.001 | 1 (25) | 30 (0.4) | 0.017 |
| Shaking of the legs in bed | 289 (4) | 14 (36.8) | 275 (3.8) | <0.001 | 2 (50) | 287 (3.9) | 0.009 |
| Tingling | 184 (2.5) | 11 (28.9) | 173 (2.4) | <0.001 | 0 (0) | 184 (2.5) | 1 |
| Numbness | 69 (0.9) | 5 (13.2) | 64 (0.9) | <0.001 | 0 (0) | 69 (0.9) | 1 |
| Variables | Total | Among Whom Matched the Criteria for Fibromyalgia | |||||
|---|---|---|---|---|---|---|---|
| n | % | 2010 ACR | 2016 ACR | ||||
| n (%); (Total: 38) | p * | n (%); (Total: 4) | p * | ||||
| Relationship with peers | Very good | 4380 | 60.2 | 9 (23.7%) | <0.001 | 1 (25%) | 0.242 |
| Quite good | 2708 | 37.2 | 19 (50%) | 3 (75%) | |||
| Quite bad | 140 | 1.9 | 9 (23.7%) | 0 | |||
| Very bad | 8 | 0.1 | 0 | 0 | |||
| Don’t know | 39 | 0.5 | 1 (2.6%) | 0 | |||
| School performance | Very good | 3535 | 48.6 | 7 (18.4%) | <0.001 | 1 (25%) | 0.558 |
| Quite good | 3052 | 42 | 20 (52.6%) | 3 (75%) | |||
| Quite bad | 238 | 3.3 | 8 (21.1%) | 0 | |||
| Very bad | 11 | 0.2 | 2 (5.3%) | 0 | |||
| Don’t know | 439 | 6.0 | 1 (2.6%) | 0 | |||
| Being bullied | Yes | 821 | 11.3 | 17 (44.7%) | <0.001 | 1 (25%) | 0.593 |
| No | 5810 | 79.9 | 17 (44.7%) | 3 (75%) | |||
| Don’t know | 644 | 8.9 | 4 (0.6%) | ||||
| Cohabiting parents | No | 1783 | 24.5 | 4 (10.5%) | 0.05 | 0 | 0.325 |
| Yes | 5492 | 75.5 | 34 (89.5%) | ||||
| Relationship with parents | Quite or very bad with at least one parent | 93 | 1.3 | 8 (21.6%) | <0.001 | 0 | 0.950 |
| At least one parent with diffuse pain | Yes | 2023 | 27.8 | 32 (84.2%) | <0.001 | 4 (100%) | 0.006 |
| At least one parent with fibromyalgia | Yes | 187 | 2.6 | 6 (15.8%) | <0.001 | 2 (50%) | 0.004 |
| At least one parent who uses or has used psychotropic drugs | Yes | 659 | 9.1 | 10 (26.3%) | 0.002 | 0 | 0.684 |
| Road accident | Yes | 205 | 2.8% | 1 (2.6%) | 0.709 | 0 | 0.892 |
| Injury in the leisure time | Yes | 493 | 6.8% | 17 (44.7%) | <0.001 | 1 (25%) | 0.245 |
| Surgery | Yes | 856 | 11.8% | 12 (31.6%) | <0.001 | 1 (25%) | 0.394 |
| Independent Variables | OR | Standard Error | p | |
|---|---|---|---|---|
| Age | <8 | 1 | - | - |
| ≥8 | 2.42 | 0.428 | 0.039 | |
| Injury in the leisure time | no | 1 | - | - |
| yes | 6.49 | 0.34 | <0.001 | |
| At least one parent with fibromyalgia | no | 1 | - | - |
| yes | 2.54 | 0.469 | 0.046 | |
| At least one parent with diffuse pain | no | 1 | - | - |
| yes | 9.09 | 0.458 | <0.001 | |
| Symptoms | Our Data (2010 ACR Criteria) | Wolfe 1990 [4] (1990 ACR Criteria) | Yunus 1985 [6] (Yunus and Masi 1985 Criteria) | Siegel 1998 [22] (1990 ACR Criteria) | Eraso 2007 [20] Specifically Designed Questionnaire | Gedalia 2000 [23] (1990 ACR Criteria) | |
|---|---|---|---|---|---|---|---|
| n = 38 | n = 45 Adults | n = 33 | n = 33 | n = 46 Onset 3–10 Years | n = 102 Onset 10–19 Years | n = 59 | |
| Diffuse pain | 100 | 98 | 97 | 93 | 100 | 100 | 97 |
| Fatigue | 94.7 | 81 | 91 | 62 | 28 | 23 | 20 |
| Sleep disturbances | 68.4 | 75 | 67 | 96 | 65 | 74 | 70 |
| Headache | 78.9 | 53 | 58 | 71 | 78 | 80 | 76 |
| Depression | 57.9 | 32 | 55 | 43 | 9 | 9 | 7 |
| Abdominal symptoms | 26.2 | 30 | 27 | 38 | 39 | 19 | 17 |
| Anxiety and nervousness | 86.8 | 48 | 70 | 22 | 2 | 2 | - |
| Subjective soft tissue swelling | 5.3 | 61 | 40 | 39 | 14 | 24 | |
| Dysmenorrhea | 31.6 * | 41 | - | 36 | - | - | - |
| Stiffness, especially in the morning | 13.2 | 77 | 79 | 53 | 39 | 21 | 30 |
| Numbness | 13.2 | 67 | 36 | 24 | 6 | 1 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maddali Bongi, S.; Vitali Rosati, G.; Bonaccorsi, G.; Lorini, C. Prevalence and Contextual Factors of Juvenile Fibromyalgia in a Population-Based Italian Sample of Children and Adolescents. Biomedicines 2023, 11, 1583. https://doi.org/10.3390/biomedicines11061583
Maddali Bongi S, Vitali Rosati G, Bonaccorsi G, Lorini C. Prevalence and Contextual Factors of Juvenile Fibromyalgia in a Population-Based Italian Sample of Children and Adolescents. Biomedicines. 2023; 11(6):1583. https://doi.org/10.3390/biomedicines11061583
Chicago/Turabian StyleMaddali Bongi, Susanna, Giovanni Vitali Rosati, Guglielmo Bonaccorsi, and Chiara Lorini. 2023. "Prevalence and Contextual Factors of Juvenile Fibromyalgia in a Population-Based Italian Sample of Children and Adolescents" Biomedicines 11, no. 6: 1583. https://doi.org/10.3390/biomedicines11061583
APA StyleMaddali Bongi, S., Vitali Rosati, G., Bonaccorsi, G., & Lorini, C. (2023). Prevalence and Contextual Factors of Juvenile Fibromyalgia in a Population-Based Italian Sample of Children and Adolescents. Biomedicines, 11(6), 1583. https://doi.org/10.3390/biomedicines11061583