
Influence of Chronic Fatigue Syndrome Codiagnosis on the Relationship between Perceived and Objective Psychoneuro-Immunoendocrine Disorders in Women with Fibromyalgia


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Experimental Design
2.2. Body Composition Measurements; Bioimpedance Analysis
2.3. Subjective Quality of Life
2.4. Determination of Objective Levels of Physical Activity and Sedentary Lifestyle
2.5. Blood Collection and Serum Isolation
2.6. Determination of Neuroimmunoendocrine Markers
2.7. Statistical Analysis
3. Results
3.1. Psychological Status and Quality of Life
3.2. Neuroimmunoendocrine Biomarkers
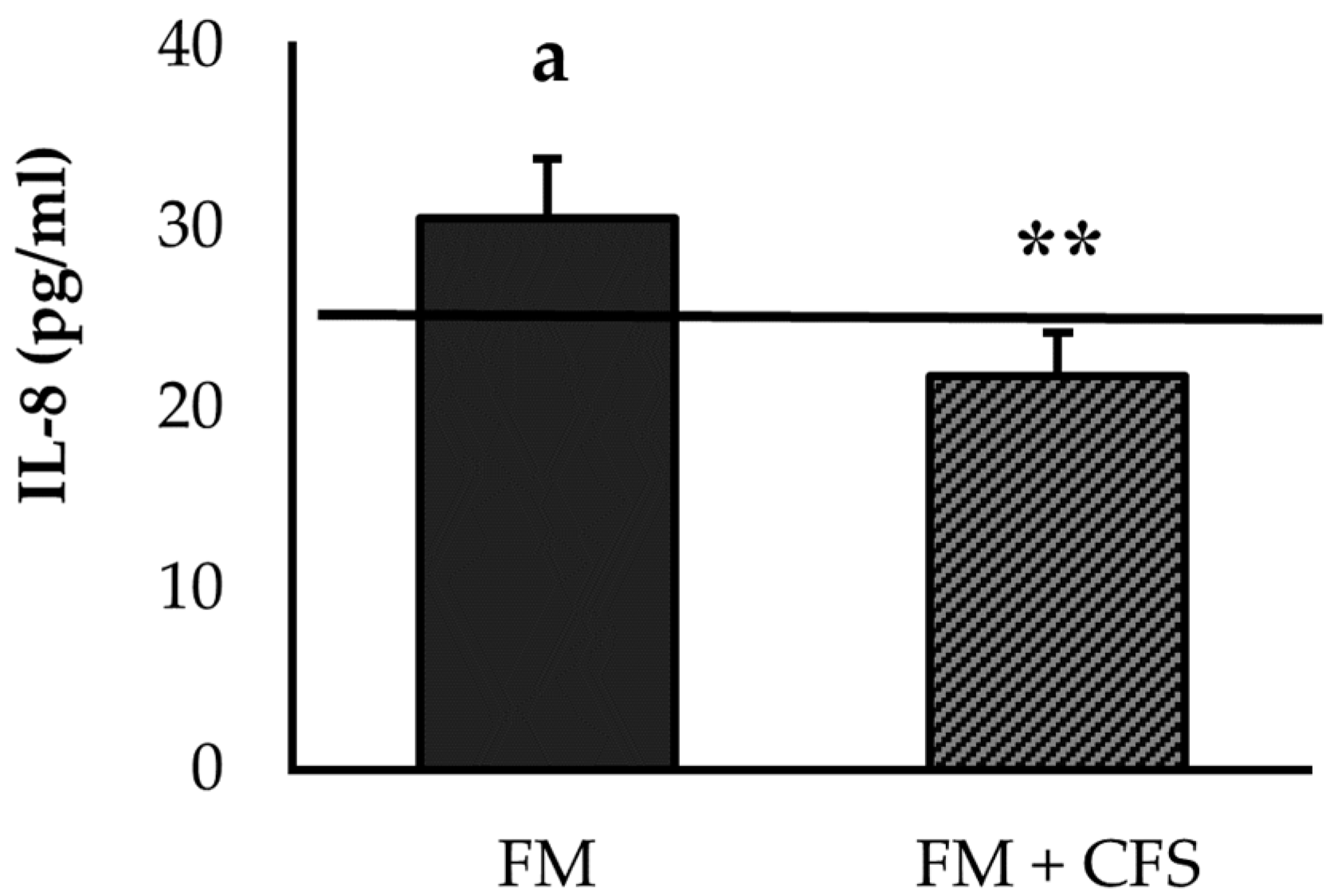
3.2.1. Influence of CFS Codiagnosis in FM Patients: Serum Levels of IL-8 and IL-10
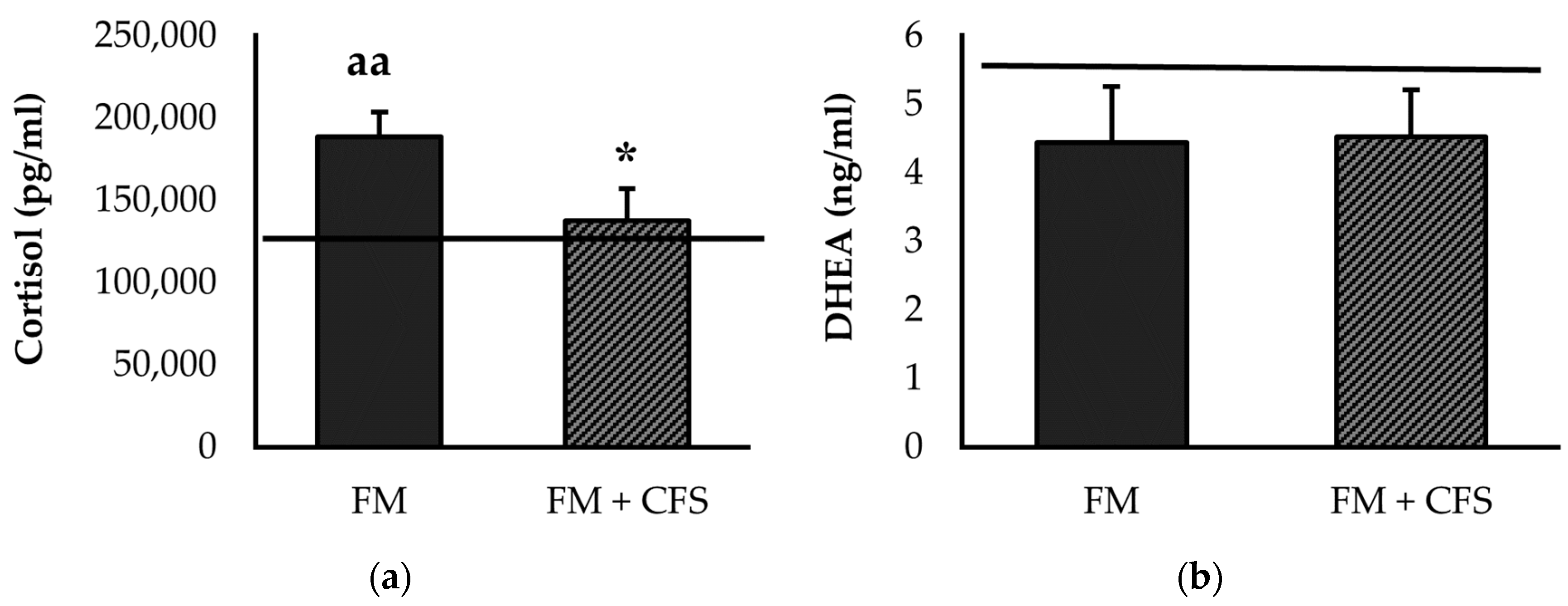
3.2.2. Influence of CFS Codiagnosis in FM Patients: Serum Levels of Cortisol and DHEA
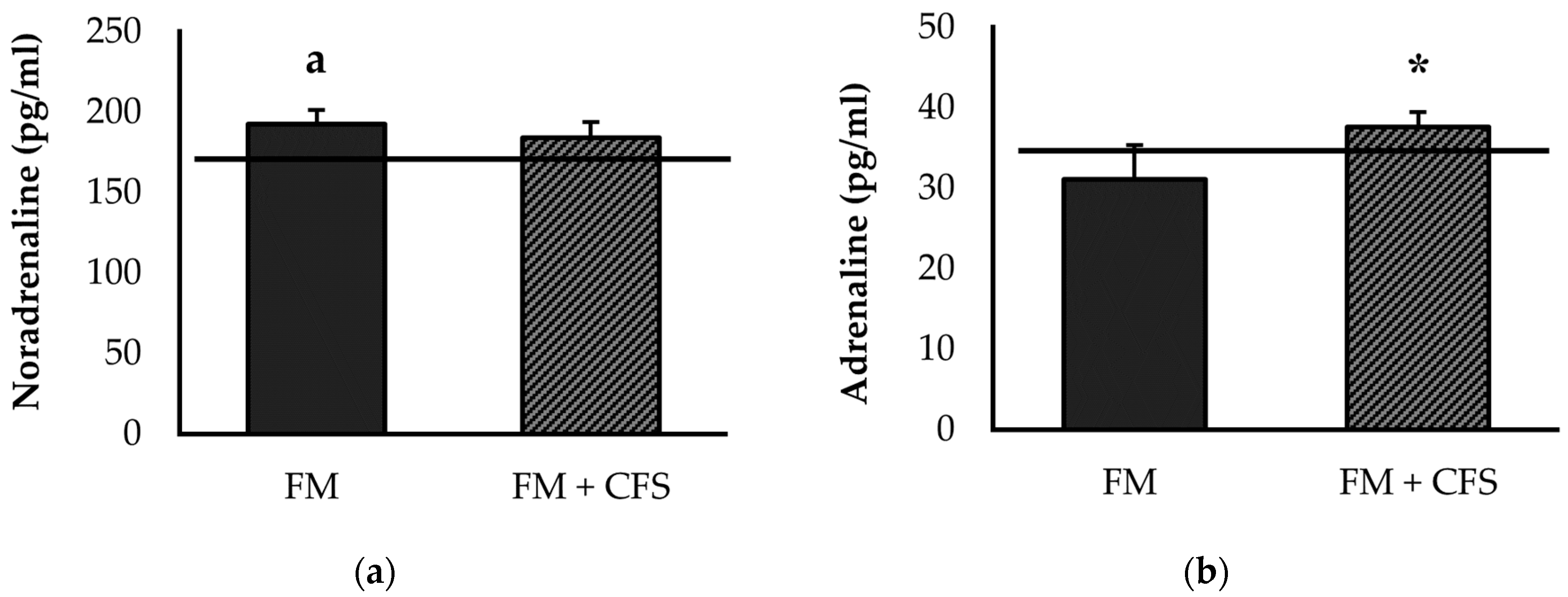
3.2.3. Influence of CFS Codiagnosis in FM Patients: Serum Levels of Noradrenaline and Adrenaline
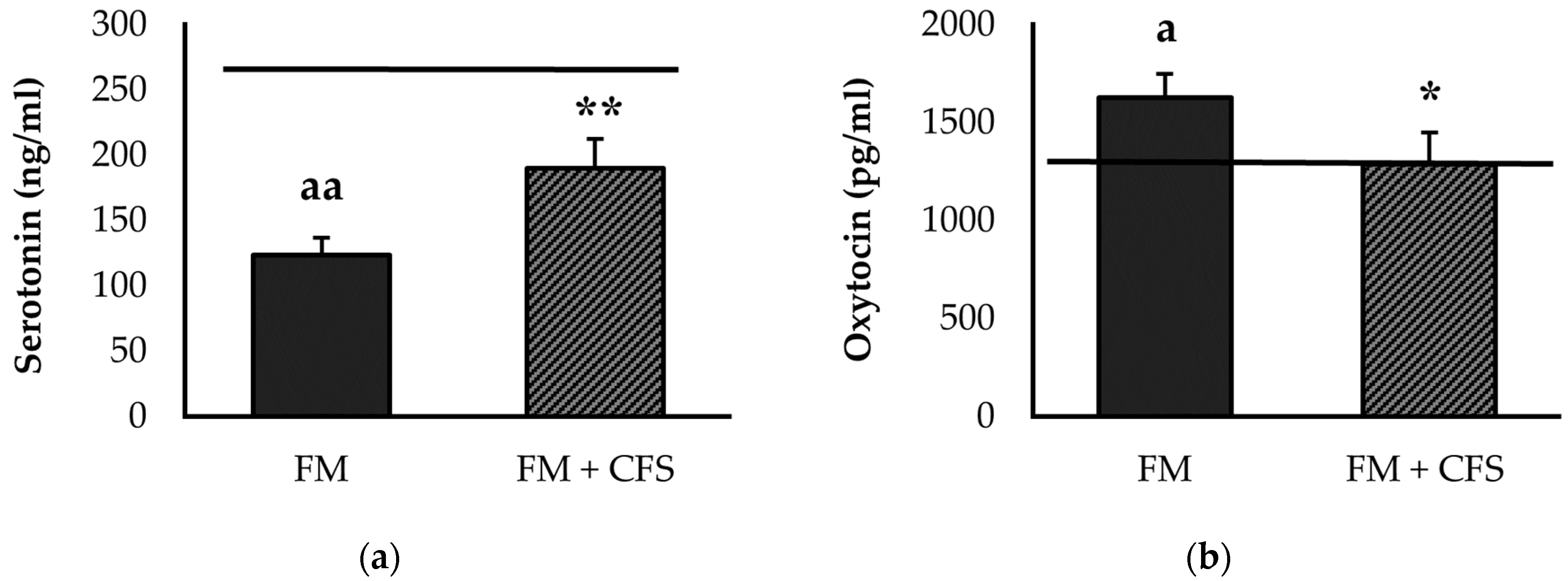
3.2.4. Influence of CFS Codiagnosis in FM Patients: Serum Levels of Serotonin and Oxytocin
3.3. Physical Activity/Sedentarism Levels Determined via Accelerometry
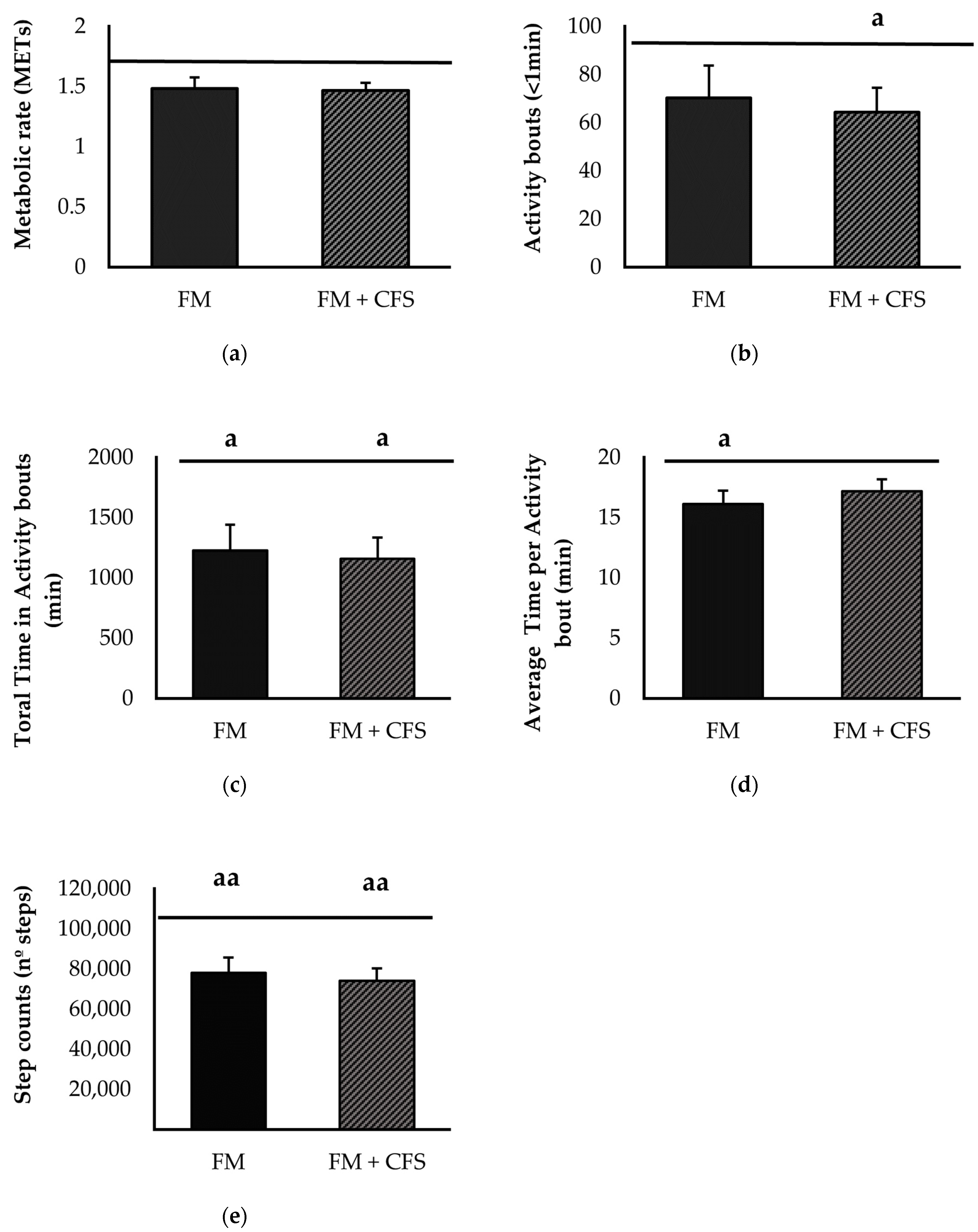
3.3.1. Influence of CFS Codiagnosis in FM Patients: Accelerometric Study of Physical Activity
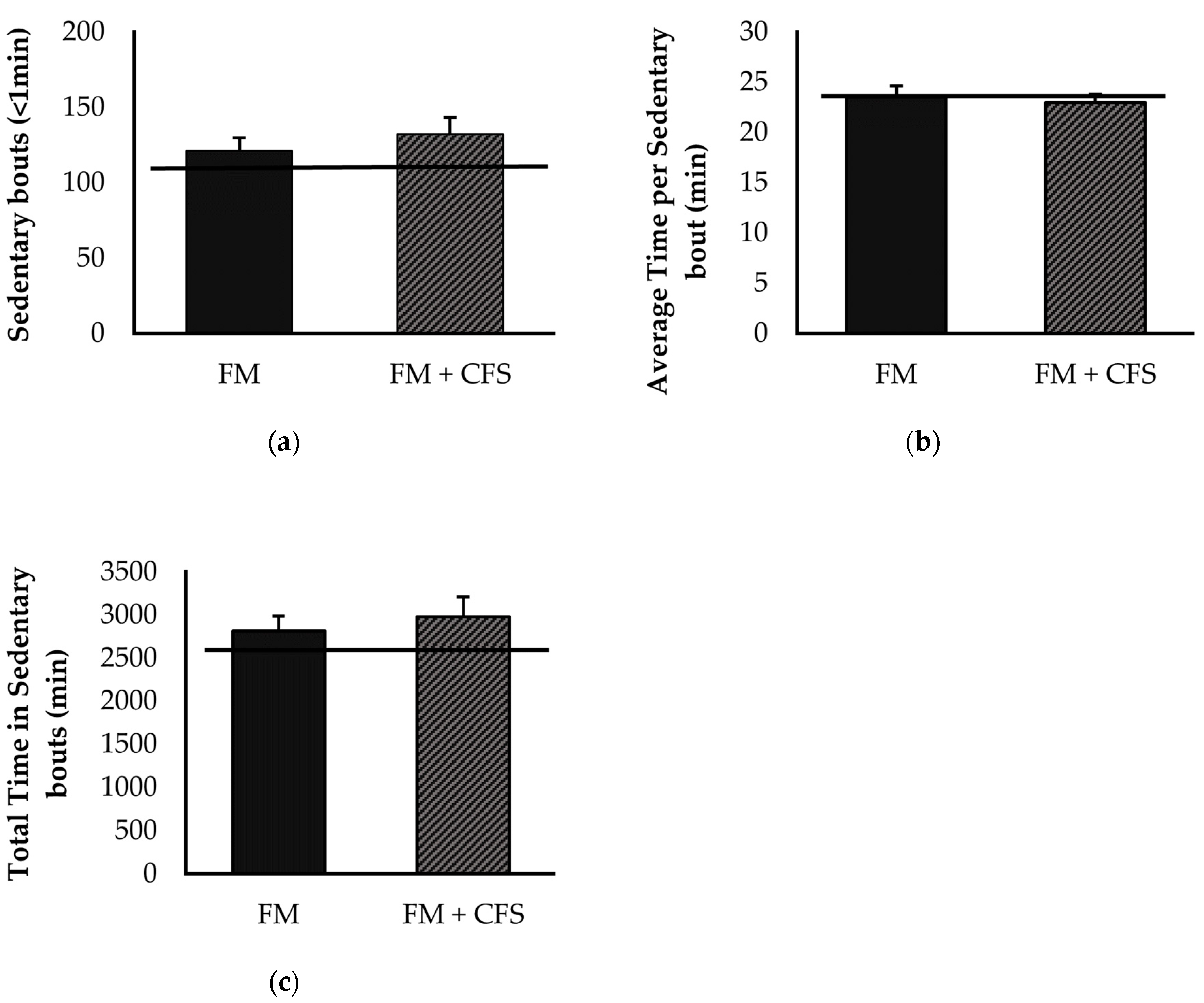
3.3.2. Influence of CFS Codiagnosis in FM Patients: Accelerometric Study of Sedentarism
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria. In Seminars in Arthritis and Rheumatism; Elsevier: Amsterdam, The Netherlands, 2016; Volume 46, pp. 319–329. [Google Scholar]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A.; International Chronic Fatigue Syndrome Study Group. The Chronic Fatigue Syndrome: A Comprehensive Approach to Its Definition and Study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Ortega, E.; García, J.J.; Bote, M.E.; Martín-Cordero, L.; Escalante, Y.; Saavedra, J.M.; Northoff, H.; Giraldo, E. Exercise in Fibromyalgia and Related Inflammatory Disorders: Known Effects and Unknown Chances. Exerc. Immunol. Rev. 2009, 15, 42–65. [Google Scholar] [PubMed]
- Bote, M.E.; Garca, J.J.; Hinchado, M.D.; Ortega, E. Inflammatory/Stress Feedback Dysregulation in Women with Fibromyalgia. Neuroimmunomodulation 2012, 19, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Hinchado, M.D.; Quero-Calero, C.D.; Otero, E.; Gálvez, I.; Ortega, E. Synbiotic Supplementation Improves Quality of Life and Inmunoneuroendocrine Response in Patients with Fibromyalgia: Influence of Codiagnosis with Chronic Fatigue Syndrome. Nutrients 2023, 15, 1591. [Google Scholar] [CrossRef]
- García, J.J.; Cidoncha, A.; Bote, M.E.; Hinchado, M.D.; Ortega, E. Altered Profile of Chemokines in Fibromyalgia Patients. Ann. Clin. Biochem. 2014, 51, 576–581. [Google Scholar] [CrossRef]
- Garcia, J.J.; Ortega, E. Soluble Fractalkine in the Plasma of Fibromyalgia Patients. Anais da Academia Brasileira de Ciências 2014, 86, 1915–1917. [Google Scholar] [CrossRef] [PubMed]
- Bote, M.E.; Garcia, J.J.; Hinchado, M.D.; Ortega, E. Fibromyalgia: Anti-Inflammatory and Stress Responses after Acute Moderate Exercise. PLoS ONE 2013, 8, e74524. [Google Scholar] [CrossRef]
- Bote, M.E.; García, J.J.; Hinchado, M.D.; Ortega, E. An Exploratory Study of the Effect of Regular Aquatic Exercise on the Function of Neutrophils from Women with Fibromyalgia: Role of IL-8 and Noradrenaline. Brain. Behav. Immun. 2014, 39, 107–112. [Google Scholar] [CrossRef]
- Cortes Rivera, M.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Comprehensive Review. Diagnostics 2019, 9, 91. [Google Scholar] [CrossRef]
- Klimas, N.G.; Broderick, G.; Fletcher, M.A. Biomarkers for Chronic Fatigue. Brain. Behav. Immun. 2012, 26, 1202–1210. [Google Scholar] [CrossRef]
- Kerr, J.R.; Petty, R.; Burke, B.; Gough, J.; Fear, D.; Sinclair, L.I.; Mattey, D.L.; Richards, S.C.M.; Montgomery, J.; Baldwin, D.A.; et al. Gene Expression Subtypes in Patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. J. Infect. Dis. 2008, 197, 1171–1184. [Google Scholar] [CrossRef] [PubMed]
- Frampton, D.; Kerr, J.; Harrison, T.J.; Kellam, P. Assessment of a 44 Gene Classifier for the Evaluation of Chronic Fatigue Syndrome from Peripheral Blood Mononuclear Cell Gene Expression. PLoS ONE 2011, 6, e16872. [Google Scholar] [CrossRef] [PubMed]
- Benavent, R.A.; Arroyo, A.A.; Sánchez, M.A.; Pizarro, M.B.; Heras, M.; Alcalde, G.G.; Miguel, C.M.; Molina, C.N.; Cogollos, L.C.; Zurián, J.C.V.; et al. Evolution and Scientific Impact of Research Grants from the Spanish Society of Cardiology and Spanish Heart Foundation (2000–2006). Rev. Española Cardiol. 2011, 64, 904–915. [Google Scholar] [CrossRef]
- Félix-Redondo, F.J.; Fernández-Bergés, D.; Fernando Pérez, J.; Zaro, M.J.; García, A.; Lozano, L.; Sanz, H.; Grau, M.; Álvarez-Palacios, P.; Tejero, V. Prevalence, Awareness, Treatment and Control of Cardiovascular Risk Factors in the Extremadura Population (Spain). HERMEX Study. Aten. Primaria 2011, 43, 426–434. [Google Scholar] [CrossRef]
- Hinchado, M.D.; Otero, E.; Navarro, M.D.C.; Martín-Cordero, L.; Gálvez, I.; Ortega, E. Influence of Codiagnosis of Chronic Fatigue Syndrome and Habitual Physical Exercise on the Psychological Status and Quality of Life of Patients with Fibromyalgia. J. Clin. Med. 2022, 11, 5735. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.; Perdigón, A.L.; Vázquez, C. The Spanish Adaptation of Beck’s Depression Inventory-II (BDI-II): 2. Psychometric Properties in the General Population. Clin. Salud 2003, 14, 249–280. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Remor, E. Psychometric Properties of a European Spanish Version of the Perceived Stress Scale (PSS). Span. J. Psychol. 2006, 9, 86–93. [Google Scholar] [CrossRef]
- Spielberger, C.D. State-Trait Anxiety Inventory for AdultsTM; American Psychological Association: Washington, DC, USA, 1983. [Google Scholar]
- Buela-Casal, G.; Guillén-Riquelme, A. Short Form of the Spanish Adaptation of the State-Trait Anxiety Inventory. Int. J. Clin. Health Psychol. 2017, 17, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Daut, R.L.; Cleeland, C.S.; Flanery, R.C. Development of the Wisconsin Brief Pain Questionnaire to Assess Pain in Cancer and Other Diseases. Pain 1983, 17, 197–210. [Google Scholar] [CrossRef]
- Mendoza, T.R.; Wang, X.S.; Cleeland, C.S.; Morrissey, M.; Johnson, B.A.; Wendt, J.K.; Huber, S.L. The Rapid Assessment of Fatigue Severity in Cancer Patients: Use of the Brief Fatigue Inventory. Cancer 1999, 85, 1186–1196. [Google Scholar] [CrossRef]
- Badia, X.; Muriel, C.; Gracia, A.; Núñez-Olarte, J.M.; Perulero, N.; Gálvez, R.; Carulla, J.; Cleeland, C.S.; Barutell, C.; Gómez, M.; et al. Validación Española Del Cuestionario Brief Pain Inventory En Pacientes Con Dolor de Causa Neoplásica. Med. Clin. 2003, 120, 52–59. [Google Scholar] [CrossRef]
- Valenzuela, J.O.; Gning, I.; Irarrázaval, M.E.; Fasce, G.; Marín, L.; Mendoza, T.R.; Palos, G.; Reynolds, R.; Wang, X.S.; Cleeland, C.S. Psychometric Validation of the Spanish Version of the Brief Fatigue Inventory; The University of Texas MD Anderson Cancer Center, Division of Internal Medicine Research Retreat: Houston, TX, USA, 2012. [Google Scholar]
- Darviri, C.; Alexopoulos, E.C.; Artemiadis, A.K.; Tigani, X.; Kraniotou, C.; Darvyri, P.; Chrousos, G.P. The Healthy Lifestyle and Personal Control Questionnaire (HLPCQ): A Novel Tool for Assessing Self-Empowerment through a Constellation of Daily Activities. BMC Public Health 2014, 14, 995. [Google Scholar] [CrossRef] [PubMed]
- Rivera, J.; González, T. The Fibromyalgia Impact Questionnaire: A Validated Spanish Version to Assess the Health Status in Women with Fibromyalgia. Clin. Exp. Rheumatol. 2004, 22, 554–560. [Google Scholar] [PubMed]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The Fibromyalgia Impact Questionnaire: Development and Validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Lee, S.A. Coronavirus Anxiety Scale: A Brief Mental Health Screener for COVID-19 Related Anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Caycho-Rodríguez, T.; Vilca, L.W.; Peña-Calero, B.N.; Barboza-Palomino, M.; White, M.; Reyes-Bossio, M. Measurement of Coronaphobia in Older Adults: Validation of the Spanish Version of the Coronavirus Anxiety Scale. Rev. Esp. Geriatr. Gerontol. 2022, 57, 20–27. [Google Scholar] [CrossRef]
- Kwasi Ahorsu, D.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef]
- Sánchez-Teruel, D.; Robles-Bello, M.A. The COVID-19 Fear Scale (FCV-19S): Psychometric Properties and Invariance of the Measure in the Spanish Version. Actas Esp. Psiquiatr. 2021, 49, 96–105. [Google Scholar]
- Santos-Lozano, A.; Santín-Medeiros, F.; Cardon, G.; Torres-Luque, G.; Bailón, R.; Bergmeir, C.; Ruiz, J.R.; Lucia, A.; Garatachea, N. Actigraph GT3X: Validation and Determination of Physical Activity Intensity Cut Points. Int. J. Sports Med. 2013, 34, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. Accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Torpy, D.J.; Papanicolaou, D.A.; Lotsikas, A.J.; Wilder, R.L.; Chrousos, G.P.; Pillemer, S.R. Responses of the Sympathetic Nervous System and the Hypothalamic–Pituitary–Adrenal Axis to Interleukin-6: A Pilot Study in Fibromyalgia. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2000, 43, 872–880. [Google Scholar] [CrossRef]
- Ablin, J.; Neumann, L.; Buskila, D. Pathogenesis of Fibromyalgia—A Review. Jt. Bone Spine 2008, 75, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.P.; Santo, A. de S. do E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of Fibromyalgia: Literature Review Update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Laroche, F. Fibromyalgia. Rev. Prat. 2019, 69, 649–651. [Google Scholar]
- Goldenberg, D.L.; Simms, R.W.; Geiger, A.; Komaroff, A.L. High Frequency of Fibromyalgia in Patients with Chronic Fatigue Seen in a Primary Care Practice. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1990, 33, 381–387. [Google Scholar] [CrossRef]
- Buchwald, D.; Garrity, D. Comparison of Patients with Chronic Fatigue Syndrome, Fibromyalgia, and Multiple Chemical Sensitivities. Arch. Intern. Med. 1994, 154, 2049–2053. [Google Scholar] [CrossRef]
- Aaron, L.A.; Buchwald, D. Chronic Diffuse Musculoskeletal Pain, Fibromyalgia and Co-Morbid Unexplained Clinical Conditions. Best Pract. Res. Clin. Rheumatol. 2003, 17, 563–574. [Google Scholar] [CrossRef]
- Yunus, M.B. The Prevalence of Fibromyalgia in Other Chronic Pain Conditions. Pain Res. Treat. 2012, 2012, 584573. [Google Scholar] [CrossRef]
- Ickmans, K.; Meeus, M.; De Kooning, M.; Lambrecht, L.; Pattyn, N.; Nijs, J. Associations between Cognitive Performance and Pain in Chronic Fatigue Syndrome: Comorbidity with Fibromyalgia Does Matter. Physiotherapy 2015, 101, e635–e636. [Google Scholar] [CrossRef]
- Mcloughlin, M.J.; Colbert, L.H.; Stegner, A.J.; Cook, D.B. Are Women with Fibromyalgia Less Physically Active than Healthy Women? Med. Sci. Sports Exerc. 2011, 43, 905. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J. Limits to the Measurement of Habitual Physical Activity by Questionnaires. Br. J. Sports Med. 2003, 37, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Conger, S.A.; Toth, L.P.; Cretsinger, C.; Raustorp, A.; Mitáš, J.; Inoue, S.; Bassett, D.R. Time Trends in Physical Activity Using Wearable Devices: A Systematic Review and Meta-Analysis of Studies from 1995 to 2017. Med. Sci. Sport. Exerc. 2022, 54, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Munguía-Izquierdo, D.; Legaz-Arrese, A.; Mannerkorpi, K. Transcultural Adaptation and Psychometric Properties of a Spanish-Language Version of Physical Activity Instruments for Patients with Fibromyalgia. Arch. Phys. Med. Rehabil. 2011, 92, 284–294. [Google Scholar] [CrossRef]
- Estévez-López, F.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Soriano-Maldonado, A.; Borges-Cosic, M.; Pulido-Martos, M.; Aparicio, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M.; Geenen, R. The Discordance between Subjectively and Objectively Measured Physical Function in Women with Fibromyalgia: Association with Catastrophizing and Self-Efficacy Cognitions. The Al-Ándalus Project. Disabil. Rehabil. 2018, 40, 329–337. [Google Scholar] [CrossRef]
- Vergauwen, K.; Huijnen, I.P.J.; Smeets, R.J.E.M.; Kos, D.; van Eupen, I.; Nijs, J.; Meeus, M. An Exploratory Study of Discrepancies between Objective and Subjective Measurement of the Physical Activity Level in Female Patients with Chronic Fatigue Syndrome. J. Psychosom. Res. 2021, 144, 110417. [Google Scholar] [CrossRef]
- Díaz Robredo, L.A.; Robles Sánchez, J.I. Estabilidad Emocional y Cortisol Como Factores Diferenciadores de La Fibromialgia. Sanid. Mil. 2011, 67, 11–17. [Google Scholar] [CrossRef]
- McCain, G.A.; Tilbe, K.S. Diurnal Hormone Variation in Fibromyalgia Syndrome: A Comparison with Rheumatoid Arthritis. J. Rheumatol. 1989, 19, 154–157. [Google Scholar]
- Crofford, L.J.; Pillemer, S.R.; Kalogeras, K.T.; Cash, J.M.; Michelson, D.; Kling, M.A.; Sternberg, E.M.; Gold, P.W.; Chrousos, G.P.; Wilder, R.L. Hypothalamic–Pituitary–Adrenal Axis Perturbations in Patients with Fibromyalgia. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1994, 37, 1583–1592. [Google Scholar] [CrossRef]
- Gur, A.; Cevik, R.; Nas, K.; Colpan, L.; Sarac, S. Cortisol and Hypothalamic–Pituitary–Gonadal Axis Hormones in Follicular-Phase Women with Fibromyalgia and Chronic Fatigue Syndrome and Effect of Depressive Symptoms on These Hormones. Arthritis Res Ther 2004, 6, R232. [Google Scholar] [CrossRef] [PubMed]
- Bonnabesse, A.L.F.; Cabon, M.; L’heveder, G.; Kermarrec, A.; Quinio, B.; Woda, A.; Marchand, S.; Dubois, A.; Giroux-Metges, M.-A.; Rannou, F. Impact of a Specific Training Programme on the Neuromodulation of Pain in Female Patient with Fibromyalgia (DouFiSport): A 24-Month, Controlled, Randomised, Double-Blind Protocol. BMJ Open 2019, 9, e023742. [Google Scholar] [CrossRef] [PubMed]
- Roerink, M.E.; Roerink, S.H.P.P.; Skoluda, N.; van der Schaaf, M.E.; Hermus, A.R.M.M.; van der Meer, J.W.M.; Knoop, H.; Nater, U.M. Hair and Salivary Cortisol in a Cohort of Women with Chronic Fatigue Syndrome. Horm. Behav. 2018, 103, 1–6. [Google Scholar] [CrossRef]
- Papandreou, M.; Philippou, A.; Taso, O.; Koutsilieris, M.; Kaperda, A. The Effect of Treatment Regimens on Salivary Cortisol Levels in Patients with Chronic Musculoskeletal Disorders. J. Bodyw. Mov. Ther. 2020, 24, 100–108. [Google Scholar] [CrossRef]
- Roberts, A.D.L.; Charler, M.-L.; Papadopoulos, A.; Wessely, S.; Chalder, T.; Cleare, A.J. Does Hypocortisolism Predict a Poor Response to Cognitive Behavioural Therapy in Chronic Fatigue Syndrome? Psychol. Med. 2010, 40, 515–522. [Google Scholar] [CrossRef]
- Powell, D.J.H.; Liossi, C.; Moss-Morris, R.; Schlotz, W. Unstimulated Cortisol Secretory Activity in Everyday Life and Its Relationship with Fatigue and Chronic Fatigue Syndrome: A Systematic Review and Subset Meta-Analysis. Psychoneuroendocrinology 2013, 38, 2405–2422. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, J.A.; Darnall, B.D.; Zwickey, H.L.; Wood, L.J.; Hanes, D.A.; Zava, D.T.; Mackey, S.C. Proinflammatory Cytokines and DHEA-S in Women with Fibromyalgia: Impact of Psychological Distress and Menopausal Status. J. Pain Res. 2014, 2014, 707–716. [Google Scholar] [CrossRef]
- Straub, R.H.; Schuld, A.; Mullington, J.; Haack, M.; Scholmerich, J.; Pollmacher, T. The Endotoxin-Induced Increase of Cytokines Is Followed by an Increase of Cortisol Relative to Dehydroepiandrosterone (DHEA) in Healthy Male Subjects. J. Endocrinol. 2002, 175, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Spencer, N.F.L.; Norton, S.D.; Harrison, L.L.; Li, G.-Z.; Daynes, R.A. Dysregulation of IL-10 Production with Aging: Possible Linkage to the Age-Associated Decline in DHEA and Its Sulfated Derivative. Exp. Gerontol. 1996, 31, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsson, M. One Year Outcome of Preadolescents with Fibromyalgia. J. Rheumatol. 1999, 26, 674–682. [Google Scholar]
- Besedovsky, H.O.; Del Rey, A. Physiology of Psychoneuroimmunology: A Personal View. Brain Behav. Immun. 2007, 21, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Ortega, E. The “Bioregulatory Effect of Exercise” on the Innate/Inflammatory Responses. J. Physiol. Biochem. 2016, 72, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Ortega, E.; Bote, M.E.; Giraldo, E.; García, J.J. Aquatic Exercise Improves the Monocyte Pro- and Anti-Inflammatory Cytokine Production Balance in Fibromyalgia Patients. Scand. J. Med. Sci. Sport. 2012, 22, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Russell, L.; Broderick, G.; Taylor, R.; Fernandes, H.; Harvey, J.; Barnes, Z.; Smylie, A.; Collado, F.; Balbin, E.G.; Katz, B.Z.; et al. Illness Progression in Chronic Fatigue Syndrome: A Shifting Immune Baseline. BMC Immunol. 2016, 17, 3. [Google Scholar] [CrossRef]
- Arnold, L.M.; Keck, P.E.J.; Welge, J.A. Antidepressant Treatment of Fibromyalgia. A Meta-Analysis and Review. Psychosomatics 2000, 41, 104–113. [Google Scholar] [CrossRef]
- Häuser, W.; Urrútia, G.; Tort, S.; Uçeyler, N.; Walitt, B. Serotonin and Noradrenaline Reuptake Inhibitors (SNRIs) for Fibromyalgia Syndrome. Cochrane Database Syst. Rev. 2013, 2013, CD010292. [Google Scholar] [CrossRef]
- Welsch, P.; Üçeyler, N.; Klose, P.; Walitt, B.; Häuser, W. Serotonin and Noradrenaline Reuptake Inhibitors (SNRIs) for Fibromyalgia. Cochrane Database Syst. Rev. 2018, 2, CD010292. [Google Scholar] [CrossRef]
- Russell, I.J.; Michalek, J.E.; Vipraio, G.A.; Fletcher, E.M.; Javors, M.A.; Bowden, C.A. Platelet 3H-Imipramine Uptake Receptor Density and Serum Serotonin Levels in Patients with Fibromyalgia/Fibrositis Syndrome. J. Rheumatol. 1992, 19, 104–109. [Google Scholar]
- Di Franco, M.; Iannuccelli, C.; Atzeni, F.; Cazzola, M.; Salaffi, F.; Valesini, G.; Sarzi-Puttini, P. Pharmacological Treatment of Fibromyalgia. Clin. Exp. Rheumatol. 2010, 28, S110–S116. [Google Scholar]
- Rus, A.; Molina, F.; Del Moral, M.L.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Catecholamine and Indolamine Pathway: A Case—Control Study in Fibromyalgia. Biol. Res. Nurs. 2018, 20, 577–586. [Google Scholar] [CrossRef]
- Elenkov, I.J.; Chrousos, G.P. Stress Hormones, Proinflammatory and Antiinflammatory Cytokines, and Autoimmunity. Ann. N. Y. Acad. Sci. 2002, 966, 290–303. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference Group (n = 11) | Total FM Patients (n = 34) | FM (n = 17) | FM + CFS (n = 17) | Statistical Significance | |
|---|---|---|---|---|---|
| Gender (%) | Women (100%) | Women (100%) | Women (100%) | Women (100%) | |
| Ethnic group (%) | White (100%) | White (100%) | White (100%) | White (100%) | |
| Duration of FM diagnosed (years) | >2 | >2 | >2 | ||
| Age (years) | 55.81 ± 2.08 | 57.84 ± 1.29 | 57.20 ± 1.84 | 58.41 ± 1.85 | p > 0.05 |
| BMI (kg/m2) | 24.62 ± 0.83 | 27.30 ± 0.91 | 27.42 ± 1.37 | 27.19 ± 1.25 | p > 0.05 |
| Employment status | Chi-Square (X2) p > 0.05 (X2 > 0.05) | ||||
| Blue collar workers (%) | 18.2 | 20.6 | 17.6 | 23.5 | |
| White collar workers (%) | 36.4 | 11.8 | 11.8 | 11.8 | |
| Unemployed (%) | 36.4 | 23.5 | 29.4 | 17.6 | |
| Medical leave (%) | 23.5 | 23.5 | 23.5 | ||
| Retired (%) | 9.1 | 20.6 | 17.6 | 23.5 | |
| Body composition | |||||
| Body fat mass (%) | 36.70 ± 1.57 | 39.61 ± 1.50 | 38.68 ± 1.54 | 40.43 ± 2.51 | p > 0.05 |
| Bone mass (kg) | 2.1 ± 0.05 | 2.11 ± 0.04 | 2.12 ± 0.05 | 2.11 ± 0.05 | p > 0.05 |
| Body water (%) | 43.67 ± 1.00 | 42.55 ± 0.63 | 42.72 ± 0.97 | 42.40 ± 0.86 | p > 0.05 |
| Muscle mass (kg) | 39.00 ± 0.80 | 39.48 ± 1.50 | 39.64 ± 0.86 | 39.34 ± 1.06 | p > 0.05 |
| Visceral fat index | 7.31 ± 0.71 | 9.13 ± 0.47 a | 9.10 ± 0.58 a | 9.14 ± 0.79 a | p < 0.05 |
| RG | Total FM Patients | FM | FM + CFS | |
|---|---|---|---|---|
| Beck’s Depression score | 6.00 ± 1.37 | 20.68 ± 2.21 aaa | 17.15 ± 3.12 aa | 23.99 ± 2.97 aaa |
| Perceived Stress score | 20.09 ± 2.60 | 31.03 ± 1.79 aaa | 28.60 ± 2.57 aa | 33.30 ± 2.41 aaa |
| State-Trait Anxiety score | 15.18 ± 2.29 | 35.65 ± 2.01 aaa | 34.42 ± 2.99 aaa | 36.80 ± 2.79 aaa |
| Healthy Life and Personal Control score | 70.72 ± 2.36 | 66.75 ± 1.90 | 66.35 ± 1.60 | 67.13 ± 3.43 |
| Brief Pain Inventory score | 1.31 ± 0.48 | 6.12 ± 0.25 aaa | 5.76 ± 0.38 aaa | 6.46 ± 0.33 aaa |
| Brief Fatigue Inventory score | 1.46 ± 0.47 | 6.75 ± 0.33 aaa | 6.13 ± 0.53 aaa | 7.33 ± 0.36 aaa * |
| Fibromyalgia Impact score | 3.5 ± 1.48 | 54.25 ± 2.41 aaa | 54.90 ± 3.98 aaa | 53.70 ± 3.04 aaa |
| Fear of COVID-19 score | 12.54 ± 1.39 | 17.62 ± 1.35 aa | 17.92 ± 2.18 a | 17.33 ± 1.72 a |
| Coronavirus Anxiety score | 0.18 ± 0.12 | 4.41 ± 1.01 aaa | 4.21 ± 1.49 aa | 4.60 ± 1.43 aa |
| RG | Total FM Patients | |
|---|---|---|
| IL-8 (pg/mL) | 23.04 ± 3.35 | 26.24 ± 1.91 |
| IL-10 (>LLD) | 9.09% | 15.62% |
| Cortisol (pg/mL) | 121,848.21 ± 15,010.97 | 158,072.90 ± 1413.34 a |
| DHEA (ng/mL) | 5.41 ± 0.88 | 4.48 ± 0.52 |
| Noradrenaline (pg/mL) | 168.48 ± 8.42 | 188.19 ± 6.33 a |
| Adrenaline (pg/mL) | 32.32 ± 4.17 | 33.31 ± 1.46 |
| Serotonin (ng/mL) | 271.07 ± 79.18 | 156.60 ± 14.29 aa |
| Oxytocin (pg/mL) | 1248.81 ± 120.08 | 1447.08 ± 93.56 |
| RG | Total FM Patients | |
|---|---|---|
| Metabolic rate (METs) | 1.61 ± 0.09 | 1.46 ± 0.04 |
| Activity bouts (<1 min) | 95.90 ± 13.36 | 67.27 ± 6.33 a |
| Total Time in Activity bouts (min) | 1968.00 ± 334.77 | 1190.51 ± 135.44 a |
| Average Time per Activity bout (min) | 19.33 ± 1.18 | 16.68 ± 0.73 a |
| Steps count (nº steps) | 109,631.00 ± 9800.09 | 76,069.51 ± 4841.51 aa |
| Sedentary bouts (<1 min) | 114.50 ± 8.98 | 126.96 ± 6.96 |
| Total Time in Sedentary bouts (min) | 2567.00 ± 131.44 | 2902.41 ± 142.54 a |
| Average Time per Sedentary bout (min) | 23.07 ± 1.21 | 23.28 ± 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otero, E.; Gálvez, I.; Ortega, E.; Hinchado, M.D. Influence of Chronic Fatigue Syndrome Codiagnosis on the Relationship between Perceived and Objective Psychoneuro-Immunoendocrine Disorders in Women with Fibromyalgia. Biomedicines 2023, 11, 1488. https://doi.org/10.3390/biomedicines11051488
Otero E, Gálvez I, Ortega E, Hinchado MD. Influence of Chronic Fatigue Syndrome Codiagnosis on the Relationship between Perceived and Objective Psychoneuro-Immunoendocrine Disorders in Women with Fibromyalgia. Biomedicines. 2023; 11(5):1488. https://doi.org/10.3390/biomedicines11051488
Chicago/Turabian StyleOtero, Eduardo, Isabel Gálvez, Eduardo Ortega, and María Dolores Hinchado. 2023. "Influence of Chronic Fatigue Syndrome Codiagnosis on the Relationship between Perceived and Objective Psychoneuro-Immunoendocrine Disorders in Women with Fibromyalgia" Biomedicines 11, no. 5: 1488. https://doi.org/10.3390/biomedicines11051488
APA StyleOtero, E., Gálvez, I., Ortega, E., & Hinchado, M. D. (2023). Influence of Chronic Fatigue Syndrome Codiagnosis on the Relationship between Perceived and Objective Psychoneuro-Immunoendocrine Disorders in Women with Fibromyalgia. Biomedicines, 11(5), 1488. https://doi.org/10.3390/biomedicines11051488