
Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms


Abstract
1. Introduction
2. Patients and Methods
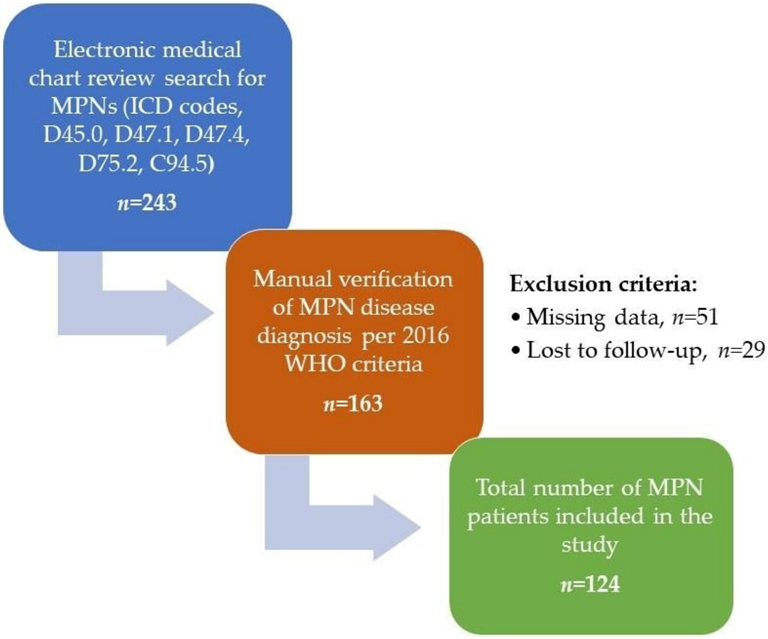
2.1. Study Design and Patient Population
2.2. Statistics
3. Results
3.1. Prevalence of Polypharmacy, PIMs, and DDIs in MPN Patients and their Clinical Correlations
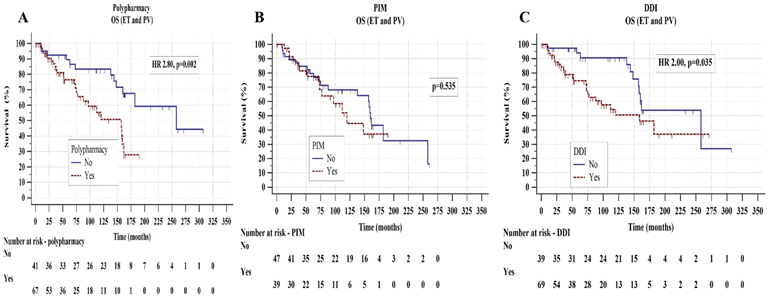
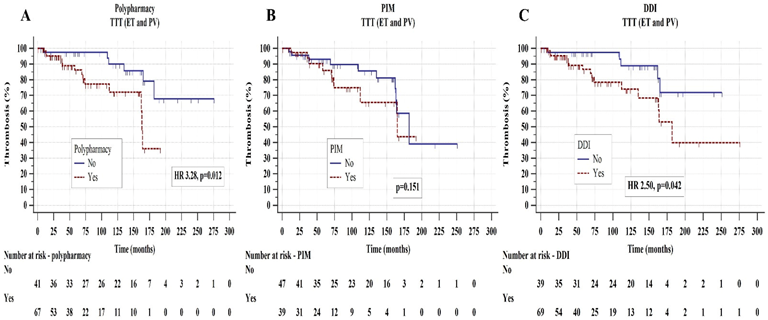
3.2. Survival Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krecak, I.; Lucijanic, M.; Verstovsek, S. Advances in Risk Stratification and Treatment of Polycythemia Vera and Essential Thrombocythemia. Curr. Hematol. Malign-Rep. 2022, 17, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A. Primary myelofibrosis: 2021 update on diagnosis, risk-stratification and management. Am. J. Hematol. 2020, 96, 145–162. [Google Scholar] [CrossRef] [PubMed]
- James, C.; Ugo, V.; Le Couédic, J.-P.; Staerk, J.; Delhommeau, F.; Lacout, C.; Garçon, L.; Raslova, H.; Berger, R.; Bennaceur-Griscelli, A.; et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature 2005, 434, 1144–1148. [Google Scholar] [CrossRef]
- Kralovics, R.; Passamonti, F.; Buser, A.S.; Teo, S.-S.; Tiedt, R.; Passweg, J.R.; Tichelli, A.; Cazzola, M.; Skoda, R.C. A Gain-of-Function Mutation of JAK2 in Myeloproliferative Disorders. N. Engl. J. Med. 2005, 352, 1779–1790. [Google Scholar] [CrossRef] [PubMed]
- Klampfl, T.; Gisslinger, H.; Harutyunyan, A.S.; Nivarthi, H.; Rumi, E.; Milosevic, J.D.; Them, N.C.C.; Berg, T.; Gisslinger, B.; Pietra, D.; et al. Somatic Mutations of Calreticulin in Myeloproliferative Neoplasms. N. Engl. J. Med. 2013, 369, 2379–2390. [Google Scholar] [CrossRef]
- Nangalia, J.; Massie, C.E.; Baxter, E.J.; Nice, F.L.; Gundem, G.; Wedge, D.C.; Avezov, E.; Li, J.; Kollmann, K.; Kent, D.G.; et al. Somatic CALR Mutations in Myeloproliferative Neoplasms with Nonmutated JAK2. N. Engl. J. Med. 2013, 369, 2391–2405. [Google Scholar] [CrossRef]
- Hasselbalch, H.C. Perspectives on chronic inflammation in essential thrombocythemia, polycythemia vera, and myelofibrosis: Is chronic inflammation a trigger and driver of clonal evolution and development of accelerated atherosclerosis and second cancer? Blood 2012, 119, 3219–3225. [Google Scholar] [CrossRef]
- Mesa, R.; Palmer, J.; Eckert, R.; Huberty, J. Quality of Life in Myeloproliferative Neoplasms: Symptoms and Management Implications. Hematol. Clin. N. Am. 2021, 35, 375–390. [Google Scholar] [CrossRef]
- Verstovsek, S.; Yu, J.; Scherber, R.M.; Verma, S.; Dieyi, C.; Chen, C.-C.; Parasuraman, S. Changes in the incidence and overall survival of patients with myeloproliferative neoplasms between 2002 and 2016 in the United States. Leuk. Lymphoma 2021, 63, 694–702. [Google Scholar] [CrossRef]
- Tefferi, A.; Rumi, E.; Finazzi, G.; Gisslinger, H.; Vannucchi, A.M.; Rodeghiero, F.; Randi, M.L.; Vaidya, R.; Cazzola, M.; Rambaldi, A.; et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: An international study. Leukemia 2013, 27, 1874–1881. [Google Scholar] [CrossRef]
- Tefferi, A.; Guglielmelli, P.; Larson, D.R.; Finke, C.; Wassie, E.A.; Pieri, L.; Gangat, N.; Fjerza, R.; Belachew, A.A.; Lasho, T.L.; et al. Long-term survival and blast transformation in molecularly annotated essential thrombocythemia, polycythemia vera, and myelofibrosis. Blood 2014, 124, 2507–2513. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.; Soric, E.; Sabljic, A.; Galusic, D.; Holik, H.; Perisa, V.; Peric, M.M.; Zekanovic, I.; Kusec, R. Patients with post polycythemia vera myelofibrosis might experience increased thrombotic risk in comparison to primary and post essential thrombocythemia myelofibrosis. Leuk. Res. 2022, 119, 106905. [Google Scholar] [CrossRef]
- Barbui, T.; Tefferi, A.; Vannucchi, A.M.; Passamonti, F.; Silver, R.T.; Hoffman, R.; Verstovsek, S.; Mesa, R.; Kiladjian, J.-J.; Hehlmann, R.; et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: Revised management recommendations from European LeukemiaNet. Leukemia 2018, 32, 1057–1069. [Google Scholar] [CrossRef]
- Barbui, T.; Carobbio, A.; Rumi, E.; Finazzi, G.; Gisslinger, H.; Rodeghiero, F.; Randi, M.L.; Rambaldi, A.; Gisslinger, B.; Pieri, L.; et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood 2014, 124, 3021–3023. [Google Scholar] [CrossRef]
- Krečak, I.; Holik, H.; Coha, B.; Perić, M.M.; Zekanović, I.; Krečak, M.V.; Gverić-Krečak, V.; Lucijanić, M. Low-density lipoprotein (LDL) and the risk of thrombotic events in essential thrombocythemia and polycythemia vera. Ann. Hematol. 2021, 100, 1335–1336. [Google Scholar] [CrossRef]
- Krečak, I.; Lucijanić, M.; Gverić-Krečak, V.; Duraković, N. Hyperuricemia might promote thrombosis in essential thrombocythemia and polycythemia vera. Leuk. Lymphoma 2020, 61, 1744–1747. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.; Galusic, D.; Sedinic, M.; Holik, H.; Perisa, V.; Peric, M.M.; Zekanovic, I.; Stoos-Veic, T.; Pejsa, V.; et al. Higher serum uric acid is associated with higher risks of thrombosis and death in patients with primary myelofibrosis. Wien. Klin. Wochenschr. 2022, 134, 97–103. [Google Scholar] [CrossRef]
- Lucijanic, M.; Krecak, I.; Kusec, R. Renal disease associated with chronic myeloproliferative neoplasms. Expert Rev. Hematol. 2022, 15, 93–96. [Google Scholar] [CrossRef]
- Krečak, I.; Holik, H.; Martina, M.P.; Zekanović, I.; Coha, B.; Gverić-Krečak, V. Chronic kidney disease could be a risk factor for thrombosis in essential thrombocythemia and polycythemia vera. Int. J. Hematol. 2020, 112, 377–384. [Google Scholar] [CrossRef]
- Lucijanic, M.; Galusic, D.; Krecak, I.; Sedinic, M.; Holik, H.; Perisa, V.; Peric, M.M.; Zekanovic, I.; Stoos-Veic, T.; Kusec, R. Reduced renal function strongly affects survival and thrombosis in patients with myelofibrosis. Ann. Hematol. 2020, 99, 2779–2785. [Google Scholar] [CrossRef]
- Sørensen, A.L.; Knudsen, T.A.; Skov, V.; Kjær, L.; Holm, N.; Ellervik, C.; Hasselbalch, H.C. Smoking impairs molecular response, and reduces overall survival in patients with chronic myeloproliferative neoplasms: A retrospective cohort study. Br. J. Haematol. 2020, 193, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Vannucchi, A.M. To be, or not to be. Blood 2020, 135, 1617–1618. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, S.; Santoro, M.; Accurso, V.; Agliastro, G.; Raso, S.; Di Piazza, F.; Perez, A.; Bono, M.; Russo, A.; Siragusa, S. Cardiovascular Risk in Polycythemia Vera: Thrombotic Risk and Survival: Can Cytoreductive Therapy Be Useful in Patients with Low-Risk Polycythemia Vera with Cardiovascular Risk Factors? Oncol. Res. Treat. 2020, 43, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Krečak, I.; Perić, M.M.; Zekanović, I.; Holik, H.; Coha, B.; Gverić-Krečak, V.; Lucijanić, M. No Impact of the Increased Number of Cardiovascular Risk Factors on Thrombosis and Survival in Polycythemia Vera. Oncol. Res. Treat. 2021, 44, 201–203. [Google Scholar] [CrossRef]
- Nicol, C.; Lacut, K.; Pan-Petesch, B.; Lippert, E.; Ianotto, J.-C. Hemorrhage in Essential Thrombocythemia or Polycythemia Vera: Epidemiology, Location, Risk Factors, and Lessons Learned from the Literature. Thromb. Haemost. 2020, 121, 553–564. [Google Scholar] [CrossRef]
- Kaifie, A.; for the Study Alliance Leukemia (SAL); Kirschner, M.; Wolf, D.; Maintz, C.; Hänel, M.; Gattermann, N.; Gökkurt, E.; Platzbecker, U.; Hollburg, W.; et al. Bleeding, thrombosis, and anticoagulation in myeloproliferative neoplasms (MPN): Analysis from the German SAL-MPN-registry. J. Hematol. Oncol. 2016, 9, 18. [Google Scholar] [CrossRef]
- Wille, K.; Huenerbein, K.; Jagenberg, E.; Sadjadian, P.; Becker, T.; Kolatzki, V.; Meixner, R.; Marchi, H.; Fuchs, C.; Griesshammer, M. Bleeding complications in bcr-abl-negative myeloproliferative neoplasms (MPN): A retrospective single-center study of 829 MPN patients. Eur. J. Haematol. 2021, 108, 154–162. [Google Scholar] [CrossRef]
- Kantor, E.D.; Rehm, C.D.; Haas, J.S.; Chan, A.T.; Giovannucci, E.L. Trends in Prescription Drug Use Among Adults in the United States From 1999–2012. JAMA 2015, 314, 1818–1831. [Google Scholar] [CrossRef]
- Morin, L.; Johnell, K.; Laroche, M.-L.; Fastbom, J.; Wastesson, J.W. The epidemiology of polypharmacy in older adults: Register-based prospective cohort study. Clin. Epidemiol. 2018, 10, 289–298. [Google Scholar] [CrossRef]
- Abolbashari, M.; Macaulay, T.E.; Whayne, T.F.; Mukherjee, D.; Saha, S. Polypharmacy in Cardiovascular Medicine: Problems and Promises! Cardiovasc. Hematol. Agents Med. Chem. 2017, 15, 31–39. [Google Scholar] [CrossRef]
- Chen, L.-J.; Trares, K.; Laetsch, D.C.; Nguyen, T.N.M.; Brenner, H.; Schöttker, B. Systematic Review and Meta-Analysis on the Associations of Polypharmacy and Potentially Inappropriate Medication With Adverse Outcomes in Older Cancer Patients. J. Gerontol. Ser. A 2020, 76, 1044–1052. [Google Scholar] [CrossRef]
- Chang, C.-B.; Chen, J.-H.; Wen, C.-J.; Kuo, H.-K.; Lu, I.-S.; Chiu, L.-S.; Wu, S.-C.; Chan, D. Potentially inappropriate medications in geriatric outpatients with polypharmacy: Application of six sets of published explicit criteria. Br. J. Clin. Pharmacol. 2011, 72, 482–489. [Google Scholar] [CrossRef]
- Xing, X.X.; Zhu, C.; Liang, H.Y.; Wang, K.; Chu, Y.Q.; Zhao, L.B.; Jiang, D.C.; Wang, Y.Q.; Yan, S.Y. Associations Between Potentially Inappropriate Medications and Adverse Health Outcomes in the Elderly: A Systematic Review and Meta-analysis. Ann. Pharmacother. 2019, 53, 1005–1019. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Desideri, G.; Castaldo, G.; Lombardi, A.; Mussap, M.; Testa, A.; Pontremoli, R.; Punzi, L.; Borghi, C. Is it time to revise the normal range of serum uric acid levels? Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 1295–1306. [Google Scholar]
- Renom-Guiteras, A.; Meyer, G.; Thürmann, P.A. The EU(7)-PIM list: A list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur. J. Clin. Pharmacol. 2015, 71, 861–875. [Google Scholar] [CrossRef]
- Lexi-Drug Interaction Online; UpToDate, Inc.: Hudson, OH, USA, 2023; (accessed on 10 February 2023).
- Karaoglu, A.O.; Kadikoylu, G.; Yukselen, V.; Yasa, M.H.; Bolaman, Z. Gastrointestinal lesions and Helicobacter pylori in patients with myeloproliferative disorders. Saudi Med. J. 2004, 25, 1913–1916. [Google Scholar]
- Torgano, G.; Mandelli, C.; Massaro, P.; Abbiati, C.; Ponzetto, A.; Bertinieri, G.; Bogetto, S.F.; Terruzzi, E.; De Franchis, R. Gastroduodenal lesions in polycythaemia vera: Frequency and role of Helicobacter pylori. Br. J. Haematol. 2002, 117, 198–202. [Google Scholar] [CrossRef]
- Rocca, B.; Tosetto, A.; Betti, S.; Soldati, D.; Petrucci, G.; Rossi, E.; Timillero, A.; Cavalca, V.; Porro, B.; Iurlo, A.; et al. A randomized double-blind trial of 3 aspirin regimens to optimize antiplatelet therapy in essential thrombocythemia. Blood 2020, 136, 171–182. [Google Scholar] [CrossRef]
- Brochmann, N.; Flachs, E.M.; Christensen, A.I.; Bak, M.; Andersen, C.; Juel, K.; Hasselbalch, H.C.; Zwisler, A.-D.; Rottmann, N. Anxiety and depression in patients with Philadelphia-negative myeloproliferative neoplasms: A nationwide population-based survey in Denmark. Clin. Epidemiol. 2018, 11, 23–33. [Google Scholar] [CrossRef]
- Holik, H.; Krečak, I.; Samardžić, I.; Pilipac, D.; Coha, B.; Gverić-Krečak, V.; Ljubičić, I.V.; Lucijanić, M.; Latić, I.R.; Vinković, L.; et al. PB2054: Hip and knee osteoarthritis in philadelphia chromosome-negative myeloproliferative neoplasms. Hemasphere 2022, 6, 1925–1926. [Google Scholar] [CrossRef]
- Farmer, S.L.H.; Horváth-Puhó, E.; Vestergaard, H.; Hermann, A.P.; Frederiksen, H. Chronic myeloproliferative neoplasms and risk of osteoporotic fractures; a nationwide population-based cohort study. Br. J. Haematol. 2013, 163, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Krečak, I.; Perić, M.M.; Zekanović, I.; Holik, H.; Coha, B.; Gverić-Krečak, V.; Lucijanić, M. Beneficial effect of ACE inhibitors on kidney function in polycythemia vera. Wien. Klin. Wochenschr. 2021, 133, 808–815. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PIMs | Total Number of PIMs = 66 | Main Reason |
|---|---|---|
| Proton pump inhibitors (>8 weeks): pantoprazole, esomeprazole | 15 (22.7%) | Long-term high-dose proton pump inhibitor therapy is associated with an increased risk of Clostridium difficile infection and hip fracture. Inappropriate if used >8 weeks in maximal dose without clear indication. |
| Tramadol | 11 (16.6%) | More adverse effects in older adults; central nervous system side effects such as confusion, vertigo, and nausea. |
| Diazepam | 6 (9.1%) | Risk of falling with hip fracture; prolonged reaction times; psychiatric reactions (can also be paradoxical, e.g., agitation, irritability, hallucinations, psychosis); cognitive impairment; depression. |
| Rivaroxaban | 5 (7.6%) | Limited information on use for older adults; risk of bleeding events; potential unavailability of a reversal agent in case of overdose; risk of bleeding may be higher in cases of severe renal failure. |
| Alprazolam | 3 (4.5%) | Risk of falling with hip fracture; prolonged reaction times; psychiatric reactions (can also be paradoxical, e.g., agitation, irritability, hallucinations, psychosis); cognitive impairment; depression. |
| Ranitidine | 3 (4.5%) | Central nervous adverse effects, including confusion. |
| Bromazepam | 2 (3%) | Risk of falling with hip fracture; prolonged reaction times; psychiatric reactions (can also be paradoxical, e.g., agitation, irritability, hallucinations, psychosis); cognitive impairment; depression. |
| Theophylline | 2 (3%) | Higher risk of central nervous system stimulant effects. |
| Maprotiline | 2 (3%) | Peripheral anticholinergic side effects (e.g., constipation, dry mouth, orthostatic hypotension, cardiac arrhythmia); central anticholinergic side effects (drowsiness, inner unrest, confusion, other types of delirium); cognitive deficit; increased risk of falling. |
| Iron supplements > 325 mg | 2 (3%) | Doses > 325 mg/day do not considerably increase the amount absorbed but greatly increase the incidence of constipation. |
| Etoricoxib | 1 (1.5%) | Very high risk of gastrointestinal bleeding, ulceration, or perforation, which may be fatal; cardiovascular contraindications. |
| Indomethacin | 1 (1.5%) | Very high risk of gastrointestinal bleeding, ulceration, or perforation, which may be fatal;risk of central nervous system disturbances. |
| Ketoprofen | 1 (1.5%) | Very high risk of gastrointestinal bleeding, ulceration, or perforation, which may be fatal. |
| Pramipexole | 1 (1.5%) | Side effects include orthostatic hypotension, gastrointestinal tract symptoms, hallucinations, confusion, insomnia, peripheral edema. |
| Metildigoxine | 1 (1.5%) | Elevated glycoside sensitivity (women > men); risk of intoxication. |
| Verapamil | 1 (1.5%) | May worsen constipation; risk of bradycardia. |
| Moxonidine | 1 (1.5%) | Risk of orthostatic hypotension, bradycardia, syncope, and central nervous system side effects (sedation, depression, cognitive impairment). |
| Amiodarone | 1 (1.5%) | Associated with QT interval problems and risk of provoking torsades de pointes.Data suggest that for most older adults rate control yields a better balance of benefits and harms than rhythm control. |
| Propafenone | 1 (1.5%) | High risk of drug interactions.Data suggest that for most older adults rate control yields a better balance of benefits and harms than rhythm control. |
| Pentoxifylline | 1 (1.5%) | No proven efficacy; unfavorable risk/benefit profile; orthostatic hypotension and fall risks are increased with most vasodilators. |
| Carbamazepine | 1 (1.5%) | Increased risk of SIADH-like syndrome; adverse events like carbamazepine-induced confusion and agitation, atrioventricular block, and bradycardia. |
| Sitagliptin | 1 (1.5%) | Limited safety data are available for adults aged ≥ 75 years old. Subjects aged 65 to 80 years had higher plasma concentrations than younger subjects. Risk of hypoglycemia, dizziness, headache, and peripheral edema. |
| Solifenacin | 1 (1.5%) | Anticholinergic side effects (e.g., constipation, dry mouth, central nervous system side effects); electrocardiogram changes (prolonged QT). |
| Aluminum hydroxide | 1 (1.5%) | Renal excretion of aluminum decreases in older individuals. Risk of central nervous system toxicity. |
| Magnesium hydroxide | 1 (1.5%) | Risk of hypermagnesemia, which is higher in moderate to severe renal failure. |
| D Category (Modify Regimen) | Interaction | Total Number of D Category DDI = 32 |
|---|---|---|
| warfarin—allopurinol | Allopurinol may enhance the anticoagulant effect of vitamin K antagonists. | 5 (15.6%) |
| OPIOID AGONISTS—CENTRAL NERVOUS SYSTEM DEPRESSANTS tramadole- bromazepam/ oxazepam/diazepam/ alprazolam/maprotiline | Central nervous system depressants may enhance the central nervous system depressant effect of opioid agonists. | 5 (15.6%) |
| hydroxyurea—denosumab | Denosumab may enhance the immunosuppressive effects of immunosuppressants. | 3 (9.3%) |
| NONSTEROIDAL ANTI- INFLAMMATORY DRUGS— LOOP DIURETICS etorocoxib—furosemide indomethacin—torasemide | Nonsteroidal anti-inflammatory agents may diminish the diuretic effect of loop diuretics. Loop diuretics may enhance the nephrotoxic effect of nonsteroidal anti-inflammatory agents. | 2 (6.25%) |
| SALICYLATES—NONSELECTIVE NONSTEROIDAL ANTI- INFLAMMATORY DRUGS aspirin—ibuprofen aspirin -ketoprofen | Nonsteroidal anti-inflammatory agents (nonselective) may enhance the adverse/toxic effect of salicylates. An increased risk of bleeding may be associated with the use of this combination. Nonsteroidal anti-inflammatory agents (nonselective) may diminish the cardioprotective effect of salicylates. Salicylates may decrease the serum concentration of nonsteroidal anti-inflammatory agents. | 2 (6.25%) |
| simvastatin—amlodipine | Amlodipine may increase the serum concentration of simvastatin, which is associated with a significant increase in the risk for adverse muscle effects; the dose of simvastatin must be limited to 20 mg if coadministering with amlodipine. | 2 (6.25%) |
| BETA BLOCKERS— ALPHA2-AGONISTS (bisoprolol—brimonidine, timolol—brimonidine) | Alpha2-agonists may enhance the AV-blocking effect of beta-blockers. Sinus node dysfunction may also be enhanced. Beta-blockers may enhance the rebound hypertensive effect of alpha2-agonists when they are abruptly withdrawn. Ophthalmic beta-blockers likely pose a reduced risk. | 2 (6.25%) |
| insulin—dapagliflozin | SGLT2 inhibitors may enhance the hypoglycemic effect of insulins. | 2 (6.25%) |
| insulin—linagliptin | Dipeptidyl peptidase-4 inhibitors may enhance the hypoglycemic effect of insulins. | 1 (3.1%) |
| insulin—dulaglutide | Glucagon-like peptide-1 agonists may enhance the hypoglycemic effect of insulins. | 1 (3.1%) |
| warfarin—indomethacin | Nonselective anti-inflammatory agents may enhance the anticoagulant effect of vitamin K antagonists because they affect platelet aggregation, increasing the risk of gastrointestinal bleeding. | 1 (3.1%) |
| warfarin—amiodarone | Amiodarone may enhance the anticoagulant effect of vitamin K antagonists. Amiodarone may increase the serum concentration of vitamin K antagonists. | 1 (3.1%) |
| simvastatine—amiodarone | Amiodarone may increase serum concentrations of the active metabolite(s) of simvastatin. Amiodarone may increase the serum concentration of simvastatin. | 1 (3.1%) |
| verapamil—atorvastatin | Atorvastatin may increase the serum concentration of verapamil. Verapamil may increase the serum concentration of atorvastatin. | 1 (3.1%) |
| prednisone—potassium | Antacids may decrease the bioavailability of oral corticosteroids. | 1 (3.1%) |
| iron sulphate—potassium | Antacids may decrease the absorption of iron preparations. | 1 (3.1%) |
| risedronate—calcium carbonate | Polyvalent cation-containing products may decrease the serum concentration of bisphosphonate derivates. | 1 (3.1%) |
| C category (monitor therapy) | Interaction | Total number of C category DDI, n = 306 |
| ANTIHYPERTENSIVE AGENTS -LOOP DIURETICS (e.g., bisoprolol—furosemide, hydrochlorothiazide—furosemide, amlodipine—furosemide, lercanidipin—furosemide, and similar combinations) | Loop diuretics may enhance the hypotensive effect of antihypertensive agents. | 43 (14%) |
| ACE-I—THIAZIDE AND THIAZIDE-LIKE DIURETICS (e.g., lisinopril—hydrochlorothiazide, perindopril—indapamide, ramipril—hydrochlorothiazide, and similar combinations) | Thiazide and thiazide-like diuretics may enhance the hypotensive and nephrotoxic effect of ACE inhibitors. | 23 (7.5%) |
| ACE-I—SALICYLATES (perindopril—aspirin, ramipril—aspirin, lisinopril—aspirin) | Salicylates may enhance the neprotoxic effect of ACE inhibitors. Salicylates may diminish the therapeutic effect of ACE inhibitors. | 21 (6.8%) |
| ANTIDIABETIC AGENTS— BETA-BLOCKERS (metformin—bisoprolol, insulin bisoprolol, dapagliflozin—bisoprolol, and similar combinations) | Beta-blockers may enhance the hypoglycemic effect of antidiabetic agents. | 16 (6.8%) |
| ALLOPURINOL—LOOP DIURETICS (allopurinol—furosemide/torasemide) | Loop diuretics may enhance the adverse/toxic effects of allopurinol. Loop diuretics may increase the serum concentration of allopurinol, specifically the concentration of its active metabolite oxypurinol. | 15 (4.9%) |
| SALICYLATES—LOOP DIURETICS (aspirin—furosemide, aspirin—torasemide) | Salicylates may diminish the therapeutic effect of loop diuretics. Loop diuretics may increase the serum concentration of salicylates. | 14 (4.5%) |
| ANTIDIABETIC AGENTS—HYPERGLYCEMIA-ASSOCIATED AGENTS (insulin—furosemide, metformine—hydrochlorothiazide, metformin—furosemide, and similar combinations) | Hyperglycemia-associated agents may diminish the the therapeutic effect of antidiabetic agents. | 14 (4.5%) |
| ALLOPURINOL—ACE INHIBITORS (Allopurinol—lisinopril/ramipril/ perindopril) | ACE inhibitors may enhance the potential for allergic or hypersensitivity reactions to allopurinol. | 13 (4.2%) |
| ALLOPURINOL—THIAZIDE AND THIAZIDE-LIKE DIURETICS (allopurinol -hydrochlorothiazide/ indapamide) | Thiazide and thiazide-like diuretics may enhance the potential for allergic or hypersensitivity reactions to allopurinol. | 12 (3.9%) |
| HYPOTENSION-ASSOCIATED AGENTS—BLOOD PRESSURE LOWERING AGENTS (amiodarone—furosemide, amiodarone—hydrochlorothiazide, amiodarone—lisinopril, bisoprolol -levodopa) | Blood pressure-lowering agents may enhance the hypotensive effect of hypotension-associated agents. | 12 (3.9%) |
| warfarin—tramadol warfarin—paracetamol warfarin—rosuvastatin warfarin—simvastatin warfarin—prednisone warfarin—levothyroxine | Drugs that may enhance the anticoagulant effect of warfarin. | 11 (3.6%) |
| ACE INHIBITORS—LOOP DIURETICS (furosemide—lisinopril, furosemide—perindopril) | Loop diuretics may enhance the hypotensive and nephrotoxic effect of ACE inhibitors. | 8 (2.6%) |
| DIURETICS—OPIOID AGONISTS (furosemide—tramadole, Hydrochlorothiazide— tramadole, indapamide—tramadol) | Opioid agonists may enhance the adverse/toxic effects of diuretics. Opioid agonists may diminish the therapeutic effect of diuretics. | 8 (2.6%) |
| METFORMIN—ACE INHIBITORS (metformin-ramipril/perindopril/ lisinopril) | ACE inhibitors may enhance the adverse/toxic effects of metformin. This includes both a risk for hypoglycemia and lactic acidosis. | 4 (1.3%) |
| warfarin—torasemide warfarin—esomeprazole warfarin—propafenone | Drugs that may increase the serum concentration of warfarin. | 3 (0.9%) |
| Variable | Overall (n = 124) | Polypharmacy (n = 76, 61.3%) | At Least One PIM (n = 46, 38.7%) | At Least One DDI-overall (n = 77, 62.1%) | At Least One DDI-C (n = 74, 61.2%) | At Least One DDI-D (n = 21, 16.9%) |
|---|---|---|---|---|---|---|
| Age, years (median, range) | 70 (21–92) | 72 * vs. 64, p = 0.001 | 76 * vs. 71, p < 0.001 | 72 * vs. 66, p = 0.010 | 72 * vs. 66, p = 0.013 | 78 * vs. 66, p < 0.001 |
| Sex, female | 76 (61.3%) | 74% * vs. 40.4%, p < 0.001 | p = 0.208 | p = 0.068 | p = 0.070 | p = 0.125 |
| ET PV MF MPN-u | 63 (50.8%) 44 (35.5%) 9 (7.3%) 8 (6.5%) | p = 0.689 | p = 0.130 | p = 0.532 | p = 0.573 | p = 0.519 |
| JAK2 mutated CALR mutated Negative/Unknown | 86 (69.4%) 7 (5.6%) 31 (25%) | p = 0.581 | p = 0.159 | p = 0.327 | p = 0.355 | p = 0.909 |
| Palpable splenomegaly (n = 122) | 36 (29.5%) | 21.6% * vs. 41.7% *, p = 0.018 | p = 0.532 | p = 0.386 | p = 0.372 | p = 0.958 |
Prior thrombosis -arterial -venous | 28 (22.6%) 16 (57.1%) 12 (42.8%) | 28.9% *, vs. 12.5%, p = 0.033 p = 0.601 | 34.8% *, vs. 16.4%, p = 0.033 p = 0.617 | p = 0.249 p = 0.722 | p = 0.267 p = 0.827 | p = 0.197 p = 0.386 |
| Disease-related symptoms | 35 (28.2%) | 35.5% * vs. 16.7%, p = 0.023 | p = 0.883 | p = 0.353 | p = 0.287 | p = 0.103 |
| Arterial hypertension | 85 (68.5%) | 85.5% * vs. 41.7%, p < 0.001 | p = 0.481 | 84.4% * vs. 42.%. p < 0.001 | 85.1% * vs. 41.7%, p < 0.001 | p = 0.064 |
| Diabetes mellitus (n = 122) | 15 (12.3%) | p = 0.315 | p = 0.271 | p = 0.348 | p = 0.309 | p = 0.253 |
| Hyperlipidemia | 45 (36.3%) | 46.1% * vs. 20.8%, p = 0.004 | p = 0.613 | 45.5% * vs. 21.3%, p = 0.006 | 44.6% vs. 20.8%, p = 0.009 | p = 0.494 |
| Chronic kidney disease (n = 101) | 15 (14.9%) | p = 0.227 | p = 0.255 | p = 0.198 | p = 0.179 | p = 0.624 |
| Chronic heart failure | 32 (26.4%) | 39.2% * vs. 6.4%, p < 0.001 | p = 0.638 | 38.7% * vs. 6.5%, p < 0.001 | 39.7% * vs. 6.5%, p = 0.001 | 50% * vs. 21.8%, p = 0.009 |
| Atrial fibrillation | 18 (14.5%) | 19.7% * vs. 6.2%, p = 0.038 | p = 0.230 | 19.5% * vs. 6.4%, p = 0.045 | 20.3% * vs. 6.2%, p = 0.033 | 28.6% * vs. 11.7%, p = 0.045 |
| Peptic ulcer disease | 16 (12.9%) | p = 0.322 | 22.9% * vs. 6.6%, p = 0.008 | p = 0.106 | p = 0.126 | p = 0.836 |
| Autoimmune disorders -thyroiditis = 5 -ulcerative colitis = 4 -rheumatoid arthritis = 4 -Raynaud syndrome with undetermined collagenosis = 1 | 12 (9.7%) | 14.5% * vs. 2.1%, p = 0.023 | p = 0.529 | p = 0.732 | p = 0.681 | p = 0.435 |
| Osteoarthritis/ osteoporosis | 18 (14.5%) | 19.7% * vs. 6.2%, p = 0.038 | p = 0.351 | 19.5% * vs. 6.4%, p = 0.045 | p = 0.108 | 33.3% * vs. 10.7%,p = 0.007 |
| Pulmonary diseases -COPD = 7 -asthma 2 -interstitial pulmonary disease = 1 | 10 (8%) | p = 0.867 | p = 0.529 | p = 0.590 | p = 0.638 | p = 0.469 |
| Neurological disorders -Parkinson’s disease = 2 -dementia = 2 -migraine = 1 -vertigo = 1 -epilepsy = 1 | 7 (6.5%) | p = 0.572 | 8.7% * vs. 0%, p = 0.026 | 9.1% * vs. 0%, p = 0.034 | 9.5% * vs. 0%, p = 0.030 | p = 0.848 |
| Psychiatric disorders -alcoholism = 3 -depression = 2 -psychoorganic syndrome = 2 -autism = 1 -anxiety = 1 | 9 (6.5%) | p = 0.732 | 13% * vs. 1.8%, p = 0.027 | p = 0.315 | p = 0.289 | 19% * vs. 4.9%, p = 0.022 |
| Hyperuricemia | 11 (8.9%) | p = 0.144 | p = 0.056 | 13% * vs. 2.1%, p = 0.039 | 12.2% * vs. 2.1%, p = 0.048 | p = 0.340 |
| Liver cirrhosis | 7 (5.6%) | p = 0.173 | 13% * vs. 1.8%, p = 0.027 | p = 0.186 | p = 0.254 | p = 0.848 |
| Smoking (active/prior vs. never) | 9 (7.3%) | p = 0.293 | p = 0.229 | p = 0.770 | p = 0.725 | p = 0.629 |
| Other malignancy -colon cancer = 1 -monoclonal gammopathy of undetermined significance = 1 | 2 (1.6%) | - | - | - | - | - |
| Cytoreduction -hydroxyurea -ruxolitinib -anagrelide -interferons | 102 82.3%) 88 (86.2%) 6 (5.8%) 5 (4.9%) 3 (2.9%) | p = 0.094 | p = 0.345 | p = 0.870 | p = 0.938 | p = 0.864 |
| Aspirin | 75 (60.5%) | p = 0.990 | p = 0.078 | p = 0.177 | p = 0.166 | p = 0.406 |
| Oral anticoagulants | 22 (18%) | 27% * vs. 4.2%, p = 0.001 | 31.1% * vs. 13%, p = 0.007 | 25% * vs. 6.5%, p = 0.010 | 24.7% * vs. 6.4%, p = 0.011 | 42.9% vs. 12.9%, p = 0.001 |
| Total leukocytes (×109/L) | 9.2 (4.4–156.6) | p = 0.280 | p = 0.726 | p = 0.312 | p = 0.303 | p = 0.105 |
| Hemoglobin (g/L) | 143 (48–229) | p = 0.529 | p = 0.397 | p = 0.761 | p = 0.923 | 151 vs. 141, p = 0.010 |
| Hematocrit | 46.2 (14.4–90) | p = 0.340 | p = 0.415 | p = 0.633 | p = 0.734 | 48.9 vs. 45.9, p = 0.005 |
| Platelets (×109/L) | 547 (40–3211) | p = 0.204 | p = 0.419 | p = 0.180 | p = 0.204 | p = 0.201 |
| LDH (IU/L) | 246 (136–529) | p = 0.301 | p = 0.823 | p = 0.358 | p = 0.307 | p = 0.787 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krečak, I.; Pivac, L.; Lucijanić, M.; Skelin, M. Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms. Biomedicines 2023, 11, 1301. https://doi.org/10.3390/biomedicines11051301
Krečak I, Pivac L, Lucijanić M, Skelin M. Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms. Biomedicines. 2023; 11(5):1301. https://doi.org/10.3390/biomedicines11051301
Chicago/Turabian StyleKrečak, Ivan, Ljerka Pivac, Marko Lucijanić, and Marko Skelin. 2023. "Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms" Biomedicines 11, no. 5: 1301. https://doi.org/10.3390/biomedicines11051301
APA StyleKrečak, I., Pivac, L., Lucijanić, M., & Skelin, M. (2023). Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms. Biomedicines, 11(5), 1301. https://doi.org/10.3390/biomedicines11051301