
Combination of Conventional Drugs with Biocompounds Derived from Cinnamic Acid: A Promising Option for Breast Cancer Therapy

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategies and Inclusion Criteria
2.2. Study Selection
2.3. Data Extraction and Analysis
2.4. Risk of Bias Assessment
3. Results and Discussion
3.1. Highlights of Studies Performed in MCF-7 Cell Line (ER+)
3.2. Highlights of Studies Performed on TNBC Cell Lines
3.3. Highlights of the Study Performed in BC Patient’s Tumor Samples
- (a)
- Other cell lines representing different types of BC and treatment-resistant BCs;
- (b)
- Other biocompounds derived from cinnamic acid;
- (c)
- Preclinical animal studies and clinical trials to confirm preclinical in vitro studies and orientate future research;
- (d)
- Exact mode of actions in different BC types.

Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
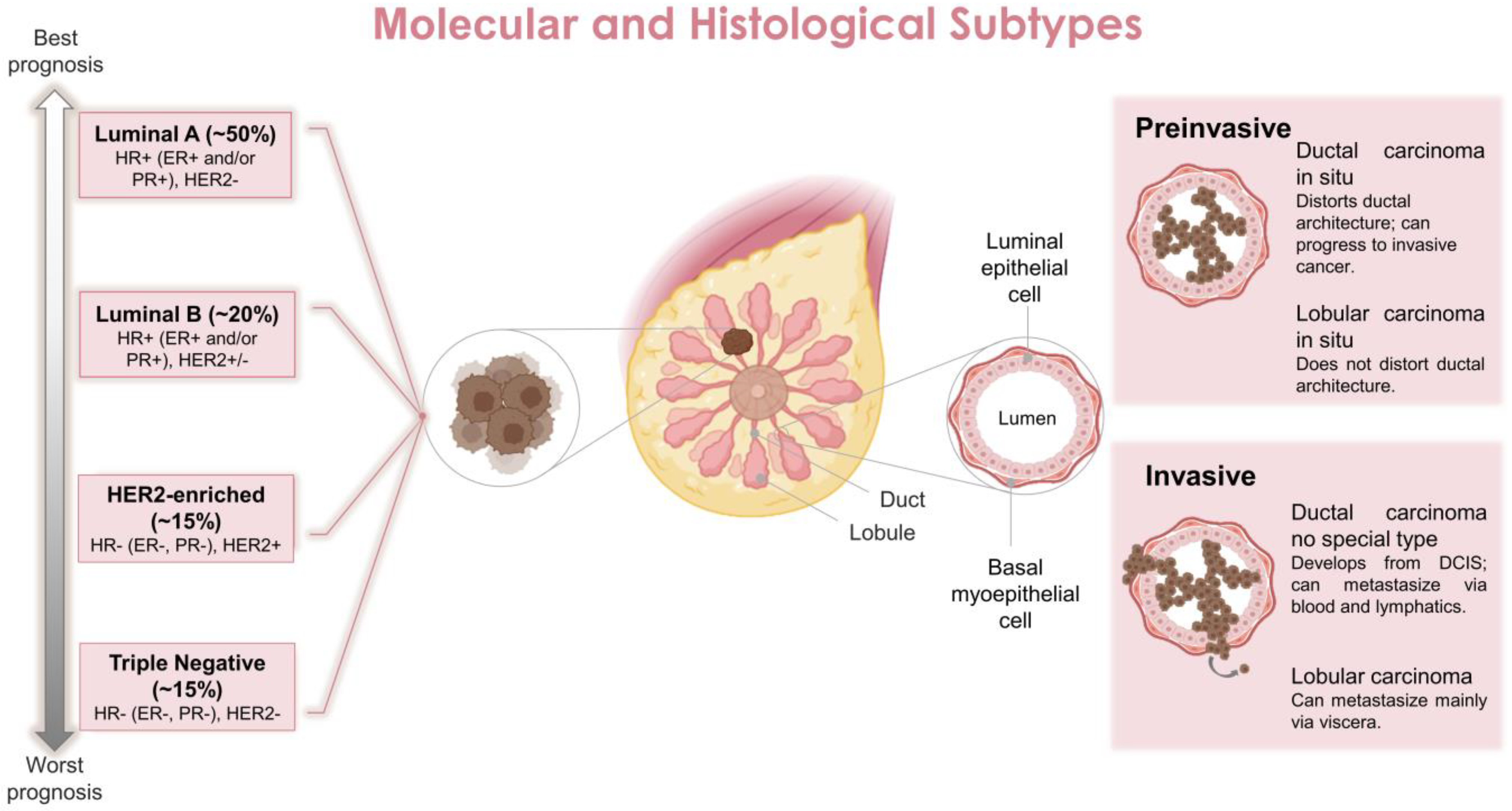
- Norum, J.H.; Andersen, K.; Sørlie, T. Lessons Learned from the Intrinsic Subtypes of Breast Cancer in the Quest for Precision Therapy. Br. J. Surg. 2014, 101, 925–938. [Google Scholar] [CrossRef] [PubMed]
- Shiovitz, S.; Korde, L.A. Genetics of Breast Cancer: A Topic in Evolution. Ann. Oncol. 2015, 26, 1291. [Google Scholar] [CrossRef] [PubMed]
- PDQ® Adult Treatment Editorial Board Breast Cancer Treatment (Adult) (PDQ®). In PDQ Cancer Information Summaries; National Cancer Institute (US): Bethesda, MD, USA, 2022; pp. 1–5.
- Danaei, G.; Vander Hoorn, S.; Lopez, A.D.; Murray, C.J.L.; Ezzati, M. Causes of Cancer in the World: Comparative Risk Assessment of Nine Behavioural and Environmental Risk Factors. Lancet 2005, 366, 1784–1793. [Google Scholar] [CrossRef]
- Sun, Y.S.; Zhao, Z.; Yang, Z.N.; Xu, F.; Lu, H.J.; Zhu, Z.Y.; Shi, W.; Jiang, J.; Yao, P.P.; Zhu, H.P. Risk Factors and Preventions of Breast Cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Makki, J. Diversity of Breast Carcinoma: Histological Subtypes and Clinical Relevance. Clin. Med. Insights. Pathol. 2015, 8, 23–31. [Google Scholar] [CrossRef]
- Dai, X.; Li, T.; Bai, Z.; Yang, Y.; Liu, X.; Zhan, J.; Shi, B. Breast Cancer Intrinsic Subtype Classification, Clinical Use and Future Trends. Am. J. Cancer Res. 2015, 5, 2929. [Google Scholar]
- Russnes, H.G.; Lingjærde, O.C.; Børresen-Dale, A.L.; Caldas, C. Breast Cancer Molecular Stratification: From Intrinsic Subtypes to Integrative Clusters. Am. J. Pathol. 2017, 187, 2152–2162. [Google Scholar] [CrossRef]
- Yu, J.; Mu, Q.; Fung, M.; Xu, X.; Zhu, L.; Ho, R.J.Y. Challenges and Opportunities in Metastatic Breast Cancer Treatments: Nano-Drug Combinations Delivered Preferentially to Metastatic Cells May Enhance Therapeutic Response. Pharmacol. Ther. 2022, 236, 108108. [Google Scholar] [CrossRef]
- Bombonati, A.; Sgroi, D.C. The Molecular Pathology of Breast Cancer Progression. J. Pathol. 2011, 223, 308–318. [Google Scholar] [CrossRef]
- Arpino, G.; Bardou, V.J.; Clark, G.M.; Elledge, R.M. Infiltrating Lobular Carcinoma of the Breast: Tumor Characteristics and Clinical Outcome. Breast Cancer Res. 2004, 6, R149. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Howell, A.; Chrissohou, M.; Swindell, R.I.C.; Hudson, M.; Sellwood, R.A. A Comparison of the Metastatic Pattern of Infiltrating Lobular Carcinoma and Infiltrating Duct Carcinoma of the Breast. Br. J. Cancer 1984, 50, 23–30. [Google Scholar] [CrossRef] [PubMed]
- About Breast Cancer—National Breast Cancer Foundation. Available online: https://www.nationalbreastcancer.org/about-breast-cancer/ (accessed on 1 August 2022).
- Sher, G.; Salman, N.A.; Khan, A.Q.; Prabhu, K.S.; Raza, A.; Kulinski, M.; Dermime, S.; Haris, M.; Junejo, K.; Uddin, S. Epigenetic and Breast Cancer Therapy: Promising Diagnostic and Therapeutic Applications. Semin. Cancer Biol. 2022, 83, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Yersal, O.; Barutca, S. Biological Subtypes of Breast Cancer: Prognostic and Therapeutic Implications. World J. Clin. Oncol. 2014, 5, 412–424. [Google Scholar] [CrossRef] [PubMed]
- Cheang, M.C.U.; Chia, S.K.; Voduc, D.; Gao, D.; Leung, S.; Snider, J.; Watson, M.; Davies, S.; Bernard, P.S.; Parker, J.S.; et al. Ki67 Index, HER2 Status, and Prognosis of Patients with Luminal B Breast Cancer. J. Natl. Cancer Inst. 2009, 101, 736–750. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Fisusi, F.A.; Akala, E.O. Drug Combinations in Breast Cancer Therapy. Pharm. Nanotechnol. 2019, 7, 3. [Google Scholar] [CrossRef]
- American Cancer Society Breast Cancer Treatment | Treatment Options for Breast Cancer. Available online: https://www.cancer.org/cancer/breast-cancer/treatment.html (accessed on 1 August 2022).
- Howell, A.; Pippen, J.; Elledge, R.M.; Mauriac, L.; Vergote, I.; Jones, S.E.; Come, S.E.; Osborne, C.K.; Robertson, J.F.R. Fulvestrant versus Anastrozole for the Treatment of Advanced Breast Carcinoma: A Prospectively Planned Combined Survival Analysis of Two Multicenter Trials. Cancer 2005, 104, 236–239. [Google Scholar] [CrossRef]
- Saputra, E.C.; Huang, L.; Chen, Y.; Tucker-Kellogg, L. Combination Therapy and the Evolution of Resistance: The Theoretical Merits of Synergism and Antagonism in Cancer. Cancer Res. 2018, 78, 2419–2431. [Google Scholar] [CrossRef]
- Hasan, M.; Leak, R.K.; Stratford, R.E.; Zlotos, D.P.; Witt-Enderby, P.A. Drug Conjugates—An Emerging Approach to Treat Breast Cancer. Pharmacol. Res. Perspect. 2018, 6, e00417. [Google Scholar] [CrossRef]
- Chatterjee, N.; Bivona, T.G. Polytherapy and Targeted Cancer Drug Resistance. Trends Cancer 2019, 5, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Negri, M.; Salci, T.P.; Shinobu-Mesquita, C.S.; Capoci, I.R.G.; Svidzinski, T.I.E.; Kioshima, E.S. Early State Research on Antifungal Natural Products. Molecules 2014, 19, 2925. [Google Scholar] [CrossRef] [PubMed]
- DArchivio, M.; Filesi, C.; Di Benedetto, R.; Gargiulo, R.; Giovannini, C.; Masella, R. Polyphenols, Dietary Sources and Bioavailability—PubMed. Ann. -Ist. Super. Sanita 2007, 43, 348–361. [Google Scholar] [PubMed]
- Bravo, L. Polyphenols: Chemistry, Dietary Sources, Metabolism, and Nutritional Significance. Nutr. Rev. 1998, 56, 317–333. [Google Scholar] [CrossRef]
- Croft, K.D. The Chemistry and Biological Effects of Flavonoids and Phenolic Acids. Ann. N. Y. Acad. Sci. 1998, 854, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Michael, N. Clifford Chlorogenic Acids and Other Cinnamates—Nature, Occurrence, Dietary Burden, Absorption and Metabolism. J. Sci. Food Agric. 2000, 80, 1033–1043. [Google Scholar]
- Crozier, A.; Jaganath, I.B.; Clifford, M.N. Dietary Phenolics: Chemistry, Bioavailability and Effects on Health. Nat. Prod. Rep. 2009, 26, 1001–1043. [Google Scholar] [CrossRef] [PubMed]
- Lafay, S.; Gil-Izquierdo, A. Bioavailability of Phenolic Acids. Phytochem. Rev. 2008, 2, 301–311. [Google Scholar] [CrossRef]
- Karakaya, S. Bioavailability of Phenolic Compounds. Crit. Rev. Food Sci. Nutr. 2004, 44, 453–464. [Google Scholar] [CrossRef]
- Mirzaei, S.; Gholami, M.H.; Zabolian, A.; Saleki, H.; Farahani, M.V.; Hamzehlou, S.; Far, F.B.; Sharifzadeh, S.O.; Samarghandian, S.; Khan, H.; et al. Caffeic Acid and Its Derivatives as Potential Modulators of Oncogenic Molecular Pathways: New Hope in the Fight against Cancer. Pharmacol. Res. 2021, 171, 105759. [Google Scholar] [CrossRef]
- Masadah, R.; Ikram, D.; Rauf, S. Effects of Propolis and Its Bioactive Components on Breast Cancer Cell Pathways and the Molecular Mechanisms Involved. Breast Dis. 2021, 40, S15–S25. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 89. [Google Scholar] [CrossRef]
- Faggion, C.M. Guidelines for Reporting Pre-Clinical In Vitro Studies on Dental Materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Suberu, J.O.; Romero-Canelón, I.; Sullivan, N.; Lapkin, A.A.; Barker, G.C. Comparative Cytotoxicity of Artemisinin and Cisplatin and Their Interactions with Chlorogenic Acids in MCF7 Breast Cancer Cells. ChemMedChem 2014, 9, 2791–2797. [Google Scholar] [CrossRef] [PubMed]
- Motawi, T.K.; Abdelazim, S.A.; Darwish, H.A.; Elbaz, E.M.; Shouman, S.A. Could Caffeic Acid Phenethyl Ester Expand the Antitumor Effect of Tamoxifen in Breast Carcinoma? Nutr. Cancer 2016, 68, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Motawi, T.K.; Abdelazim, S.A.; Darwish, H.A.; Elbaz, E.M.; Shouman, S.A. Modulation of Tamoxifen Cytotoxicity by Caffeic Acid Phenethyl Ester in MCF-7 Breast Cancer Cells. Oxid. Med. Cell. Longev. 2016, 2016, 3017108. [Google Scholar] [CrossRef] [PubMed]
- Fouad, M.A.; Sayed-Ahmed, M.M.; Huwait, E.A.; Hafez, H.F.; Osman, A.M.M. Epigenetic Immunomodulatory Effect of Eugenol and Astaxanthin on Doxorubicin Cytotoxicity in Hormonal Positive Breast Cancer Cells. BMC Pharmacol. Toxicol. 2021, 22, 8. [Google Scholar] [CrossRef]
- Zheng, X.; Chen, S.; Yang, Q.; Cai, J.; Zhang, W.; You, H.; Xing, J.; Dong, Y. Salvianolic Acid A Reverses the Paclitaxel Resistance and Inhibits the Migration and Invasion Abilities of Human Breast Cancer Cells by Inactivating Transgelin 2. Cancer Biol. Ther. 2015, 16, 1407. [Google Scholar] [CrossRef]
- Torki, S.; Soltani, A.; Shirzad, H.; Esmaeil, N.; Ghatrehsamani, M. Synergistic Antitumor Effect of NVP-BEZ235 and CAPE on MDA-MB-231 Breast Cancer Cells. Biomed. Pharmacother. 2017, 92, 39–45. [Google Scholar] [CrossRef]
- Islam, S.S.; Al-Sharif, I.; Sultan, A.; Al-Mazrou, A.; Remmal, A.; Aboussekhra, A. Eugenol Potentiates Cisplatin Anti-Cancer Activity through Inhibition of ALDH-Positive Breast Cancer Stem Cells and the NF-ΚB Signaling Pathway. Mol. Carcinog. 2018, 57, 333–346. [Google Scholar] [CrossRef]
- Choi, Y.E.; Park, E. Ferulic Acid in Combination with PARP Inhibitor Sensitizes Breast Cancer Cells as Chemotherapeutic Strategy. Biochem. Biophys. Res. Commun. 2015, 458, 520–524. [Google Scholar] [CrossRef]
- Carranza-Torres, I.E.; Guzmán-Delgado, N.E.; Coronado-Martínez, C.; Bañuelos-García, J.I.; Viveros-Valdez, E.; Morán-Martínez, J.; Carranza-Rosales, P. Organotypic Culture of Breast Tumor Explants as a Multicellular System for the Screening of Natural Compounds with Antineoplastic Potential. Biomed Res. Int. 2015, 2015, 618021. [Google Scholar] [CrossRef] [PubMed]
- Gierach, G.L.; Freedman, N.D.; Andaya, A.; Hollenbeck, A.R.; Park, Y.; Schatzkin, A.; Brinton, L.A. Coffee Intake and Breast Cancer Risk in the NIH-AARP Diet and Health Study Cohort. Int. J. Cancer 2012, 131, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Ulanowska, M.; Olas, B. Biological Properties and Prospects for the Application of Eugenol—A Review. Int. J. Mol. Sci. 2021, 22, 3671. [Google Scholar] [CrossRef] [PubMed]
- Zari, A.T.; Zari, T.A.; Rehman Hakeem, K.; Ferreira de Oliveira, P.; Ribeiro, D.; Ascenso, A.; Santos, C. Anticancer Properties of Eugenol: A Review. Molecules 2021, 26, 7407. [Google Scholar] [CrossRef] [PubMed]
- Huan, S.K.H.; Wang, K.T.; Der Yeh, S.; Lee, C.J.; Lin, L.C.; Liu, D.Z.; Wang, C.C. Antiproliferative and Molecular Mechanism of Eugenol-Induced Apoptosis in Cancer Cells. Molecules 2012, 17, 6277–6289. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, J.E.; Dillon, P.M.; Conaway, M.R.; Silva, C.M.; Parsons, S.J. A Mechanistic Study of the Effect of Doxorubicin/Adriamycin on the Estrogen Response in a Breast Cancer Model. Oncology 2012, 83, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Ponnusamy, L.; Mahalingaiah, P.K.S.; Singh, K.P. Treatment Schedule and Estrogen Receptor-Status Influence Acquisition of Doxorubicin Resistance in Breast Cancer Cells. Eur. J. Pharm. Sci. 2017, 104, 424–433. [Google Scholar] [CrossRef]
- Prinjha, R.K.; Shapland, C.E.; Hsuan, J.J.; Totty, N.F.; Mason, I.J.; Lawson, D. Cloning and Sequencing of CDNAs Encoding the Actin Cross-Linking Protein Transgelin Defines a New Family of Actin-Associated Proteins. Cell Motil. Cytoskeleton 1994, 28, 243–255. [Google Scholar] [CrossRef]
- Yoshino, H.; Chiyomaru, T.; Enokida, H.; Kawakami, K.; Tatarano, S.; Nishiyama, K.; Nohata, N.; Seki, N.; Nakagawa, M. The Tumour-Suppressive Function of MiR-1 and MiR-133a Targeting TAGLN2 in Bladder Cancer. Br. J. Cancer 2011, 104, 808–818. [Google Scholar] [CrossRef]
- Kim, T.R.; Cho, E.W.; Paik, S.G.; Kim, I.G. Hypoxia-Induced SM22α in A549 Cells Activates the IGF1R/PI3K/Akt Pathway, Conferring Cellular Resistance against Chemo- and Radiation Therapy. FEBS Lett. 2012, 586, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-Negative Breast Cancer. N. Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sørile, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Ress, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular Portraits of Human Breast Tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Castro, A.C.; Lin, N.U.; Polyak, K. Insights into Molecular Classifications of Triple-Negative Breast Cancer: Improving Patient Selection for Treatment. Cancer Discov. 2019, 9, 176–198. [Google Scholar] [CrossRef] [PubMed]
- Lyons, T.G. Targeted Therapies for Triple-Negative Breast Cancer. Curr. Treat. Options Oncol. 2019, 20, 82. [Google Scholar] [CrossRef] [PubMed]
- Pickup, M.; Novitskiy, S.; Moses, H.L. The Roles of TGFβ in the Tumour Microenvironment. Nat. Rev. Cancer 2013, 13, 788–799. [Google Scholar] [CrossRef]
- Paplomata, E.; O’Regan, R. The PI3K/AKT/MTOR Pathway in Breast Cancer: Targets, Trials and Biomarkers. Ther. Adv. Med. Oncol. 2014, 6, 154–166. [Google Scholar] [CrossRef]
- Li, C.J.; Chang, J.K.; Chou, C.H.; Wang, G.J.; Ho, M.L. The PI3K/Akt/FOXO3a/P27Kip1 Signaling Contributes to Anti-Inflammatory Drug-Suppressed Proliferation of Human Osteoblasts. Biochem. Pharmacol. 2010, 79, 926–937. [Google Scholar] [CrossRef]
- Yang, J.Y.; Hung, M.C. A New Fork for Clinical Application: Targeting Forkhead Transcription Factors in Cancer. Clin. Cancer Res. 2009, 15, 752–757. [Google Scholar] [CrossRef]
- Yang, J.Y.; Zong, C.S.; Xia, W.; Yamaguchi, H.; Ding, Q.; Xie, X.; Lang, J.Y.; Lai, C.C.; Chang, C.J.; Huang, W.C.; et al. ERK Promotes Tumorigenesis by Inhibiting FOXO3a via MDM2-Mediated Degradation. Nat. Cell Biol. 2008, 10, 138–148. [Google Scholar] [CrossRef]
- Tzivion, G.; Dobson, M.; Ramakrishnan, G. FoxO Transcription Factors; Regulation by AKT and 14-3-3 Proteins. Biochim. Biophys. Acta—Mol. Cell Res. 2011, 1813, 1938–1945. [Google Scholar] [CrossRef]
- Hamunyela, R.H.; Serafin, A.M.; Akudugu, J.M. Strong Synergism between Small Molecule Inhibitors of HER2, PI3K, MTOR and Bcl-2 in Human Breast Cancer Cells. Toxicol. In Vitro 2017, 38, 117–123. [Google Scholar] [CrossRef] [PubMed]
- McEleny, K.; Coffey, R.; Morrissey, C.; Fitzpatrick, J.M.; Watson, R.W.G. Caffeic Acid Phenethyl Ester-Induced PC-3 Cell Apoptosis Is Caspase-Dependent and Mediated through the Loss of Inhibitors of Apoptosis Proteins. BJU Int. 2004, 94, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C.; Kuo, W.H.; Lee, Y.J.; Lin, W.L.; Chou, F.P.; Tseng, T.H. Inhibitory Effect of Caffeic Acid Phenethyl Ester on the Growth of C6 Glioma Cells in Vitro and in Vivo. Cancer Lett. 2006, 234, 199–208. [Google Scholar] [CrossRef]
- He, Y.J.; Liu, B.H.; Xiang, D.B.; Qiao, Z.Y.; Fu, T.; He, Y.H. Inhibitory Effect of Caffeic Acid Phenethyl Ester on the Growth of SW480 Colorectal Tumor Cells Involves β-Catenin Associated Signaling Pathway down-Regulation. World J. Gastroenterol. 2006, 12, 4981. [Google Scholar] [CrossRef]
- Goodwin, C.M.; Rossanese, O.W.; Olejniczak, E.T.; Fesik, S.W. Myeloid Cell Leukemia-1 Is an Important Apoptotic Survival Factor in Triple-Negative Breast Cancer. Cell Death Differ. 2015, 22, 2098–2106. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, G.; Senovilla, L.; Galluzzi, L.; André, F.; Zitvogel, L. Natural and Therapy-Induced Immunosurveillance in Breast Cancer. Nat. Med. 2015, 21, 1128–1138. [Google Scholar] [CrossRef] [PubMed]
- Kida, K.; Ishikawa, T.; Yamada, A.; Shimada, K.; Narui, K.; Sugae, S.; Shimizu, D.; Tanabe, M.; Sasaki, T.; Ichikawa, Y.; et al. Effect of ALDH1 on Prognosis and Chemoresistance by Breast Cancer Subtype. Breast Cancer Res. Treat. 2016, 156, 261–269. [Google Scholar] [CrossRef]
- Ma, F.; Li, H.; Li, Y.; Ding, X.; Wang, H.; Fan, Y.; Lin, C.; Qian, H.; Xu, B. Aldehyde Dehydrogenase 1 (ALDH1) Expression Is an Independent Prognostic Factor in Triple Negative Breast Cancer (TNBC). Medicine 2017, 96, e6561. [Google Scholar] [CrossRef]
- Godwin, P.; Baird, A.M.; Heavey, S.; Barr, M.P.; O’Byrne, K.J.; Gately, K. Targeting Nuclear Factor-Kappa B to Overcome Resistance to Chemotherapy. Front. Oncol. 2013, 3, 120. [Google Scholar] [CrossRef]
- Fathy, M.; Fawzy, M.A.; Hintzsche, H.; Nikaido, T.; Dandekar, T.; Othman, E.M. Eugenol Exerts Apoptotic Effect and Modulates the Sensitivity of HeLa Cells to Cisplatin and Radiation. Molecules 2019, 24, 3979. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Brahmbhatt, K.; Priyani, A.; Ahmed, M.; Rizvi, T.A.; Sharma, C. Eugenol Enhances the Chemotherapeutic Potential of Gemcitabine and Induces Anticarcinogenic and Anti-Inflammatory Activity in Human Cervical Cancer Cells. Cancer Biother. Radiopharm. 2011, 26, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Su, P.; Shi, Y.; Wang, J.; Shen, X.; Zhang, J. Anticancer agents derived from natural cinnamic acids. Anticancer Agents Med. Chem. 2015, 15, 980–987. [Google Scholar] [CrossRef] [PubMed]
- De, P.; Baltas, M.; Bedos-Belval, F. Cinnamic acid derivatives as anticancer agents-a review. Curr. Med. Chem. 2011, 18, 1672–1703. [Google Scholar] [CrossRef] [PubMed]
- McGranahan, N.; Swanton, C. Clonal Heterogeneity and Tumor Evolution: Past, Present, and the Future. Cell 2017, 168, 613–628. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Conventional Drug | Cinnamic Acid Biocompound | BC Cell Line | Main Analysis | Key Findings |
|---|---|---|---|---|---|
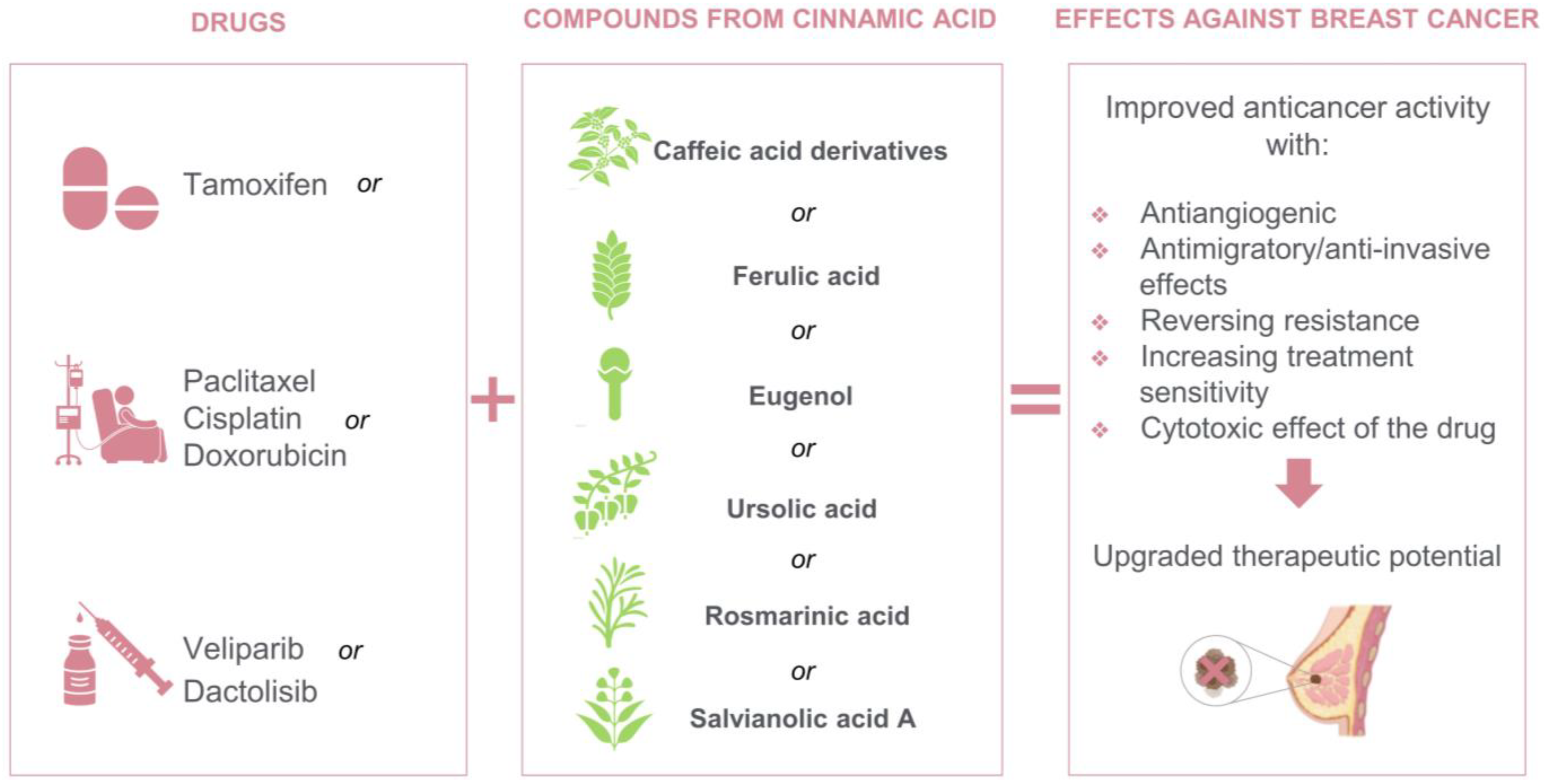
| [37] | Cisplatin | 3-caffeoylquinic acid | MCF-7 | In vitro growth inhibition assays and IC50 modulation experiments | Reduced the IC50 and promoted a 2.5-fold enhancement in the effect of cisplatin. |
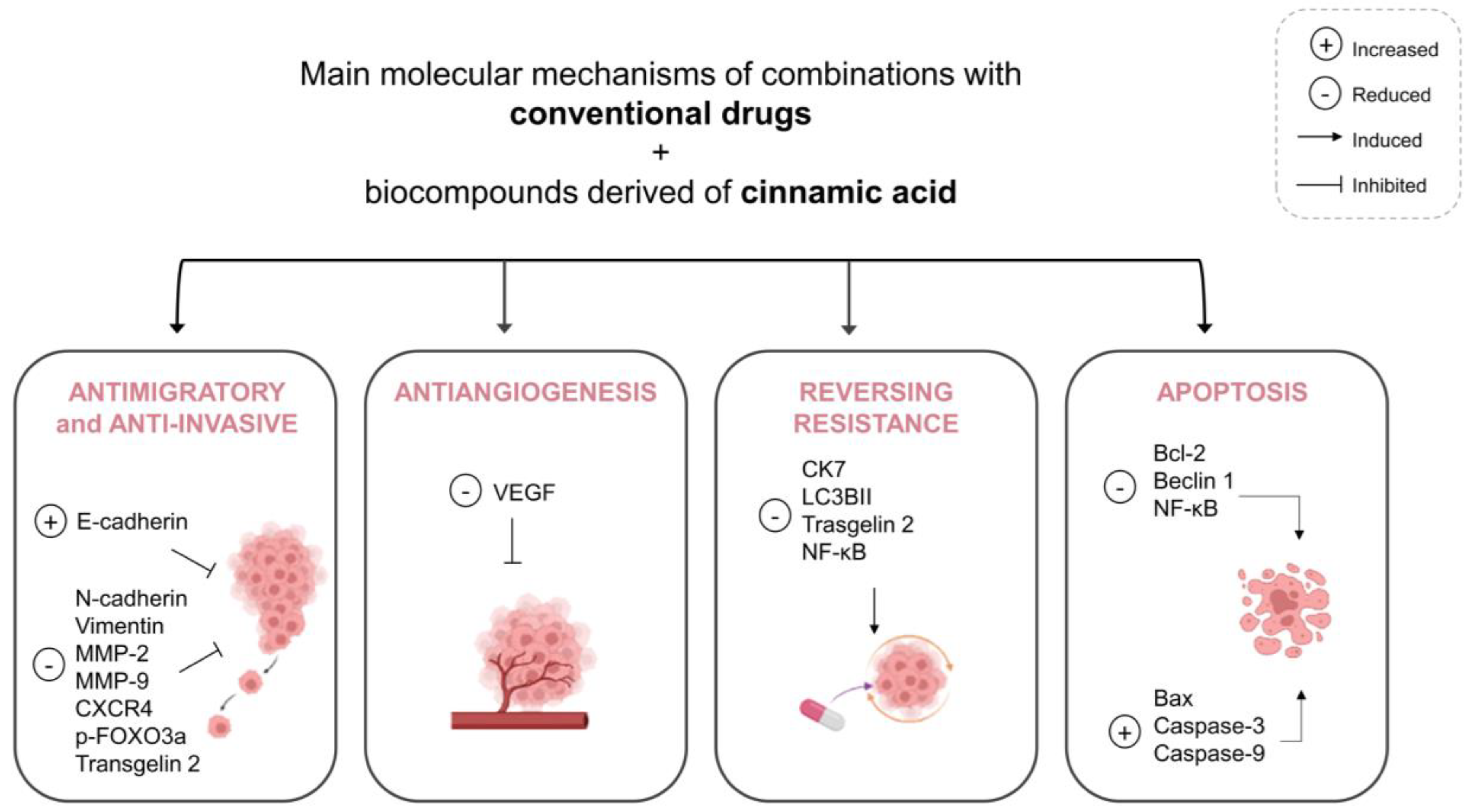
| [38] | Tamoxifen | CAPE | MCF-7 | Cytotoxicity assay, evaluation of drug interaction, determination of caspase-3 activity, caspase-9, Bcl-2, LC3-I and -II, beclin-1 and VEGF. | Evident cytotoxic action with lower tamoxifen and higher CAPE concentrations; increased cell death via caspase-3 e 9 and significant reduction of a factor related with angiogenesis (VEGF). |
| [39] | Tamoxifen | CAPE | MCF-7 | Cytotoxicity assay, evaluation of drug interaction, determination of caspase-9, LC3-II, caspase-3, Bcl-2, beclin-1, VEGF, glutathione, and nitric oxide, analysis for cell death and DNA fragmentation. | Enhanced tamoxifen cytotoxicity via a multitarget approach, including weakening of autophagy, strengthening of both apoptotic and angiostatic potentials and increasing both glutathione and cellular nitric oxide levels. |
| [40] | Doxorubicin | Eugenol | MCF-7 | Cytotoxicity assay, cell cycle and apoptosis analysis, determination of TNFα, IFNγ, FOXP3, Bax, Bcl-2, and caspase 8 genes, analysis of aromatase, EGFR, CK7, and LC3B antibodies and caspase-3, histones extraction and the determination of global H3 and H4 acetylation and activity of multidrug resistance (MDR). | Increased cytotoxic activity of doxorubicin with synergized cytotoxicity in HR+ breast cancer cells, mainly through the non-MDR pathway of histones acetylation and immunomodulation. |
| [41] | Paclitaxel | Salvianolic acid A | MCF-7/ PTX | Cytotoxicity assay, wound healing scratch assay, transwell invasion assay, analysis of E-cadherin, N-cadherin, Vimentin and transgelin 2. | Reversed paclitaxel resistance and inhibited invasion, migration, and growth in a dose-dependent manner. |
| [44] | Veliparib | Ferulic acid | MDA-MB-231 and MCF-7 | Colony assay (cell survival analysis). | Increased sensitivity to the PARP inhibitor in both BC cell lines |
| [42] | Dactolisib | CAPE | MDA-MB-231 | Cytotoxicity assay, analysis of apoptosis, surface expression of CXCR4, analysis of phospho-FOXO3a or pan-Akt antibodies and CXCR-4 and TWIST-1 genes. | Inhibited cell growth and reduced tumor metastasis. |
| [43] | Cisplatin | Eugenol | MDA-MB-231, MDA-MB-468 and BT-20 | Cytotoxicity assay, apoptosis analysis, invasion assay, analysis of caspase 3, caspase 9, Bax, Bcl-2, MMP-2 and MMP-9, colony formation assay and sphere formation assay. | Increased cytotoxicity and pro-apoptotic effects, mediated through suppressing breast cancer stem cells self-renewal and activity. |
| [45] | Paclitaxel | Caffeic acid, rosmarinic acid and ursolic acid | NA | Viability assay, lactate dehydrogenase assessment, histopathological analysis, immunohistochemistry for Ki-67 expression in infiltrating ductal adenocarcinoma specimens. | A synergistic effect was observed. Promoted reduction of >40% in the population of necrotic cells with widespread necrotic areas. The response to the treatments was different in the samples from each patient. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meirelles, L.E.d.F.; Souza, M.V.F.d.; Carobeli, L.R.; Morelli, F.; Mari, N.L.; Damke, E.; Shinobu Mesquita, C.S.; Teixeira, J.J.V.; Consolaro, M.E.L.; Silva, V.R.S.d. Combination of Conventional Drugs with Biocompounds Derived from Cinnamic Acid: A Promising Option for Breast Cancer Therapy. Biomedicines 2023, 11, 275. https://doi.org/10.3390/biomedicines11020275
Meirelles LEdF, Souza MVFd, Carobeli LR, Morelli F, Mari NL, Damke E, Shinobu Mesquita CS, Teixeira JJV, Consolaro MEL, Silva VRSd. Combination of Conventional Drugs with Biocompounds Derived from Cinnamic Acid: A Promising Option for Breast Cancer Therapy. Biomedicines. 2023; 11(2):275. https://doi.org/10.3390/biomedicines11020275
Chicago/Turabian StyleMeirelles, Lyvia Eloiza de Freitas, Maria Vitória Felipe de Souza, Lucimara Rodrigues Carobeli, Fabrício Morelli, Natália Lourenço Mari, Edilson Damke, Cristiane Suemi Shinobu Mesquita, Jorge Juarez Vieira Teixeira, Marcia Edilaine Lopes Consolaro, and Vânia Ramos Sela da Silva. 2023. "Combination of Conventional Drugs with Biocompounds Derived from Cinnamic Acid: A Promising Option for Breast Cancer Therapy" Biomedicines 11, no. 2: 275. https://doi.org/10.3390/biomedicines11020275
APA StyleMeirelles, L. E. d. F., Souza, M. V. F. d., Carobeli, L. R., Morelli, F., Mari, N. L., Damke, E., Shinobu Mesquita, C. S., Teixeira, J. J. V., Consolaro, M. E. L., & Silva, V. R. S. d. (2023). Combination of Conventional Drugs with Biocompounds Derived from Cinnamic Acid: A Promising Option for Breast Cancer Therapy. Biomedicines, 11(2), 275. https://doi.org/10.3390/biomedicines11020275