
Correlation between Neutrophil-to-Lymphocyte Ratio and Cerebral Edema in Children with Severe Diabetic Ketoacidosis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Protocol
2.2. Clinical and Laboratory Data
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics Stratified by the Severity of Neurological Impairment
3.1.1. General Description of the Study Lot
3.1.2. Laboratory Parameters upon Admission
3.2. Correlation and Association Analysis between Different Clinical Parameters and Cerebral Edema
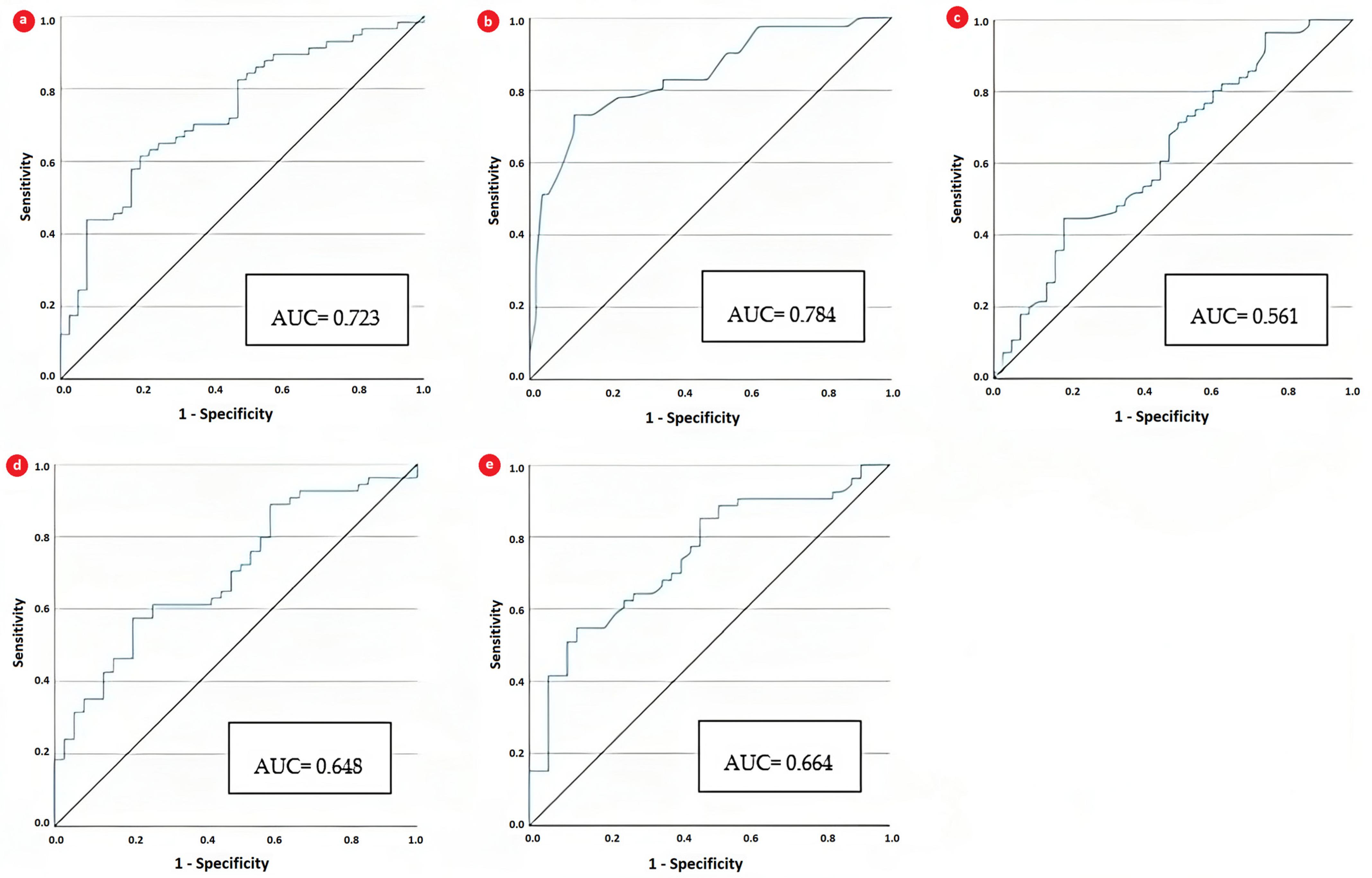
3.3. Diagnostic Performance of NLR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muir, A.B.; Quisling, R.G.; Yang, M.C.; Rosenbloom, A.L. Cerebral Edema in Childhood Diabetic Ketoacidosis: Natural history, radiographic findings, and early identification. Diabetes Care 2004, 27, 1541–1546. [Google Scholar] [CrossRef] [PubMed]
- Wolfsdorf, J.I.; Allgrove, J.; E Craig, M.; Edge, J.; Glaser, N.; Jain, V.; Lee, W.W.; Mungai, L.N.; Rosenbloom, A.L.; Sperling, M.A.; et al. ISPAD Clinical Practice Consensus Guidelines 2014. Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr. Diabetes 2014, 15 (Suppl. S20), 154–179. [Google Scholar] [CrossRef] [PubMed]
- Levin, D.L. Cerebral edema in diabetic ketoacidosis. Pediatr. Crit. Care Med. 2008, 9, 320–329. [Google Scholar] [CrossRef]
- Harris, G.D.; Fiordalisi, I.; Harris, W.L.; Mosovich, L.L.; Finberg, L. Minimizing the risk of brain herniation during treatment of diabetic ketoacidemia: A retrospective and prospective study. J. Pediatr. 1990, 117 Pt 1, 22–31, Correction in J. Pediatr. 1991, 118, 166–167. [Google Scholar] [CrossRef] [PubMed]
- Glaser, N.; Barnett, P.; McCaslin, I.; Nelson, D.; Trainor, J.; Louie, J.; Kaufman, F.; Quayle, K.; Roback, M.; Malley, R.; et al. Risk factors for cerebral edema in children with diabetic ketoacidosis. The Pediatric emergency medicine collaborative research Committee of the American Academy of Pediatrics. N. Engl. J. Med. 2001, 344, 264–269. [Google Scholar] [CrossRef]
- Edge, J.A. Cerebral oedema during treatment of diabetic ketoacidosis: Are we any nearer finding a cause? Diabetes Metab. Res. Rev. 2000, 16, 316–324. [Google Scholar] [CrossRef] [PubMed]
- A Edge, J.; E Ford-Adams, M.; Dunger, D.B. Causes of death in children with insulin dependent diabetes 1990-1996. Arch. Dis. Child. 1999, 81, 318–323. [Google Scholar] [CrossRef]
- Deeb, L.C. Development of fatal cerebral oedema during outpatient therapy for diabetic ketoacidosis. Pract. Diabetes Int. 1989, 6, 212–213. [Google Scholar] [CrossRef]
- Glasgow, A.M. Devastating cerebral edema in diabetic ketoacidosis before therapy. Diabetes Care 1991, 14, 77–78. [Google Scholar] [CrossRef]
- Rosenbloom, A.L. Cerebral edema in diabetic ketoacidosis and other acute devastating complications: Recent observations. Pediatr. Diabetes 2005, 6, 41–49. [Google Scholar] [CrossRef]
- Glaser, N.; Chu, S.; Hung, B.; Fernandez, L.; Wulff, H.; Tancredi, D.; E Odonnell, M. Acute and chronic neuroinflammation is triggered by diabetic ketoacidosis in a rat model. BMJ Open Diabetes Res. Care 2020, 8, e001793. [Google Scholar] [CrossRef] [PubMed]
- Aktas, G. Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus. J. Clin. Med. 2023, 12, 5952. [Google Scholar] [CrossRef] [PubMed]
- Ferro, D.; Matias, M.; Neto, J.; Dias, R.; Moreira, G.; Petersen, N.; Azevedo, E.; Castro, P. Neutrophil-to-Lymphocyte Ratio Predicts Cerebral Edema and Clinical Worsening Early After Reperfusion Therapy in Stroke. Stroke 2021, 52, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, W.H.; Casanova, M.F.; Cudrici, C.D.; Zakranskaia, E.; Venugopalan, R.; Nag, S.; Oglesbee, M.J.; Rus, H. Neuroinflammatory response of the choroid plexus epithelium in fatal diabetic ketoacidosis. Exp. Mol. Pathol. 2007, 83, 65–72. [Google Scholar] [CrossRef][Green Version]
- Tasker, R.C.; Acerini, C.L. Cerebral edema in children with diabetic ketoacidosis: Vasogenic rather than cellular? Pediatr. Diabetes 2014, 15, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, W.H.; Siedlak, S.L.; Wang, Y.; Castellani, R.J.; Smith, M.A. Oxidative damage is present in the fatal brain edema of diabetic ketoacidosis. Brain Res. 2011, 1369, 194–202. [Google Scholar] [CrossRef]
- Mastrocola, R.; Restivo, F.; Vercellinatto, I.; Danni, O.; Brignardello, E.; Aragno, M.; Boccuzzi, G. Oxidative and nitrosative stress in brain mitochondria of diabetic rats. J. Endocrinol. 2005, 187, 37–44. [Google Scholar] [CrossRef]
- Sima, A.A.; Zhang, W.; Kreipke, C.W.; Rafols, J.A.; Hoffman, W.H. Inflammation in diabetic encephalopathy is prevented by C-peptide. Rev. Diabet. Stud. 2009, 6, 37–42. [Google Scholar] [CrossRef]
- Sima, A.A.; Zhang, W.; Muzik, O.; Kreipke, C.W.; Rafols, J.A.; Hoffman, W.H. Sequential abnormalities in Type 1 diabetic encephalopathy and the effects of C-Peptide. Rev. Diabet. Stud. 2009, 6, 211–222. [Google Scholar] [CrossRef]
- Woo, M.M.H.M.; Patterson, E.K.; Clarson, C.; Cepinskas, G.D.; Bani-Yaghoub, M.; Stanimirovic, D.B.; Fraser, D.D. Elevated leukocyte azurophilic enzymes in human diabetic ketoacidosis plasma degrade cerebrovascular endothelial junctional proteins. Crit. Care Med. 2016, 44, e846–e853. [Google Scholar] [CrossRef]
- Cheng, Y.; Yu, W.; Zhou, Y.; Zhang, T.; Chi, H.; Xu, C. Novel predictor of the occurrence of DKA in T1DM patients without infection: A combination of neutrophil/lymphocyte ratio and white blood cells. Open Life Sci. 2021, 16, 1365–1376. [Google Scholar] [CrossRef]
- Dalton, R.R.; Hoffman, W.H.; Passmore, G.G.; Martin, S.L.A. Plasma C-reactive protein levels in severe diabetic ketoacidosis. Ann. Clin. Lab. Sci. 2003, 33, 435–442. [Google Scholar] [PubMed]
- Wan, H.; Wang, Y.; Fang, S.; Chen, Y.; Zhang, W.; Xia, F.; Wang, N.; Lu, Y. Associations between the Neutrophil-to-Lymphocyte Ratio and Diabetic Complications in Adults with Diabetes: A Cross-Sectional Study. J. Diabetes Res. 2020, 2020, 6219545. [Google Scholar] [CrossRef] [PubMed]
- Scutca, A.-C.; Nicoară, D.-M.; Mărăzan, M.; Brad, G.-F.; Mărginean, O. Neutrophil-to-Lymphocyte Ratio Adds Valuable Information Regarding the Presence of DKA in Children with New-Onset T1DM. J. Clin. Med. 2023, 12, 221. [Google Scholar] [CrossRef]
- Mahajan, M.; Prasad, M.K.; Ashok, C.; Guria, R.T.; Marandi, S.; Subrat, S.; Chowdhury, A. The Correlation of the Neutrophil-to-Lymphocyte Ratio With Microvascular Complications in Patients With Diabetes Mellitus. Cureus 2023, 15, e44601. [Google Scholar] [CrossRef]
- American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes 2021. Diabetes Care 2021, 44 (Suppl. S1), S111–S124. [Google Scholar] [CrossRef]
- Kuczmarski, R.R.J.; Ogden, C.L.C.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development. National Center for Health Statistics; Vital and Health Statistics, Series 11, Number 246; U.S. Government Printing Office: Washington, DC, USA, 2002; 190p.
- Walsh, S.; Cook, E.; Goulder, F.; Justin, T.; Keeling, N. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef]
- Smithline, N.; Gardner, K.D. Gaps—Anionic and osmolal. Am. J. Physiol.-Endocrinol. Metab. 1976, 236, 1594–1597. [Google Scholar]
- Katz, M.A. Hyperglycemia-Induced Hyponatremia—Calculation of Expected Serum Sodium Depression. N. Engl. J. Med. 1973, 289, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Jeziorny, K.; Waszczykowska, A.; Barańska, D.; Szadkowska, A.; Młynarski, W.; Zmysłowska, A. Can we effectively predict the occurrence of cerebral edema in children with ketoacidosis in the course of type 1 diabetes?—Case report and literature review. J. Pediatr. Endocrinol. Metab. 2020, 33, 319–322. [Google Scholar] [CrossRef]
- Glaser, N. Cerebral edema in children with diabetic ketoacidosis. Curr. Diabetes Rep. 2001, 1, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Wootton-Gorges, S.L.; Buonocore, M.H.; Kuppermann, N.; Marcin, J.P.; Barnes, P.D.; Neely, E.K.; DiCarlo, J.; McCarthy, T.; Glaser, N.S. Cerebral proton magnetic resonance spectroscopy in children with dia betic ketoacidosis. AJNR Am. J. Neuroradiol. 2007, 28, 895–899. [Google Scholar] [PubMed]
- Glaser, N.S.; Wootton-Gorges, S.L.; Marcin, J.P.; Buonocore, M.H.; DiCarlo, J.; Neely, E.; Barnes, P.; Bottomly, J.; Kuppermann, N. Mechanism of cerebral edema in children with diabetic ketoacidosis. J. Pediatr. 2004, 145, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.I.; Anderson, S.E.; Glaser, N.; O’donnell, M.E. Bumetanide reduces cerebral edema formation in rats with diabetic ketoacidosis. Diabetes 2005, 54, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, R.E.; Hoffman, W.H.; Momin, Z.; Pancholy, A.; Passmore, G.G.; Allison, J. Study of subclinical cerebral edema in diabetic ketoacidosis by magnetic resonance imaging T2 relaxometry and apparent diffusion coefficient maps. Endocr. Res. 2005, 31, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, C.; Vlcek, B.; Del Aguila, M. Risk factors for developing brain herniation during diabetic ketoacidosis. Pediatr. Neurol. 1999, 21, 721–727. [Google Scholar] [CrossRef]
- Hammond, P.; Wallis, S. Cerebral oedema in diabetic ketoaci dosis. BMJ 1992, 305, 203–204. [Google Scholar] [CrossRef][Green Version]
- Muir, A. Therapeutic controversy. Cerebral edema in diabetic ketoacidosis: A look beyond rehydration. J. Clin. Endocrinol. Metab. 2000, 85, 509–513. [Google Scholar] [CrossRef]
- Long, B.; Koyfman, A. Emergency medicine myths: Cerebral edema in pediatric diabetic ketoacidosis and intravenous fluids. J. Emerg. Med. 2017, 53, 212–221. [Google Scholar] [CrossRef]
- Harris, G.; Fiordalisi, I.; Finberg, L. Safe management of diabetic ketoacidemia. J. Pediatr. 1988, 113, 65–67. [Google Scholar] [CrossRef]
- Arieff, A.; Kleeman, C. Cerebral edema in diabetic comas: II: Effects of hyperosmolality, hyperglycemia and insulin in diabetic rabbits. J. Clin. Endocrinol. Metab. 1974, 38, 1057–1067. [Google Scholar] [CrossRef]
- Prockop, L. Hyperglycemia, polyol accumulation, and increased intracranial pressure. Arch. Neurol. 1971, 25, 126–140. [Google Scholar] [CrossRef] [PubMed]
- Glaser, N.S.; Wootton-Gorges, S.L.; Buonocore, M.H.; Tancredi, D.J.; Marcin, J.P.; Caltagirone, R.; Lee, Y.; Murphy, C.; Kuppermann, N. Subclinical cerebral edema in children with diabetic ketoacidosis randomized to 2 different rehydration protocols. Pediatrics 2013, 131, e73–e80. [Google Scholar] [CrossRef]
- Vavilala, M.S.; Richards, T.L.; Roberts, J.S.; Chiu, H.; Pihoker, C.; Bradford, H.; Deeter, K.; Marro, K.I.; Shaw, D. Change in blood-brain barrier permeability during pediatric diabetic ketoacidosis treat ment. Pediatr. Crit. Care Med. 2010, 11, 332–338. [Google Scholar]
- Young, E.; Bradley, R.F. Cerebral edema with irreversible coma in severe diabetic ketoacidosis. N. Engl. J. Med. 1967, 276, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Salem, M.A.K.; Matta, L.F.; Tantawy, A.A.G.; Hussein, M.; Gad, G.I. Single photon emission tomography (SPECT) study of regional cerebral blood flow in normoalbuminuric children and adolescents with type 1 diabetes. Pediatr. Diabetes 2002, 3, 155–162. [Google Scholar] [CrossRef]
- Duck, S.C.; Wyatt, D.T. Factors associated with brain herniation in the treatment of diabetic ketoacidosis. J. Pediatr. 1988, 113, 10–14. [Google Scholar] [CrossRef]
- Arieff, A.I.; Kleeman, C.R. Studies on mechanisms of cerebral edema in diabetic comas. J. Clin. Investig. 1973, 52, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Tornheim, P.A. Regional localization of cerebral edema following fluid and insulin therapy in streptozotocin-diabetic rats. Diabetes 1981, 30, 762–766. [Google Scholar] [CrossRef]
- Isales, C.M.; Min, L.; Hoffman, W.H. Acetoacetate and beta-hydroxybutyrate differentially regulate endothelin-1 and vascular endothelial growth factor in mouse brain microvascular endothelial cells. J. Diabetes Complicat. 1999, 13, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, W.H.; Cheng, C.; Passmore, G.G.; E Carroll, J.; Hess, D. Acetoacetate increases expression of intercellular adhesion molecule-1 (ICAM-1) in human brain microvascular endothelial cells. Neurosci. Lett. 2002, 334, 71–74. [Google Scholar] [CrossRef]
- Hoffman, W.H.; Steinhart, C.M.; El Gammal, T.; Steele, S.; Cuadrado, A.R.; Morse, P.K. Cranial CT in children and adolescents with diabetic ketoacidosis. Am. J. Neuroradiol. 1988, 9, 733–739. [Google Scholar] [PubMed]
- Krane, E.J.; Rockoff, M.A.; Wallman, J.K.; Wolfsdorf, J.I. Subclinical brain swelling in children during treatment of diabetic ketoacidosis. N. Engl. J. Med. 1985, 312, 1147–1151. [Google Scholar] [CrossRef]
- Olivieri, L.; Chasm, R. Diabetic ketoacidosis in the pediatric emergency department. Emerg. Med. Clin. N. Am. 2013, 31, 755–773. [Google Scholar] [CrossRef]
- Rosenbloom, A.L. The management of diabetic ketoacidosis in children. Diabetes Ther. 2010, 1, 103–120. [Google Scholar] [CrossRef] [PubMed]
- Watts, W.; Edge, J.A. How can cerebral edema during treatment of diabetic ketoacidosis be avoided? Pediatr. Diabetes 2014, 15, 271–276. [Google Scholar] [CrossRef]
- Azova, S.; Rapaport, R.; Wolfsdorf, J. Brain injury in children with diabetic ketoacidosis: Review of the literature and a proposed pathophysiologic pathway for the development of cerebral edema. Pediatr. Diabetes. 2021, 22, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Bello, F.; Sotos, J. Cerebral oedema in diabetic ketoacidosis in children. Lancet 1990, 336, 64. [Google Scholar] [CrossRef] [PubMed]
- Finn, B.P.; Power, C.; McSweeney, N.; Breen, D.; Wyse, G.; O’Connell, S.M. Subarachnoid and parenchymal haemorrhages as a complication of severe diabetic ketoacidosis in a preadolescent with new onset type 1 diabetes. Pediatr. Diabetes 2018, 19, 1487–1491. [Google Scholar] [CrossRef]
- Abbas, Q.; Arbab, S.; Haque, A.U.; Humayun, K.N. Spectrum of complications of severe DKA in children in pediatric Intensive Care Unit. Pak. J. Med. Sci. 2018, 34, 106–109. [Google Scholar] [CrossRef]
- Dunger, D.B.; Sperling, M.A.; Acerini, C.L.; Bohn, D.J.; Daneman, D.; Danne, T.P.; Glaser, N.S.; Hanas, R.; Hintz, R.L.; Levitsky, L.L.; et al. European society for paediatric endocrinology/lawson wilkins pediatric endocrine society consensus statement on diabetic ketoacidosis in children and adolescents. Pediatrics 2004, 113, e133–e140. [Google Scholar] [CrossRef] [PubMed]
- Mozzillo, E.; D’Amico, A.; Fattorusso, V.; Carotenuto, B.; Buono, P.; De Nitto, E.; Falco, M.; Franzese, A. Cerebral Accidents in Pediatric Diabetic Ketoacidosis: Different Complications and Different Evolutions. Horm. Res. Paediatr. 2015, 84, 139–144. [Google Scholar] [CrossRef] [PubMed]
- A Edge, J.; Hawkins, M.M.; Winter, D.L.; Dunger, D.B.; Greene, S. The risk and outcome of cerebral oedema developing during diabetic ketoacidosis. Arch. Dis. Child. 2001, 85, 16–22. [Google Scholar] [CrossRef]
- Lawrence, S.E.; Cummings, E.A.; Gaboury, I.; Daneman, D. Population-based study of incidence and risk factors for cerebral edema in pediatric diabetic ketoacidosis. J. Pediatr. 2005, 146, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Edge, J.A.; Jakes, R.W.; Roy, Y.; Hawkins, M.; Winter, D.; Ford-Adams, M.E.; Murphy, N.P.; Bergomi, A.; Widmer, B.; Dunger, D.B. The UK case–control study of cerebral oedema complicating diabetic ketoacidosis in children. Diabetologia 2006, 49, 2002–2009. [Google Scholar] [CrossRef]
- Japan and Pittsburgh Childhood Diabetes Research Groups. Coma at the onset of young insulin-dependent diabetes in Japan: The results of a nationwide survey. Diabetes. 1985, 34, 1241–1246. [Google Scholar] [CrossRef]
- Nyenwe, E.A.; Razavi, L.N.; Kitabchi, A.E.; Khan, A.N.; Wan, J.Y. Acidosis: The prime determinant of depressed sensorium in diabetic ketoacidosis. Diabetes Care 2010, 33, 1837–1839. [Google Scholar] [CrossRef]
- Yaneva, N.Y.; Konstantinova, M.M.; Iliev, D.I. Risk factors for cerebral oedema in children and adolescents with diabetic ketoacidosis. Biotechnol. Biotechnol. Equip. 2016, 30, 1142–1147. [Google Scholar] [CrossRef]
- Tiwari, L.K.; Jayashree, M.; Singhi, S. Risk factors for cerebral edema in diabetic ketoacidosis in a developing country: Role of fluid refractory shock. Pediatr. Crit. Care Med. 2012, 13, e91–e96. [Google Scholar] [CrossRef]
- Rosenbloom, A. Hyperglycemic Crises and their Complications in Children. J. Pediatr. Endocrinol. Metab. 2007, 20, 5–18. [Google Scholar] [CrossRef]
- Marcin, J.P.; Glaser, N.; Barnett, P.; McCaslin, I.; Nelson, D.; Trainor, J.; Louie, J.; Kaufman, F.; Quayle, K.; Roback, M.; et al. Factors associated with adverse outcomes in children with diabetic ketoacidosis-related cerebral edema. J. Pediatr. 2002, 141, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Bureau, M.A.; Bégin, R.; Berthiaume, Y.; Shapcott, D.; Khoury, K.; Gagnon, N. Cerebral hypoxia from bicarbonate infusion in diabetic acidosis. J. Pediatr. 1980, 96, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Durr, J.A.; Hoffman, W.H.; Sklar, A.H.; El Gammal, T.; Steinhart, C.M. Correlates of brain edema in uncontrolled IDDM. Diabetes 1992, 41, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, A.L.; Riley, W.J.; Weber, F.T.; Malone, J.I.; Donnelly, W.H. Cerebral edema complicating diabetic ketoacidosis in childhood. J. Pediatr. 1980, 96, 357–361. [Google Scholar] [CrossRef]
- Rosenbloom, A.L. Intracerebral Crises During Treatment of Diabetic Ketoacidosis. Diabetes Care 1990, 13, 22–33. [Google Scholar] [CrossRef]
- Hale, P.; Rezvani, I.; Braunstein, A.; Lipman, T.; Martinez, N.; Garibaldi, L. Factors predicting cerebral edema in young children with diabetic ketoacidosis and new onset type I diabetes. Acta Paediatr. 1997, 86, 626–631. [Google Scholar] [CrossRef]
- A Edge, J.; Roy, Y.; Bergomi, A.; Murphy, N.P.; E Ford-Adams, M.; Ong, K.K.; Dunger, D.B. Conscious level in children with diabetic ketoacidosis is related to severity of acidosis and not to blood glucose concentration. Pediatr. Diabetes 2006, 7, 11–15. [Google Scholar] [CrossRef]
- Hoorn, E.J.; Carlotti, A.P.; Costa, L.A.; MacMahon, B.; Bohn, G.; Zietse, R.; Halperin, M.L.; Bohn, D. Preventing a drop in effective plasma osmolality to minimize the likelihood of cerebral edema during treatment of children with diabetic ketoacidosis. J. Pediatr. 2007, 150, 467–473. [Google Scholar] [CrossRef]
- Close, T.E.; Cepinskas, G.; Omatsu, T.; Rose, K.L.; Summers, K.; Patterson, E.K.; Fraser, D.D. Diabetic ketoacidosis elicits systemic inflammation associated with cerebrovascular endothelial cell dysfunction. Microcirculation 2013, 20, 534–543. [Google Scholar] [CrossRef]
- Lin, B.; Ginsberg, M.D.; Busto, R.; Li, L. Hyperglycemia triggers massive neutrophil deposition in brain following transient ischemia in rats. Neurosci. Lett. 2000, 278, 1–4. [Google Scholar] [CrossRef]
- Omatsu, T.; Cepinskas, G.; Clarson, C.; Patterson, E.K.; Alharfi, I.M.; Summers, K.; Couraud, P.-O.; Romero, I.A.; Weksler, B.; Fraser, D.D. CXCL1/CXCL8 (GROalpha/IL-8) in human diabetic ketoacidosis plasma facilitates leukocyte recruitment to cerebrovascular endothelium in vitro. Am. J. Physiol. Endocrinol. Metab. 2014, 306, E1077–E1084. [Google Scholar] [CrossRef] [PubMed]
- Garro, A.; Chodobski, A.; Szmydynger-Chodobska, J.; Shan, R.; Bialo, S.R.; Bennett, J.; Quayle, K.; Rewers, A.; Schunk, J.E.; Casper, T.C.; et al. Circulating matrix metalloproteinases in children with diabetic ketoacidosis. Pediatr. Diabetes 2016, 18, 95–102. [Google Scholar] [CrossRef]
- Hoffman, W.H.; Cudrici, C.D.; Boodhoo, D.; Tatomir, A.; Rus, V.; Rus, H. Intracerebral matrix metalloproteinase 9 in fatal diabetic ketoacidosis. Exp. Mol. Pathol. 2019, 108, 97–104. [Google Scholar] [CrossRef]
- Poovazhagi, V. Risk factors for mortality in children with diabetic keto acidosis from developing countries. World J. Diabetes 2014, 5, 932–938. [Google Scholar] [PubMed]
- Tecchio, C.; Micheletti, A.; Cassatella, M.A. Neutrophil-derived cytokines: Facts beyond expression. Front. Immunol. 2014, 5, 508. [Google Scholar] [CrossRef]
- Karavanaki, K.; Karanika, E.; Georga, S.; Bartzeliotou, A.; Tsouvalas, M.; Konstantopoulos, I.; Fotinou, A.; Papassotiriou, I.; Karayianni, C. Cytokine response to diabetic ketoacidosis (DKA) in children with type 1 diabetes (T1DM). Endocr. J. 2011, 58, 1045–1053. [Google Scholar] [CrossRef]
- Deeter, K.H.; Roberts, J.S.; Bradford, H.; Richards, T.; Shaw, D.; Marro, K.; Chiu, H.; Pihoker, C.; Lynn, A.; Vavilala, M.S. Hypertension despite dehydration during severe pediatric diabetic ketoacidosis. Pediatr. Diabetes 2011, 12, 295–301. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Horvat, C.M.; Ismail, H.M.; Au, A.K.; Garibaldi, L.; Siripong, N.; Kantawala, S.; Aneja, R.K.; Hupp, D.S.; Kochanek, P.M.; Clark, R.S.B. Presenting predictors and temporal trends of treatment-related outcomes in diabetic ketoacidosis. Pediatr. Diabetes 2018, 19, 985–992. [Google Scholar] [CrossRef]
- Hanas, R.; Lindgren, F.; Lindblad, B. Diabetic ketoacidosis and cerebral oedema in Sweden?a 2-year paediatric population study. Diabet. Med. 2007, 24, 1080–1085. [Google Scholar] [CrossRef]
- Raghupathy, P. Diabetic ketoacidosis in children and adolescents. Indian. J. Endocrinol. Metab. 2015, 19, 55–57. [Google Scholar] [CrossRef]
- Glaser, N.S.; Wootton-Gorges, S.L.; Buonocore, M.H.; Marcin, J.P.; Rewers, A.; Strain, J.; DiCarlo, J.; Neely, E.K.; Barnes, P.; Kuppermann, N. Frequency of sub-clinical cerebral edema in children with diabetic ketoacidosis. Pediatr. Diabetes 2006, 7, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Hom, J.; Sinert, R. Evidence-based emergency medicine/critically appraised topic. Is fluid therapy associated with cerebral edema in children with diabetic ketoacidosis? Ann. Emerg. Med. 2008, 52, 69–75.e1. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Alert (n = 28) | Subclinical Cerebral Edema (n = 59) | Overt Cerebral Edema (n = 11) | p Value |
|---|---|---|---|---|
| Age (years) | 10.2 (4.8, 14) | 9.60 (5.03, 13.01) | 9 (2.4, 12.1) | 0.637 |
| Males % (n) | 64.3 (18) | 42.4 (25) | 27.3 (3) | 0.186 |
| Duration of symptoms (days) | 14 (10, 24.6) | 10 (7, 16) | 14 (6, 30) | 0.099 |
| New onset DKA | 89.3 (25) | 84.7 (50) | 91.6 (11) | 0.351 |
| Overweight % (n) | 10.7 (3) | 10.2 (6) | 18.2 (2) | 0.597 |
| Underweight % (n) | 28.5 (8) | 20.3 (12) | 9.1 (1) | 0.616 |
| Co-infection % (n) | 21.4 (6) | 16.9 (10) | 54.5 (6) | 0.022 |
| Vital signs at presentation, | ||||
| SBPp (mmHg) | 92 (64.5, 97) | 99 (95, 100) | 100 (98, 100) | 0.002 |
| DBPp (mmHg) | 86 (62.5, 97) | 95 (76, 99) | 96 (90, 100) | 0.076 |
| HR (beats/min) | 111.5 (97.6, 128.9) | 130 (117, 142) | 131 (120, 142) | 0.002 |
| RR (respiration/min) | 30 (23.2, 35) | 34 (27.5, 39) | 31 (30, 33) | 0.258 |
| Insulin before admission % (n) | 10.7 (3) | 15.3 (9) | 27.3 (3) | 0.308 |
| Duration of PICU stay (days) | 1 (1, 2) | 2 (1, 2.5) | 4 (3, 4) | <0.001 |
| Time to correction of acidosis (hours) | 9 (7, 12.7) | 21 (16, 25) | 28 (26, 38) | <0.001 |
| Variables | Alert (n = 28) | Subclinical Cerebral Edema (n = 59) | Overt Cerebral Edema (n = 11) | p-Value |
|---|---|---|---|---|
| Venous pH | 7.07 (6.97, 7.08) | 6.97 (6.98, 7.01) | 6.84 (6.80, 6.93) | <0.001 |
| Glycemia (mg/dL) | 445 (383, 532) | 478 (381, 529) | 557 (464, 590) | 0.087 |
| Base excess (mmol/L) | −23.5 (−26, −22) | −26.3 (−28.2, −25) | −29.8 (−30.9, −27.9) | <0.001 |
| Lactate (mmol/L) | 1.78 (1.34, 2.80) | 2.30 (1.49, 3.02) | 1.93 (1.13, 2.02) | 0.170 |
| Corrected sodium (mmol/L) | 144.7 (142.2, 147.2) | 145.4 (143.5, 147.8) | 148.8 (146.5, 151,8) | 0.019 |
| Osmolality (mosmol/L) | 306.7 (301.7, 310.6) | 309.9 (303.4, 317.8) | 320.8 (311.9, 329.5) | 0.005 |
| Creatinine (umol/L) | 53 (44, 66) | 56.5 (39.7, 73.2) | 55 (28, 97) | 0.926 |
| HbA1c (%) | 11.55 (12.62, 14.92) | 11.40 (10.15, 12.68) | 11.31 (10.25, 12.45) | 0.563 |
| Insulinemia (uIU/mL) | 3.82 (2.39, 12.95) | 2.19 (1.14, 11.07) | 1.90 (1.67, 15.7) | 0.156 |
| Basal C-peptide (nmol/L) | 0.402 (0.182, 0.721) | 0.338 (0.218, 0.472) | 0.265 (0.183, 0.508) | 0.605 |
| CRP (mg/L) | 1.18 (0.39, 7.87) | 2.07 (0.82, 7.09) | 12.4 (1.78, 27.3) | 0.078 |
| BUN (mmol/L) | 22.4 (15.5, 26.1) | 24.7 (18.6, 35.5) | 35.1 (29.5, 50.9) | 0.002 |
| Variables | Alert (n = 28) | Subclinical Cerebral Edema (n = 59) | Overt Cerebral Edema (n = 11) | p-Value |
|---|---|---|---|---|
| WBC (×103/mm3) | 14.4 (10.7, 16.6) | 18.8 (13.8 25.5) | 18.5 (8.64, 24.5) | 0.008 |
| Neutrophils (×103/mm3) | 9.34 (6.29, 12.1) | 14.7 (9.80, 20.7) | 14.7 (9.22, 19.6) | 0.001 |
| Lymphocytes (×103/mm3) | 2.95 (2.36, 4.03) | 2.59 (1.96, 3.91) | 1.71 (0.97, 2.91) | 0.042 |
| Monocytes (×103/mm3) | 1.21 (0.85, 1.60) | 1.69 (1.14, 2.47) | 2.37 (1.85, 2.78) | <0.001 |
| Basophiles (×103/mm3) | 0.04 (0.03, 0.05) | 0.04 (0.03, 0.07) | 0.03 (0.02, 0.05) | 0.266 |
| Eosinophiles (×103/mm3) | 0.02 (0, 0.12) | 0.01 (0, 0.03) | 0 (0, 0.01) | 0.026 |
| Immature granulocytes % (×103/mm3) | 0.07 (0.03, 0.13) | 0.15 (0.06, 0.37) | 0.21 (0.09, 0.42) | 0.012 |
| Platelets (×103/mm3) | 328 (294, 402) | 342 (275, 440) | 327 (275, 400) | 0.992 |
| NLR | 2.82 (2.28, 4.23) | 5.66 (3.95, 7.88) | 8.60 (4.73, 12.17) | <0.001 |
| Univariate Model (Groups 1 to 3) | Multivariate Model (Group 1 vs. 2+) r2 = 0.265 | |||
|---|---|---|---|---|
| Variables | Correlation Coefficient | p | B (95%CI) | p |
| Age r | −0.077 | 0.449 | −0.018 (−0.038, 0.003) | 0.088 |
| Gender χ2 | 0.182 | 0.073 | ||
| Coinfection χ2 | 0.186 | 0.071 | ||
| pH r | −0.528 | <0.001 | −1.326 (−2.325, −0.327) | 0.010 |
| Glycemia r | 0.173 | 0.090 | ||
| HbA1c r | 0.092 | 0.288 | ||
| Corrected sodium * r | 0.248 | 0.016 | −0.003 (−0.025, 0.019) | 0.815 |
| BUN r | 0.346 | <0.001 | 0.007 (0.001, 0.013) | 0.042 |
| NLR r | 0.404 | <0.001 | 0.030 (0.001, 0.060) | 0.045 |
| AUC | SE | 95%CI | Sensitivity | Specificity | Cut-Off | p-Value | |
|---|---|---|---|---|---|---|---|
| NLR | 0.723 | 0.051 | 0.619–0.827 | 0.716 | 0.538 | 4.05 | <0.001 |
| pH | 0.784 | 0.052 | 0.682–0.886 | 0.774 | 0.552 | 6.96 | <0.001 |
| Glycemia | 0.561 | 0.064 | 0.435–0.687 | 0.545 | 0.54.8 | 473 | 0.334 |
| Corrected sodium * | 0.600 | 0.061 | 0.481–0.719 | 0.585 | 0.533 | 145.3 | 0.118 |
| Osmolality | 0.648 | 0.058 | 0.534–0.761 | 0.635 | 0.500 | 306.7 | 0.025 |
| BUN | 0.664 | 0.056 | 0.553–0.774 | 0.645 | 0.48.3 | 21.6 | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scutca, A.-C.; Nicoară, D.-M.; Mang, N.; Jugănaru, I.; Brad, G.-F.; Mărginean, O. Correlation between Neutrophil-to-Lymphocyte Ratio and Cerebral Edema in Children with Severe Diabetic Ketoacidosis. Biomedicines 2023, 11, 2976. https://doi.org/10.3390/biomedicines11112976
Scutca A-C, Nicoară D-M, Mang N, Jugănaru I, Brad G-F, Mărginean O. Correlation between Neutrophil-to-Lymphocyte Ratio and Cerebral Edema in Children with Severe Diabetic Ketoacidosis. Biomedicines. 2023; 11(11):2976. https://doi.org/10.3390/biomedicines11112976
Chicago/Turabian StyleScutca, Alexandra-Cristina, Delia-Maria Nicoară, Niculina Mang, Iulius Jugănaru, Giorgiana-Flavia Brad, and Otilia Mărginean. 2023. "Correlation between Neutrophil-to-Lymphocyte Ratio and Cerebral Edema in Children with Severe Diabetic Ketoacidosis" Biomedicines 11, no. 11: 2976. https://doi.org/10.3390/biomedicines11112976
APA StyleScutca, A.-C., Nicoară, D.-M., Mang, N., Jugănaru, I., Brad, G.-F., & Mărginean, O. (2023). Correlation between Neutrophil-to-Lymphocyte Ratio and Cerebral Edema in Children with Severe Diabetic Ketoacidosis. Biomedicines, 11(11), 2976. https://doi.org/10.3390/biomedicines11112976