

Depressive Symptomatology as a Predictor of Cognitive Impairment: Evidence from the Korean Longitudinal Study of Aging (KLOSA), 2006–2020


Abstract
:1. Introduction
2. Materials and Methods
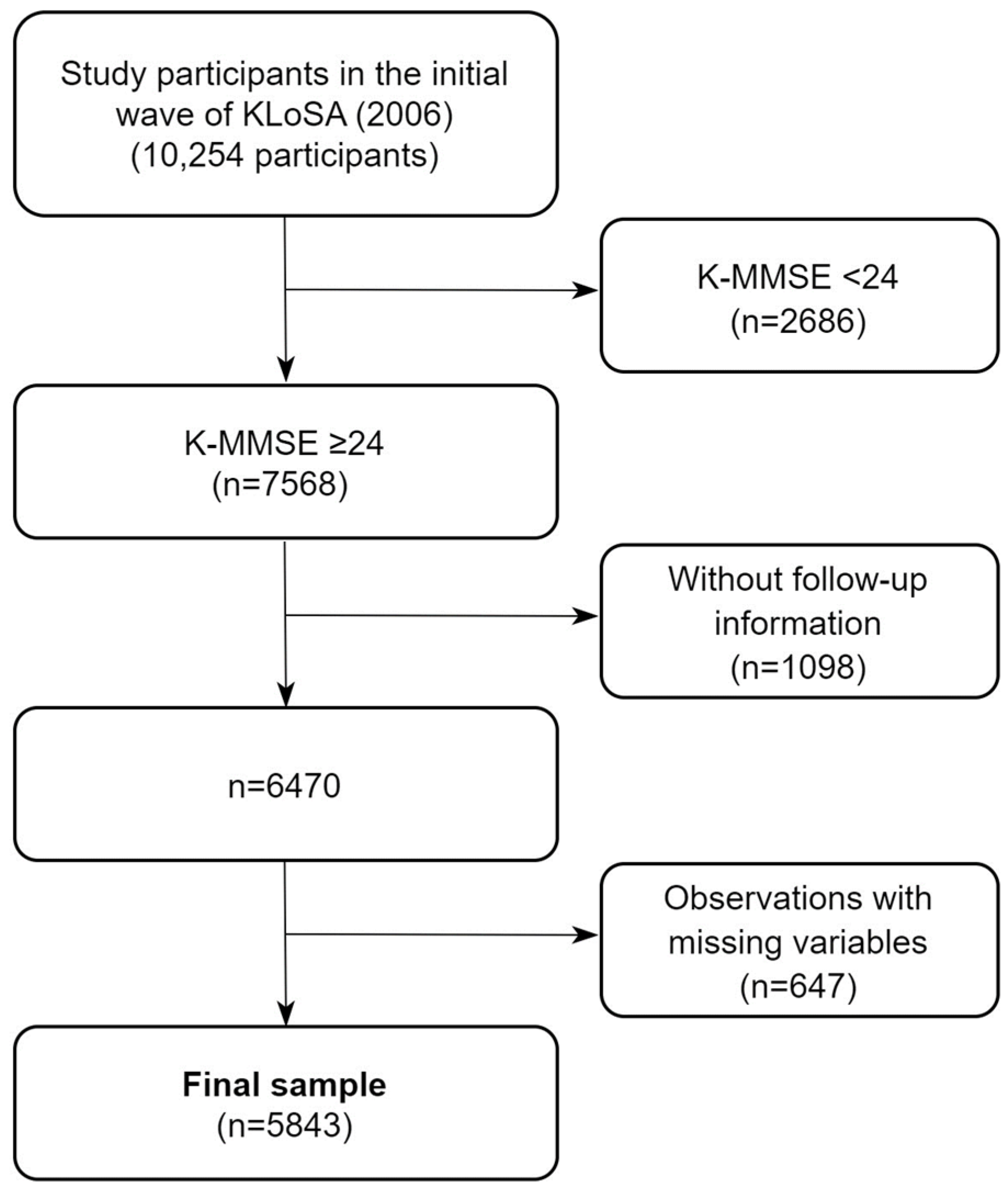
2.1. Study Sample
2.2. Data Availablity and Ethics Statement
2.3. Variables
2.3.1. Exposure
2.3.2. Outcome
2.3.3. Moderator
2.3.4. Confounders
2.4. Statistical Analysis
2.5. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Shon, C.; Yoon, H. Health-economic burden of dementia in South Korea. BMC Geriatr. 2021, 21, 549. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.W.; Noh, J.H.; Kim, D.J. The prevalence of and factors associated with depressive symptoms in the Korean adults: The 2014 and 2016 Korea National Health and Nutrition Examination Survey. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.E.; Jo, M.W.; Shin, Y.W. Increased prevalence of depression in South Korea from 2002 to 2013. Sci. Rep. 2020, 10, 16979. [Google Scholar] [CrossRef] [PubMed]
- Shin, M. Depressive symptoms with cognitive dysfunction increase the risk of cognitive impairment: Analysis of the Korean Longitudinal Study of Aging (KLoSA), 2006–2018. Int. Psychogeriatr. 2021, 33, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Dugravot, A.; Fournier, A.; Abell, J.; Ebmeier, K.; Kivimaki, M.; Sabia, S. Trajectories of Depressive Symptoms Before Diagnosis of Dementia: A 28-Year Follow-Up Study. JAMA Psychiatry 2017, 74, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Dafsari, F.S.; Jessen, F. Depression-an underrecognized target for prevention of dementia in Alzheimer’s disease. Transl. Psychiatry 2020, 10, 160. [Google Scholar] [CrossRef] [PubMed]
- Byers, A.L.; Yaffe, K. Depression and risk of developing dementia. Nat. Rev. Neurol. 2011, 7, 323–331. [Google Scholar] [CrossRef]
- Butters, M.A.; Young, J.B.; Lopez, O.; Aizenstein, H.J.; Mulsant, B.H.; Reynolds, C.F., 3rd; DeKosky, S.T.; Becker, J.T. Pathways linking late-life depression to persistent cognitive impairment and dementia. Dialogues Clin. Neurosci. 2008, 10, 345–357. [Google Scholar] [CrossRef]
- Hakim, A. Perspectives on the complex links between depression and dementia. Front. Aging Neurosci. 2022, 14, 821866. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve and Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2006, 20, 112–117. [Google Scholar] [CrossRef]
- Wilson, R.S.; Yu, L.; Lamar, M.; Schneider, J.A.; Boyle, P.A.; Bennett, D.A. Education and cognitive reserve in old age. Neurology 2019, 92, e1041–e1050. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.P.; Smith, D.M.; Mukherjee, S.; Zhang, Y.; Hou, W.; Link, B.G.; Richards, M. Education and Cognitive Decline: An Integrative Analysis of Global Longitudinal Studies of Cognitive Aging. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, e151–e160. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Tan, L.; Wang, H.F.; Tan, M.S.; Tan, L.; Li, J.Q.; Zhao, Q.F.; Yu, J.T. Education and Risk of Dementia: Dose-Response Meta-Analysis of Prospective Cohort Studies. Mol. Neurobiol. 2016, 53, 3113–3123. [Google Scholar] [CrossRef] [PubMed]
- Iso-Markku, P.; Kaprio, J.; Lindgren, N.; Rinne, J.O.; Vuoksimaa, E. Education as a moderator of middle-age cardiovascular risk factor-old-age cognition relationships: Testing cognitive reserve hypothesis in epidemiological study. Age Ageing 2022, 51, afab228. [Google Scholar] [CrossRef]
- Vonk, J.M.J.; Arce Renteria, M.; Medina, V.M.; Pericak-Vance, M.A.; Byrd, G.S.; Haines, J.; Brickman, A.M.; Manly, J.J. Education Moderates the Relation Between APOE varepsilon4 and Memory in Nondemented Non-Hispanic Black Older Adults. J. Alzheimer’s Dis. 2019, 72, 495–506. [Google Scholar] [CrossRef]
- Lee, J.; Park, H.; Chey, J. Education as a Protective Factor Moderating the Effect of Depression on Memory Impairment in Elderly Women. Psychiatry Investig. 2018, 15, 70–77. [Google Scholar] [CrossRef]
- Kim, D. Effects of Depression on Changes in Cognitive Function in Older Adults: A Fixed-effects Model Analysis Using the Korean Longitudinal Study of Aging (KLoSA). Alzheimer Dis. Assoc. Disord. 2022, 36, 319–326. [Google Scholar] [CrossRef]
- Yu, Y.; Wang, S. Evolution from pseudodementia to dementia: Is depressive symptom an optional extra? Int. Psychogeriatr. 2021, 33, 751–754. [Google Scholar] [CrossRef]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Shin, S. Validity Study of Short Forms of the Korean Version Center for Epidemiologic Studies Depression Scale (CES-D). Master’s Thesis, Seoul National University, Seoul, Republic of Korea, 2011. [Google Scholar]
- Lee, K.-S.; Cheong, H.-K.; Oh, B.-H.; Hong, C.-H. Comparison of the validity of screening tests for dementia and mild cognitive impairment of the elderly in a community: K-MMSE, MMSE-K, MMSE-KC, and K-HDS. J. Korean Neuropsychiatr. Assoc. 2009, 48, 61–69. [Google Scholar]
- Kang, Y.; NA, D.-L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neuropsychiatr. Assoc. 1997, 15, 300–308. [Google Scholar]
- Shin, J.; Cho, E. Patterns and risk factors of cognitive decline among community-dwelling older adults in South Korea. Arch. Gerontol. Geriatr. 2023, 104, 104809. [Google Scholar] [CrossRef]
- Kim, S. Rapid expansion of higher education in South Korea: Political economy of education fever. In The Worldwide Transformation of Higher Education; Baker, D.P., Wiseman, A.W., Eds.; International Perspectives on Education and Society; Emerald Group Publishing Limited: Bingley, UK, 2008; Volume 9, pp. 223–268. [Google Scholar]
- Hubbard, A.E.; Ahern, J.; Fleischer, N.L.; Van der Laan, M.; Lippman, S.A.; Jewell, N.; Bruckner, T.; Satariano, W.A. To GEE or not to GEE: Comparing population average and mixed models for estimating the associations between neighborhood risk factors and health. Epidemiology 2010, 21, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.T.C.; Fung, A.W.T.; Richards, M.; Chan, W.C.; Chiu, H.F.K.; Lee, R.S.Y.; Lam, L.C.W. Risk of incident dementia varies with different onset and courses of depression. J. Affect. Disord. 2021, 282, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Skogen, J.C.; Bergh, S.; Stewart, R.; Knudsen, A.K.; Bjerkeset, O. Midlife mental distress and risk for dementia up to 27 years later: The Nord-Trondelag Health Study (HUNT) in linkage with a dementia registry in Norway. BMC Geriatr. 2015, 15, 23. [Google Scholar] [CrossRef]
- Bennett, S.; Thomas, A.J. Depression and dementia: Cause, consequence or coincidence? Maturitas 2014, 79, 184–190. [Google Scholar] [CrossRef]
- Kong, J.; Kang, M.; Kang, H. The Relationship between Late-Life Depression and Cognitive Function in Older Korean Adults: A Moderation Analysis of Physical Activity Combined with Lower-Body Muscle Strength. Int. J. Environ. Res. Public Health 2022, 19, 8769. [Google Scholar] [CrossRef]
- Kim, H.; Jeong, W.; Kwon, J.; Kim, Y.; Park, E.C.; Jang, S.I. Association between depression and the risk of Alzheimer’s disease using the Korean National Health Insurance Service-Elderly Cohort. Sci. Rep. 2021, 11, 22591. [Google Scholar] [CrossRef]
- Seth, M.J. Education Fever: Society, Politics, and the Pursuit of Schooling in South Korea; University of Hawaii Press: Honolulu, HI, USA, 2002. [Google Scholar]
- Rodriguez, F.S.; Zheng, L.; Chui, H.C.; Aging Brain: Vasculature, I.; Behavior, S. Psychometric Characteristics of Cognitive Reserve: How High Education Might Improve Certain Cognitive Abilities in Aging. Dement. Geriatr. Cogn. Disord. 2019, 47, 335–344. [Google Scholar] [CrossRef]
- Chen, Y.; Lv, C.; Li, X.; Zhang, J.; Chen, K.; Liu, Z.; Li, H.; Fan, J.; Qin, T.; Luo, L.; et al. The positive impacts of early-life education on cognition, leisure activity, and brain structure in healthy aging. Aging 2019, 11, 4923–4942. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; D’Arcy, C. Education and dementia in the context of the cognitive reserve hypothesis: A systematic review with meta-analyses and qualitative analyses. PLoS ONE 2012, 7, e38268. [Google Scholar] [CrossRef]
- Lam, R.W.; Kennedy, S.H.; McLntyre, R.S.; Khullar, A. Cognitive dysfunction in major depressive disorder: Effects on psychosocial functioning and implications for treatment. Can. J. Psychiatry 2014, 59, 649–654. [Google Scholar] [CrossRef]
- Hung, Y.C.; Lao, W.L.; Yeh, C.J.; Lee, M.C. The mediating effect of leisure activities in the relationship between depression and cognitive decline in middle age and older adults in Taiwan. BMC Geriatr. 2023, 23, 315. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Tang, F.; Chen, Y.; Silverstein, M.; Liu, S.; Dong, X. Education, Activity Engagement, and Cognitive Function in US Chinese Older Adults. J. Am. Geriatr. Soc. 2019, 67, S525–S531. [Google Scholar] [CrossRef] [PubMed]
- Potvin, O.; Forget, H.; Preville, M.; Berbiche, D.; Chagnon, Y.C.; Hudon, C. Relationship between cortisol level and prevalent/incident cognitive impairment and its moderating factors in older adults. Int. Psychogeriatr. 2013, 25, 252–262. [Google Scholar] [CrossRef]
- Azur, M.J.; Stuart, E.A.; Frangakis, C.; Leaf, P.J. Multiple imputation by chained equations: What is it and how does it work? Int. J. Methods Psychiatr. Res. 2011, 20, 40–49. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Overall | Depressive Symptoms | p Value * | ||
|---|---|---|---|---|
| Yes | No | |||
| n = 5843 | n = 857 | n = 4986 | ||
| Sex | <0.001 | |||
| Male | 2866 (49.1%) | 343 (40.0%) | 2523 (50.6%) | |
| Female | 2977 (50.9%) | 514 (60.0%) | 2463 (49.4%) | |
| Age | <0.001 | |||
| Mean (standard deviation) | 58.4 (9.4) | 61.1 (9.9) | 58.0 (9.2) | |
| Educational level | <0.001 | |||
| Elementary school or below | 2059 (35.2%) | 478 (55.8%) | 1581 (31.7%) | |
| Middle school | 1122 (19.2%) | 152 (17.7%) | 970 (19.5%) | |
| High school | 1957 (33.5%) | 185 (21.6%) | 1772 (35.5%) | |
| College or above | 705 (12.1%) | 42 (4.9%) | 663 (13.3%) | |
| Residential area | 0.036 | |||
| Metropolis | 2625 (44.9%) | 371 (43.3%) | 2254 (45.2%) | |
| Urban region | 1889 (32.3%) | 262 (30.6%) | 1627 (32.6%) | |
| Rural region | 1329 (22.7%) | 224 (26.1%) | 1105 (22.2%) | |
| Income level | <0.001 | |||
| Q1 | 886 (15.2%) | 188 (21.9%) | 698 (14.0%) | |
| Q2 | 1045 (17.9%) | 232 (27.1%) | 813 (16.3%) | |
| Q3 | 1617 (27.7%) | 239 (27.9%) | 1378 (27.6%) | |
| Q4 | 1029 (17.6%) | 107 (12.5%) | 922 (18.5%) | |
| Q5 | 1266 (21.7%) | 91 (10.6%) | 1175 (23.6%) | |
| Marital status | <0.001 | |||
| Married | 5024 (86.0%) | 597 (69.7%) | 4427 (88.8%) | |
| Unmarried | 769 (13.2%) | 247 (28.8%) | 522 (10.5%) | |
| Others | 50 (0.9%) | 13 (1.5%) | 37 (0.7%) | |
| Employment status | <0.001 | |||
| Employed | 2845 (48.7%) | 294 (34.3%) | 2551 (51.2%) | |
| Unemployed | 2998 (51.3%) | 563 (65.7%) | 2435 (48.8%) | |
| Hypertension | <0.001 | |||
| Yes | 1407 (24.1%) | 266 (31.0%) | 1141 (22.9%) | |
| No | 4436 (75.9%) | 591 (69.0%) | 3845 (77.1%) | |
| Diabetes mellitus | <0.001 | |||
| Yes | 609 (10.4%) | 135 (15.8%) | 474 (9.5%) | |
| No | 5234 (89.6%) | 722 (84.2%) | 4512 (90.5%) | |
| Cancer | <0.001 | |||
| Yes | 130 (2.2%) | 42 (4.9%) | 88 (1.8%) | |
| No | 5713 (97.8%) | 815 (95.1%) | 4898 (98.2%) | |
| Pulmonary disease | <0.001 | |||
| Yes | 95 (1.6%) | 28 (3.3%) | 67 (1.3%) | |
| No | 5748 (98.4%) | 829 (96.7%) | 4919 (98.7%) | |
| Liver disease | ||||
| Yes | 95 (1.6%) | 20 (2.3%) | 75 (1.5%) | 0.135 |
| No | 5748 (98.4%) | 837 (97.7%) | 4911 (98.5%) | |
| Cardiovascular disease | <0.001 | |||
| Yes | 233 (4.0%) | 62 (7.2%) | 171 (3.4%) | |
| No | 5610 (96.0%) | 795 (92.8%) | 4815 (96.6%) | |
| Baseline K-MMSE | <0.001 | |||
| Mean (standard deviation) | 27.9 (1.9) | 27.2 (2.0) | 28.0 (1.8) | |
| Cognitive Impairment Onset | p Value * | ||
|---|---|---|---|
| Yes | No | ||
| n = 3188 | n = 24,720 | ||
| Depressive symptoms | <0.001 | ||
| Not depressed | 2,178 (9.4%) | 20,925 (90.6%) | |
| Depressed | 1010 (21.0%) | 3795 (79.0%) | |
| Sex | <0.001 | ||
| Male | 1336 (9.8%) | 12,338 (90.2%) | |
| Female | 1852 (13.0%) | 12,382 (87.0%) | |
| Age | <0.001 | ||
| 45–54 | 272 (4.4%) | 5888 (95.6%) | |
| 55–64 | 816 (7.4%) | 10,152 (92.6%) | |
| 65–74 | 1313 (16.7%) | 6546 (83.3%) | |
| ≥75 | 787 (26.9%) | 2134 (73.1%) | |
| Educational level | <0.001 | ||
| Elementary school or below | 1800 (20.8%) | 6844 (79.2%) | |
| Middle school | 580 (10.3%) | 5051 (89.7%) | |
| High school | 645 (6.4%) | 9384 (93.6%) | |
| College or above | 163 (4.5%) | 3441 (95.5%) | |
| Residential area | <0.001 | ||
| Metropolis | 1229 (9.9%) | 11,157 (90.1%) | |
| Urban region | 986 (10.8%) | 8146 (89.2%) | |
| Rural region | 973 (15.2%) | 5417 (84.8%) | |
| Income level | <0.001 | ||
| Q1 | 847 (23.0%) | 2834 (77.0%) | |
| Q2 | 824 (15.3%) | 4568 (84.7%) | |
| Q3 | 675 (9.9%) | 6115 (90.1%) | |
| Q4 | 498 (7.9%) | 5802 (92.1%) | |
| Q5 | 344 (6.0%) | 5401 (94.0%) | |
| Marital status | <0.001 | ||
| Married | 2442 (10.2%) | 21,522 (89.8%) | |
| Unmarried | 714 (19.1%) | 3026 (80.9%) | |
| Others | 32 (15.7%) | 172 (84.3%) | |
| Employment status | <0.001 | ||
| Employed | 1084 (7.8%) | 12,891 (92.2%) | |
| Unemployed | 2104 (15.1%) | 11,829 (84.9%) | |
| Hypertension | <0.001 | ||
| Yes | 1377 (15.3%) | 7601 (84.7%) | |
| No | 1811 (9.6%) | 17,119 (90.4%) | |
| Diabetes mellitus | <0.001 | ||
| Yes | 599 (15.6%) | 3240 (84.4%) | |
| No | 2589 (10.8%) | 21,480 (89.2%) | |
| Cancer | <0.001 | ||
| Yes | 175 (14.7%) | 1014 (85.3%) | |
| No | 3013 (11.3%) | 23,706 (88.7%) | |
| Pulmonary disease | <0.001 | ||
| Yes | 110 (19.9%) | 443 (80.1%) | |
| No | 3078 (11.3%) | 24,277 (88.7%) | |
| Liver disease | <0.001 | ||
| Yes | 85 (12.8%) | 581 (87.2%) | |
| No | 3103 (11.4%) | 24,139 (88.6%) | |
| Cardiovascular disease | <0.001 | ||
| Yes | 292 (17.1%) | 1420 (82.9%) | |
| No | 2896 (11.1%) | 23,300 (88.9%) | |
| Baseline K-MMSE | <0.001 | ||
| 24–26 | 1614 (25.1%) | 4820 (74.9%) | |
| 27–28 | 845 (10.8%) | 6964 (89.2%) | |
| 29–30 | 729 (5.3%) | 12,936 (94.7%) | |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Depressive symptoms | ||||||
| Not depressed | Reference | Reference | Reference | |||
| Depressed | 2.17 (2.00–2.36) | <0.001 | 1.61 (1.47–1.76) | <0.001 | 1.43 (1.27–1.62) | <0.001 |
| Sex | ||||||
| Male | Reference | Reference | ||||
| Female | 1.22 (1.10–1.34) | <0.001 | 1.21 (1.10–1.34) | <0.001 | ||
| Age | ||||||
| Continuous variable | 1.06 (1.05–1.06) | <0.001 | 1.05 (1.05–1.06) | <0.001 | ||
| Educational level | ||||||
| Elementary school or below | Reference | Reference | ||||
| Middle school | 0.73 (0.64–0.82) | <0.001 | 0.69 (0.60–0.79) | <0.001 | ||
| High school | 0.56 (0.50–0.63) | <0.001 | 0.52 (0.45–0.59) | <0.001 | ||
| College or above | 0.40 (0.33–0.48) | <0.001 | 0.34 (0.27–0.43) | <0.001 | ||
| Residential area | ||||||
| Metropolis | Reference | Reference | ||||
| Urban region | 1.14 (1.03–1.27) | 0.012 | 1.13 (1.02–1.26) | 0.017 | ||
| Rural region | 1.28 (1.14–1.42) | <0.001 | 1.27 (1.14–1.42) | <0.001 | ||
| Income level | ||||||
| Q1 | Reference | Reference | ||||
| Q2 | 0.87 (0.77–0.97) | 0.015 | 0.87 (0.77–0.97) | 0.014 | ||
| Q3 | 0.78 (0.68–0.88) | <0.001 | 0.77 (0.68–0.88) | <0.001 | ||
| Q4 | 0.82 (0.71–0.94) | 0.006 | 0.82 (0.71–0.94) | 0.004 | ||
| Q5 | 0.86 (0.73–1.01) | 0.067 | 0.86 (0.73–1.01) | 0.071 | ||
| Marital status | ||||||
| Married | Reference | Reference | ||||
| Unmarried | 1.04 (0.92–1.17) | 0.552 | 1.04 (0.92–1.17) | 0.529 | ||
| Others | 1.86 (1.14–3.03) | 0.013 | 1.83 (1.13–2.94) | 0.013 | ||
| Employment status | ||||||
| Employed | Reference | Reference | ||||
| Unemployed | 1.20 (1.09–1.32) | <0.001 | 1.20 (1.09–1.32) | <0.001 | ||
| Hypertension | ||||||
| Yes | 1.06 (0.97–1.16) | 0.222 | 1.06 (0.96–1.16) | 0.244 | ||
| No | Reference | Reference | ||||
| Diabetes mellitus | ||||||
| Yes | 1.09 (0.97–1.23) | 0.156 | 1.09 (0.97–1.23) | 0.150 | ||
| No | Reference | Reference | ||||
| Cancer | ||||||
| Yes | 1.08 (0.90–1.31) | 0.406 | 1.08 (0.89–1.30) | 0.445 | ||
| No | Reference | Reference | ||||
| Pulmonary disease | ||||||
| Yes | 1.32 (1.05–1.66) | 0.017 | 1.32 (1.05–1.66) | 0.017 | ||
| No | Reference | Reference | ||||
| Liver disease | ||||||
| Yes | 1.01 (0.78–1.30) | 0.962 | 1.01 (0.78–1.30) | 0.929 | ||
| No | Reference | Reference | ||||
| Cardiovascular disease | ||||||
| Yes | 1.07 (0.92–1.26) | 0.381 | 1.08 (0.92–1.26) | 0.367 | ||
| No | Reference | Reference | ||||
| Baseline K-MMSE | ||||||
| Continuous variable | 0.76 (0.75–0.78) | <0.001 | 0.76 (0.75–0.78) | <0.001 | ||
| Depressive symptoms × Educational levels | ||||||
| Depressed × Middle school | 1.18 (0.94–1.48) | 0.160 | ||||
| Depressed × High school | 1.31 (1.05–1.64) | 0.018 | ||||
| Depressed × College or above | 1.73 (1.19–2.52) | 0.004 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, S.-U.; Yoon, J.-H. Depressive Symptomatology as a Predictor of Cognitive Impairment: Evidence from the Korean Longitudinal Study of Aging (KLOSA), 2006–2020. Biomedicines 2023, 11, 2713. https://doi.org/10.3390/biomedicines11102713
Baek S-U, Yoon J-H. Depressive Symptomatology as a Predictor of Cognitive Impairment: Evidence from the Korean Longitudinal Study of Aging (KLOSA), 2006–2020. Biomedicines. 2023; 11(10):2713. https://doi.org/10.3390/biomedicines11102713
Chicago/Turabian StyleBaek, Seong-Uk, and Jin-Ha Yoon. 2023. "Depressive Symptomatology as a Predictor of Cognitive Impairment: Evidence from the Korean Longitudinal Study of Aging (KLOSA), 2006–2020" Biomedicines 11, no. 10: 2713. https://doi.org/10.3390/biomedicines11102713
APA StyleBaek, S.-U., & Yoon, J.-H. (2023). Depressive Symptomatology as a Predictor of Cognitive Impairment: Evidence from the Korean Longitudinal Study of Aging (KLOSA), 2006–2020. Biomedicines, 11(10), 2713. https://doi.org/10.3390/biomedicines11102713