
Prevalence of Fibromyalgia and Chronic Fatigue Syndrome among Individuals with Irritable Bowel Syndrome: An Analysis of United States National Inpatient Sample Database
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
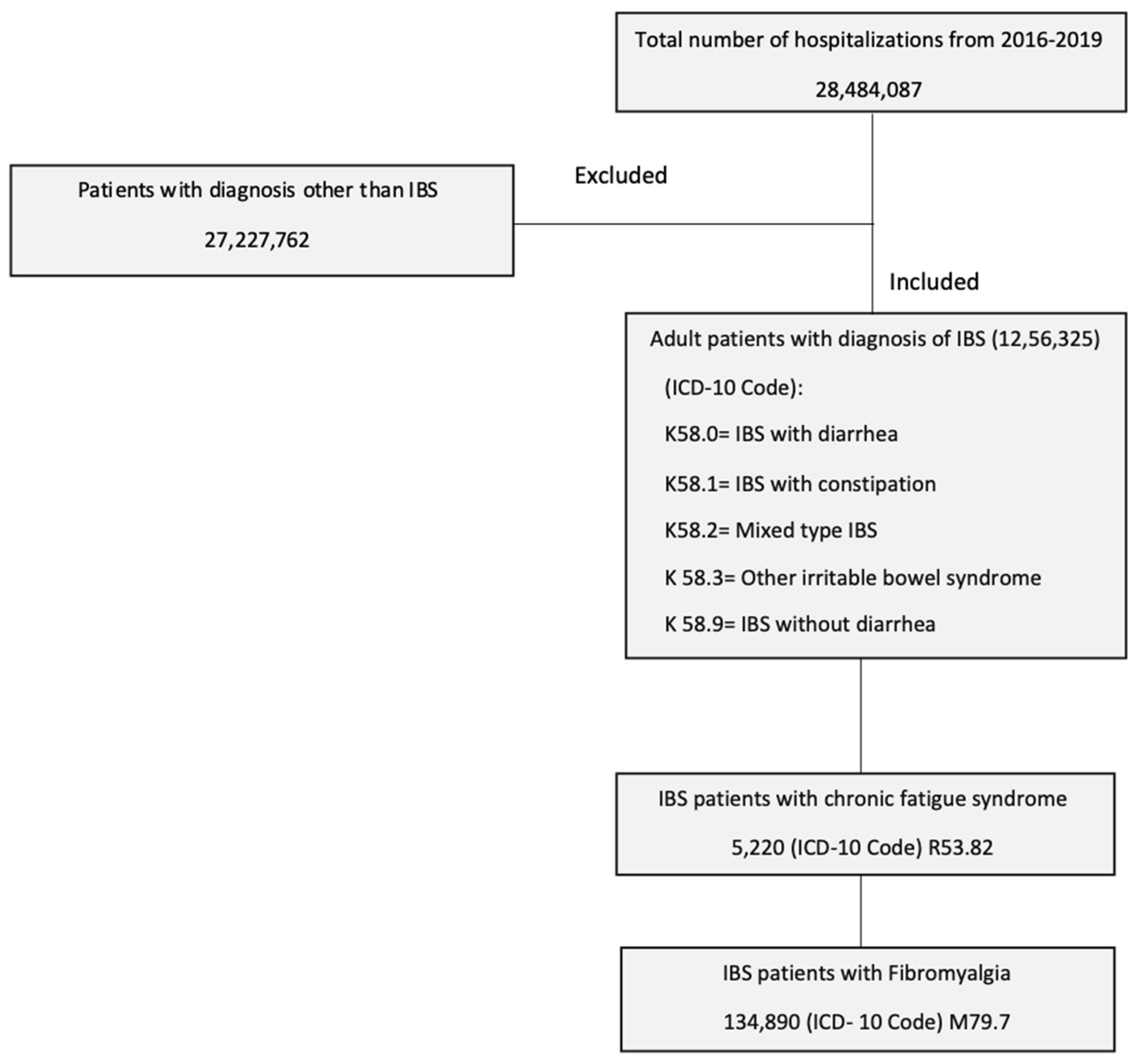
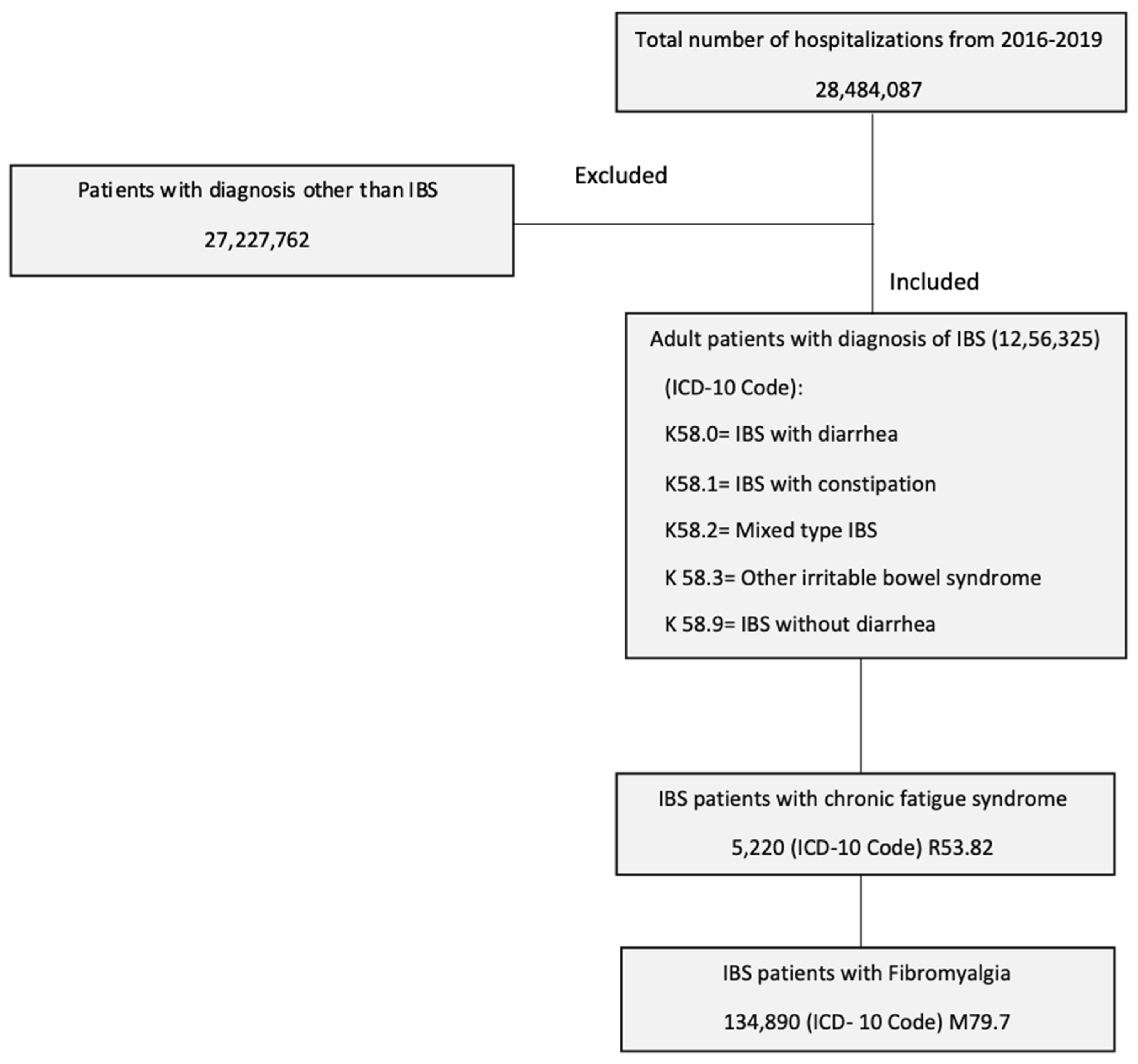
2.2. Study Population
2.3. Study Outcomes and Variables
2.4. Statistical Analysis
3. Results
3.1. Prevalence and Adjusted Odds of Fibromyalgia and Chronic Fatigue Syndrome in Patients with Irritable Bowel Syndrome
3.2. Resource Utilization
3.3. Predictors of Chronic Fatigue Syndrome and Fibromyalgia
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407.e5. [Google Scholar] [CrossRef]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e113. [Google Scholar] [CrossRef]
- Everhart, J.E.; Renault, P.F. Irritable bowel syndrome in office-based practice in the United States. Gastroenterology 1991, 100, 998–1005. [Google Scholar] [CrossRef]
- Lovell, R.M.; Ford, A.C. Effect of gender on prevalence of irritable bowel syndrome in the community: Systematic review and meta-analysis. Am. J. Gastroenterol. 2012, 107, 991–1000. [Google Scholar] [CrossRef]
- Lovell, R.M.; Ford, A.C. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin. Gastroenterol. Hepatol. 2012, 10, 712–721.e714. [Google Scholar] [CrossRef]
- Staller, K.; Olen, O.; Soderling, J.; Roelstraete, B.; Tornblom, H.; Khalili, H.; Joshi, A.D.; Nguyen, L.H.; Song, M.; Kuo, B.; et al. Mortality Risk in Irritable Bowel Syndrome: Results From a Nationwide Prospective Cohort Study. Am. J. Gastroenterol. 2020, 115, 746–755. [Google Scholar] [CrossRef]
- Chey, W.D.; Kurlander, J.; Eswaran, S. Irritable bowel syndrome: A clinical review. JAMA 2015, 313, 949–958. [Google Scholar] [CrossRef]
- Goldenberg, D.L. Fibromyalgia syndrome. An emerging but controversial condition. JAMA 1987, 257, 2782–2787. [Google Scholar] [CrossRef]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef]
- Sperber, A.D.; Atzmon, Y.; Neumann, L.; Weisberg, I.; Shalit, Y.; Abu-Shakrah, M.; Fich, A.; Buskila, D. Fibromyalgia in the irritable bowel syndrome: Studies of prevalence and clinical implications. Am. J. Gastroenterol. 1999, 94, 3541–3546. [Google Scholar] [CrossRef] [PubMed]
- Lubrano, E.; Iovino, P.; Tremolaterra, F.; Parsons, W.J.; Ciacci, C.; Mazzacca, G. Fibromyalgia in patients with irritable bowel syndrome. An association with the severity of the intestinal disorder. Int. J. Color. Dis. 2001, 16, 211–215. [Google Scholar] [CrossRef]
- Costantini, R.; Affaitati, G.; Wesselmann, U.; Czakanski, P.; Giamberardino, M.A. Visceral pain as a triggering factor for fibromyalgia symptoms in comorbid patients. Pain 2017, 158, 1925–1937. [Google Scholar] [CrossRef]
- Veale, D.; Kavanagh, G.; Fielding, J.F.; Fitzgerald, O. Primary fibromyalgia and the irritable bowel syndrome: Different expressions of a common pathogenetic process. Br. J. Rheumatol. 1991, 30, 220–222. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Mil. Med. 2015, 180, 721–723. [Google Scholar] [CrossRef]
- Hamilton, W.T.; Gallagher, A.M.; Thomas, J.M.; White, P.D. Risk markers for both chronic fatigue and irritable bowel syndromes: A prospective case-control study in primary care. Psychol. Med. 2009, 39, 1913–1921. [Google Scholar] [CrossRef]
- Donnachie, E.; Schneider, A.; Mehring, M.; Enck, P. Incidence of irritable bowel syndrome and chronic fatigue following GI infection: A population-level study using routinely collected claims data. Gut 2018, 67, 1078–1086. [Google Scholar] [CrossRef]
- Moss-Morris, R.; Spence, M. To “lump” or to “split” the functional somatic syndromes: Can infectious and emotional risk factors differentiate between the onset of chronic fatigue syndrome and irritable bowel syndrome? Psychosom. Med. 2006, 68, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Alammar, N.; Singh, R.; Nanavati, J.; Song, Y.; Chaudhary, R.; Mullin, G.E. Gut Microbial Dysbiosis in the Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Case-Control Studies. J. Acad. Nutr. Diet. 2020, 120, 565–586. [Google Scholar] [CrossRef]
- Freidin, M.B.; Stalteri, M.A.; Wells, P.M.; Lachance, G.; Baleanu, A.F.; Bowyer, R.C.E.; Kurilshikov, A.; Zhernakova, A.; Steves, C.J.; Williams, F.M.K. An association between chronic widespread pain and the gut microbiome. Rheumatology 2021, 60, 3727–3737. [Google Scholar] [CrossRef] [PubMed]
- König, R.S.; Albrich, W.C.; Kahlert, C.R.; Bahr, L.S.; Löber, U.; Vernazza, P.; Scheibenbogen, C.; Forslund, S.K. The Gut Microbiome in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Front. Immunol. 2021, 12, 628741. [Google Scholar] [CrossRef] [PubMed]
- Healthcare Cost and Utilization Project (HCUP). HCUP Facts and Figures: Statistics on Hospital-Based Care in the United States, 2009; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2019.
- Blatchford, O.; Murray, W.R.; Blatchford, M. A risk score to predict need for treatment for uppergastrointestinal haemorrhage. Lancet 2000, 356, 1318–1321. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.W.; Schroder, A.; Jorgensen, T.; Ornbol, E.; Dantoft, T.M.; Eliasen, M.; Carstensen, T.W.; Falgaard Eplov, L.; Fink, P. Prevalence of functional somatic syndromes and bodily distress syndrome in the Danish population: The DanFunD study. Scand. J. Public Health 2020, 48, 567–576. [Google Scholar] [CrossRef]
- Janssens, K.A.; Zijlema, W.L.; Joustra, M.L.; Rosmalen, J.G. Mood and Anxiety Disorders in Chronic Fatigue Syndrome, Fibromyalgia, and Irritable Bowel Syndrome: Results From the LifeLines Cohort Study. Psychosom. Med. 2015, 77, 449–457. [Google Scholar] [CrossRef]
- Whitehead, W.E.; Palsson, O.; Jones, K.R. Systematic review of the comorbidity of irritable bowel syndrome with other disorders: What are the causes and implications? Gastroenterology 2002, 122, 1140–1156. [Google Scholar] [CrossRef] [PubMed]
- Barton, A.; Pal, B.; Whorwell, P.J.; Marshall, D. Increased prevalence of sicca complex and fibromyalgia in patients with irritable bowel syndrome. Am. J. Gastroenterol. 1999, 94, 1898–1901. [Google Scholar] [CrossRef]
- Iovino, P.; Tremolaterra, F.; Consalvo, D.; Sabbatini, F.; Mazzacca, G.; Ciacci, C. Perception of electrocutaneous stimuli in irritable bowel syndrome. Am. J. Gastroenterol. 2006, 101, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Straus, S.E. The chronic mononucleosis syndrome. J. Infect. Dis. 1988, 157, 405–412. [Google Scholar] [CrossRef]
- Jones, J.F.; Ray, C.G.; Minnich, L.L.; Hicks, M.J.; Kibler, R.; Lucas, D.O. Evidence for active Epstein-Barr virus infection in patients with persistent, unexplained illnesses: Elevated anti-early antigen antibodies. Ann. Intern. Med. 1985, 102, 1–7. [Google Scholar] [CrossRef]
- Straus, S.E.; Tosato, G.; Armstrong, G.; Lawley, T.; Preble, O.T.; Henle, W.; Davey, R.; Pearson, G.; Epstein, J.; Brus, I.; et al. Persisting illness and fatigue in adults with evidence of Epstein-Barr virus infection. Ann. Intern. Med. 1985, 102, 7–16. [Google Scholar] [CrossRef]
- Creed, F. Review article: The incidence and risk factors for irritable bowel syndrome in population-based studies. Aliment. Pharmacol. Ther. 2019, 50, 507–516. [Google Scholar] [CrossRef]
- Creed, F. A review of the incidence and risk factors for fibromyalgia and chronic widespread pain in population-based studies. Pain 2020, 161, 1169–1176. [Google Scholar] [CrossRef]
- Ley, R.E.; Backhed, F.; Turnbaugh, P.; Lozupone, C.A.; Knight, R.D.; Gordon, J.I. Obesity alters gut microbial ecology. Proc. Natl. Acad. Sci. USA 2005, 102, 11070–11075. [Google Scholar] [CrossRef]
- Jeffery, I.B.; Quigley, E.M.; Ohman, L.; Simren, M.; O’Toole, P.W. The microbiota link to irritable bowel syndrome: An emerging story. Gut Microbes 2012, 3, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, F.; Karaca, Z.; Unluhizarci, K.; Kelestimur, F. The hypothalamo-pituitary-adrenal axis in chronic fatigue syndrome and fibromyalgia syndrome. Stress 2007, 10, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martinez, L.A.; Mora, T.; Vargas, A.; Fuentes-Iniestra, M.; Martinez-Lavin, M. Sympathetic nervous system dysfunction in fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, and interstitial cystitis: A review of case-control studies. J. Clin. Rheumatol. 2014, 20, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Bose, M.; Olivan, B.; Laferrere, B. Stress and obesity: The role of the hypothalamic-pituitary-adrenal axis in metabolic disease. Curr. Opin. Endocrinol. Diabetes Obes. 2009, 16, 340–346. [Google Scholar] [CrossRef]
- Snitker, S.; Macdonald, I.; Ravussin, E.; Astrup, A. The sympathetic nervous system and obesity: Role in aetiology and treatment. Obes. Rev. 2000, 1, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Pamuk, O.N.; Donmez, S.; Cakir, N. The frequency of smoking in fibromyalgia patients and its association with symptoms. Rheumatol. Int. 2009, 29, 1311–1314. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.B.; Arslan, S.; Aldag, J.C. Relationship between fibromyalgia features and smoking. Scand. J. Rheumatol. 2002, 31, 301–305. [Google Scholar] [CrossRef]
- Woolley, J.; Allen, R.; Wessely, S. Alcohol use in chronic fatigue syndrome. J. Psychosom. Res. 2004, 56, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Collin, S.M.; Bakken, I.J.; Nazareth, I.; Crawley, E.; White, P.D. Trends in the incidence of chronic fatigue syndrome and fibromyalgia in the UK, 2001-2013: A Clinical Practice Research Datalink study. J. R. Soc. Med. 2017, 110, 231–244. [Google Scholar] [CrossRef]
- Bhui, K.S.; Dinos, S.; Ashby, D.; Nazroo, J.; Wessely, S.; White, P.D. Chronic fatigue syndrome in an ethnically diverse population: The influence of psychosocial adversity and physical inactivity. BMC Med. 2011, 9, 26. [Google Scholar] [CrossRef]
- Keel, P. Pain management strategies and team approach. Baillieres Best Pract. Res. Clin. Rheumatol. 1999, 13, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.; Adams, N. Physical and other non-pharmacological interventions for fibromyalgia. Baillieres Best Pract. Res. Clin. Rheumatol. 1999, 13, 507–523. [Google Scholar] [CrossRef]
- Bennett, R.M.; Clark, S.R.; Goldberg, L.; Nelson, D.; Bonafede, R.P.; Porter, J.; Specht, D. Aerobic fitness in patients with fibrositis. A controlled study of respiratory gas exchange and 133xenon clearance from exercising muscle. Arthritis Rheum. 1989, 32, 454–460. [Google Scholar] [CrossRef]
- Gurer, G.; Sendur, O.F.; Ay, C. Serum lipid profile in fibromyalgia women. Clin. Rheumatol. 2006, 25, 300–303. [Google Scholar] [CrossRef]
- Erdrich, S.; Hawrelak, J.A.; Myers, S.P.; Harnett, J.E. A systematic review of the association between fibromyalgia and functional gastrointestinal disorders. Ther. Adv. Gastroenterol. 2020, 13, 1756284820977402. [Google Scholar] [CrossRef] [PubMed]
- Triadafilopoulos, G.; Simms, R.W.; Goldenberg, D.L. Bowel dysfunction in fibromyalgia syndrome. Dig. Dis. Sci. 1991, 36, 59–64. [Google Scholar] [CrossRef]
- Sharon, G.; Sampson, T.R.; Geschwind, D.H.; Mazmanian, S.K. The Central Nervous System and the Gut Microbiome. Cell 2016, 167, 915–932. [Google Scholar] [CrossRef]
- Tomasello, G.; Mazzola, M.; Bosco, V.; Tomasello, G.; Damiani, P.; Sinagra, E.; Carini, F. Intestinal dysbiosis and hormonal neuroendocrine secretion in the fibromyalgic patient: Relationship and correlations. Biomed. Pap. Med. Fac. Palacky Univ. Olomouc Czech Repub. 2018, 162, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, L.P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.A.; Rothman, K.J.; Cabral, H.J.; Zhang, Y.; Farraye, F.A. Migraine, fibromyalgia, and depression among people with IBS: A prevalence study. BMC Gastroenterol. 2006, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- den Boer, C.; Dries, L.; Terluin, B.; van der Wouden, J.C.; Blankenstein, A.H.; van Wilgen, C.P.; Lucassen, P.; van der Horst, H.E. Central sensitization in chronic pain and medically unexplained symptom research: A systematic review of definitions, operationalizations and measurement instruments. J. Psychosom. Res. 2019, 117, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Basnayake, C.; Kamm, M.A.; Stanley, A.; Wilson-O’Brien, A.; Burrell, K.; Lees-Trinca, I.; Khera, A.; Kantidakis, J.; Wong, O.; Fox, K.; et al. Standard gastroenterologist versus multidisciplinary treatment for functional gastrointestinal disorders (MANTRA): An open-label, single-centre, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2020, 5, 890–899. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Baseline Characteristics | Total Number of IBS Patients 1,256,325 (1.04%) | p-Value Fibromyalgia | p-Value Chronic Fatigue Syndrome | |
|---|---|---|---|---|
| Fibromyalgia n = 134,890 (10.73%) | Chronic Fatigue syndrome n = 5220 (0.42%) | |||
| Mean Age [years] | 58.7 (58.5–59.0) | 59.9 (58.9–60.8) | <0.001 | 0.0003 |
| Women [n (%)] | 130,169 (96.5%) | (89.9%) | <0.001 | <0.001 |
| Race [n (%)] | <0.001 | <0.001 | ||
| White | 116,680 (86.5%) | 4735 (90.7%) | ||
| Black | 9200 (6.82%) | 198 (3.8%) | ||
| Hispanic | 6111 (4.53%) | 181 (3.46%) | ||
| Asians | 391 (0.29%) | IS | ||
| Native Americans | 540 (0.41%) | 26 (0.49%) | ||
| Others | 1915 (1.42%) | 72 (1.38%) | ||
| Charlson Co-Morbidity Index [n (%)] | <0.001 | <0.001 | ||
| 0 | 33,722 (25.0%) | 1639 (31.4%) | ||
| 1 | 39,118 (29.0%) | 1389 (26.6%) | ||
| 2 | 25,494 (18.9%) | 867 (16.6%) | ||
| 3 or more | 36,555 (27.1%) | 1326 (25.4%) | ||
| Median Household Income in Zip code (Quartile) * | <0.001 | <0.001 | ||
| 1st (0–25th) | 35,746 (26.5%) | 1237 (23.7%) | ||
| 2nd (26th–50th) | 38,983 (28.9%) | 1216 (23.3%) | ||
| 3rd (51st–75th) | 34,802 (25.8%) | 1389 (26.6%) | ||
| 4th (76th–100th) | 25,224 (18.7%) | 1378 (26.4%) | ||
| Hospital Region [n (%)] | <0.001 | <0.001 | ||
| Northeast | 21,852 (16.2%) | 809 (15.5%) | ||
| Midwest | 42,221 (31.3%) | 1336 (25.6%) | ||
| South | 48,965 (36.3%) | 1843 (35.3%) | ||
| West | 21,852 (16.2%) | 1232 (23.6%) | ||
| Insurance Status [n (%)] | <0.001 | <0.001 | ||
| Medicare | 77,292(57.3%) | 3001 (57.5%) | ||
| Medicaid | 17,940(13.3%) | 441 (8.45%) | ||
| Private/Self pay | 34,262 (25.4%) | 1561 (29.9%) | ||
| Uninsured | 2104 (1.56%) | 81 (1.54%) | ||
| Hospital bed size [n (%)] | 0.21 | 0.0001 | ||
| Small | 29,001 (21.5%) | 1138 (21.8%) | ||
| Medium | 37,095 (27.5%) | 1430 (27.4%) | ||
| Large | 69,199 (51.3%) | 2652 (50.8%) | ||
| Hospital teaching status [n (%)] | 0.007 | 0.009 | ||
| Rural | 12,410 (9.2%) | 449 (8.6%) | ||
| Urban non-teaching | 29,811 (22.1%) | 1211 (23.2%) | ||
| Urban teaching | 92,669 (68.7%) | 3560 (68.2%) | ||
| Co-Morbidities | ||||
| Smoking | 32,374 (24.0%) | 1206 (23.1%) | 0.001 | 0.20 |
| Alcohol abuse | 3507 (2.6%) | 178 (3.4%) | <0.001 | 0.81 |
| Obesity | 34,667 (25.7%) | 1101 (21.1%) | <0.001 | 0.60 |
| Hypertension | 61,240 (45.4%) | 2234 (42.6%) | <0.001 | 0.96 |
| Dyslipidemia | 48,830 (36.2%) | 1884 (36.1%) | 0.003 | 0.53 |
| Diabetes Mellitus | 33,857 (25.1%%) | 1039 (19.9%) | <0.001 | 0.009 |
| Congestive heart Failure | 13,084 (9.7%) | 454 (8.7%) | <0.001 | 0.01 |
| Coronary Artery Disease | 18,615 (13.8%) | 679 (13.0%) | <0.001 | 0.003 |
| Cerebro-Vascular Accident | 324 (0.24%) | 35 (0.67%) | 0.01 | 0.05 |
| Chronic kidney Disease | 15,243 (11.3%) | 465 (8.9%) | <0.001 | <0.001 |
| Malnutrition | 5800 (4.3%) | 266 (5.1%) | <0.001 | 0.50 |
| Malignancy | 4856 (3.6%) | 256 (4.9%) | <0.001 | 0.95 |
| Outcomes | Adjusted Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Fibromyalgia | 5.33 | 5.24–5.41 | <0.001 |
| Chronic fatigue syndrome | 5.40 | 5.04–5.78 | <0.001 |
| Outcomes | IBS-Diarrhea | IBS-Constipation | IBS-Mixed | |||
|---|---|---|---|---|---|---|
| AOR | p-Value | AOR | p-Value | AOR | p-Value | |
| Fibromyalgia | 4.38 (4.20–4.57) | <0.001 | 4.96 (4.66–5.28) | <0.001 | 4.96 (4.41–5.58) | <0.001 |
| Chronic fatigue syndrome | 4.41 (3.60–5.40) | <0.001 | 6.76 (5.28–8.65) | <0.001 | 5.32 (3.17–8.95) | <0.001 |
| Outcomes | Fibromyalgia | CFS | ||
|---|---|---|---|---|
| AOR (95%CI) | p-Value | AOR (95%CI) | p-Value | |
| Adjusted mean LOS | −0.13 (−0.72 to 0.44) | 0.64 | −0.26 (−0.51 to −0.02) | 0.06 |
| Adjusted mean total hospital charges | 156$ (−563 $ to −904$) | 0.68 | −5118$ (−8195$ to −2041$) | 0.001 |
| Predictors | CFS | Fibromyalgia | ||||
|---|---|---|---|---|---|---|
| AOR | 95% CI | p Value | AOR | 95% CI | p Value | |
| Age | 1.02 | 1.01–1.03 | <0.001 | 1.02 | 1.01–1.04 | <0.001 |
| Female sex | 1.86 | 1.78–1.93 | <0.001 | 11.2 | 11.1–11.4 | <0.001 |
| White race * | 1.69 | 1.34–2.13 | <0.001 | 2.04 | 1.95–2.12 | <0.001 |
| Black race | 0.75 | 0.59–0.97 | 0.003 | 0.47 | 0.46–0.49 | 0.02 |
| Hispanic | 0.60 | 0.47–0.76 | <0.001 | 1.03 | 0.98–1.08 | 0.17 |
| Asian | 0.61 | 0.45–0.82 | <0.001 | 0.31 | 0.29–0.34 | <0.001 |
| Low socioeconomic status * (1st–25th) quartile | 0.81 | 0.76–0.87 | <0.001 | 1.35 | 1.32–1.38 | <0.001 |
| 26th–50th quartile | 1.11 | 1.04–1.17 | <0.001 | 0.97 | 0.96–0.99 | <0.001 |
| 51st–75th quartile | 1.22 | 1.15–1.29 | <0.001 | 0.89 | 0.87–0.91 | <0.001 |
| 76th–100th quartile | 1.22 | 1.14–1.30 | <0.001 | 0.73 | 0.72–0.75 | <0.001 |
| Smoking | 1.14 | 1.09–1.19 | <0.001 | 1.24 | 1.22–1.25 | <0.001 |
| Obesity | 1.30 | 1.24–1.36 | <0.001 | 1.86 | 1.84–1.88 | <0.001 |
| Malnutrition | 1.09 | 0.99–1.01 | 0.08 | 0.86 | 0.84–0.88 | <0.001 |
| Alcohol use | 0.80 | 0.73–0.88 | <0.001 | 1.09 | 1.06–1.12 | <0.001 |
| Hyperlipidemia | 1.28 | 1.23–1.33 | <0.001 | 1.30 | 1.29–1.32 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarar, Z.I.; Farooq, U.; Nawaz, A.; Gandhi, M.; Ghouri, Y.A.; Bhatt, A.; Cash, B.D. Prevalence of Fibromyalgia and Chronic Fatigue Syndrome among Individuals with Irritable Bowel Syndrome: An Analysis of United States National Inpatient Sample Database. Biomedicines 2023, 11, 2594. https://doi.org/10.3390/biomedicines11102594
Tarar ZI, Farooq U, Nawaz A, Gandhi M, Ghouri YA, Bhatt A, Cash BD. Prevalence of Fibromyalgia and Chronic Fatigue Syndrome among Individuals with Irritable Bowel Syndrome: An Analysis of United States National Inpatient Sample Database. Biomedicines. 2023; 11(10):2594. https://doi.org/10.3390/biomedicines11102594
Chicago/Turabian StyleTarar, Zahid Ijaz, Umer Farooq, Ahmad Nawaz, Mustafa Gandhi, Yezaz A. Ghouri, Asmeen Bhatt, and Brooks D. Cash. 2023. "Prevalence of Fibromyalgia and Chronic Fatigue Syndrome among Individuals with Irritable Bowel Syndrome: An Analysis of United States National Inpatient Sample Database" Biomedicines 11, no. 10: 2594. https://doi.org/10.3390/biomedicines11102594
APA StyleTarar, Z. I., Farooq, U., Nawaz, A., Gandhi, M., Ghouri, Y. A., Bhatt, A., & Cash, B. D. (2023). Prevalence of Fibromyalgia and Chronic Fatigue Syndrome among Individuals with Irritable Bowel Syndrome: An Analysis of United States National Inpatient Sample Database. Biomedicines, 11(10), 2594. https://doi.org/10.3390/biomedicines11102594