
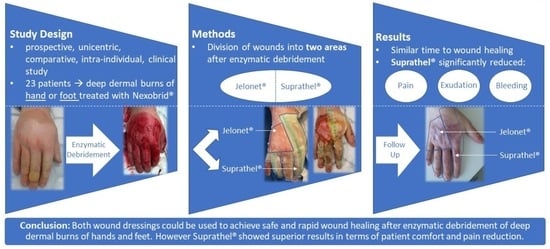
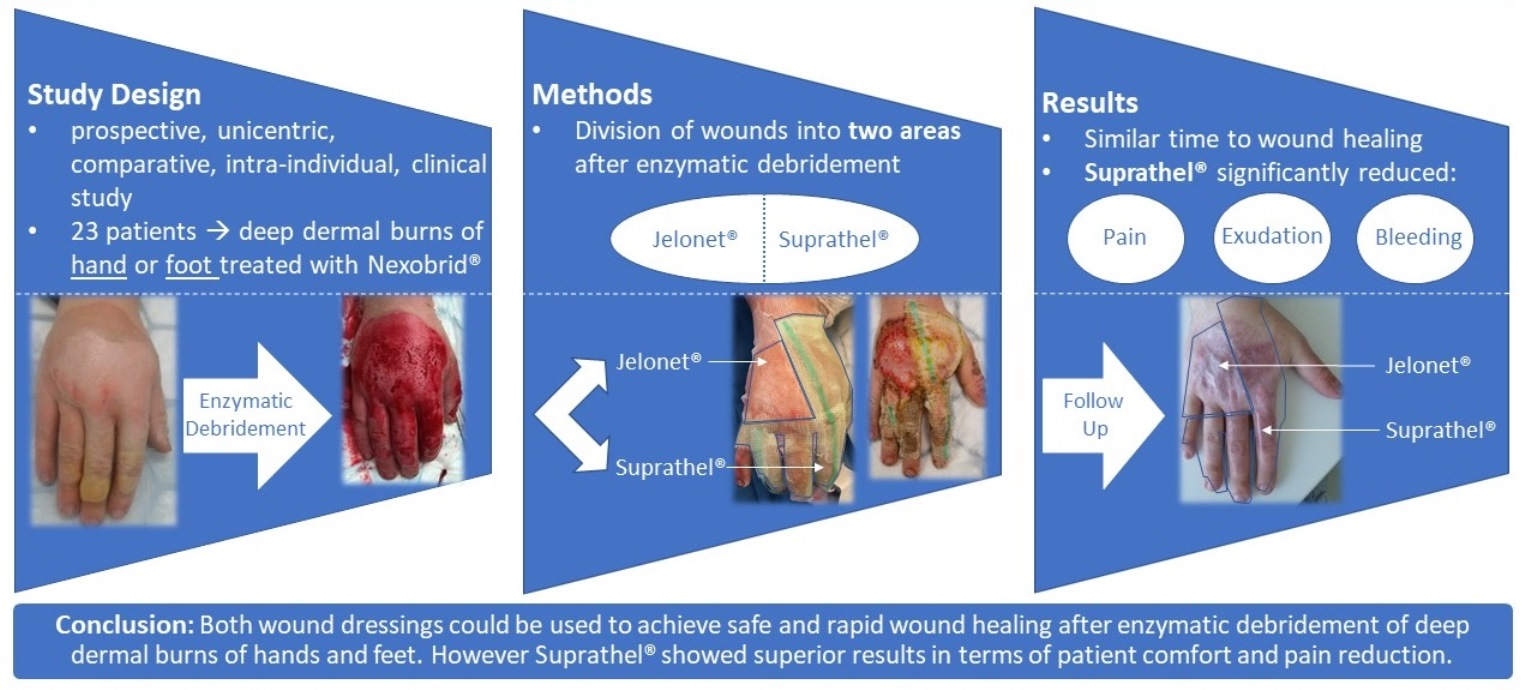
Comparative Clinical Study of Suprathel® and Jelonet® Wound Dressings in Burn Wound Healing after Enzymatic Debridement

 , ,
, ,  , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. Evaluation of Wound Parameters
2.4. Statistical Analysis
3. Results
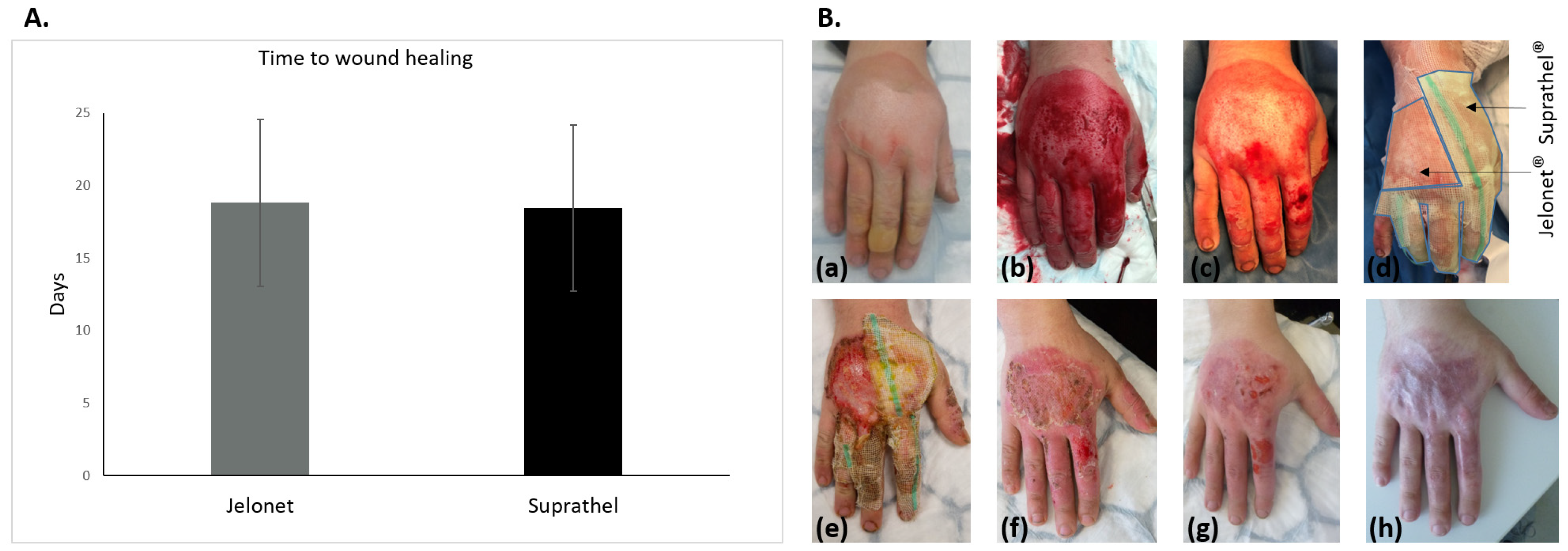
3.1. Wound Healing
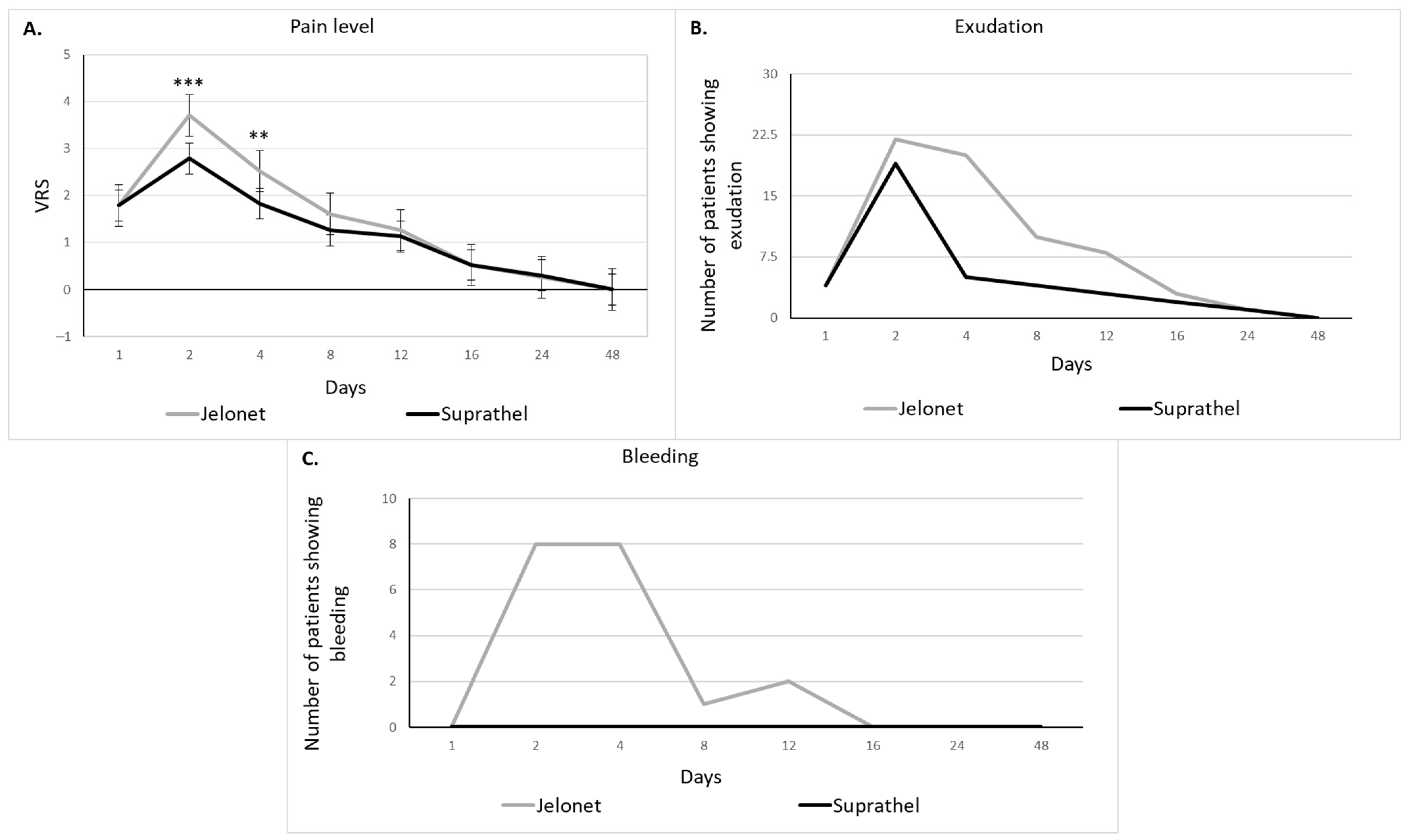
3.2. Pain, Bleeding, Exudation, and Time Needed for Dressing Changes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peck, M.D. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns 2011, 37, 1087–1100. [Google Scholar] [CrossRef]
- Mata-Ribeiro, L.; Vieira, L.; Vilela, M. Epidemiology and Outcome Assessment Of Hand Burns: A 3-Year Retrospective Analysis In A Burn Unit. Ann. Burn. Fire Disasters 2022, 35, 18–25. [Google Scholar]
- Spronk, I.; Van Loey, N.E.E.; van der Vlies, C.H.; Haagsma, J.A.; Polinder, S.; van Baar, M.E. Burden of Burn Injuries Study Group. Activity Impairment, Work Status, and Work Productivity Loss in Adults 5–7 Years After Burn Injuries. J. Burn. Care Res. 2022, 43, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Heitzmann, W.; Fuchs, P.C.; Schiefer, J.L. Historical Perspectives on the Development of Current Standards of Care for Enzymatic Debridement. Medicina 2020, 56, 706. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Perbix, W.; Shoham, Y. Our initial learning curve in the enzymatic debridement of severely burned hands—Management and pitfalls of initial treatments and our development of a post debridement wound treatment algorithm. Burns 2017, 43, 326–336. [Google Scholar] [CrossRef]
- Hirche, C.; Citterio, A.; Hoeksema, H.; Koller, J.; Lehner, M.; Martinez, J.R.; Monstrey, S.; Murray, A.; Plock, J.A.; Sander, F.; et al. Eschar removal by bromelain based enzymatic debridement (Nexobrid®) in burns: An European consensus. Burns 2017, 43, 1640–1653. [Google Scholar] [CrossRef]
- Moussa, A.; Lo, C.H.; Cleland, H. Burn wound excision within 24 h: A 9-year review. Burns 2021, 47, 1300–1307. [Google Scholar] [CrossRef]
- Gurfinkel, R.; Rosenberg, L.; Cohen, S.; Cohen, A.; Barezovsky, A.; Cagnano, E.; Singer, A.J. Histological assessment of tangentially excised burn eschars. J. Plast. Surg. Fall 2010, 18, 33–36. [Google Scholar]
- Krieger, Y.; Bogdanov-Berezovsky, A.; Gurfinkel, R.; Silberstein, E.; Sagi, A.; Rosenberg, L. Efficacy of enzymatic debridement of deeply burned hands. Burns 2012, 38, 108–112. [Google Scholar] [CrossRef]
- Cherubino, M.; Valdatta, L.; Baroni, T.; Pellegatta, I.; Tamborini, F.; Garutti, L.; Di Summa, P.; Adani, R. Selective Enzymatic Debridement for The Management Of Acute Upper Limb Burns. Ann. Burn. Fire Disasters 2021, 34, 328–333. [Google Scholar]
- Rosenberg, L.; Krieger, Y.; Bogdanov-Berezovski, A.; Silberstein, E. A novel rapid and selective enzymatic debridement agent for burn wound management: A multi-center RCT. Burns 2014, 40, 466–474. [Google Scholar] [CrossRef]
- Rosenberg, L.; Krieger, Y.; Silberstein, E. Selectivity of a bromelain based enzymatic debridement agent: A porcine study. Burns 2012, 38, 1035–1040. [Google Scholar] [CrossRef]
- Schulz, A.; Fuchs, P.C.; Rothermundt, I. Enzymatic debridement of deeply burned faces: Healing and early scarring based on tissue preservation compared to traditional surgical debridement. Burns 2017, 43, 1233–1243. [Google Scholar] [CrossRef]
- Korzeniowski, T.; Grywalska, E.; Strużyna, J.; Bugaj-Tobiasz, M.; Surowiecka, A.; Korona-Głowniak, I.; Staśkiewicz, M.; Torres, K. Preliminary Single-Center Experience of Bromelain-Based Eschar Removal in Children with Mixed Deep Dermal and Full Thickness Burns. J. Clin. Med. 2022, 11, 4800. [Google Scholar] [CrossRef] [PubMed]
- Finnerty, C.C.; Jeschke, M.G.; Branski, L.K.; Barret, J.P. Hypertrophic scarring: The greatest unmet challenge after burn injury. Lancet 2016, 388, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Hirche, C.; Almeland, S.K.; Dheansa, B.; Fuchs, P.; Governa, M.; Hoeksema, H.; Korzeniowski, T.; Lumenta, D.B.; Marinescu, S.; Martinez-Mendez, J.R.; et al. Eschar removal by bromelain based enzymatic debridement (Nexobrid®) in burns: European consensus guidelines update. Burns 2020, 46, 782–796. [Google Scholar] [CrossRef] [PubMed]
- Blome-Eberwein, S.A.; Amani, H.; Lozano, D.D.; Gogal, C.; Boorse, D.; Pagella, P. A bio-degradable synthetic membrane to treat superficial and deep second degree burn wounds in adults and children—4 year experience. Burns 2021, 47, 838–846. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Aretz, G.F.; Fuchs, P.C.; Bagheri, M.; Funk Schulz, A.; Daniels, M. Comparison of wound healing and patient comfort in partial-thickness burn wounds treated with SUPRATHEL and epictehydro wound dressings. Int. Wound J. 2022, 19, 782–790. [Google Scholar] [CrossRef]
- Rosenberg, L. Enzymatic debridement of burn wounds. Total Burn. Care 2012, 2, 131. [Google Scholar]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Andreae, J.; Fuchs, P.C.; Lefering, R.; Heidekrueger, P.I.; Schulz, A.; Bagheri, M. Evaluation of Scar Quality after Treatment of Superficial Burns with Dressilk® and Suprathel®–In an Intraindividual Clinical Setting. J. Clin. Med. 2022, 11, 2857. [Google Scholar] [CrossRef] [PubMed]
- Hundeshagen, G.; Collins, V.N.; Wurzer, P.; Sherman, W.; Voigt, C.D.; Cambiaso-Daniel, J.; Lopez, O.N.; Sheaffer, J.; Herndon, D.N.; Finnerty, C.C.; et al. A Prospective, Randomized, Controlled Trial Comparing the Outpatient Treatment of Pediatric and Adult Partial-Thickness Burns with Suprathel or Mepilex Ag. J. Burn. Care Res. 2018, 39, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Rashaan, Z.M.; Krijnen, P.; Allema, J.H.; Vloemans, A.F.; Schipper, I.B.; Breederveld, R.S. Usability and effectiveness of Suprathel® in partial thickness burns in children. Eur. J. Trauma Emerg. Surg. 2017, 43, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Keck, M.; Selig, H.F.; Lumenta, D.B.; Kamolz, L.P.; Mittlböck, M.; Frey, M. The use of Suprathel® in deep dermal burns: First results of a prospective study. Burns 2012, 38, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Dadras, M.; Wagner, J.M.; Wallner, C.; Sogorski, A.; Sacher, M.; Harati Lehnhardt, M.; Behr, B. Enzymatic debridement of hands with deep burns: A single center experience in the treatment of 52 hands. J. Plast. Surg. Hand Surg. 2020, 54, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Tolles, J. Emergency department management of patients with thermal burns. Emerg. Med. Pract. 2018, 20, 1–24. [Google Scholar]
- Evers, L.H.; Bhavsar, D.; Mailänder, P. The biology of burn injury. Exp. Dermatol. 2010, 19, 777–783. [Google Scholar] [CrossRef]
- Fischer, S.; Kremer, T.; Horter, J.; Schaefer, A.; Ziegler, B.; Kneser, U.; Hirche, C. Suprathel® for severe burns in the elderly: Case report and review of the literature. Burns 2016, 42, e86–e92. [Google Scholar] [CrossRef]
- Gonzalez, M.R.; Fleuchot, B.; Lauciello, L.; Jafari, P.; Applegate, L.A.; Raffoul, W.; Que, Y.-A.; Perron, K. Effect of Human Burn Wound Exudate on Pseudomonas aeruginosa Virulence. Sphere 2016, 1, e00111-15. [Google Scholar] [CrossRef]
- Ghasemian, S.; Karami-Zarandi, M.; Heidari, H.; Khoshnood, S.; Kouhsari, E.; Ghafourian, S.; Maleki, A.; Kazemian, H. Molecular characterizations of antibiotic resistance, biofilm formation, and virulence determinants of Pseudomonas aeruginosa isolated from burn wound infection. J. Clin. Lab. Anal. 2023, 37, e24850. [Google Scholar] [CrossRef]
- Lima, W.G.; Silva Alves, G.C.; Sanches, C.; Antunes Fernandes, S.O.; de Paiva, M.C. Carbapenem-resistant Acinetobacter baumannii in patients with burn injury: A systematic review and meta-analysis. Burns 2019, 45, 1495–1508. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, H.A.; Yowler, C.J.; Claridge, J.A. Burn Wound Colonization, Infection, and Sepsis. Surg. Infect. (Larchmt) 2021, 22, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Cambiaso-Daniel, J.; Gallagher, J.J.; Norbury, W.B.; Finnerty, C.C.; Herndon, D.N.; Culnan, D.M. Treatment of Infection in Burn Patients. In Total Burn Care, 5th ed.; Herndon, D.N., Ed.; Elsevier Inc.: Philadelphia, PA, USA, 2018; pp. 93–113. [Google Scholar]
- Li, S.; Renick, P.; Senkowsky, J.; Nair, A.; Tang, L. Diagnostics for Wound Infections. Adv. Wound Care 2021, 10, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, H.; Kinoshita, M.; Saito, A.; Fujie, T.; Kabata, K.; Hara, E.; Ono, S.; Takeoka, S.; Saitoh, D. An ultrathin poly (L-lactic acid) nanosheet as a burn wound dressing for protection against bacterial infection. Wound Repair Regen. 2012, 20, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Kaartinen, I.S.; Kuokkanen, H.O. Suprathel® causes less bleeding and scarring than Mepilex® Transfer in the treatment of donor sites of split-thickness skin grafts. J. Plast. Surg. Hand Surg. 2011, 45, 200–203. [Google Scholar] [CrossRef]
- Suprathel® [Homepage]. Denkendorf: PolyMedics Innovations GmbH; © 2010. Available online: http://www.suprathel.de (accessed on 5 June 2023).


{kind=link}
{kind=link}
{kind=link}
| Pat. ID | Gender | Age (y) | TBSA (%) | Burn Cause | Wound Area | Burn Depth | WH S (Days) | WH J (Days) |
|---|---|---|---|---|---|---|---|---|
| 1 | Male | 33 | 0.5 | Explosion | Left hand | pt-to-dd | 13 | 13 |
| 2 | Male | 31 | 1 | Flame | Left foot | pt-to-dd | 21 | 28 |
| 3 | Male | 24 | 5 | Scald | Both hands | pt-to-dd | 15 | 18 |
| 4 | Male | 31 | 23 | Scald | Right hand | pt-to-dd | 13 | 13 |
| 5 | Male | 32 | 2 | Scald | Right hand | pt-to-dd | 22 | 22 |
| 6 | Female | 63 | 8 | Oil burn | Right hand | pt-to-dd | 13 | 13 |
| 7 | Female | 48 | 2 | Flame | Both hands | pt-to-dd | 24 | 30 |
| 8 | Male | 21 | 0.3 | Scald | Right hand | pt-to-dd | 28 | 31 |
| 9 | Male | 22 | 2 | Oil burn | Left foot | dd | Skin graft needed | 21 |
| 10 | Male | 34 | 1 | Explosion | Both hands | pt-to-dd | 11 | 11 |
| 11 | Male | 35 | 1.5 | Scald | Right hand | pt-to-dd | 13 | 10 |
| 12 | Male | 21 | 0.8 | Flame | Right hand | pt-to-dd | 21 | 21 |
| 13 | Male | 55 | 2 | Flame | Both hands | pt-to-dd | 21 | 21 |
| 14 | Male | 25 | 1 | Scald | Right hand | pt-to-dd | 12 | 12 |
| 15 | Male | 21 | 2 | Explosion | Right hand | pt-to-dd | 14 | 14 |
| 16 | Male | 49 | 10 | Flame | Right hand | pt-to-dd | 17 | 17 |
| 17 | Female | 72 | 1 | Scald | Right hand | pt-to-dd | 18 | 14 |
| 18 | Female | 47 | 16 | Flame | Left hand | pt-to-dd | 28 | 28 |
| 19 | Trans | 54 | 1.5 | Scald | Left hand | pt-to-dd | 23 | 18 |
| 20 | Male | 40 | 1 | Flame | Left hand | pt-to-dd | 22 | 22 |
| 21 | Male | 58 | 10 | Flame | Right hand | pt-to-dd | 18 | 18 |
| 22 | Male | 46 | 5 | Scald | Left hand | pt-to-dd | 22 | 22 |
| 23 | Male | 39 | 2.5 | Scald | Right hand | pt-to-dd | 15 | 15 |
| MEAN | 39.17 | 4.31 | 18.44 | 18.81 | ||||
| SD | 14.67 | 5.68 | 4.78 | 5.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heitzmann, W.; Mossing, M.; Fuchs, P.C.; Akkan, J.; Seyhan, H.; Grieb, G.; Opländer, C.; Schiefer, J.L. Comparative Clinical Study of Suprathel® and Jelonet® Wound Dressings in Burn Wound Healing after Enzymatic Debridement. Biomedicines 2023, 11, 2593. https://doi.org/10.3390/biomedicines11102593
Heitzmann W, Mossing M, Fuchs PC, Akkan J, Seyhan H, Grieb G, Opländer C, Schiefer JL. Comparative Clinical Study of Suprathel® and Jelonet® Wound Dressings in Burn Wound Healing after Enzymatic Debridement. Biomedicines. 2023; 11(10):2593. https://doi.org/10.3390/biomedicines11102593
Chicago/Turabian StyleHeitzmann, Wolfram, Mitja Mossing, Paul Christian Fuchs, Jan Akkan, Harun Seyhan, Gerrit Grieb, Christian Opländer, and Jennifer Lynn Schiefer. 2023. "Comparative Clinical Study of Suprathel® and Jelonet® Wound Dressings in Burn Wound Healing after Enzymatic Debridement" Biomedicines 11, no. 10: 2593. https://doi.org/10.3390/biomedicines11102593
APA StyleHeitzmann, W., Mossing, M., Fuchs, P. C., Akkan, J., Seyhan, H., Grieb, G., Opländer, C., & Schiefer, J. L. (2023). Comparative Clinical Study of Suprathel® and Jelonet® Wound Dressings in Burn Wound Healing after Enzymatic Debridement. Biomedicines, 11(10), 2593. https://doi.org/10.3390/biomedicines11102593